Sun, Jun 21, 2026
Volume 16, Issue 2 (Spring 2026)
PTJ 2026, 16(2): 133-150 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Khaliliyan H, Bahramizadeh M, Faghih Jouibari M, Ansari M, Batra K, Ghaffari F, et al . Effects of Ergonomic Chairs on Workplace Musculoskeletal Health: A Systematic Review. PTJ 2026; 16 (2) :133-150
URL: http://ptj.uswr.ac.ir/article-1-837-en.html
URL: http://ptj.uswr.ac.ir/article-1-837-en.html
Hanieh Khaliliyan1 

 , Mahmood Bahramizadeh *2 , Morteza Faghih Jouibari3 , Majid Ansari4 , Kavita Batra5 , Farhad Ghaffari6 , Arash Sharafatvaziri7 , Amir Reza Vosoughi8 , Hicham Khabbache9 , Francesco Chirico10
, Mahmood Bahramizadeh *2 , Morteza Faghih Jouibari3 , Majid Ansari4 , Kavita Batra5 , Farhad Ghaffari6 , Arash Sharafatvaziri7 , Amir Reza Vosoughi8 , Hicham Khabbache9 , Francesco Chirico10
, Mahmood Bahramizadeh *2 , Morteza Faghih Jouibari3 , Majid Ansari4 , Kavita Batra5 , Farhad Ghaffari6 , Arash Sharafatvaziri7 , Amir Reza Vosoughi8 , Hicham Khabbache9 , Francesco Chirico10
1- Department of Orthotics and Prosthetics, School of Rehabilitation Sciences, Isfahan University of Medical Sciences, Isfahan, Iran.
2- Neuromusculoskeletal Rehabilitation Research Center, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
3- Department of neurosurgery, Shariati Hospital, Tehran University of Medical Sciences, Tehran, Iran.
4- Sports Medicine Research Center, Neuroscience Institute, Tehran University of Medical Sciences, Tehran, Iran.
5- Department of Medical Education and Office of Research, Kirk Kerkorian School of Medicine, University of Nevada, Las Vegas, United States.
6- Orthopedic and Rehabilitation Research Center, Shiraz University of Medical Sciences, Shiraz, Iran.
7- Center for Orthopedic Trans-Disciplinary Applied Research, Tehran University of Medical Sciences, Tehran, Iran.
8- Department of Orthopedic Surgery, Foot & Ankle Surgeon, Orthopedic & Rehabilitation Research Center, School of Medicine, Shiraz University of Medical Sciences, Shiraz, Iran.
9- Department of Psychology, Faculty of Arts and Human Sciences, Fès-Saïss, Sidi Mohamed Ben Abdellah University, Fes, Morocco.
10- Department of Health Service, School of Occupational Health, Università Cattolica del Sacro Cuore, Roma, Italy.
2- Neuromusculoskeletal Rehabilitation Research Center, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
3- Department of neurosurgery, Shariati Hospital, Tehran University of Medical Sciences, Tehran, Iran.
4- Sports Medicine Research Center, Neuroscience Institute, Tehran University of Medical Sciences, Tehran, Iran.
5- Department of Medical Education and Office of Research, Kirk Kerkorian School of Medicine, University of Nevada, Las Vegas, United States.
6- Orthopedic and Rehabilitation Research Center, Shiraz University of Medical Sciences, Shiraz, Iran.
7- Center for Orthopedic Trans-Disciplinary Applied Research, Tehran University of Medical Sciences, Tehran, Iran.
8- Department of Orthopedic Surgery, Foot & Ankle Surgeon, Orthopedic & Rehabilitation Research Center, School of Medicine, Shiraz University of Medical Sciences, Shiraz, Iran.
9- Department of Psychology, Faculty of Arts and Human Sciences, Fès-Saïss, Sidi Mohamed Ben Abdellah University, Fes, Morocco.
10- Department of Health Service, School of Occupational Health, Università Cattolica del Sacro Cuore, Roma, Italy.
Keywords: Chair, Musculoskeletal disorders, Public health, Health promotion, Sitting posture, Sedentary worker
Full-Text [PDF 757 kb]
(1992 Downloads)
| Abstract (HTML) (1664 Views)
Methodological quality assessment
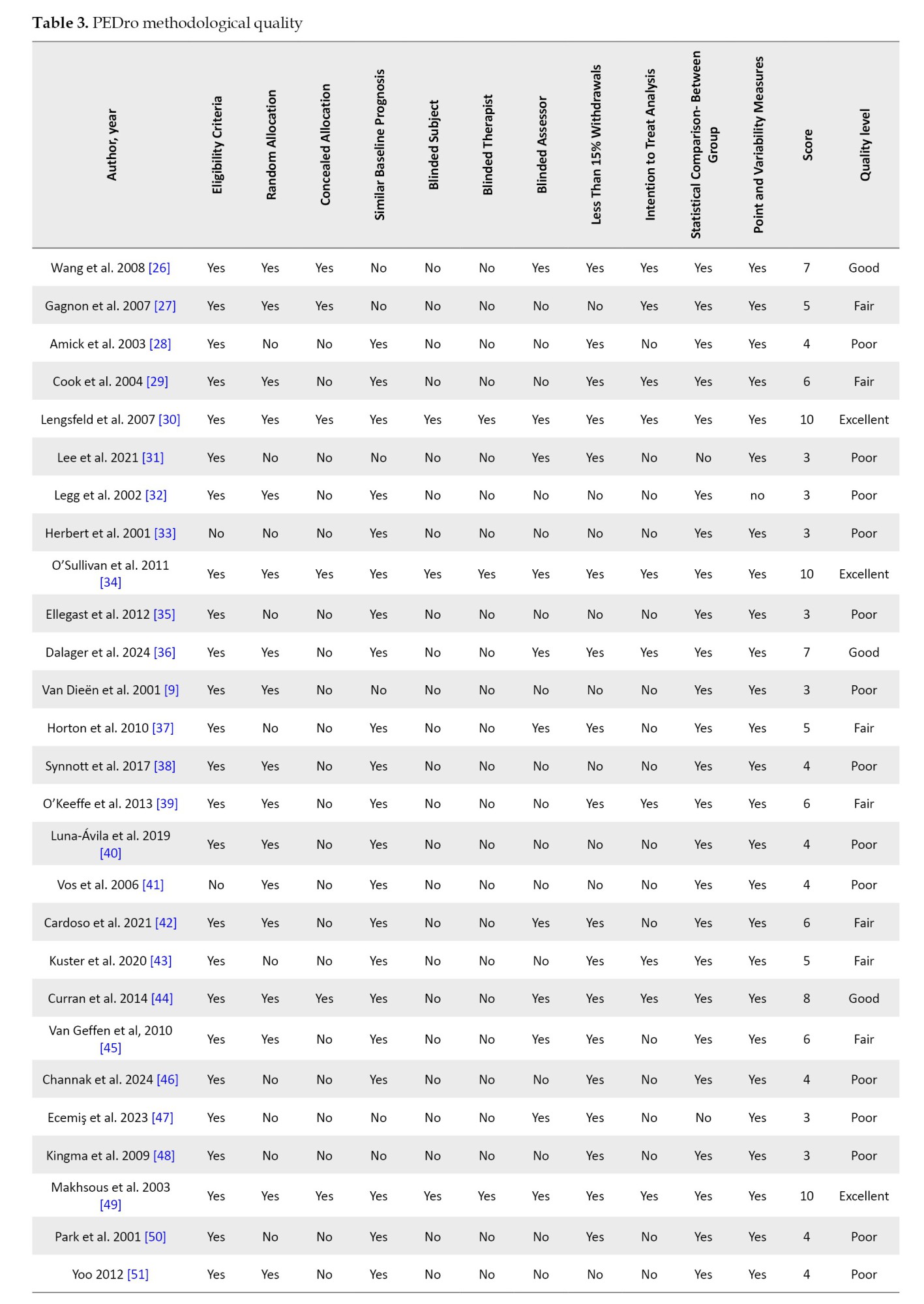
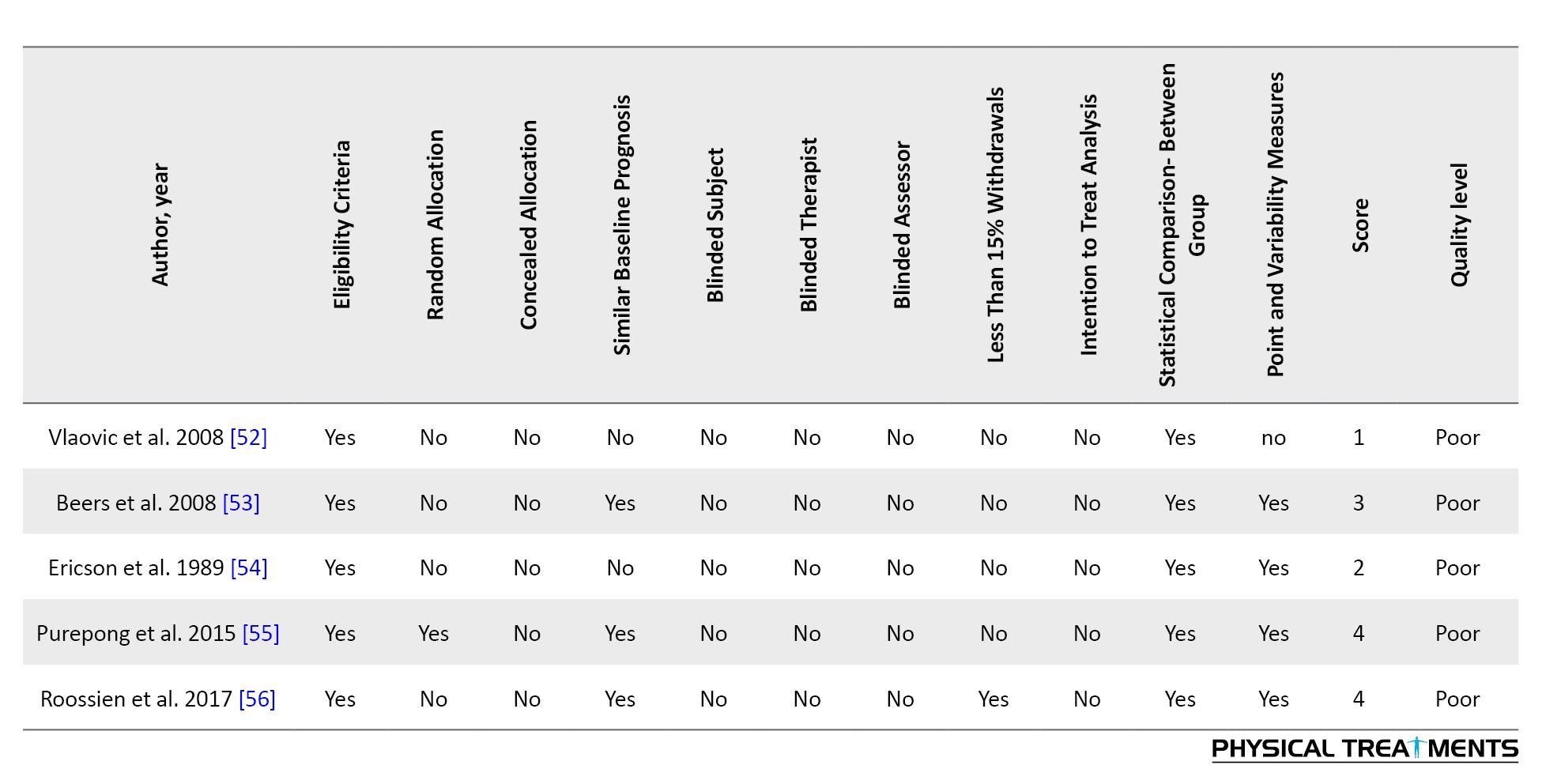
Prior to discussion, reviewers Hanieh Khaliliyan and Mahmood Bahramizadeh demonstrated an agreement rate of 89% (314 out of 352) on the PEDro scores. The overall inter-rater reliability yielded a kappa coefficient of 0.79 with a standard error of 0.05. After resolving discrepancies through discussion, the reviewers reached complete consensus, achieving 100% agreement (352 out of 352). For this sample of 32 studies, the scores ranged from a minimum score of 1 to a maximum score of 10, with a general mean score of approximately 5. This mean indicates the overall quality level within the fair category, reflecting a moderate quality of evidence across the reviewed studies. The distribution of the quality levels further breaks down as follows: Three articles rated as excellent [30, 34, 50], representing 9.37%; 3 rated as good [26, 36, 44], which is 9.37%; and 19 articles rated as poor [9, 28, 31-33, 35, 38, 40, 41, 46-48, 50-56], making up 59.37%. Furthermore, 7 articles were rated fair [27, 29, 38, 40, 43, 44, 46], accounting for 21.87% of the total. Table 2 presents the methodological quality assessment.
Study characteristics
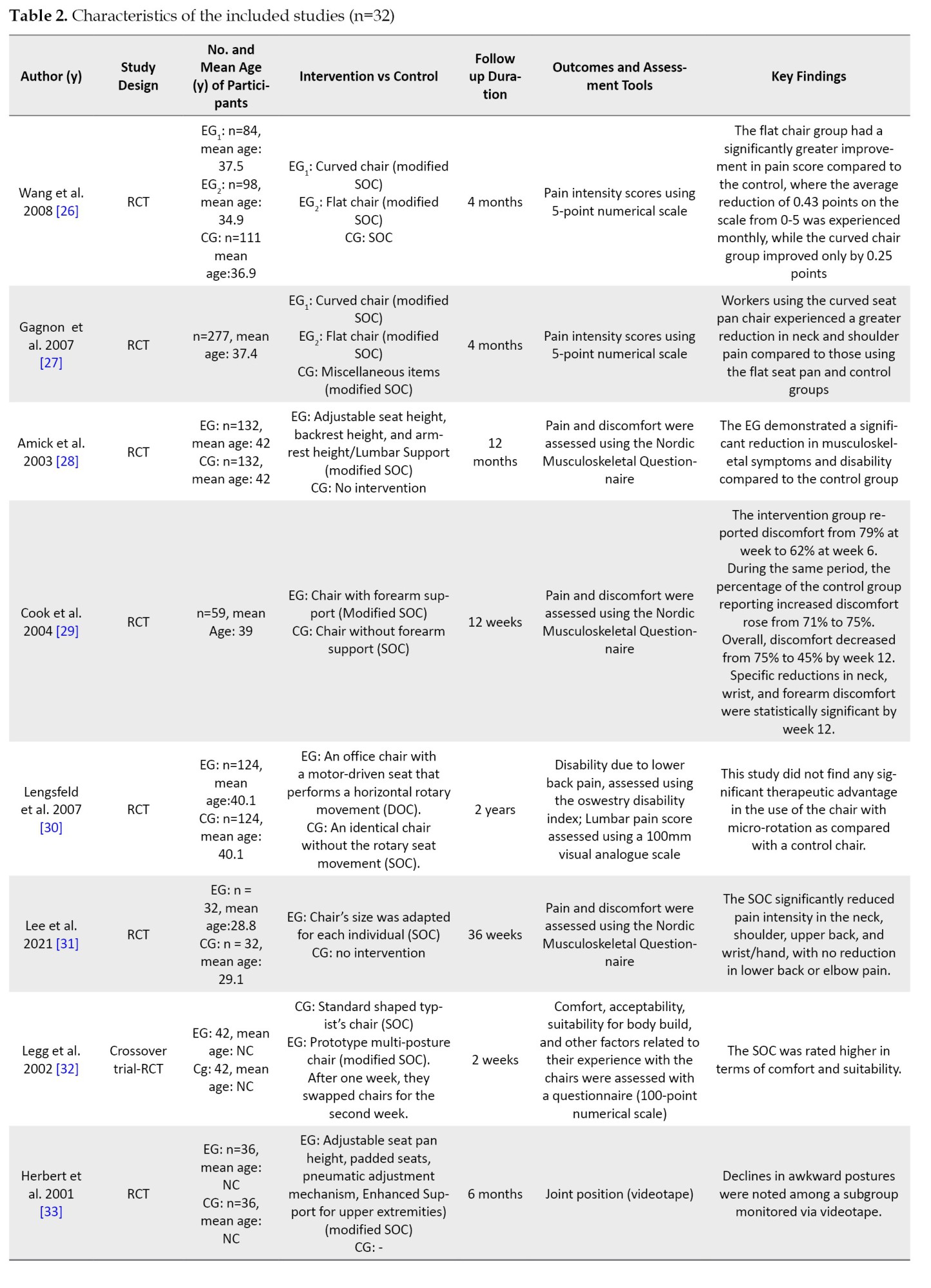
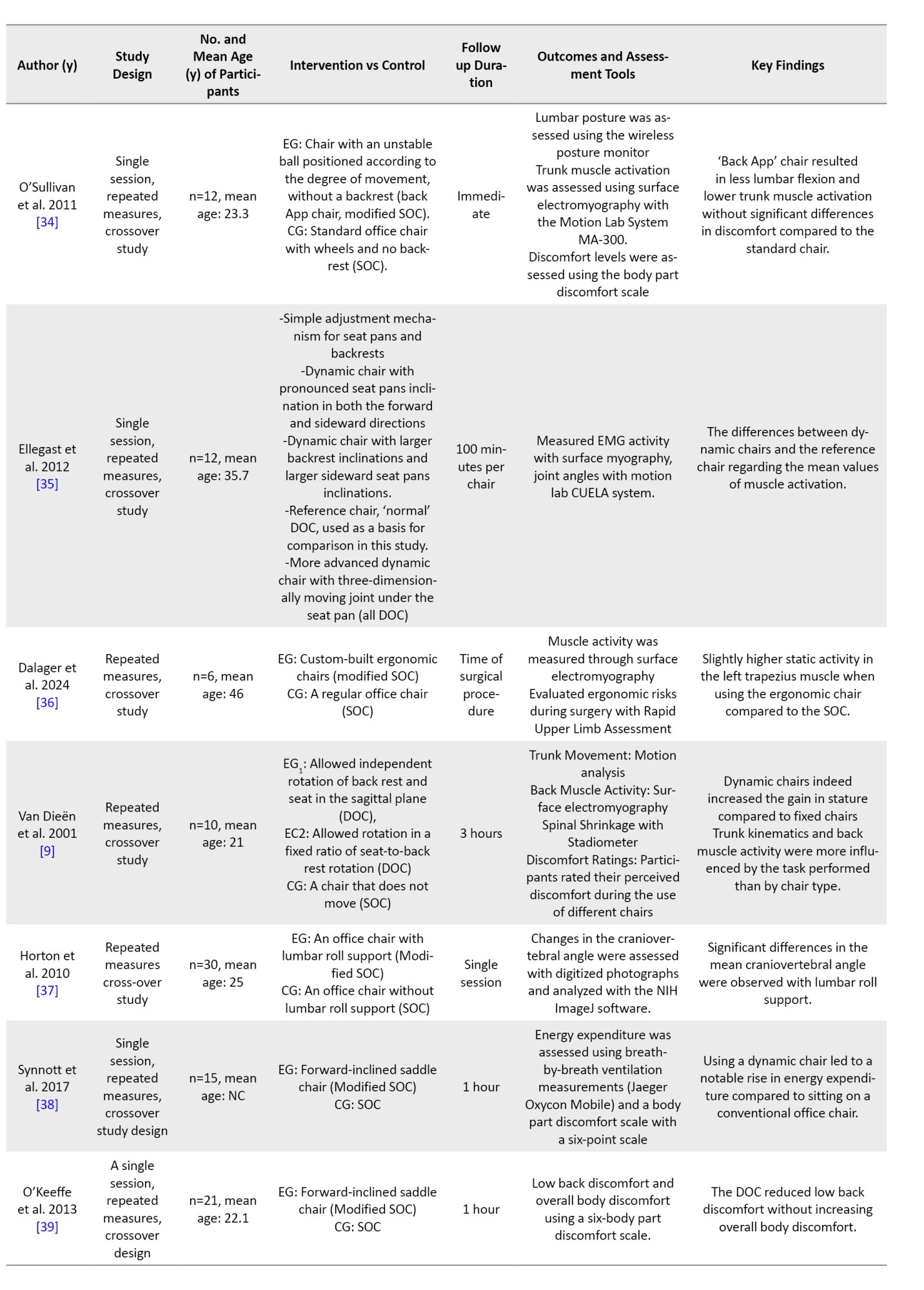
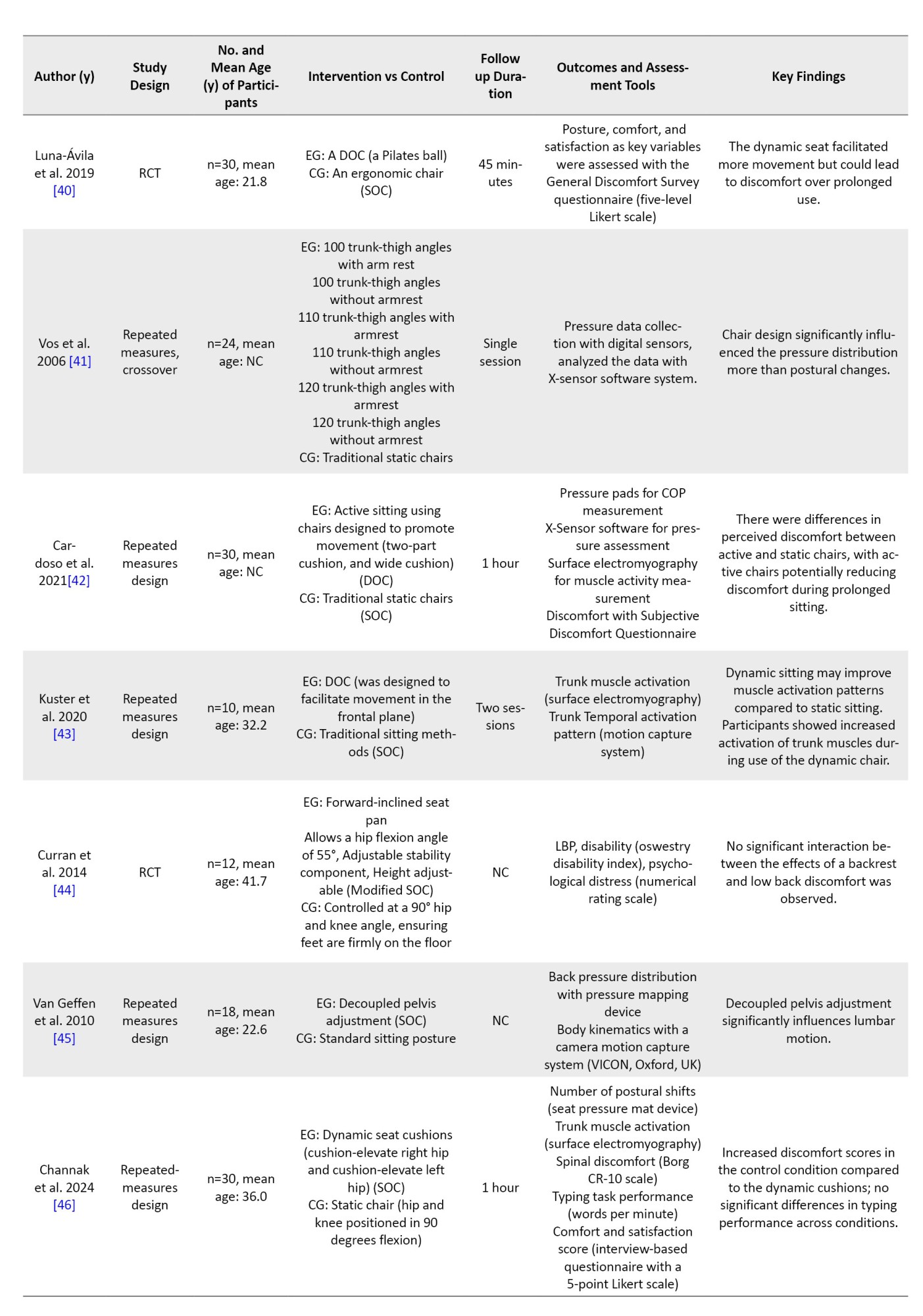
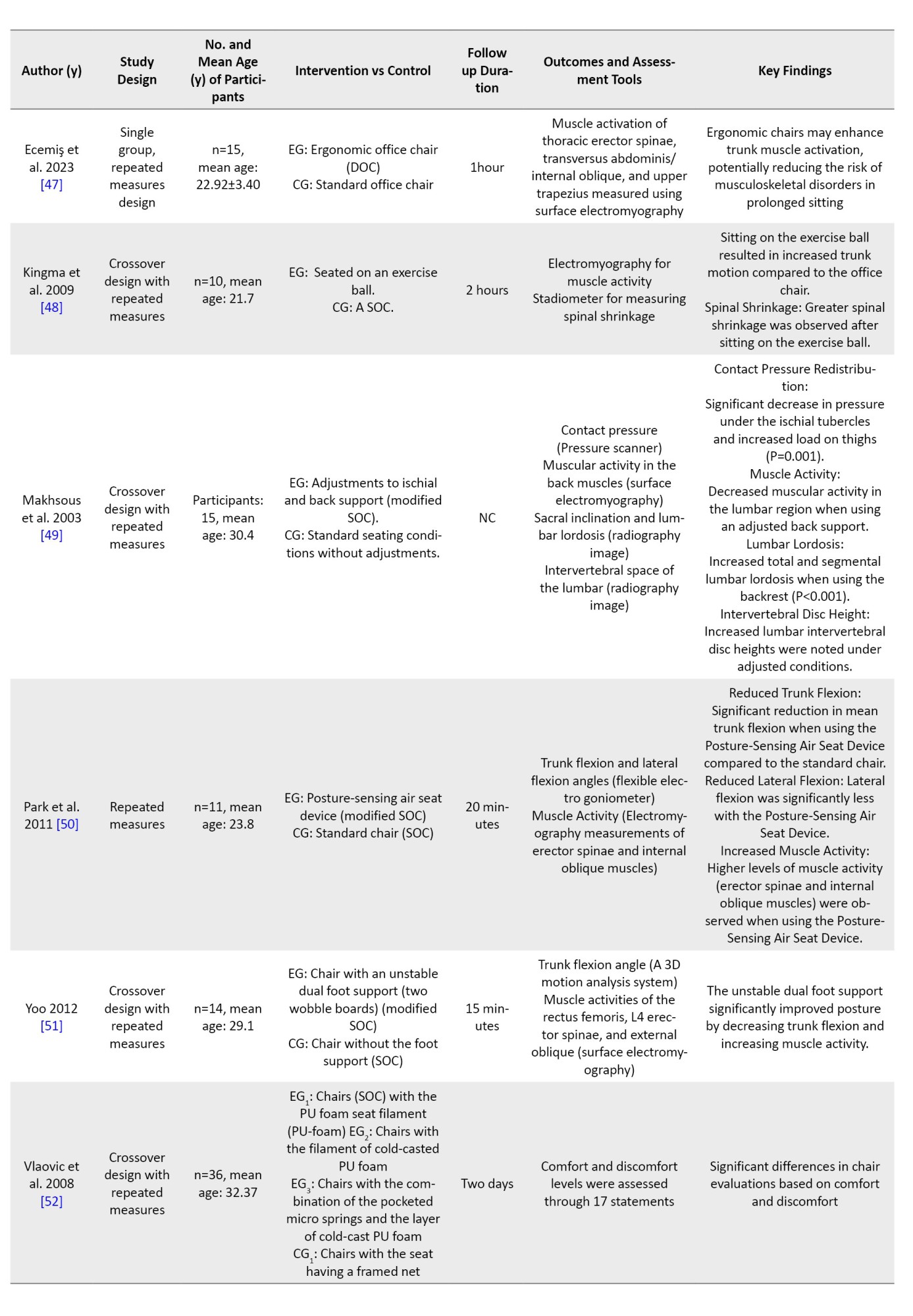
Table 3 summarizes the features of the 32 articles included in this review.
In the present analysis, office chairs were categorized into three types: 1) Standard office chair (SOC), defined as a conventional swivel chair with basic adjustability (e.g. seat height, backrest), used as a control or baseline condition in studies such as [9, 26, 27, 28, 31, 32, 40, 45, 46, 48, 50, 51, 52, 53]; 2) Modified SOC, a standard chair enhanced with specific ergonomic accessories (e.g. lumbar support, forearm supports, acupressure backrests, or posture-sensing systems), as implemented in [26-29, 32-34, 36, 37, 44, 46, 49-51, 55, 56]; and 3) dynamic office chair (DOC), characterized by movable seat pans and/or backrests that allow active sitting (e.g. saddle chairs, exercise balls, chairs with 3D-moving joints, or frontal-plane movement mechanisms), evaluated in [9, 30, 34, 35, 38-40, 42, 43, 47, 48]. Note that some studies employed multiple chair types across experimental conditions [9, 26, 27, 34, 40, 46, 48], and categorization was based on the specific intervention arm described. The total number of participants varied across studies, ranging from 6 to 277. In total, 1,637 participants had a mean age of 32.3±8.33 years.
Effect of ergonomic chair on clinical outcomes
Table 4 presents the GRADE assessment of articles related to the effectiveness of ergonomic chairs on clinical outcomes.
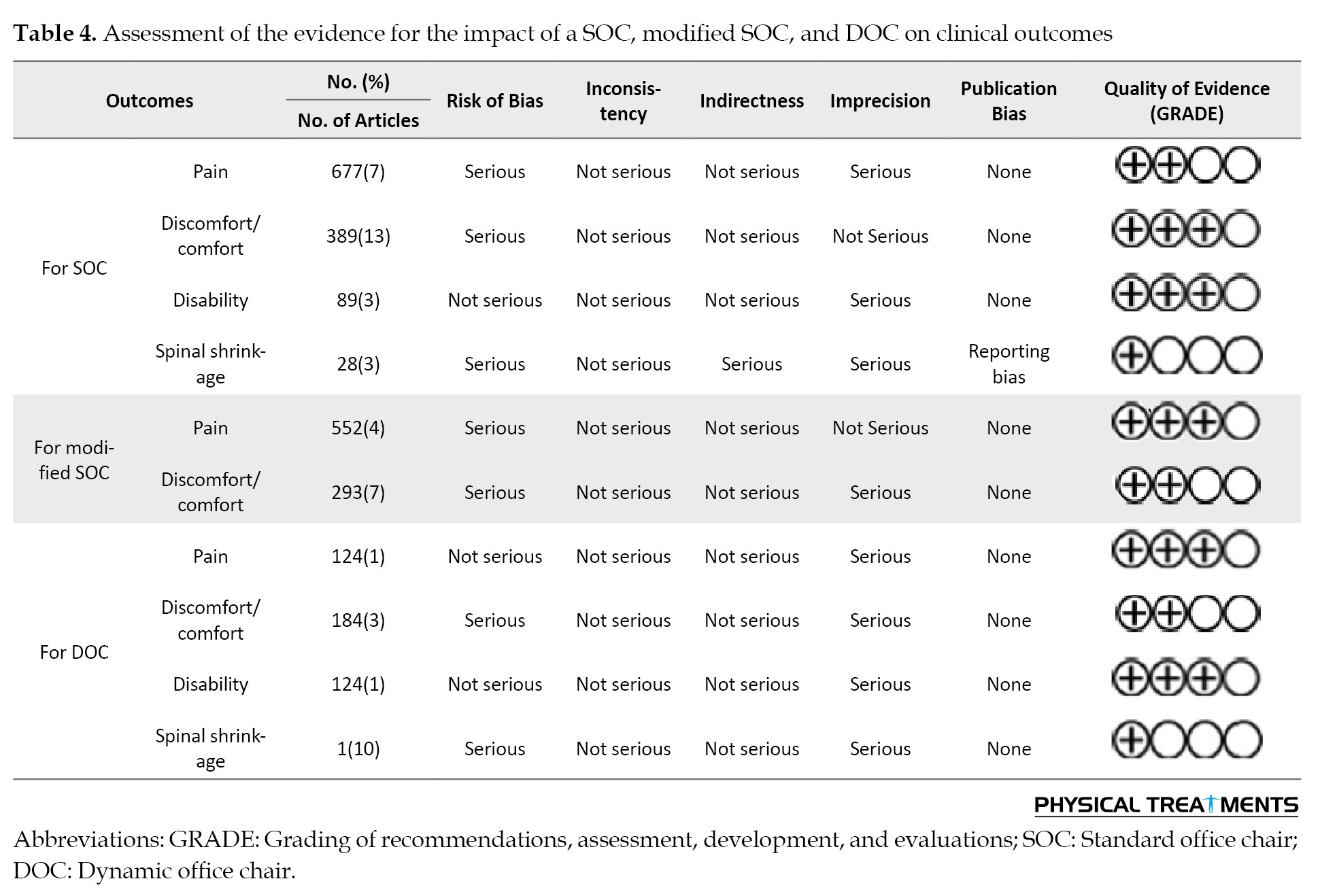
Effect of ergonomic chair on pain
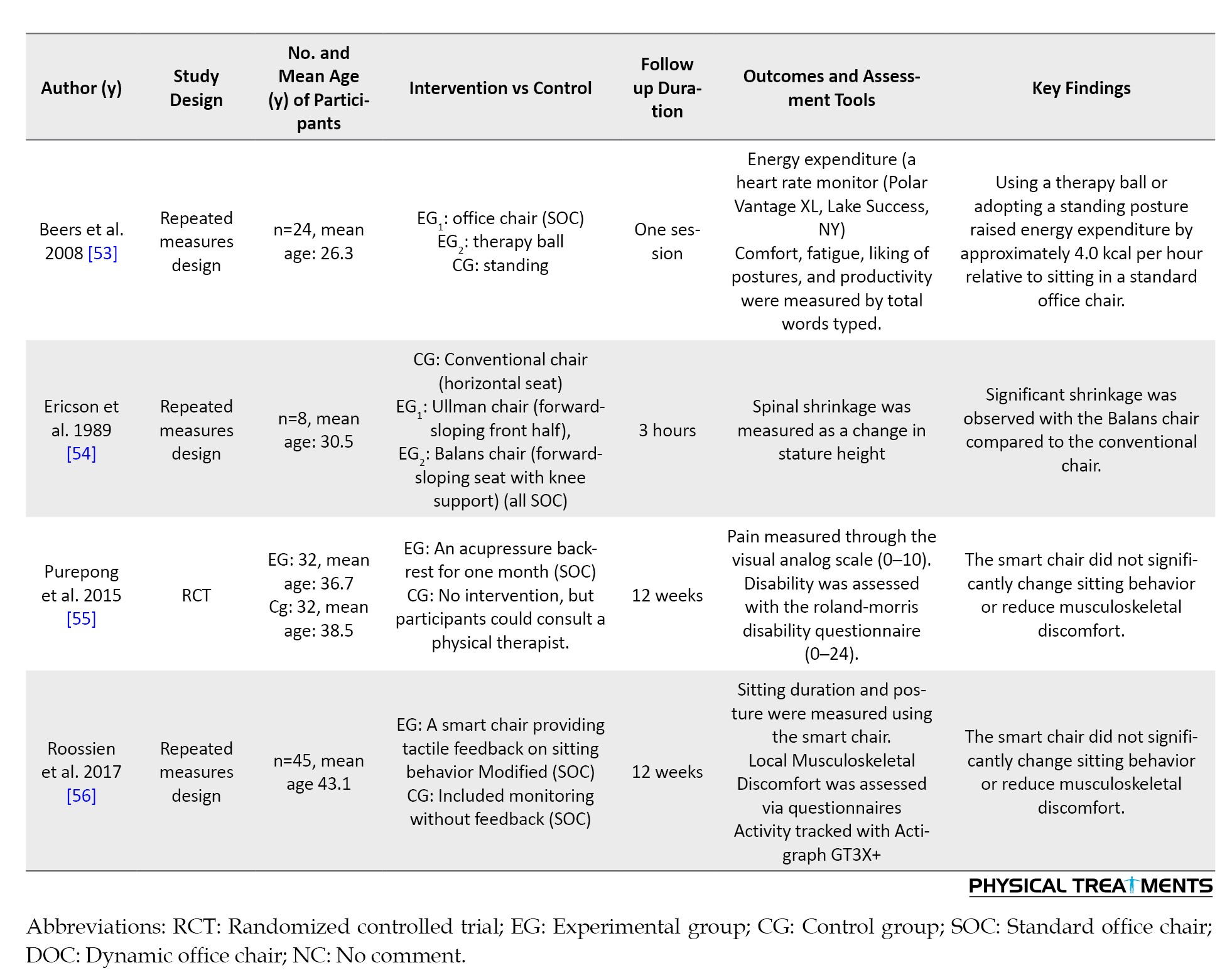
One study compared two ergonomic chair designs: Flat and curved. The flat chair was more effective at reducing pain, with a moderate improvement. People using it reported a noticeable drop in pain levels. The curved chair also helped reduce pain, but the improvement was smaller [26]. In a second study, when looking specifically at pain during activities, the flat chair had a very small effect; therefore, small that it may not have made a real difference. However, the curved chair in this case showed a moderate effect, suggesting it helped ease activity-related pain more than the flat chair [27]. A third study tested an acupressure backrest for one month, comparing it to no treatment. The results showed that this backrest had almost no effect on pain. The difference in pain levels between those who used it and those who did not was so small it likely would not be felt in real life [55].
Effect of ergonomic chair on comfort/discomfort
One study found that using an ergonomic chair did not have a significant impact on outcomes, as measured by the nordic musculoskeletal questionnaire [28]. However, the presence of forearm support in chairs significantly influenced musculoskeletal discomfort [29]. Comparing raising the right or left hip against a static chair with flexed hips and knees demonstrated a positive impact on comfort and satisfaction [46].
O’Keeffe et al. (2013) found that the use of a forward-inclined saddle chair was associated with a significant reduction in low back discomfort compared to SOC [39]. Furthermore, utilizing a dynamic seat, specifically a Pilates ball, significantly reduced scores on the General Discomfort Survey compared to a seat designed to ergonomic criteria [40]. Additionally, two-part cushions significantly reduced discomfort compared to static chairs, as measured by a discomfort-related questionnaire [42].
Effect of ergonomic chair on disability
Lengsfeld et al. (2007) investigated the impact of a chair with horizontal rotary movement compared to a standard chair. Their assessment included the Oswestry Disability Index, but the results did not demonstrate a significant effect [30]. Similarly, an acupressure backrest, as assessed using the roland-morris disability Questionnaire, also failed to show a significant effect [55]. Curran et al. (2014) studied a forward-inclined seat pan that allowed hip flexion, contrasting it with a controlled group maintained at a traditional 90-degree hip and knee angle. The Oswestry Disability Index results suggested a small, but potentially noteworthy, effect [44]. Finally, Roossien et al. assessed the efficacy of a smart chair against a no-intervention group, monitoring activity levels. Their findings, utilizing the Actigraph GT3X+, did not reveal a significant effect [56].
Effect of ergonomic chair on spinal shrinkage
Research indicates that dynamic chairs, particularly those allowing independent or fixed-ratio rotation of the backrest and seat, significantly reduce spinal shrinkage compared to traditional fixed chairs [9].
Effect of ergonomic chair on biomechanical outcomes
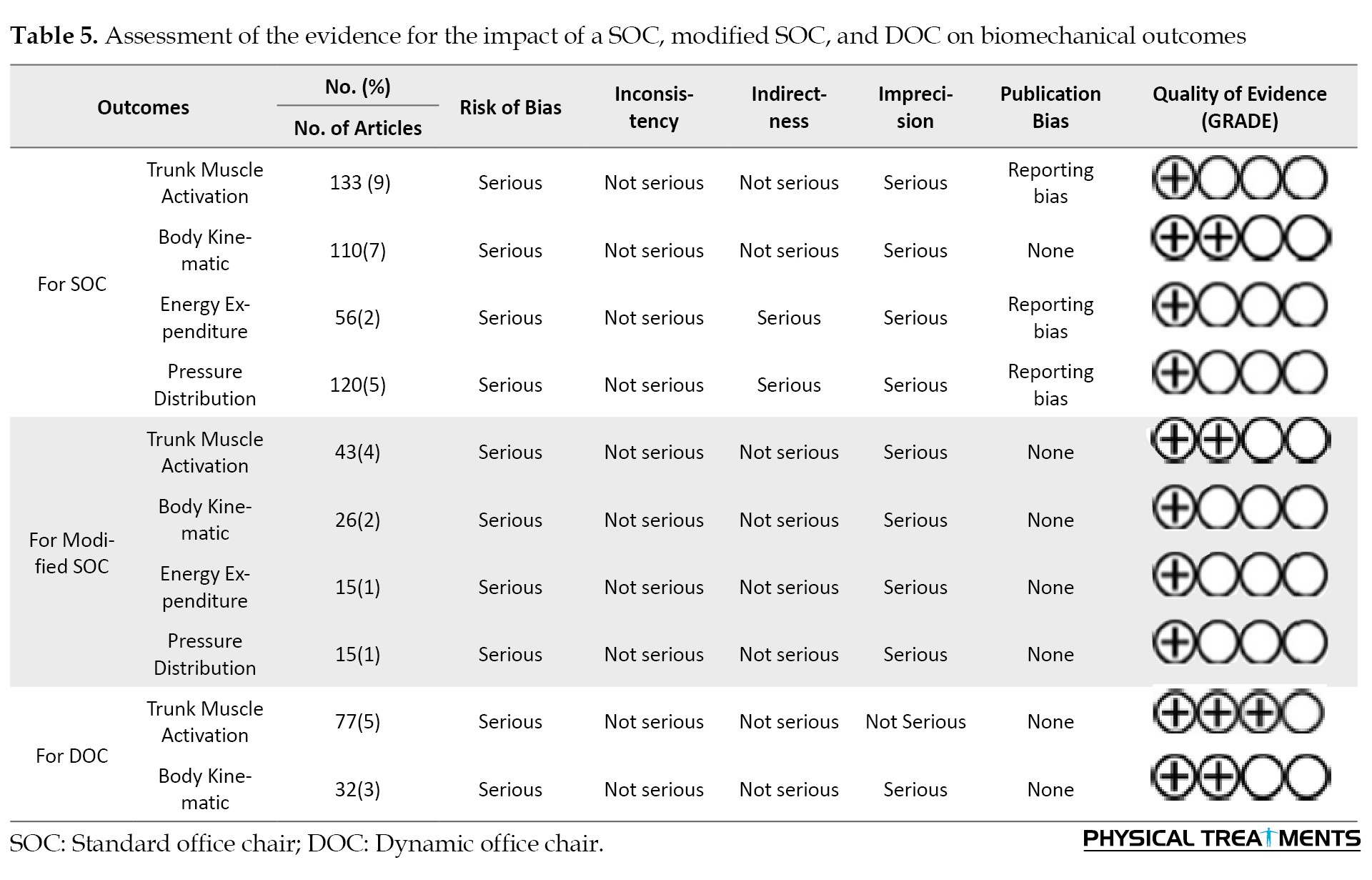
Table 4 presents the GRADE assessment of articles related to the effectiveness of ergonomic chairs on biomechanical outcomes.
Effect of ergonomic chair on muscle activation
One study comparing a dynamic chair with a three-dimensionally moving joint beneath the seat pan to a standard DOC showed no clear significant impact on trunk muscle activation [35]. Dalager et al. (2024) found that a custom-built ergonomic chair had a positive effect on left trapezius muscle activity compared to conventional office chairs [36]. Ecemiş et al. (2023) compared an ergonomic office chair to a SOC, noting positive effects on the transversus abdominis/internal oblique and the upper trapezius [47].
Kingma et al. reported that seated posture on an exercise ball resulted in greater lumbar muscle activation than a SOC [48]. Makhsous et al. (2003) found that adjustments to ischial and back support decreased muscular activity in the back muscles compared to standard seating conditions [49]. The posture-sensing air seat device showed a positive effect on muscle activity when compared to a standard chair [50]. A chair equipped with an unstable dual-foot support (wobble board) demonstrated a significant decrease in normalized electromyography (EMG) for the rectus femoris, lumbar multifidus, and external oblique muscles compared to a chair lacking foot support [51]. Finally, a DOC designed to promote movement in the frontal plane increased trunk muscle activity compared to traditional static chairs [43].
Effect of ergonomic chair on energy expenditure
One study indicated that using a forward-inclined saddle chair significantly increased energy expenditure compared to using a SOC [38]. However, a study by Beers et al. (2018) found that using a DOC resulted in lower energy expenditure compared to standing [53].
Effect of ergonomic chair on body kinematics
The findings across multiple studies indicate that ergonomic chair features have a significant positive impact on posture-related outcomes [33, 34, 37, 45, 49-51]. Adjustments, such as lumbar support, pelvis movement, posture-sensing systems, and unstable footrests, were consistently associated with improved spinal and joint alignment. Notably, the largest effects were observed with interventions targeting lumbar posture and head-neck alignment, such as lumbar roll support and the Back App chair [34, 45, 49-51]. These features not only enhance sitting posture but may also help prevent musculoskeletal strain associated with prolonged seated work [33].
Effect of ergonomic chair on pressure distribution
In one study, a trunk-thigh angle of 110 degrees resulted in a moderate positive effect size on pressure distribution compared to SOC [41]. Another study investigated modifications to the ischial and back support on a prototype chair, revealing a negative effect compared to unadjusted conditions [49].
Discussion
This review evaluated 32 studies examining the effects of chairs on clinical and biomechanical musculoskeletal outcomes in sedentary workers. The chair interventions were analyzed both generally and by chair type (specifically SOC, modified SOC, and DOC).
The studies showed significant heterogeneity in the population, intervention, comparison, outcomes, and follow-up time. Evidence on the effects of chairs on clinical and biomechanical outcomes, such as pain, discomfort/comfort, disability, spinal shrinkage, trunk muscle activation, body kinematics, energy expenditure, and pressure distribution, ranged from very low to moderate quality among sedentary workers. Additionally, these interventions showed effect sizes ranging from not significant to highly significant for the clinical and biomechanical outcomes. The findings from 1,637 participants highlight a complex interplay among chair designs and their impact on health-related measures.
Chair design and clinical outcomes
The results regarding pain reduction are conflicting, with some ergonomic chair designs demonstrating significant improvements, while findings are not consistently positive across all studies [26, 27] (SOC: Low-quality; modified SOC: Moderate quality; and DOC: Moderate quality [Table 4]). This variability may be attributed to differences in study design, participant demographics, and intervention durations. In contrast, the results regarding the effect of ergonomic chairs on comfort/discomfort are consistent and indicate positive outcomes [28, 29, 39, 40, 42, 46] (SOC: Moderate-quality; modified SOC: Low-quality; DOC: Low-quality [Table 4]). The intervention’s impact on disability was not significant [30, 44, 55, 56] (SOC: Moderate-quality; and DOC: moderate quality). Additionally, the intervention resulted in reduced spinal shrinkage [37, 48, 49, 54] (SOC: Very low quality; and DOC: Very low quality [Table 4]).
In a similar review, Van Niekerk et al. conducted a systematic review across various occupations and noted discomfort in several body regions. Various works encounter distinct working environments that affect employees’ well-being. However, the methodologies of the two studies differ, yet their results confirm each other [57].
When selecting a chair, both the seat height and seat pan depth must be adjusted to the user’s anthropometric dimensions [58]. When this is not matched correctly by the chair, the postural muscles’ ability to support it may be impaired, possibly leading to unusual stress on the neuromuscular system and discomfort [59].
Chair design and biomechanical outcomes
The use of ergonomic chairs has a significant impact on muscle activation [35, 36, 43, 47-51] (SOC: Very low, modified SOC: Low quality, and DOC: Very low quality [Table 5]), energy expenditure (SOC: Very low, modified SOC: very low quality, as indicated in Table 5), body kinematics (SOC: Low, modified SOC: Very low quality, and DOC: Low quality [Table 5]), and pressure distribution (SOC: Very low, modified SOC: Low quality [Table 5]). Dynamic chairs and custom-designed ergonomic systems demonstrate increased trunk stability and decreased muscle activation compared with conventional chairs.
More specifically, chair designs like forward-inclined saddle chairs increase energy expenditure [39, 54]. Adjustable features of the ergonomic chair are positively associated with joint posture [33, 34, 37, 45, 49-51].
The chair seat pans, designed with forward-tilting seats that relieve ischial pressure and combined with lumbar support, were associated with increased lumbar lordosis [49]. Some researchers recommended sustained neutral lumbar lordosis during sitting for LBP. Some studies attempted to modify an office chair to maintain neutral spinal alignment and prevent poor sitting posture [60, 61]. However, some studies found increased trunk muscle activation and greater comfort. Certain research indicates that fatigue onset aligns with a low level of trunk muscle activation, around 2–5%, maintained for as brief as 30 minutes in healthy individuals [62].
Methodological considerations, limitations, and recommendations for future research
A lack of robust methodology, especially regarding concealed allocation and blinding, is evident in these studies. The general characteristics were small sample sizes and/or short follow-up periods in the majority of these studies, making it difficult to generalize reliable findings. Investigations into the biomechanical and physiological mechanisms underlying how ergonomic chairs may affect pain and discomfort, and related health outcomes, are needed across more varied user groups and working settings to estimate wider generalizability and benefits.
Conclusion
The results regarding the effect of ergonomic chairs on pain reduction are mixed. While some chair designs indicated benefits, others did not yield uniformly positive results. By contrast, the effects of ergonomic chairs on comfort and discomfort are consistently positive. The interventions had no impact on disability, while evidence for a reduction in spinal shrinkage is of very low quality.
The use of dynamic chairs and individually designed ergonomic systems has been shown to increase trunk muscle activation when compared with conventional chairs. Forward-leaning saddle chairs increase energy expenditure, while adjustable features in ergonomic chairs improve joint posture.
Ethical Considerations
Compliance with ethical guidelines
The complete protocol for this systematic review is available on PROSPERO (registration code: CRD42024598129).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization, methodology and resources: Hicham Khabbache and Mahmood Bahramizadeh; Validation: Mahmood Bahramizadeh; Formal analysis: Mahmood Bahramizadeh, Hicham Khabbache, Kavita Batra, Majid Ansari and Morteza Faghih Jouibari; Investigation: Mahmood Bahramizadeh, Hicham Khabbache and Farhad Ghaffari; Data collection: Hanieh Khaliliyan; Writing the original draft: Hanieh Khaliliyan, Mahmood Bahramizadeh and Majid Ansari; Writing review and editing: Kavita Batra, Mahmood Bahramizadeh and Hanieh Khaliliyan; Supervision: Mahmood Bahramizadeh; Final approval: All authors.
Conflict of interest
The authors declared no conflicts of interest.
Full-Text: (45 Views)
Introduction
Work-related musculoskeletal disorders (WMSDs) encompass a range of inflammatory and degenerative conditions resulting from occupational activities [1]. The 12-month prevalence of WMSDs in the neck, back, and upper limbs is reported to be 55-69%, 31-54%, and 15-25%, respectively [2]. Nearly a million workers stop working every year owing to musculoskeletal pain and loss of function [3, 4].
Factors that have been associated with symptoms of WMSD, both modifiable and non-modifiable risks, include genetic predisposition and structural deformities of the spine. Modifiable factors include posture, task nature, work demands, and the physical characteristics of the job [5]. Offices are workplaces where employees spend much of their time working in a seated position. With more than 45 million computers in the United States alone in the 1990s, concern about WMSDs grew [6]. Over 72% of the employees work in a sitting posture in Western countries [7]. It has been established that prolonged sitting in suboptimal posture is associated with WMSDs [5, 8].
Sedentary work may contribute to WMSDs of the spine, likely due to prolonged periods of low static activity in the trunk muscles. For instance, patients with low back pain (LBP) have been reported to exhibit atrophy of the lumbar multifidus and trunk muscles, which are inactive for approximately 30% of sitting time [9-11]. Additionally, patients with LBP often show a reduction in spinal range of motion, similar to other spinal conditions, such as spinal stenosis, disc prolapse, and degenerative disc disease [12].
The adjustments in the workplace typically focus on the work surface and the chair [13]. Since the chair directly affects body posture, patients experiencing WMSD symptoms from prolonged sitting are advised to adjust their chairs to use ergonomic features. Often, due to environmental constraints, changing the work surface is not feasible, and an adjustable work surface may not be economically viable [5, 13, 14]. Therefore, adjusting the chair is often the most accessible step to reduce the likelihood of WMSDs.
Active movements of the intervertebral discs and spinal muscles are superior to maintaining a single static posture [15, 16]. Continuous postural changes lead to variations in the activity of the posterior muscles, spinal loading, and trunk-thigh angle [17, 18]. These factors are essential for preventing sitting-related LBP, degenerative disc disease, and muscular dysfunction. A total of 24-39% of individuals with LBP report that walking alleviates their LBP [19, 20]. Therefore, dynamic movements between different sections of a chair should also be considered a potential ergonomic feature.
Although laboratory studies have been conducted on the impact of chair features, such as seat pan depth, lumbar and full back support, adjustable seat height, and lower arm support, on musculoskeletal symptoms in the back as well as the upper and lower extremities, no systematic review has evaluated the effects of these interventions on clinical and biomechanical outcomes. This study aimed to review the effects of ergonomic chairs on the clinical and biomechanical outcomes of individuals who work in a seated posture.
Materials and Methods
Search strategy
Two reviewers (Hanieh Khaliliyan and Mahmood Bahramizadeh) independently conducted parallel searches in three electronic databases, including PubMed, Scopus, and Web of Science on 29 October 2024, using the queries outlined in Table 1.
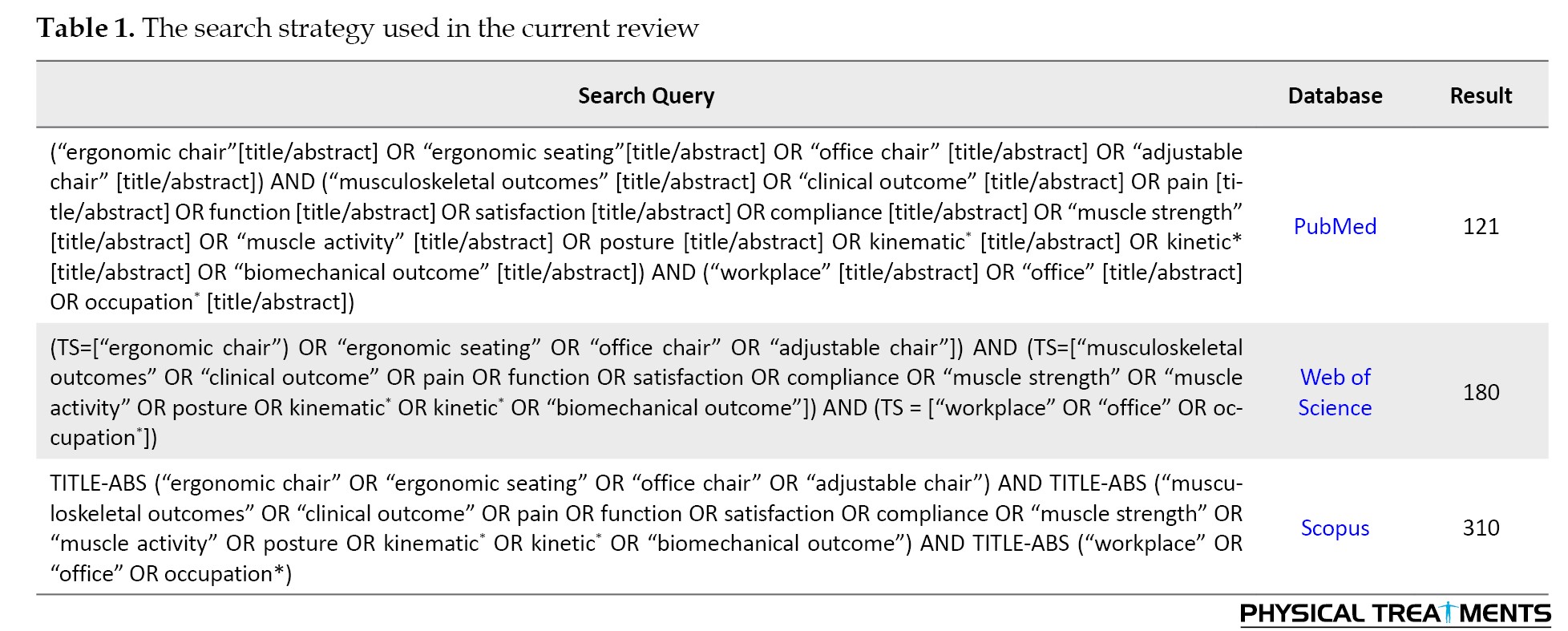
These queries were constructed by the principal author (Mahmood Bahramizadeh) based on population, intervention, comparison, and outcome (PICO) items [21], with synonyms obtained from the MeSH database.
Study selection
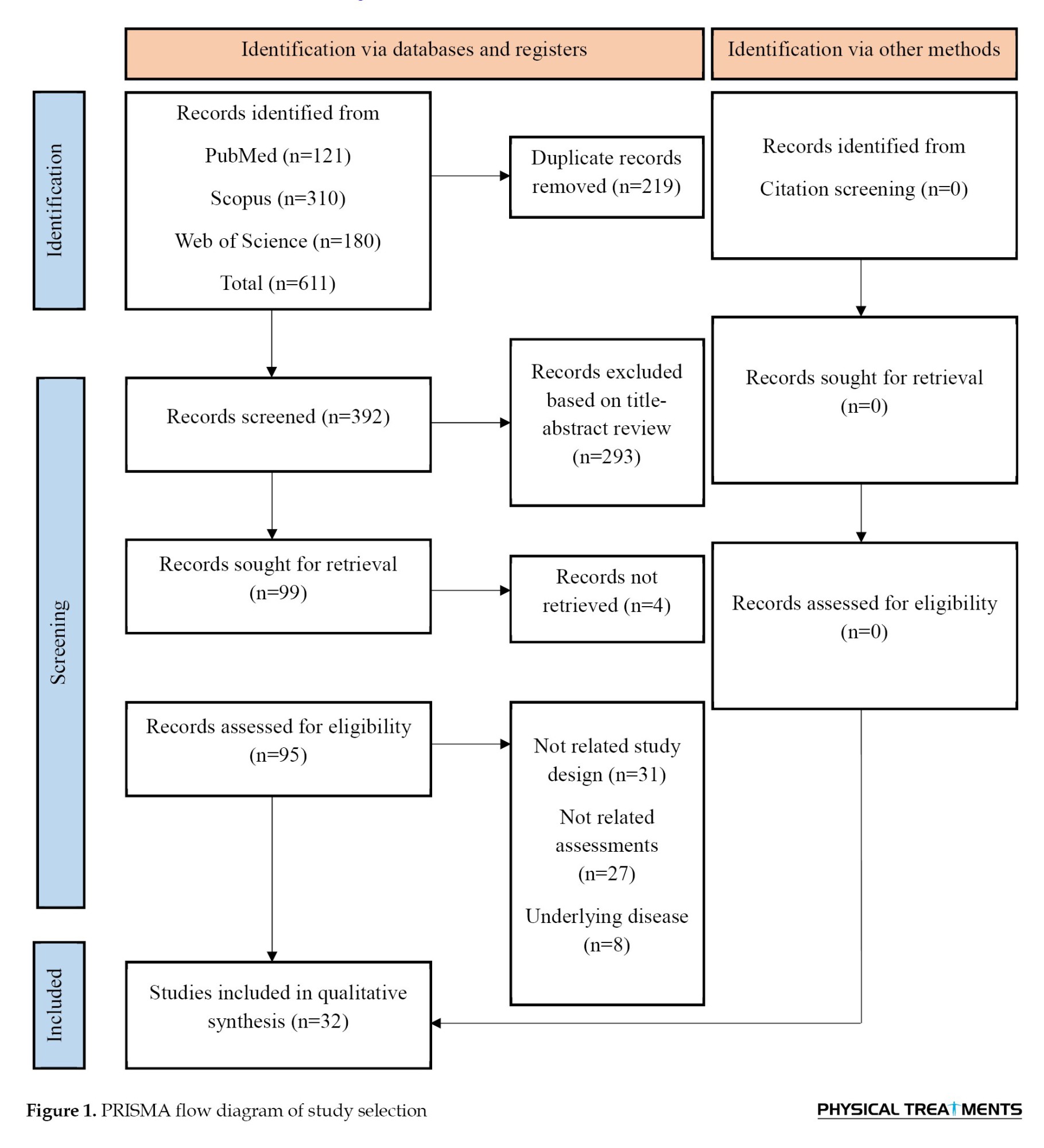
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were followed for the study selection process [22]. After removing duplicate records, the remaining articles were screened according to the predefined eligibility criteria based on the PICOS framework. The study population (P) included individuals engaged in predominantly sedentary work performed in a sitting position. The intervention (I) consisted of chairs incorporating ergonomic design modifications. Comparisons (C) were made between the intervention group and either a control group or pre-intervention conditions. Outcomes (O) included all reported biomechanical and clinical measures. The study design (S) was restricted to randomized controlled trials (RCTs). In addition, only peer-reviewed articles published in English were considered eligible for inclusion.
The titles and abstracts of the articles were assessed against the inclusion criteria, followed by a second assessment of the full texts using the same criteria. The selection process was conducted independently by two reviewers, Hanieh Khaliliyan and Mahmood Bahramizadeh with any conflicts resolved through discussion.
Methodological quality assessment
The 11-item criteria recommended by the physiotherapy evidence database (PEDro) score were used for quality assessment. Each item was rated as Yes or No and received a score of 1, except for the eligibility criteria. In this method, final quality was determined based on the total score (1-4: Poor, 5-6: Fair, 7-8: Good, and 9-10: excellent) [23]. Two reviewers (Hanieh Khaliliyan and Mahmood Bahramizadeh) performed this step; any conflicts were resolved with input from another reviewer (Majid Ansari).
Data extraction
We extracted the data in the form of standard Excel files (Microsoft Excel, software, version 2019, USA). The data items were author, year, study design, participant demographics, intervention, follow-up duration, outcomes, assessment tool, and key findings. Three reviewers (Hanieh Khaliliyan, Mahmood Bahramizadeh, and Francesco Chirico) double-checked the data entry; another author (kavita batra) checked the data, and in the case of inconsistency, she made the final decision.
Data analysis
The grading of recommendations, assessment, development, and evaluations (GRADE) system was used to assess the certainty of the evidence. The study limitations were downgraded when more than 25% of the samples were obtained using low-quality methods, as assessed by the PEDro score. Inconsistency was downgraded if effects were in opposing directions, while indirectness was downgraded if the participants, interventions, outcomes, or comparisons of the study did not align with the objectives of this review. Imprecision was downgraded when the sample size was below 400 or if only one study was included. Publication bias was downgraded when the proportion of significant studies displayed asymmetry [24]. A narrative analysis was performed since data pooling was unfeasible, as there were fewer than three studies with consistent methodologies for each outcome.
Results
Study selection
An automated search of the PubMed, Scopus, and Web of Science databases yielded 611 references. After removing duplicate entries and conducting an initial screening, 32 studies met our inclusion criteria (Figure 1).
Work-related musculoskeletal disorders (WMSDs) encompass a range of inflammatory and degenerative conditions resulting from occupational activities [1]. The 12-month prevalence of WMSDs in the neck, back, and upper limbs is reported to be 55-69%, 31-54%, and 15-25%, respectively [2]. Nearly a million workers stop working every year owing to musculoskeletal pain and loss of function [3, 4].
Factors that have been associated with symptoms of WMSD, both modifiable and non-modifiable risks, include genetic predisposition and structural deformities of the spine. Modifiable factors include posture, task nature, work demands, and the physical characteristics of the job [5]. Offices are workplaces where employees spend much of their time working in a seated position. With more than 45 million computers in the United States alone in the 1990s, concern about WMSDs grew [6]. Over 72% of the employees work in a sitting posture in Western countries [7]. It has been established that prolonged sitting in suboptimal posture is associated with WMSDs [5, 8].
Sedentary work may contribute to WMSDs of the spine, likely due to prolonged periods of low static activity in the trunk muscles. For instance, patients with low back pain (LBP) have been reported to exhibit atrophy of the lumbar multifidus and trunk muscles, which are inactive for approximately 30% of sitting time [9-11]. Additionally, patients with LBP often show a reduction in spinal range of motion, similar to other spinal conditions, such as spinal stenosis, disc prolapse, and degenerative disc disease [12].
The adjustments in the workplace typically focus on the work surface and the chair [13]. Since the chair directly affects body posture, patients experiencing WMSD symptoms from prolonged sitting are advised to adjust their chairs to use ergonomic features. Often, due to environmental constraints, changing the work surface is not feasible, and an adjustable work surface may not be economically viable [5, 13, 14]. Therefore, adjusting the chair is often the most accessible step to reduce the likelihood of WMSDs.
Active movements of the intervertebral discs and spinal muscles are superior to maintaining a single static posture [15, 16]. Continuous postural changes lead to variations in the activity of the posterior muscles, spinal loading, and trunk-thigh angle [17, 18]. These factors are essential for preventing sitting-related LBP, degenerative disc disease, and muscular dysfunction. A total of 24-39% of individuals with LBP report that walking alleviates their LBP [19, 20]. Therefore, dynamic movements between different sections of a chair should also be considered a potential ergonomic feature.
Although laboratory studies have been conducted on the impact of chair features, such as seat pan depth, lumbar and full back support, adjustable seat height, and lower arm support, on musculoskeletal symptoms in the back as well as the upper and lower extremities, no systematic review has evaluated the effects of these interventions on clinical and biomechanical outcomes. This study aimed to review the effects of ergonomic chairs on the clinical and biomechanical outcomes of individuals who work in a seated posture.
Materials and Methods
Search strategy
Two reviewers (Hanieh Khaliliyan and Mahmood Bahramizadeh) independently conducted parallel searches in three electronic databases, including PubMed, Scopus, and Web of Science on 29 October 2024, using the queries outlined in Table 1.
These queries were constructed by the principal author (Mahmood Bahramizadeh) based on population, intervention, comparison, and outcome (PICO) items [21], with synonyms obtained from the MeSH database.
Study selection
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were followed for the study selection process [22]. After removing duplicate records, the remaining articles were screened according to the predefined eligibility criteria based on the PICOS framework. The study population (P) included individuals engaged in predominantly sedentary work performed in a sitting position. The intervention (I) consisted of chairs incorporating ergonomic design modifications. Comparisons (C) were made between the intervention group and either a control group or pre-intervention conditions. Outcomes (O) included all reported biomechanical and clinical measures. The study design (S) was restricted to randomized controlled trials (RCTs). In addition, only peer-reviewed articles published in English were considered eligible for inclusion.
The titles and abstracts of the articles were assessed against the inclusion criteria, followed by a second assessment of the full texts using the same criteria. The selection process was conducted independently by two reviewers, Hanieh Khaliliyan and Mahmood Bahramizadeh with any conflicts resolved through discussion.
Methodological quality assessment
The 11-item criteria recommended by the physiotherapy evidence database (PEDro) score were used for quality assessment. Each item was rated as Yes or No and received a score of 1, except for the eligibility criteria. In this method, final quality was determined based on the total score (1-4: Poor, 5-6: Fair, 7-8: Good, and 9-10: excellent) [23]. Two reviewers (Hanieh Khaliliyan and Mahmood Bahramizadeh) performed this step; any conflicts were resolved with input from another reviewer (Majid Ansari).
Data extraction
We extracted the data in the form of standard Excel files (Microsoft Excel, software, version 2019, USA). The data items were author, year, study design, participant demographics, intervention, follow-up duration, outcomes, assessment tool, and key findings. Three reviewers (Hanieh Khaliliyan, Mahmood Bahramizadeh, and Francesco Chirico) double-checked the data entry; another author (kavita batra) checked the data, and in the case of inconsistency, she made the final decision.
Data analysis
The grading of recommendations, assessment, development, and evaluations (GRADE) system was used to assess the certainty of the evidence. The study limitations were downgraded when more than 25% of the samples were obtained using low-quality methods, as assessed by the PEDro score. Inconsistency was downgraded if effects were in opposing directions, while indirectness was downgraded if the participants, interventions, outcomes, or comparisons of the study did not align with the objectives of this review. Imprecision was downgraded when the sample size was below 400 or if only one study was included. Publication bias was downgraded when the proportion of significant studies displayed asymmetry [24]. A narrative analysis was performed since data pooling was unfeasible, as there were fewer than three studies with consistent methodologies for each outcome.
Results
Study selection
An automated search of the PubMed, Scopus, and Web of Science databases yielded 611 references. After removing duplicate entries and conducting an initial screening, 32 studies met our inclusion criteria (Figure 1).
Methodological quality assessment
Prior to discussion, reviewers Hanieh Khaliliyan and Mahmood Bahramizadeh demonstrated an agreement rate of 89% (314 out of 352) on the PEDro scores. The overall inter-rater reliability yielded a kappa coefficient of 0.79 with a standard error of 0.05. After resolving discrepancies through discussion, the reviewers reached complete consensus, achieving 100% agreement (352 out of 352). For this sample of 32 studies, the scores ranged from a minimum score of 1 to a maximum score of 10, with a general mean score of approximately 5. This mean indicates the overall quality level within the fair category, reflecting a moderate quality of evidence across the reviewed studies. The distribution of the quality levels further breaks down as follows: Three articles rated as excellent [30, 34, 50], representing 9.37%; 3 rated as good [26, 36, 44], which is 9.37%; and 19 articles rated as poor [9, 28, 31-33, 35, 38, 40, 41, 46-48, 50-56], making up 59.37%. Furthermore, 7 articles were rated fair [27, 29, 38, 40, 43, 44, 46], accounting for 21.87% of the total. Table 2 presents the methodological quality assessment.
Study characteristics
Table 3 summarizes the features of the 32 articles included in this review.
In the present analysis, office chairs were categorized into three types: 1) Standard office chair (SOC), defined as a conventional swivel chair with basic adjustability (e.g. seat height, backrest), used as a control or baseline condition in studies such as [9, 26, 27, 28, 31, 32, 40, 45, 46, 48, 50, 51, 52, 53]; 2) Modified SOC, a standard chair enhanced with specific ergonomic accessories (e.g. lumbar support, forearm supports, acupressure backrests, or posture-sensing systems), as implemented in [26-29, 32-34, 36, 37, 44, 46, 49-51, 55, 56]; and 3) dynamic office chair (DOC), characterized by movable seat pans and/or backrests that allow active sitting (e.g. saddle chairs, exercise balls, chairs with 3D-moving joints, or frontal-plane movement mechanisms), evaluated in [9, 30, 34, 35, 38-40, 42, 43, 47, 48]. Note that some studies employed multiple chair types across experimental conditions [9, 26, 27, 34, 40, 46, 48], and categorization was based on the specific intervention arm described. The total number of participants varied across studies, ranging from 6 to 277. In total, 1,637 participants had a mean age of 32.3±8.33 years.
Effect of ergonomic chair on clinical outcomes
Table 4 presents the GRADE assessment of articles related to the effectiveness of ergonomic chairs on clinical outcomes.
Effect of ergonomic chair on pain
One study compared two ergonomic chair designs: Flat and curved. The flat chair was more effective at reducing pain, with a moderate improvement. People using it reported a noticeable drop in pain levels. The curved chair also helped reduce pain, but the improvement was smaller [26]. In a second study, when looking specifically at pain during activities, the flat chair had a very small effect; therefore, small that it may not have made a real difference. However, the curved chair in this case showed a moderate effect, suggesting it helped ease activity-related pain more than the flat chair [27]. A third study tested an acupressure backrest for one month, comparing it to no treatment. The results showed that this backrest had almost no effect on pain. The difference in pain levels between those who used it and those who did not was so small it likely would not be felt in real life [55].
Effect of ergonomic chair on comfort/discomfort
One study found that using an ergonomic chair did not have a significant impact on outcomes, as measured by the nordic musculoskeletal questionnaire [28]. However, the presence of forearm support in chairs significantly influenced musculoskeletal discomfort [29]. Comparing raising the right or left hip against a static chair with flexed hips and knees demonstrated a positive impact on comfort and satisfaction [46].
O’Keeffe et al. (2013) found that the use of a forward-inclined saddle chair was associated with a significant reduction in low back discomfort compared to SOC [39]. Furthermore, utilizing a dynamic seat, specifically a Pilates ball, significantly reduced scores on the General Discomfort Survey compared to a seat designed to ergonomic criteria [40]. Additionally, two-part cushions significantly reduced discomfort compared to static chairs, as measured by a discomfort-related questionnaire [42].
Effect of ergonomic chair on disability
Lengsfeld et al. (2007) investigated the impact of a chair with horizontal rotary movement compared to a standard chair. Their assessment included the Oswestry Disability Index, but the results did not demonstrate a significant effect [30]. Similarly, an acupressure backrest, as assessed using the roland-morris disability Questionnaire, also failed to show a significant effect [55]. Curran et al. (2014) studied a forward-inclined seat pan that allowed hip flexion, contrasting it with a controlled group maintained at a traditional 90-degree hip and knee angle. The Oswestry Disability Index results suggested a small, but potentially noteworthy, effect [44]. Finally, Roossien et al. assessed the efficacy of a smart chair against a no-intervention group, monitoring activity levels. Their findings, utilizing the Actigraph GT3X+, did not reveal a significant effect [56].
Effect of ergonomic chair on spinal shrinkage
Research indicates that dynamic chairs, particularly those allowing independent or fixed-ratio rotation of the backrest and seat, significantly reduce spinal shrinkage compared to traditional fixed chairs [9].
Effect of ergonomic chair on biomechanical outcomes
Table 4 presents the GRADE assessment of articles related to the effectiveness of ergonomic chairs on biomechanical outcomes.
Effect of ergonomic chair on muscle activation
One study comparing a dynamic chair with a three-dimensionally moving joint beneath the seat pan to a standard DOC showed no clear significant impact on trunk muscle activation [35]. Dalager et al. (2024) found that a custom-built ergonomic chair had a positive effect on left trapezius muscle activity compared to conventional office chairs [36]. Ecemiş et al. (2023) compared an ergonomic office chair to a SOC, noting positive effects on the transversus abdominis/internal oblique and the upper trapezius [47].
Kingma et al. reported that seated posture on an exercise ball resulted in greater lumbar muscle activation than a SOC [48]. Makhsous et al. (2003) found that adjustments to ischial and back support decreased muscular activity in the back muscles compared to standard seating conditions [49]. The posture-sensing air seat device showed a positive effect on muscle activity when compared to a standard chair [50]. A chair equipped with an unstable dual-foot support (wobble board) demonstrated a significant decrease in normalized electromyography (EMG) for the rectus femoris, lumbar multifidus, and external oblique muscles compared to a chair lacking foot support [51]. Finally, a DOC designed to promote movement in the frontal plane increased trunk muscle activity compared to traditional static chairs [43].
Effect of ergonomic chair on energy expenditure
One study indicated that using a forward-inclined saddle chair significantly increased energy expenditure compared to using a SOC [38]. However, a study by Beers et al. (2018) found that using a DOC resulted in lower energy expenditure compared to standing [53].
Effect of ergonomic chair on body kinematics
The findings across multiple studies indicate that ergonomic chair features have a significant positive impact on posture-related outcomes [33, 34, 37, 45, 49-51]. Adjustments, such as lumbar support, pelvis movement, posture-sensing systems, and unstable footrests, were consistently associated with improved spinal and joint alignment. Notably, the largest effects were observed with interventions targeting lumbar posture and head-neck alignment, such as lumbar roll support and the Back App chair [34, 45, 49-51]. These features not only enhance sitting posture but may also help prevent musculoskeletal strain associated with prolonged seated work [33].
Effect of ergonomic chair on pressure distribution
In one study, a trunk-thigh angle of 110 degrees resulted in a moderate positive effect size on pressure distribution compared to SOC [41]. Another study investigated modifications to the ischial and back support on a prototype chair, revealing a negative effect compared to unadjusted conditions [49].
Discussion
This review evaluated 32 studies examining the effects of chairs on clinical and biomechanical musculoskeletal outcomes in sedentary workers. The chair interventions were analyzed both generally and by chair type (specifically SOC, modified SOC, and DOC).
The studies showed significant heterogeneity in the population, intervention, comparison, outcomes, and follow-up time. Evidence on the effects of chairs on clinical and biomechanical outcomes, such as pain, discomfort/comfort, disability, spinal shrinkage, trunk muscle activation, body kinematics, energy expenditure, and pressure distribution, ranged from very low to moderate quality among sedentary workers. Additionally, these interventions showed effect sizes ranging from not significant to highly significant for the clinical and biomechanical outcomes. The findings from 1,637 participants highlight a complex interplay among chair designs and their impact on health-related measures.
Chair design and clinical outcomes
The results regarding pain reduction are conflicting, with some ergonomic chair designs demonstrating significant improvements, while findings are not consistently positive across all studies [26, 27] (SOC: Low-quality; modified SOC: Moderate quality; and DOC: Moderate quality [Table 4]). This variability may be attributed to differences in study design, participant demographics, and intervention durations. In contrast, the results regarding the effect of ergonomic chairs on comfort/discomfort are consistent and indicate positive outcomes [28, 29, 39, 40, 42, 46] (SOC: Moderate-quality; modified SOC: Low-quality; DOC: Low-quality [Table 4]). The intervention’s impact on disability was not significant [30, 44, 55, 56] (SOC: Moderate-quality; and DOC: moderate quality). Additionally, the intervention resulted in reduced spinal shrinkage [37, 48, 49, 54] (SOC: Very low quality; and DOC: Very low quality [Table 4]).
In a similar review, Van Niekerk et al. conducted a systematic review across various occupations and noted discomfort in several body regions. Various works encounter distinct working environments that affect employees’ well-being. However, the methodologies of the two studies differ, yet their results confirm each other [57].
When selecting a chair, both the seat height and seat pan depth must be adjusted to the user’s anthropometric dimensions [58]. When this is not matched correctly by the chair, the postural muscles’ ability to support it may be impaired, possibly leading to unusual stress on the neuromuscular system and discomfort [59].
Chair design and biomechanical outcomes
The use of ergonomic chairs has a significant impact on muscle activation [35, 36, 43, 47-51] (SOC: Very low, modified SOC: Low quality, and DOC: Very low quality [Table 5]), energy expenditure (SOC: Very low, modified SOC: very low quality, as indicated in Table 5), body kinematics (SOC: Low, modified SOC: Very low quality, and DOC: Low quality [Table 5]), and pressure distribution (SOC: Very low, modified SOC: Low quality [Table 5]). Dynamic chairs and custom-designed ergonomic systems demonstrate increased trunk stability and decreased muscle activation compared with conventional chairs.
More specifically, chair designs like forward-inclined saddle chairs increase energy expenditure [39, 54]. Adjustable features of the ergonomic chair are positively associated with joint posture [33, 34, 37, 45, 49-51].
The chair seat pans, designed with forward-tilting seats that relieve ischial pressure and combined with lumbar support, were associated with increased lumbar lordosis [49]. Some researchers recommended sustained neutral lumbar lordosis during sitting for LBP. Some studies attempted to modify an office chair to maintain neutral spinal alignment and prevent poor sitting posture [60, 61]. However, some studies found increased trunk muscle activation and greater comfort. Certain research indicates that fatigue onset aligns with a low level of trunk muscle activation, around 2–5%, maintained for as brief as 30 minutes in healthy individuals [62].
Methodological considerations, limitations, and recommendations for future research
A lack of robust methodology, especially regarding concealed allocation and blinding, is evident in these studies. The general characteristics were small sample sizes and/or short follow-up periods in the majority of these studies, making it difficult to generalize reliable findings. Investigations into the biomechanical and physiological mechanisms underlying how ergonomic chairs may affect pain and discomfort, and related health outcomes, are needed across more varied user groups and working settings to estimate wider generalizability and benefits.
Conclusion
The results regarding the effect of ergonomic chairs on pain reduction are mixed. While some chair designs indicated benefits, others did not yield uniformly positive results. By contrast, the effects of ergonomic chairs on comfort and discomfort are consistently positive. The interventions had no impact on disability, while evidence for a reduction in spinal shrinkage is of very low quality.
The use of dynamic chairs and individually designed ergonomic systems has been shown to increase trunk muscle activation when compared with conventional chairs. Forward-leaning saddle chairs increase energy expenditure, while adjustable features in ergonomic chairs improve joint posture.
Ethical Considerations
Compliance with ethical guidelines
The complete protocol for this systematic review is available on PROSPERO (registration code: CRD42024598129).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization, methodology and resources: Hicham Khabbache and Mahmood Bahramizadeh; Validation: Mahmood Bahramizadeh; Formal analysis: Mahmood Bahramizadeh, Hicham Khabbache, Kavita Batra, Majid Ansari and Morteza Faghih Jouibari; Investigation: Mahmood Bahramizadeh, Hicham Khabbache and Farhad Ghaffari; Data collection: Hanieh Khaliliyan; Writing the original draft: Hanieh Khaliliyan, Mahmood Bahramizadeh and Majid Ansari; Writing review and editing: Kavita Batra, Mahmood Bahramizadeh and Hanieh Khaliliyan; Supervision: Mahmood Bahramizadeh; Final approval: All authors.
Conflict of interest
The authors declared no conflicts of interest.
References
- Kaka B, Idowu OA, Fawole HO, Adeniyi AF, Ogwumike OO, Toryila MT. An analysis of work-related musculoskeletal disorders among butchers in kano metropolis, Nigeria.Safety and Health at Work. 2016; 7:218-24 [DOI:10.1016/j.shaw.2016.01.001] [PMID]
- Wærsted M, Hanvold TN, Veiersted KB. Computer work and musculoskeletal disorders of the neck and upper extremity: A systematic review. BMC Musculoskeletal Disorders. 2010; 11(79):1-15. [DOI:10.1186/1471-2474-11-79] [PMID]
- Almusawi A AH, Al-Hindy H AM. Exploring back pain characteristics: Insights from Hilla, Iraq. Iranian Rehabilitation Journal. 2024; 22(4):605-14. [DOI:10.32598/irj.22.4.1619.7]
- Acquadro Maran D, Varetto A, Begotti T, Rizzo A, Yıldırım M, Batra K, et al. Consequences and coping strategies among students and workers experiencing stalking. Iranian Rehabilitation Journal. 2025; 23(2):217-32. [DOI:10.32598/irj.23.2.2288.3]
- Ali DA, Oukhouya K, Aziz A, Bouhali H, El Khiat A, El Koutbi M, et al. Prevalence of musculoskeletal disorders among healthcare professionals: A hospital-based study. Advances in Medicine, Psychology, and Public Health. 2024; 1(1):12-25. [Link]
- Tittiranonda P, Rempel D, Armstrong T, Burastero S. Effect of four computer keyboards in computer users with upper extremity musculoskeletal disorders. American Journal of Industrial Medicine. 1999; 35(6):647-61. [DOI:10.1002/(SICI)1097-0274(199906)35:63.0.CO;2-5]
- Shahbazi A, Mokhtarinia HR, Biglarian A, Gabel CP. The prevalence of musculoskeletal symptoms in iranian spinner workers in the textile industry and its association with demographic and lifestyle characteristics. Iranian Rehabilitation Journal. 2020; 18(4):395-404. [DOI:10.32598/irj.18.4.919.2]
- Ziaeefar P, Hatami H, Panahi D, Poursadeghiyan M, Salehi Sahlabadi A. Neck pain severity and work ability index: A study of Tehran dental students. Iranian Rehabilitation Journal. 2024; 22(2):265-76. [DOI:10.32598/irj.22.2.2004.2]
- van Diee¨n JH, De Looze MP, Hermans V. Effects of dynamic office chairs on trunk kinematics, trunk extensor EMG and spinal shrinkage. Ergonomics. 2001; 44(7):739-50. [DOI:10.1080/00140130120297] [PMID]
- Vergara M, Page A’. Relationship between comfort and back posture and mobility in sitting-posture. Applied Ergonomics. 2002; 33(1):1-8. [DOI:10.1016/S0003-6870(01)00056-4] [PMID]
- Nairn BC, Azar NR, Drake JD. Transient pain developers show increased abdominal muscle activity during prolonged sitting. Journal of Electromyography and Kinesiology. 2013; 23(6):1421-7. [DOI:10.1016/j.jelekin.2013.09.001] [PMID]
- McGregor A, McCarthy I, Dore’ C, Hughes S. Quantitative assessment of the motion of the lumbar spine in the low back pain population and the effect of different spinal pathologies of this motion. European Spine Journal. 1997; 6(5):308-15. [DOI:10.1007/BF01142676] [PMID]
- Bouzaboul M, Abidli Z, Ait Ali D, Rami Y, Amraoui J, Hadri A, et al. Assessing visual perception and working memory using digital pen in moroccan students with learning difficulties. Iranian Rehabilitation Journal. 2025; 23(1):105-16. [Link]
- Kuster RP, Bauer CM, Baumgartner D. Is active sitting on a dynamic office chair controlled by the trunk muscles?. Plos One. 2020; 15(11):e0242854. [DOI:10.1371/journal.pone.0242854] [PMID]
- Adams MA, Dolan P. Spine biomechanics. Journal of Biomechanics. 2005; 38(10):1972-83. [DOI:10.1016/j.jbiomech.2005.03.028] [PMID]
- Rabal-Pelay J, Cimarras-Otal C, Berzosa C, Bernal-Lafuente M, Ballestín-López JL, Laguna-Miranda C, et al. Spinal sagittal alignment, spinal shrinkage and back pain changes in office workers during a workday. International Journal of Occupational Safety and Ergonomics. 2022; 28(1):1-7. [DOI:10.1080/10803548.2019.1701238] [PMID]
- Bush TR, Hubbard RP, Design B. A comparison of four office chairs using biomechanical measures. Human Factors. 2008; 50(4):629-42. [DOI:10.1518/001872008X288321] [PMID]
- Harrison DDE, Harrison SO, Croft AC, Harrison DDE, Troyanovich SJ. Sitting biomechanics part I: Review of the literature. Journal of Manipulative and Physiological Therapeutics. 1999; 22(9):594-609. [DOI:10.1016/S0161-4754(99)70020-5] [PMID]
- Sadeghi Y, Hatamizadeh N, Shahshahani S, Hosseinzadeh S. Goal attainment scale (GAS) administration workshop and its effects on job motivation and burnout of pediatric occupational therapists. Iranian Rehabilitation Journal 2023; 21(1):49-56. [DOI:10.32598/irj.21.1.417.2]
- van Deursen LL, Patijn J, Durinck JR, Brouwer R, van Erven-Sommers JR, Vortman BJ. Sitting and low back pain: the positive effect of rotatory dynamic stimuli during prolonged sitting. European Spine Journal. 1999; 8:187-93. [DOI:10.1007/s005860050155] [PMID]
- Eriksen MB, Frandsen TF. The impact of patient, intervention, comparison, outcome (PICO) as a search strategy tool on literature search quality: A systematic review. Journal of the Medical Library Association. 2018; 106(4):420. [DOI:10.5195/jmla.2018.345] [PMID]
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021; 372. [DOI:10.1136/bmj.n71] [PMID]
- Maher CG, Sherrington C, Herbert RD, Moseley AM, Elkins M. Reliability of the PEDro scale for rating quality of randomized controlled trials. Physical Therapy. 2003; 83(8):713-721. [DOI:10.1093/ptj/83.8.713] [PMID]
- Brożek JL, Akl EA, Alonso-Coello P, Lang D, Jaeschke R, Williams JW, et al. Grading quality of evidence and strength of recommendations in clinical practice guidelines: Part 1 of 3. An overview of the GRADE approach and grading quality of evidence about interventions. Allergy. 2009; 64(5):669-77. [DOI:10.1111/j.1398-9995.2009.01973.x] [PMID]
- Goulet-Pelletier JC, Cousineau D. A review of effect sizes and their confidence intervals, Part I: The Cohen’sd family. The Quantitative Methods for Psychology. 2018; 14(4):242-65. [DOI:10.20982/tqmp.14.4.p242]
- Wang PC, Ritz BR, Janowitz I, Harrison RJ, Yu F, Chan J, et al. A randomized controlled trial of chair interventions on back and hip pain among sewing machine operators: the los angeles garment study. Journal of Occupational and Environmental Medicine. 2008; 50(3):255-62. [DOI:10.1097/JOM.0b013e318163869a] [PMID]
- Gagnon D, Nadeau S, Noreau L, Eng JJ, Gravel D. Electromyographic patterns of upper extremity muscles during sitting pivot transfers performed by individuals with spinal cord injury. Journal of Electromyography and Kinesiology. 2009; 19(3):509-20. [DOI:10.1016/j.jelekin.2007.12.005]
- Amick III BC, Robertson MM, DeRango K, Bazzani L, Moore A, Rooney T, Harrist R. Effect of office ergonomics intervention on reducing musculoskeletal symptoms. Spine. 2003; 28(24):2706-11. [DOI:10.1097/01.BRS.0000099740.87791.F7] [PMID]
- Cook C, Burgess-Limerick R. The effect of forearm support on musculoskeletal discomfort during call centre work. Applied Ergonomics. 2004; 35(4):337-42. [DOI:10.1016/j.apergo.2004.03.005] [PMID]
- Lengsfeld M, König IR, Schmelter J, Ziegler A. Passive rotary dynamic sitting at the workplace by office-workers with lumbar pain: A randomized multicenter study. The Spine Journal. 2007; 7(5):531-40. [DOI:10.1016/j.spinee.2006.06.390] [PMID]
- Lee S, De Barros FC, De Castro CS, Sato TD. Effect of an ergonomic intervention involving workstation adjustments on musculoskeletal pain in office workers-A randomized controlled clinical trial. Industrial Health. 2021; 59(2):78-85. [DOI:10.2486/indhealth.2020-0188] [PMID]
- Legg SJ, Mackie HW, Milicich W. Evaluation of a prototype multi-posture office chair. Ergonomics. 2002; 45(2):153-63. [DOI:10.1080/00140130110120042] [PMID]
- Herbert R, Dropkin J, Warren N, Sivin D, Doucette J, Kellogg L, et al. Impact of a joint labor-management ergonomics program on upper extremity musculoskeletal symptoms among garment workers. Applied Ergonomics. 2001; 32(5):453-60. [DOI:10.1016/S0003-6870(01)00024-2] [PMID]
- O’Sullivan K, McCarthy R, White A, O’Sullivan L, Dankaerts W. Lumbar posture and trunk muscle activation during a typing task when sitting on a novel dynamic ergonomic chair. Ergonomics. 2012; 55(12):1586-95. [DOI:10.1080/00140139.2012.721521] [PMID]
- Ellegast RP, Kraft K, Groenesteijn L, Krause F, Berger H, Vink P. Comparison of four specific dynamic office chairs with a conventional office chair: Impact upon muscle activation, physical activity and posture. Applied Ergonomics. 2012; 43(2):296-307. [DOI:10.1016/j.apergo.2011.06.005] [PMID]
- Dalager T, Jensen PT, Winther TS, Savarimuthu TR, Markauskas A, Mogensen O, et al. Surgeons’ muscle load during robotic-assisted laparoscopy performed with a regular office chair and the preferred of two ergonomic chairs: A pilot study. Applied Ergonomics. 2019; 78:286-92. [DOI:10.1016/j.apergo.2018.03.016] [PMID]
- Horton SJ, Johnson GM, Skinner MA. Changes in head and neck posture using an office chair with and without lumbar roll support. Spine. 2010; 35(12):E542-8. [DOI:10.1097/BRS.0b013e3181cb8f82] [PMID]
- Synnott A, Dankaerts W, Seghers J, Purtill H, O’Sullivan K. The effect of a dynamic chair on seated energy expenditure. Ergonomics. 2017; 60(10):1384-92. [DOI:10.1080/00140139.2017.1324114] [PMID]
- O’Keeffe M, Dankaerts W, O’Sullivan P, O’Sullivan L, O’Sullivan K. Specific flexion-related low back pain and sitting: Comparison of seated discomfort on two different chairs. Ergonomics. 2013; 56(4):650-8. [DOI:10.1080/00140139.2012.762462] [PMID]
- Luna-Ávila GP, González-Muñoz EL. Comparison of posture, comfort and satisfaction between a dynamic seat and a seat with ergonomic criteria. Paper presented at: Advances in Ergonomics in Design: Proceedings of the AHFE 2018 International Conference on Ergonomics in Design. 21 July 2018; Orlando, USA. [DOI:10.1007/978-3-319-94706-8_57]
- Vos GA, Congleton JJ, Moore JS, Amendola AA, Ringer L. Postural versus chair design impacts upon interface pressure. Applied ergonomics. 2006; 37(5):619-28. [DOI:10.1016/j.apergo.2005.09.002] [PMID]
- Cardoso MR, Cardenas AK, Albert WJ. A biomechanical analysis of active vs static office chair designs. Applied Ergonomics. 2021; 96:103481. [DOI:10.1016/j.apergo.2021.103481] [PMID]
- Desroches G, Gagnon D, Nadeau S, Popovic M. Magnitude of forward trunk flexion influences upper limb muscular efforts and dynamic postural stability requirements during sitting pivot transfers in individuals with spinal cord injury. Journal of Electromyography and Kinesiology. 2013; 23(6):1325-33. [DOI:10.1016/j.jelekin.2013.09.004]
- Curran M, Dankaerts W, O’Sullivan P, O’Sullivan L, O’Sullivan K. The effect of a backrest and seatpan inclination on sitting discomfort and trunk muscle activation in subjects with extension-related low back pain. Ergonomics. 2014; 57(5):733-43. [DOI:10.1080/00140139.2014.897378] [PMID]
- Van Geffen P, Reenalda J, Veltink PH, Koopman BF. Decoupled pelvis adjustment to induce lumbar motion: A technique that controls low back load in sitting. International Journal of Industrial Ergonomics. 2010; 40(1):47-54. [DOI:10.1016/j.ergon.2009.08.015]
- Channak S, Speklé EM, van der Beek AJ, Janwantanakul P. Effect of two dynamic seat cushions on postural shift, trunk muscle activation and spinal discomfort in office workers. Applied Ergonomics. 2024; 120:104337. [DOI:10.1016/j.apergo.2024.104337] [PMID]
- Ecemiş ZB, Güzel NA, Çobanoğlu G, Kafa N. Comparing the effects of ergonomic and standard office chairs on trunk muscle activation. Journal of Basic and Clinical Health Sciences. 2021; 7(2):628-34. [DOI:10.30621/jbachs.1140904]
- Kingma I, van Dieën JH. Static and dynamic postural loadings during computer work in females: Sitting on an office chair versus sitting on an exercise ball. Applied Ergonomics. 2009; 40(2):199-205. [DOI:10.1016/j.apergo.2008.04.004] [PMID]
- Makhsous M, Lin F, Hendrix RW, Hepler M, Zhang LQ. Sitting with adjustable ischial and back supports: Biomechanical changes. Spine. 2003; 28(11):1113-21. [DOI:10.1097/01.BRS.0000068243.63203.A8] [PMID]
- Park SY, Yoo WG. Effects of a posture-sensing air seat device (PSASD) on kinematics and trunk muscle activity during continuous computer work. Journal of Physiological Anthropology. 2011; 30(4):147-51. [DOI:10.2114/jpa2.30.147] [PMID]
- Yoo WG. Effects of an unstable dual foot support on the trunk flexion angle and RF, L4-ES, EO muscle activities during computer work. Journal of Physical Therapy Science. 2013; 25(3):235-6. [DOI:10.1589/jpts.25.235]
- Vlaović Z, Bogner A, Grbac I. Comfort evaluation as the example of anthropotechnical furniture design. Collegium Antropologicum. 2008; 32(1):277-83. [Link]
- Beers EA, Roemmich JN, Epstein LH, Horvath PJ. Increasing passive energy expenditure during clerical work. European Journal of Applied Physiology. 2008; 103:353-60. [DOI:10.1007/s00421-008-0713-y] [PMID]
- Ericson MO, Goldie I. Spinal shrinkage with three different types of chair whilst performing video display unit work. international Journal of Industrial Ergonomics. 1989; 3(3):177-83. [DOI:10.1016/0169-8141(89)90017-6]
- Purepong N, Channak S, Boonyong S, Thaveeratitham P, Janwantanakul P. The effect of an acupressure backrest on pain and disability in office workers with chronic low back pain: A randomized, controlled study and patients’ preferences. Complementary Therapies in Medicine. 2015; 23(3):347-55. [DOI:10.1016/j.ctim.2015.03.005] [PMID]
- Roossien CC, Stegenga J, Hodselmans AP, Spook SM, Koolhaas W, Brouwer S, et al. Can a smart chair improve the sitting behavior of office workers?. Applied ergonomics. 2017; 65:355-61. [DOI:10.1016/j.apergo.2017.07.012] [PMID]
- van Niekerk SM, Louw QA, Hillier S. The effectiveness of a chair intervention in the workplace to reduce musculoskeletal symptoms. A systematic review. BMC Musculoskeletal Disorders. 2012; 13:145. [DOI:10.1186/1471-2474-13-145] [PMID]
- Dianat I, Molenbroek J, Castellucci HI. A review of the methodology and applications of anthropometry in ergonomics and product design. Ergonomics. 2018; 61(12):1696-720. [DOI:10.1080/00140139.2018.1502817] [PMID]
- Braganca S, Castellucci I, Costa E, Arezes P, Carvalho M. Anthropometric data for wheelchair users: A systematic literature review. International Journal of Occupational Safety and Ergonomics. 2020; 2019:1-42. [Link]
- Kastelic K, Kozinc Ž, Šarabon N. Sitting and low back disorders: An overview of the most commonly suggested harmful mechanisms. Collegium Antropologicum. 2018; 42(1):73-9. [Link]
- Lis AM, Black KM, Korn H, Nordin M. Association between sitting and occupational LBP. European Spine Journal. 2007; 16(2):283-98. [DOI:10.1007/s00586-006-0143-7] [PMID]
- van Dieën JH, Westebring-van der Putten EP, Kingma I, et al. Low level activity of the trunk extensor muscles causes electromyographic manifestations of fatigue in absence of decreased oxygenation. Nerve Conduction Studies and Electromyography. 2009; 19(3):398-406. [DOI:10.1016/j.jelekin.2007.11.010] [PMID]
Type of Study: Systematic Review |
Subject:
Occupational Therapy
Received: 2025/10/6 | Accepted: 2025/10/14 | Published: 2026/04/1
Received: 2025/10/6 | Accepted: 2025/10/14 | Published: 2026/04/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
