Tue, Jul 28, 2026
Volume 15, Issue 2 (Spring 2025)
PTJ 2025, 15(2): 101-110 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Massah O, Arab A M, Farhoudian A, Noroozi M, Hashemirad F. The Relationship Between Opium Smoking and Sway Back Posture and Spinal Musculoskeletal Disorders. PTJ 2025; 15 (2) :101-110
URL: http://ptj.uswr.ac.ir/article-1-643-en.html
URL: http://ptj.uswr.ac.ir/article-1-643-en.html



1- Substance Abuse and Dependence Researcher Center, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
2- Department of Physiotherapy, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
3- Department of Psychiatry, School of Medicine, Tehran University of Medical Sciences, Tehran, Iran.
4- Substance Abuse and Dependence Researcher Center, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran. & Department of Psychiatry, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran. & Psychosis Research Center, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
2- Department of Physiotherapy, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
3- Department of Psychiatry, School of Medicine, Tehran University of Medical Sciences, Tehran, Iran.
4- Substance Abuse and Dependence Researcher Center, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran. & Department of Psychiatry, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran. & Psychosis Research Center, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
Full-Text [PDF 488 kb]
(553 Downloads)
| Abstract (HTML) (4436 Views)
Full-Text: (456 Views)
Introduction
Opium use disorder has increased worldwide due to the increase in poppy cultivation in countries such as Myanmar and Afghanistan in recent years [1, 2]. This problem is severe in Asia and has become a constant crisis in the neighboring countries of opium producers. Iran has a long border with Afghanistan and is a suitable route for opium transit and smuggling to Europe and America [3]. Most opium seized in the world is reported from Iran. Iran ranks second in opium consumption in the world and first in terms of opium consumption through smoking [1]. One of the main health concerns in Iran is the high prevalence of opioid use and dependence, and opium smoking has been common in parts of Asia, especially Iran, for centuries [4].
In Iran, opium dependence is associated with another addictive behavior. This addictive behavior is the same as opium smoking. In fact, in addition to dependence on morphine of opium, people are also dependent on smoking opium. They do not accept the oral consumption of opium and smoke opium even in impossible conditions. Since ancient times in Iran, there has been a strong interest in opium smoking with Wafour (Vafour) or hookah, and it usually takes long minutes a day [3-5]. The body position during opium smoking is usually non-standard and non-ergonomic.
Posture deformity is any change in the relative arrangement of body parts associated with excessive tension or pressure on body tissues and structures. According to the musculoskeletal chain system and the body’s posture, any change and deformity will cause a compensatory change in the shape and function of the adjacent muscles and joints [6]. In case of continuation and repetition of placement in abnormal positions, the postural abnormalities of the spine will increase quantitatively and qualitatively. For example, previous studies have reported that people with hyperkyphosis of the spine use the hip or ankle joint to control balance more than healthy people [7]. Therefore, knowing and preventing these abnormal positions at any stage can have health and even economic (cost-benefit) justification.
Sway-back posture is one of the most common spine deformities, which has been reported to be very high (between 10% and 62%) in research [8, 9]. The prevalence of this abnormality is high in some athletes and is also related to musculoskeletal disorders and diseases [10, 11, 12]. Many drug users are not normal in terms of physical condition (posture), and at first glance, kyphotic or sway-back posture is evident in them [13, 14]. Opium is the most smoked substance in Iran. More than 75% of the substances used in Iran are opiates.
On the other hand, more than 95% of drug consumption in Iran is through smoking [4, 15]. Opium smoking is a slow and time-consuming process, usually taking 1-3 hours a day [3, 5]. Since the body position is not neutral during opium smoking, there is a possibility of postural deformity after years of opium smoking. Alternatively, those who inhale or inject heroin immediately after consumption experience a sharp and sudden loss of consciousness and fall asleep for long minutes (in a non-ergonomic, kyphotic, head-down position) [16, 17].
Considering the high prevalence of opium smoking in Iran, the need to pay attention to the possible consequences of this issue is a health priority, and the sooner it is fixed, the less expensive it will be. It seems that due to the high prevalence of marijuana, cocaine, and heroin consumption in Europe and America, the duration of their smoking is short, and the non-ergonomic state of the body while smoking is not a priority for health and rehabilitation. However, this problem exists in Iran in many different forms. Various studies have shown that some postural deformities are more common in the labor force, who work several hours a day, or in athletes who train for hours in a non-neutral position [18-20]. The review of the literature testifies that the study of musculoskeletal disorders and postural deformities in people who smoke opium has received little attention. Considering the high prevalence of opium smoking in Iran, this study was conducted to compare sway-back posture and musculoskeletal problems between those who smoke opium and normal people and investigate the factors affecting it.
Materials and Methods
Study participants
This cross-sectional study was done through a comparative method in Tehran City, Iran, in 2022. The statistical population of the patient group in this research comprised people with opioid use disorder living in Tehran. To select study samples, 4 centers from different areas of Tehran were selected as sampling heads. Then, among the clients at these centers, the first and primary samples were selected, and other samples were selected using the snowball method. In this way, 80 people with opioid use disorder were selected according to the study criteria. Also, 74 healthy people from friends and relatives of the first group were included in the study by matching method. To have the greatest similarity between the two groups’ samples, each cluster’s main branches were chosen randomly. Then we asked each of these people to introduce two people to us. One of his friends or colleagues or relatives who uses drugs and one who does not use drugs, and so on, the introduction of the following examples continued.
The following criteria were considered to select the samples of the drug user group: Diagnosis of substance use disorder (opioid dependence) according to ICD-11 criteria [21], opium is the main substance used in the samples, and the main method of consumption is smoking, ability to stand, aged between 25 and 50 years and body mass index (BMI) below 27.5 kg/m2 (because with this age range and BMI range, musculoskeletal disorders are not caused by the aging process or obesity) [22-24].
The exclusion criteria were as follows: history of musculoskeletal or neuromuscular disease, having any history of surgery or intervention and manipulation in shoulder girdle areas and spine, having a history of championship or regular championship sport exercises, any imbalance disorder caused by a specific disease, any obvious deformity in posture and anatomical disorder, and daily use of mobile phones and tablets for more than one hour [25].
Tools and data gathering
Data collection was done using a demographic questionnaire, the drug use section of ASI (Addiction Severity Index), and the Persian version of the Leeds dependence questionnaire (LDQ) [26, 27].
The sway angle was measured on a digital photo photographed from a sagittal view. The swing angle is formed by the vertical line that connects the spinous process of the acromion to the middle point of the greater trochanter of the femur and the line that connects the greater trochanter of the femur to the tip of the external ankle. The intersection of these two lines is the swing angle. Usually, people with a greater or equal swing angle of 10 degrees are classified as people with a sway-back posture [28].
We evaluated pain, disability, and musculoskeletal injuries in different areas of the body, including the neck, shoulders, upper back, lower back, lumbar, and upper and lower limbs, using the Nordic questionnaire. This questionnaire collects information about musculoskeletal symptoms and disorders from 9 anatomical areas of the body related to the last 7 days and 12 months [29].
To confirm the reliability of the measurement method, we conducted a primary test-retest. Ten participants were rated in an extra 4 testing sessions of the sway back posture test in 2 weeks.
Data analysis
We analyzed data using the Kolmogorov-Smirnov test, correlation coefficient tests (the Pearson correlation coefficient and Spearman correlation test), and paired t-test using SPSS software, version 23, at a significance level of <0.05.
Results
Basic variables
The average age in the group of drug users was 38.20±6.55 years, and in the non-user group was 37.80±5.88 years. Also, the average BMI was 24.05±2.05 kg/m2 in the drug-user group and 23.67±1.98 kg/m2 in the non-user group. The age and BMI of the two groups were not significantly different. There were 5 women (6.25%) in the opium-smoker group and 4 women (5.4%) in the non-user group.
Inter-rater and intra-rater reliability tests were done to confirm the reliability of sway angle measurement. For inter-rater reliability, the intraclass correlation coefficient (ICC) was 0.67 (CI, 0.19-0.91; P=0.42), and for intra-rater reliability, ICC was 0.63 (CI, 0.22-0.89; P=0.39).
Main variables
The sway angle was 9.4±1.41 degrees in the drug-use group and 6.62±1.35 degrees in the non-users group. Regarding sway-back posture, the two groups differed significantly (P=0.007).
Correlation tests were used to investigate the possible relationship between the independent variables of opium smoking and the increase in the sway angle in the drug-user group.
As seen in Table 1, dependence severity, the number of months of opium smoking, the daily duration of opium smoking (minutes), and homelessness have a significant relationship with the sway angle.
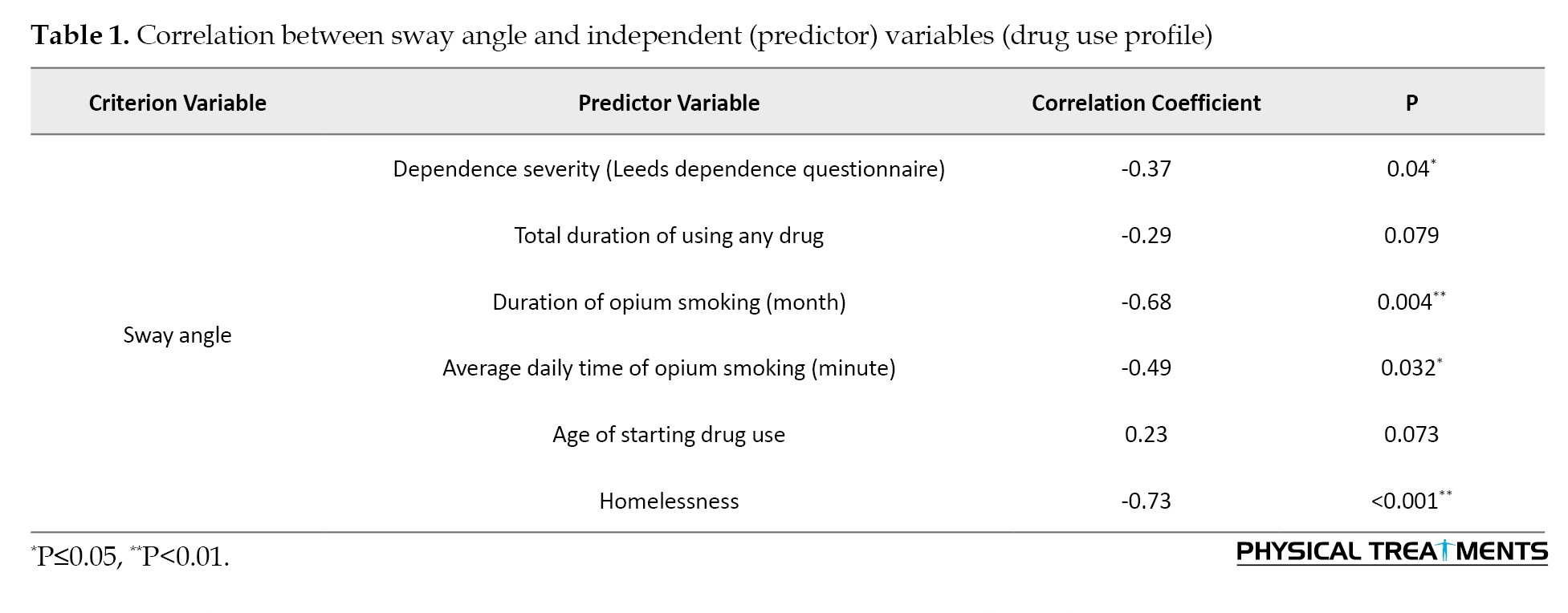
As it is clear, homelessness has the strongest correlation and significance. In addition, among the number of months of opium smoking during life and the daily duration of opium smoking (minutes), the number of months of opium smoking showed a stronger correlation with sway-back posture.
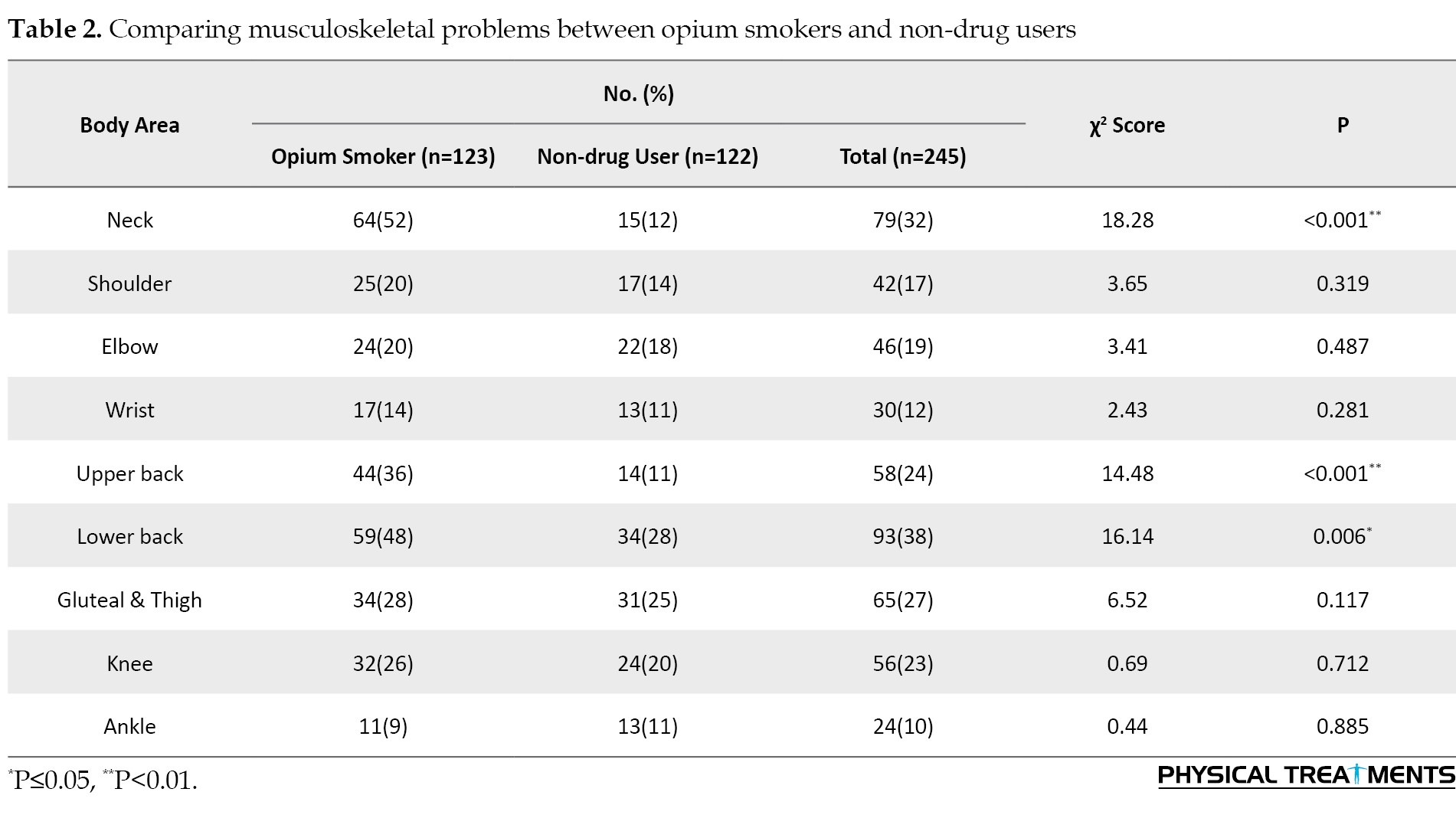
To compare the musculoskeletal problems between the two groups, we used the Nordic questionnaire. As seen in Table 2, opium smokers had significantly more problems in the neck as well as the upper and lower back.
Considering the significant difference between the two groups in neck and upper and lower back problems, the correlation of musculoskeletal problems in these three body areas and independent variables (drug use profile) was investigated to identify more related factors.
The correlation results of neck and upper and lower back musculoskeletal problems with independent variables (drug use profile) are presented in Table 3.
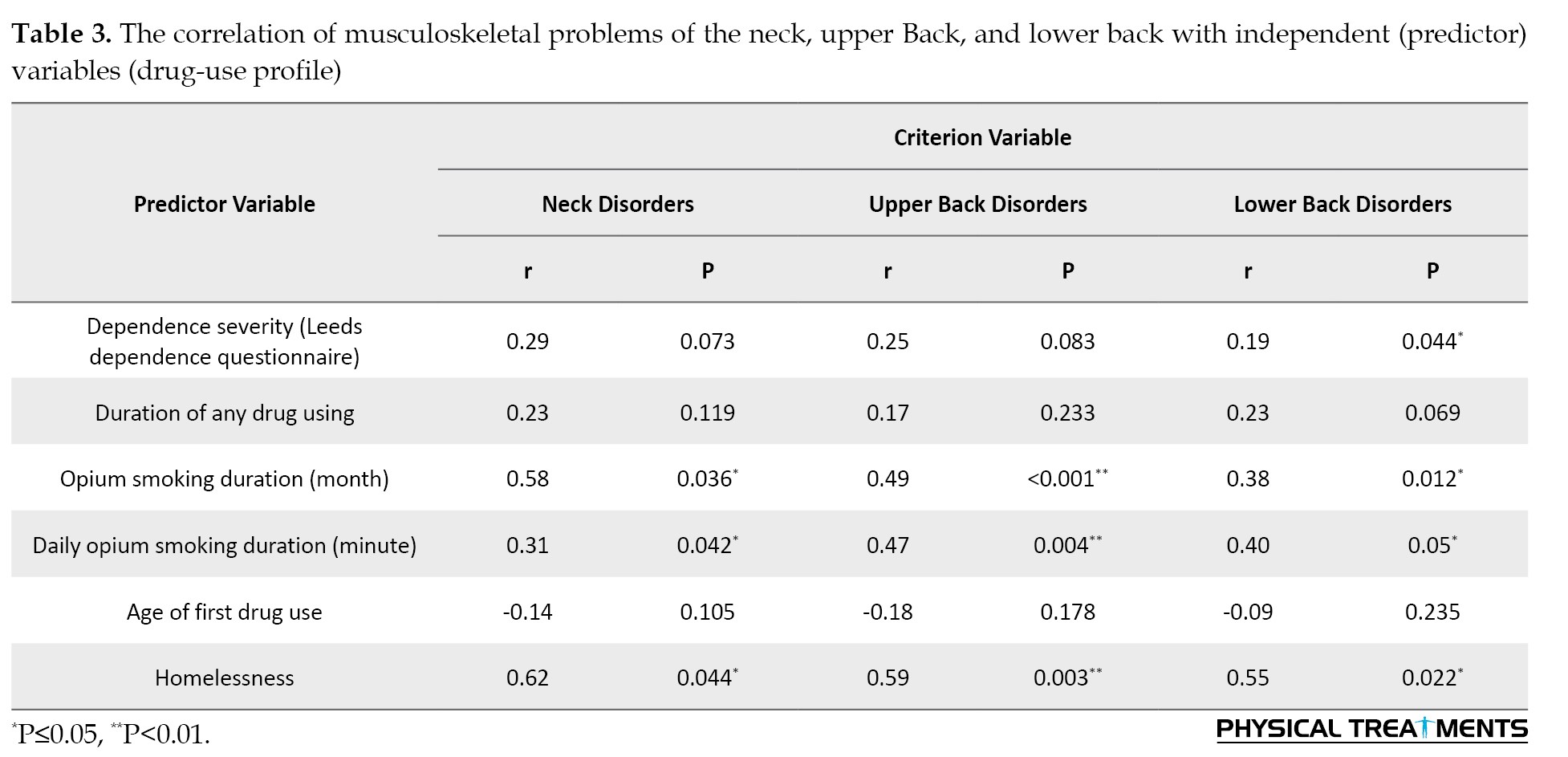
As seen in Table 3, there is a significant correlation between the number of months of opium smoking during life, the duration of daily minutes of opium smoking, and homelessness with neck and upper and lower back musculoskeletal problems. Like the sway angle, musculoskeletal problems in these three body areas strongly correlate with homelessness. The dependence severity has a significant correlation only with lower back musculoskeletal problems.
Discussion
Although the transmission of infectious diseases among drug addicts in Iran was significantly reduced and almost controlled following the national opioid addiction treatment program with agonist drugs, opioid abuse is still prevalent in Iran, especially opium smoking, and this problem has increased after the COVID-19 pandemic. Opium smoking by traditional methods and with its special tools in Iran causes a large volume of smoke to enter the lungs for several hours a day. Also, they sit in a non-neutral position for several hours a day, and the possibility of musculoskeletal complications due to being in such a position for many years is very high. These problems have been shown in various industries, office jobs, and sports. For example, hyperkyphosis is very common in professional cyclists because they practice for hours a day in a bent and non-ergonomic position and suffer from postural deformity after a few years [11]. Also, forward head posture, kyphosis, and lordosis are more prevalent in ping pong and Wushu athletes than in the general population because these athletes train for hours in positions that lead to postural deformity after years [18, 20]. Musculoskeletal disorders and postural deformity are more common in many occupations requiring long hours of work in a non-neutral posture, those who perform repetitive movements with their hands up and head forward, or people who sit in a static position inactively [30-34].
Although the effect of opium smoking on people’s posture has not been investigated in past studies, the non-neutral position of the body during opium smoking and several hours of immobility is similar to many occupations and work-related posture deformity and musculoskeletal disorders. For example, the Rosecrance et al.'s study showed that 50% of musculoskeletal disorders in construction industry workers are due to non-neutral body positions during work and long-term static positions [35]. Also, studies have shown that among the variables investigated in construction, the duration of standing and sitting during work has a significant relationship with back disorders [36, 37]. In jobs that work with machines and are usually done sitting, the harmful position of sitting on a chair, bending, and alternating rotations of the person to the sides (for better control of the work) increase the disorders in the lumbar region [38].
Being in certain positions and repeating them daily for several hours causes changes in posture, as previous studies have shown that professional gymnasts and cyclists have a more deviant sway-back posture. Although the exact reason for the higher prevalence of sway-back posture in cyclists and gymnasts is unknown, many studies have proven a higher prevalence [12, 39]. In this study, sway-back posture was more common in opium smokers. The higher prevalence of postural deformity in a certain group suggests the possibility of correlation with their occupational position, sports status, or daily habits. For this reason, the higher prevalence of bent posture in opium smokers is probably caused by their posture while smoking opium.
In this study, based on the results of the Nordic questionnaire, musculoskeletal disorders of the neck, upper back, and lower back were found to be more common in opium smokers. They were correlated with prolonged sitting in a non-neutral position (both lifetime duration of opium smoking in months and daily duration of opium smoking in minutes). Similarly, Rahmani’s study reported neck pain and problems in dentists [40]. Musculoskeletal problems of the neck in dentists are correlated with their long-term sitting in the dental unit, poor posture, and repetitive occupational movements [41, 42]. Working in non-ergonomic positions has been reported as a risk factor for neck pain and musculoskeletal problems in computer operators whose keyboards are in an inappropriate position [43, 44]. Musculoskeletal problems of the upper and lower back are also prevalent in many jobs because they must work several hours a day in a non-neutral position (sitting or standing) [45-47]. The association of non-neutral body posture and harmful position with neck, shoulder, and back disorders in dam construction workers has also been reported. Their posture during sitting activities during work, standing or sitting static positions is the main cause of back disorders [48, 49].
The high prevalence of hyperkyphosis in people with sway-back posture has been shown in previous studies [50, 51]. A higher prevalence of hyperkyphosis has also been shown in people who smoke opium [13, 14], and in this study, they also had a more sway-back posture. Also, forward head posture is more prevalent in people with a sway-back posture, which is in line with Posture’s findings in opium smokers [6].
Although longitudinal and prospective causal studies have not been conducted on opium smokers regarding the definitive effect of body posture during opium smoking on musculoskeletal disorders and posture deformity, many studies have proven the association between improper body posture and musculoskeletal disorders. Therefore, with the high probability of a causal relationship between the non-ergonomic position of opium smoking and postural deformity and musculoskeletal disorders, it is suggested that other studies confirm this relationship.
Conclusion
Non-ergonomic position while smoking opium is strongly associated with musculoskeletal problems such as pain and dysfunction in the neck, upper back, and lower back and sway back posture. Different methods of opium smoking for long hours a day, after several years, can lead to neck and upper and lower back musculoskeletal disorders and an increase in sway angle (sway-back posture). It seems that plasticity and structural and functional adaptations of the posture occur due to opium smoking, and further studies are recommended.
The limitations of this study that should be addressed are as follows. First, there are few similar studies in this field in Iran and the world. Therefore, a literature review gives the researcher few experiences and comparative analysis of data with similar data is impossible. Another limitation of the study was the non-participation of women, so the data were not analyzed and compared by gender because there were very few women. There is a possibility of inaccurate answers, underestimation, and even dishonest answers in this study, which should be considered the third limitation.
Ethical Considerations
Compliance with ethical guidelines
We obtained written consent from all participants, who were allowed to withdraw from the research at any stage. The study has been approved by the Ethics Committee of the University of Social Welfare and Rehabilitation Sciences (Code: IR.USWR.REC.1398.120).
Funding
The present article was extracted from the PhD dissertation of Omid Massah and approved by Ethics Committee of University of Social Welfare and Rehabilitation Sciences.
Authors' contributions
Data collection and Data analysis: Omid Massah; Design, Drafting, Writing, and Editing: Omid Massah, Amir Masoud Arab, Ali Farhoudian, Mehdi Noroozi, and Fahimeh Hashemirad; Approval the latest version: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
We thank the participants of both groups for taking part in this study.
References
Opium use disorder has increased worldwide due to the increase in poppy cultivation in countries such as Myanmar and Afghanistan in recent years [1, 2]. This problem is severe in Asia and has become a constant crisis in the neighboring countries of opium producers. Iran has a long border with Afghanistan and is a suitable route for opium transit and smuggling to Europe and America [3]. Most opium seized in the world is reported from Iran. Iran ranks second in opium consumption in the world and first in terms of opium consumption through smoking [1]. One of the main health concerns in Iran is the high prevalence of opioid use and dependence, and opium smoking has been common in parts of Asia, especially Iran, for centuries [4].
In Iran, opium dependence is associated with another addictive behavior. This addictive behavior is the same as opium smoking. In fact, in addition to dependence on morphine of opium, people are also dependent on smoking opium. They do not accept the oral consumption of opium and smoke opium even in impossible conditions. Since ancient times in Iran, there has been a strong interest in opium smoking with Wafour (Vafour) or hookah, and it usually takes long minutes a day [3-5]. The body position during opium smoking is usually non-standard and non-ergonomic.
Posture deformity is any change in the relative arrangement of body parts associated with excessive tension or pressure on body tissues and structures. According to the musculoskeletal chain system and the body’s posture, any change and deformity will cause a compensatory change in the shape and function of the adjacent muscles and joints [6]. In case of continuation and repetition of placement in abnormal positions, the postural abnormalities of the spine will increase quantitatively and qualitatively. For example, previous studies have reported that people with hyperkyphosis of the spine use the hip or ankle joint to control balance more than healthy people [7]. Therefore, knowing and preventing these abnormal positions at any stage can have health and even economic (cost-benefit) justification.
Sway-back posture is one of the most common spine deformities, which has been reported to be very high (between 10% and 62%) in research [8, 9]. The prevalence of this abnormality is high in some athletes and is also related to musculoskeletal disorders and diseases [10, 11, 12]. Many drug users are not normal in terms of physical condition (posture), and at first glance, kyphotic or sway-back posture is evident in them [13, 14]. Opium is the most smoked substance in Iran. More than 75% of the substances used in Iran are opiates.
On the other hand, more than 95% of drug consumption in Iran is through smoking [4, 15]. Opium smoking is a slow and time-consuming process, usually taking 1-3 hours a day [3, 5]. Since the body position is not neutral during opium smoking, there is a possibility of postural deformity after years of opium smoking. Alternatively, those who inhale or inject heroin immediately after consumption experience a sharp and sudden loss of consciousness and fall asleep for long minutes (in a non-ergonomic, kyphotic, head-down position) [16, 17].
Considering the high prevalence of opium smoking in Iran, the need to pay attention to the possible consequences of this issue is a health priority, and the sooner it is fixed, the less expensive it will be. It seems that due to the high prevalence of marijuana, cocaine, and heroin consumption in Europe and America, the duration of their smoking is short, and the non-ergonomic state of the body while smoking is not a priority for health and rehabilitation. However, this problem exists in Iran in many different forms. Various studies have shown that some postural deformities are more common in the labor force, who work several hours a day, or in athletes who train for hours in a non-neutral position [18-20]. The review of the literature testifies that the study of musculoskeletal disorders and postural deformities in people who smoke opium has received little attention. Considering the high prevalence of opium smoking in Iran, this study was conducted to compare sway-back posture and musculoskeletal problems between those who smoke opium and normal people and investigate the factors affecting it.
Materials and Methods
Study participants
This cross-sectional study was done through a comparative method in Tehran City, Iran, in 2022. The statistical population of the patient group in this research comprised people with opioid use disorder living in Tehran. To select study samples, 4 centers from different areas of Tehran were selected as sampling heads. Then, among the clients at these centers, the first and primary samples were selected, and other samples were selected using the snowball method. In this way, 80 people with opioid use disorder were selected according to the study criteria. Also, 74 healthy people from friends and relatives of the first group were included in the study by matching method. To have the greatest similarity between the two groups’ samples, each cluster’s main branches were chosen randomly. Then we asked each of these people to introduce two people to us. One of his friends or colleagues or relatives who uses drugs and one who does not use drugs, and so on, the introduction of the following examples continued.
The following criteria were considered to select the samples of the drug user group: Diagnosis of substance use disorder (opioid dependence) according to ICD-11 criteria [21], opium is the main substance used in the samples, and the main method of consumption is smoking, ability to stand, aged between 25 and 50 years and body mass index (BMI) below 27.5 kg/m2 (because with this age range and BMI range, musculoskeletal disorders are not caused by the aging process or obesity) [22-24].
The exclusion criteria were as follows: history of musculoskeletal or neuromuscular disease, having any history of surgery or intervention and manipulation in shoulder girdle areas and spine, having a history of championship or regular championship sport exercises, any imbalance disorder caused by a specific disease, any obvious deformity in posture and anatomical disorder, and daily use of mobile phones and tablets for more than one hour [25].
Tools and data gathering
Data collection was done using a demographic questionnaire, the drug use section of ASI (Addiction Severity Index), and the Persian version of the Leeds dependence questionnaire (LDQ) [26, 27].
The sway angle was measured on a digital photo photographed from a sagittal view. The swing angle is formed by the vertical line that connects the spinous process of the acromion to the middle point of the greater trochanter of the femur and the line that connects the greater trochanter of the femur to the tip of the external ankle. The intersection of these two lines is the swing angle. Usually, people with a greater or equal swing angle of 10 degrees are classified as people with a sway-back posture [28].
We evaluated pain, disability, and musculoskeletal injuries in different areas of the body, including the neck, shoulders, upper back, lower back, lumbar, and upper and lower limbs, using the Nordic questionnaire. This questionnaire collects information about musculoskeletal symptoms and disorders from 9 anatomical areas of the body related to the last 7 days and 12 months [29].
To confirm the reliability of the measurement method, we conducted a primary test-retest. Ten participants were rated in an extra 4 testing sessions of the sway back posture test in 2 weeks.
Data analysis
We analyzed data using the Kolmogorov-Smirnov test, correlation coefficient tests (the Pearson correlation coefficient and Spearman correlation test), and paired t-test using SPSS software, version 23, at a significance level of <0.05.
Results
Basic variables
The average age in the group of drug users was 38.20±6.55 years, and in the non-user group was 37.80±5.88 years. Also, the average BMI was 24.05±2.05 kg/m2 in the drug-user group and 23.67±1.98 kg/m2 in the non-user group. The age and BMI of the two groups were not significantly different. There were 5 women (6.25%) in the opium-smoker group and 4 women (5.4%) in the non-user group.
Inter-rater and intra-rater reliability tests were done to confirm the reliability of sway angle measurement. For inter-rater reliability, the intraclass correlation coefficient (ICC) was 0.67 (CI, 0.19-0.91; P=0.42), and for intra-rater reliability, ICC was 0.63 (CI, 0.22-0.89; P=0.39).
Main variables
The sway angle was 9.4±1.41 degrees in the drug-use group and 6.62±1.35 degrees in the non-users group. Regarding sway-back posture, the two groups differed significantly (P=0.007).
Correlation tests were used to investigate the possible relationship between the independent variables of opium smoking and the increase in the sway angle in the drug-user group.
As seen in Table 1, dependence severity, the number of months of opium smoking, the daily duration of opium smoking (minutes), and homelessness have a significant relationship with the sway angle.
As it is clear, homelessness has the strongest correlation and significance. In addition, among the number of months of opium smoking during life and the daily duration of opium smoking (minutes), the number of months of opium smoking showed a stronger correlation with sway-back posture.
To compare the musculoskeletal problems between the two groups, we used the Nordic questionnaire. As seen in Table 2, opium smokers had significantly more problems in the neck as well as the upper and lower back.
Considering the significant difference between the two groups in neck and upper and lower back problems, the correlation of musculoskeletal problems in these three body areas and independent variables (drug use profile) was investigated to identify more related factors.
The correlation results of neck and upper and lower back musculoskeletal problems with independent variables (drug use profile) are presented in Table 3.
As seen in Table 3, there is a significant correlation between the number of months of opium smoking during life, the duration of daily minutes of opium smoking, and homelessness with neck and upper and lower back musculoskeletal problems. Like the sway angle, musculoskeletal problems in these three body areas strongly correlate with homelessness. The dependence severity has a significant correlation only with lower back musculoskeletal problems.
Discussion
Although the transmission of infectious diseases among drug addicts in Iran was significantly reduced and almost controlled following the national opioid addiction treatment program with agonist drugs, opioid abuse is still prevalent in Iran, especially opium smoking, and this problem has increased after the COVID-19 pandemic. Opium smoking by traditional methods and with its special tools in Iran causes a large volume of smoke to enter the lungs for several hours a day. Also, they sit in a non-neutral position for several hours a day, and the possibility of musculoskeletal complications due to being in such a position for many years is very high. These problems have been shown in various industries, office jobs, and sports. For example, hyperkyphosis is very common in professional cyclists because they practice for hours a day in a bent and non-ergonomic position and suffer from postural deformity after a few years [11]. Also, forward head posture, kyphosis, and lordosis are more prevalent in ping pong and Wushu athletes than in the general population because these athletes train for hours in positions that lead to postural deformity after years [18, 20]. Musculoskeletal disorders and postural deformity are more common in many occupations requiring long hours of work in a non-neutral posture, those who perform repetitive movements with their hands up and head forward, or people who sit in a static position inactively [30-34].
Although the effect of opium smoking on people’s posture has not been investigated in past studies, the non-neutral position of the body during opium smoking and several hours of immobility is similar to many occupations and work-related posture deformity and musculoskeletal disorders. For example, the Rosecrance et al.'s study showed that 50% of musculoskeletal disorders in construction industry workers are due to non-neutral body positions during work and long-term static positions [35]. Also, studies have shown that among the variables investigated in construction, the duration of standing and sitting during work has a significant relationship with back disorders [36, 37]. In jobs that work with machines and are usually done sitting, the harmful position of sitting on a chair, bending, and alternating rotations of the person to the sides (for better control of the work) increase the disorders in the lumbar region [38].
Being in certain positions and repeating them daily for several hours causes changes in posture, as previous studies have shown that professional gymnasts and cyclists have a more deviant sway-back posture. Although the exact reason for the higher prevalence of sway-back posture in cyclists and gymnasts is unknown, many studies have proven a higher prevalence [12, 39]. In this study, sway-back posture was more common in opium smokers. The higher prevalence of postural deformity in a certain group suggests the possibility of correlation with their occupational position, sports status, or daily habits. For this reason, the higher prevalence of bent posture in opium smokers is probably caused by their posture while smoking opium.
In this study, based on the results of the Nordic questionnaire, musculoskeletal disorders of the neck, upper back, and lower back were found to be more common in opium smokers. They were correlated with prolonged sitting in a non-neutral position (both lifetime duration of opium smoking in months and daily duration of opium smoking in minutes). Similarly, Rahmani’s study reported neck pain and problems in dentists [40]. Musculoskeletal problems of the neck in dentists are correlated with their long-term sitting in the dental unit, poor posture, and repetitive occupational movements [41, 42]. Working in non-ergonomic positions has been reported as a risk factor for neck pain and musculoskeletal problems in computer operators whose keyboards are in an inappropriate position [43, 44]. Musculoskeletal problems of the upper and lower back are also prevalent in many jobs because they must work several hours a day in a non-neutral position (sitting or standing) [45-47]. The association of non-neutral body posture and harmful position with neck, shoulder, and back disorders in dam construction workers has also been reported. Their posture during sitting activities during work, standing or sitting static positions is the main cause of back disorders [48, 49].
The high prevalence of hyperkyphosis in people with sway-back posture has been shown in previous studies [50, 51]. A higher prevalence of hyperkyphosis has also been shown in people who smoke opium [13, 14], and in this study, they also had a more sway-back posture. Also, forward head posture is more prevalent in people with a sway-back posture, which is in line with Posture’s findings in opium smokers [6].
Although longitudinal and prospective causal studies have not been conducted on opium smokers regarding the definitive effect of body posture during opium smoking on musculoskeletal disorders and posture deformity, many studies have proven the association between improper body posture and musculoskeletal disorders. Therefore, with the high probability of a causal relationship between the non-ergonomic position of opium smoking and postural deformity and musculoskeletal disorders, it is suggested that other studies confirm this relationship.
Conclusion
Non-ergonomic position while smoking opium is strongly associated with musculoskeletal problems such as pain and dysfunction in the neck, upper back, and lower back and sway back posture. Different methods of opium smoking for long hours a day, after several years, can lead to neck and upper and lower back musculoskeletal disorders and an increase in sway angle (sway-back posture). It seems that plasticity and structural and functional adaptations of the posture occur due to opium smoking, and further studies are recommended.
The limitations of this study that should be addressed are as follows. First, there are few similar studies in this field in Iran and the world. Therefore, a literature review gives the researcher few experiences and comparative analysis of data with similar data is impossible. Another limitation of the study was the non-participation of women, so the data were not analyzed and compared by gender because there were very few women. There is a possibility of inaccurate answers, underestimation, and even dishonest answers in this study, which should be considered the third limitation.
Ethical Considerations
Compliance with ethical guidelines
We obtained written consent from all participants, who were allowed to withdraw from the research at any stage. The study has been approved by the Ethics Committee of the University of Social Welfare and Rehabilitation Sciences (Code: IR.USWR.REC.1398.120).
Funding
The present article was extracted from the PhD dissertation of Omid Massah and approved by Ethics Committee of University of Social Welfare and Rehabilitation Sciences.
Authors' contributions
Data collection and Data analysis: Omid Massah; Design, Drafting, Writing, and Editing: Omid Massah, Amir Masoud Arab, Ali Farhoudian, Mehdi Noroozi, and Fahimeh Hashemirad; Approval the latest version: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
We thank the participants of both groups for taking part in this study.
References
- United Nations Office on Drugs and Crime. World Drug Report 2022. Vienna, Austria: United Nations Office on Drugs and Crime; 2022. [Link]
- Datta A, Maran HH, Kuwornu JK. Investigation of the farmers' perceptions and participation in opium poppy cultivation in the Northern Shan State, Myanmar. International Journal of Agricultural Resources, Governance and Ecology. 2019; 15(3):181-94. [DOI:10.1504/IJARGE.2019.103307]
- Zarghami M. Iranian Common Attitude Toward Opium Consumption. Iranian Journal of Psychiatry and Behavioral sciences. 2015; 9(2):e2074. [DOI:10.17795/ijpbs2074] [PMID]
- Regavim RB. The most sovereign of masters: The history of opium in modern Iran, 1850-1955 [PhD dissertation]. Pennsylvania: University of Pennsylvania; 2012. [Link]
- Ghiabi M. Drugs politics: Managing Disorder in the Islamic Republic of Iran. Cambridge: Cambridge University Press; 2019. [Link]
- Conroy VM, Murray Jr BN, Alexopulos QT, McCreary J. Kendall's muscles: Testing and function with posture and pain. Philadelphia: Wolters Kluwer Health; 2022. [Link]
- Knudson D. Mechanics of the musculoskeletal system. In: Fundamentals of biomechanics. Cham: Springer International Publishing; 2021. [Link]
- Røgind H, Lykkegaard JJ, Bliddal H, Danneskiold-Samsøe B. Postural sway in normal subjects aged 20-70 years. Clinical Physiology and Functional Imaging. 2003; 23(3):171-6. [DOI:10.1046/j.1475-097X.2003.00492.x]
- Gill J, Allum JH, Carpenter MG, Held-Ziolkowska M, Adkin AL, Honegger F, et al. Trunk sway measures of postural stability during clinical balance tests: Effects of age. The Journals of Gerontology: Series A, Biological Sciences and Medical Sciences. 2001; 56(7):M438-47. [DOI:10.1093/gerona/56.7.m438] [PMID]
- Öhlen G, Wredmark T, Spangfort E. Spinal sagittal configuration and mobility related to low-back pain in the female gymnast. Spine. 1989; 14(8):847-50. [DOI:10.1097/00007632-198908000-00013]
- Muyor JM, López-Miñarro PA, Alacid F. Comparison of sagittal lumbar curvature between elite cyclists and non-athletes. Science & Sports. 2013; 28(6):e167-73. [DOI:10.1016/j.scispo.2013.04.003]
- Mulhearn S, George K. Abdominal muscle endurance and its association with posture and low back pain: An initial investigation in male and female élite gymnasts. Physiotherapy. 1999; 85(4):210-6. [DOI:10.1016/S0031-9406(05)65666-0]
- Massah O, Arab AM, Farhoudian A, Noroozi M, Hashemirad F. The correlation between neck pain and disability, forward head posture, and hyperkyphosis with opium smoking: A cross-sectional study from Iran. Brain Sciences. 2023; 13(9):1281. [DOI:10.3390/brainsci13091281] [PMID]
- Massah O, Arab AM, Farhoudian A, Noroozi M, Hashemirad F. Association between opium smoking and neck and upper spine posture disorders. Iran J Psychiatry Behav Sci. 2023; 17(3):e138142. [DOI:10.5812/ijpbs-138142]
- Rafiey H, Alipour F, Madani S, Narenjiha H. [Rapid situation assessment of drug abuse in Iran, 2018 (Persian)]. Tehran: Department of Research and Education, Drug Control Headquarters; 2018.
- Alambyan V, Pace J, Miller B, Cohen ML, Gokhale S, Singh G, et al. The emerging role of inhaled heroin in the opioid epidemic: A review. JAMA Neurology. 2018; 75(11):1423-34. [Link]
- Sporer KA. Acute heroin overdose. Annals of Internal Medicine. 1999; 130(7):584-90. [DOI:10.7326/0003-4819-130-7-199904060-0001]
- Sadeghi M, Ghasemi GA, Iraj F. [Comparing selected spinal column postural abnormalities of professional and amateur Wushu athletes with those of non-athletes (Persian)]. Journal of Research in Rehabilitation Sciences. 2012; 8(3):582-9. [Link]
- Valachi B, Valachi K. Mechanisms leading to musculoskeletal disorders in dentistry. The Journal of the American Dental Association. 2003; 134(10):1344-50. [DOI:10.14219/jada.archive.2003.0048] [PMID]
- Bagherian S, Rahnama N, Mahmudi F. Investigation of Curves of the spinal cord of the table tennis athletes. Proceedings of the 6th National Conference on Physical Education Students. 2011; 24-6. [Link]
- Poznyak V, Reed GM, Medina-Mora ME. Aligning the ICD-11 classification of disorders due to substance use with global service needs. Epidemiology and Psychiatric Sciences. 2018; 27(3):212-8. [DOI:10.1017/S2045796017000622]
- Mozafari A, Vahedian M, Mohebi S, Najafi M. Work-related musculoskeletal disorders in truck drivers and official workers. Acta Medica Iranica. 2015; 53(7):432-8. [PMID]
- Hambright WS, Niedernhofer LJ, Huard J, Robbins PD. Murine models of accelerated aging and musculoskeletal disease. Bone. 2019; 125:122-7. [DOI:10.1016/j.bone.2019.03.002] [PMID]
- Sethi J, Sandhu JS, Imbanathan V. Effect of Body Mass Index on work related musculoskeletal discomfort and occupational stress of computer workers in a developed ergonomic setup. Sports Medicine, Arthroscopy, Rehabilitation, Therapy & Technology. 2011; 3(1):22. [DOI:10.1186/1758-2555-3-22] [PMID]
- Fiebert I, Kistner F, Gissendanner C, DaSilva C. Text neck: An adverse postural phenomenon. Work. 2021; 69(4):1261-70.[DOI:10.3233/WOR-213547]
- Cacciola JS, Alterman AI, McLellan AT, Lin YT, Lynch KG. Initial evidence for the reliability and validity of a “Lite” version of the Addiction Severity Index. Drug and Alcohol Dependence. 2007; 87(2):297-302. [DOI:10.1016/j.drugalcdep.2006.09.002]
- Massah O, Rafiey H, Shariatirad S, Radfar SR, Ahounbar E, Farhoudian A. The Validity and Reliability of the Persian Version of the Leeds Dependence Questionnaire. Iranian Rehabilitation Journal. 2019; 17(2):91-6. [DOI:10.32598/irj.17.2.91]
- Petermann XB, Meereis EC. Postural body: a systematic review about assessment methods. Manual Therapy, Posturology & Rehabilitation Journal. 2016 ; 1-9. [DOI:10.17784/mtprehabjournal.2016.14.0273]
- Kuorinka I, Jonsson B, Kilbom A, Vinterberg H, Biering-Sørensen F, Andersson G, et al. Standardised Nordic questionnaires for the analysis of musculoskeletal symptoms. Applied Ergonomics. 1987; 18(3):233-7. [DOI:10.1016/0003-6870(87)90010-x] [PMID]
- Anghel M, Argesanu V, Talpos-Niculescu C, Lungeanu D. Musculoskeletal disorders (MSDs)-consequences of prolonged static postures. Journal of Experimental Medical & Surgical Research. 2007; 4:167-72. [Link]
- Lee YK, Park HS. Workers’ perception of the changes of work environment and its relation to the occurrence of work-related musculoskeletal disorders. Journal of Occupational Health. 2007; 49(2):152-4. [Link]
- Diana V. Literature review: Effect of static conditions on Musculoskeletal Disorders (MSDs). Basic and Applied Nursing Research Journal. 2021; 2(2):52-9. [Link]
- Epstein S, Sparer EH, Tran BN, Ruan QZ, Dennerlein JT, Singhal D, et al. Prevalence of work-related musculoskeletal disorders among surgeons and interventionalists: A systematic review and meta-analysis. JAMA Surgery. 2018; 153(2):e174947. [DOI:10.1001/jamasurg.2017.4947] [PMID]
- Pascarelli EF, Hsu YP. Understanding work-related upper extremity disorders: Clinical Findings in 485 Computer Users, Musicians, and Others. Journal of Occupational Rehabilitation. 2001; 11(1):1-21. [DOI:10.1023/a:1016647923501]
- Rosecrance J, Pórszász J, Cook T, Fekecs E, Karácsony T, Merlino L, et al. Musculoskeletal disorders among construction apprentices in Hungary. Central European Journal of Public Health. 2001; 9(4):183-7. [PMID]
- Hajaghazadeh M, Nasl saraji J, Hosseini M, Adl J. [Ergonomic assessment of musculoskeletal disorder risk factors in construction workers by PATH method (Persian)]. Journal of School of Public Health and Institute of Public Health Research. 2008; 6(1):37-45. [Link]
- Rwamamara RA, Lagerqvist O, Olofsson T, Johansson BM, Kaminskas KA. Evidence-based prevention of work-related musculoskeletal injuries in construction industry. Journal of Civil engineering and Management. 2010; 16(4):499-509. [Link]
- Armstrong T BP, Fine L, Hagberg M, Haring-Sweeney M, Martin B, Punnett L, et al. Musculoskeletal Disorders: Work-related Risk Factors and Prevention. International Journal of Occupational and Environmental Health. 1996; 2(3):239-46.[Link]
- Muyor JM, López-Miñarro PA, Alacid F. Spinal posture of thoracic and lumbar spine and pelvic tilt in highly trained cyclists. Journal of Sports Science & Medicine. 2011; 10(2):355-61. [PMID]
- Rahmani N, Amiri M, Ali Mohseni-Bandpei M, Mohsenifar H, Pourahmadi MR. Work related neck pain in Iranian dentists: An epidemiological study. Journal of Back and Musculoskeletal Rehabilitation. 2013; 26(1):9-15. [DOI:10.3233/BMR-2012-0343] [PMID]
- Alexopoulos EC, Stathi IC, Charizani F. Prevalence of musculoskeletal disorders in dentists. BMC Musculoskeletal Disorders. 2004; 5:16. [DOI:10.1186/1471-2474-5-16] [PMID] [PMCID]
- Zhou Y, Zhou W, Aisaiti A, Wang B, Zhang J, Svensson P, et al. Dentists have a high occupational risk of neck disorders with impact on somatosensory function and neck mobility. Journal of Occupational Health. 2021; 63(1):e12269. [DOI:10.1002/1348-9585.12269] [PMID] [PMCID]
- Korhonen T, Ketola R, Toivonen R, Luukkonen R, Häkkänen M, Viikari-Juntura E. Work related and individual predictors for incident neck pain among office employees working with video display units. Occupational and Environmental Medicine. 2003; 60(7):475-82. [DOI:10.1136/oem.60.7.475] [PMID]
- Keown GA, Tuchin PA. Workplace Factors Associated With Neck Pain Experienced by Computer Users: A systematic review. Journal of Manipulative and Physiological Therapeutics. 2018; 41(6):508-29. [DOI:10.1016/j.jmpt.2018.01.005]
- Long MH, Bogossian FE, Johnston V. The prevalence of work-related neck, shoulder, and upper back musculoskeletal disorders among midwives, nurses, and physicians: A systematic review. Workplace Health & Safety. 2013; 61(5):223-9. [DOI:10.1177/216507991306100506]
- Panel on Musculoskeletal Disorders and the Workplace, Commission on Behavioral and Social Sciences and Education, National Research Council. Musculoskeletal Disorders and the Workplace: Low Back and Upper Extremities. Washington: National Academies Press; 2001. [Link]
- Russo F, Papalia GF, Vadalà G, Fontana L, Iavicoli S, Papalia R, et al. The effects of workplace interventions on low back pain in workers: A systematic review and meta-analysis. International Journal of Environmental Research and Public Health. 2021; 18(23):12614. [DOI:10.3390/ijerph182312614]
- Gheibi L, Zeraati H, Pouryaghub G. Assessment of ergonomic situation of workers in a dam construction workshops using the NIOSH-CPWR Checklist. Journal of School of Public Health and Institute of Public Health Research. 2009; 7(3):13-24. [Link]
- Fredriksson K, Alfredsson L, Thorbjörnsson CB, Punnett L, Toomingas A, Torgén M, et al. Risk factors for neck and shoulder disorders: A nested case-control study covering a 24-year period. American Journal of Industrial Medicine. 2000; 38(5):516-28. [DOI:10.1002/1097-0274(200011)38:5<516::aid-ajim4>3.0.co;2-0] [PMID]
- Abdolvahabi Z, Salimi naini S, kallashi M, Shabani A, Rahmati H, Letafatkar K. The effect of sway back abnormality on structural changes of body parts. Journal of Research in Rehabilitation Sciences. 2010; 6(1):52-62. [Link]
- Czaprowski D, Stoliński Ł, Tyrakowski M, Kozinoga M, Kotwicki T. Non-structural misalignments of body posture in the sagittal plane. Scoliosis and Spinal Disorders. 2018; 13:6. [PMID]
Type of Study: Research |
Subject:
General
Received: 2024/06/1 | Accepted: 2024/12/9 | Published: 2025/04/1
Received: 2024/06/1 | Accepted: 2024/12/9 | Published: 2025/04/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
