Thu, Jul 30, 2026
Volume 16, Issue 2 (Spring 2026)
PTJ 2026, 16(2): 233-238 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Vadamalai G, Ramalingam K, M K, Tamildasan K, N S, K K. Return-to-play Rehabilitation of a Professional Fast Bowler Following Rotator Cuff Tear, Superior Labrum AnteriorPosterior Repair and Shoulder Impingement: A Case Study. PTJ 2026; 16 (2) :233-238
URL: http://ptj.uswr.ac.ir/article-1-815-en.html
URL: http://ptj.uswr.ac.ir/article-1-815-en.html
Geethapriya Vadamalai1 

 , Karthika Ramalingam *2 , Kamalakannan M1 , Karthik Tamildasan3 , Suriya N1 , Kavitha K4
, Karthika Ramalingam *2 , Kamalakannan M1 , Karthik Tamildasan3 , Suriya N1 , Kavitha K4
, Karthika Ramalingam *2 , Kamalakannan M1 , Karthik Tamildasan3 , Suriya N1 , Kavitha K4
1- Saveetha College of Physiotherapy, Saveetha Institute of Medical and Technical Sciences, Chennai, India.
2- Saveetha College of Physiotherapy, Saveetha Institute of Medical and Technical Sciences, Chennai, India. & Pachamuthu College of Physiotherapy, Dharmapuri, India.
3- Cricket Association, Pondicherry, India.
4- Meenakshi Academy of Higher Education and Research Centre, Chennai, Chennai, India.
2- Saveetha College of Physiotherapy, Saveetha Institute of Medical and Technical Sciences, Chennai, India. & Pachamuthu College of Physiotherapy, Dharmapuri, India.
3- Cricket Association, Pondicherry, India.
4- Meenakshi Academy of Higher Education and Research Centre, Chennai, Chennai, India.
Keywords: Rotator cuff tear, Superior labrum anteriorposterior (SLAP) lesion, Fast bowler, Shoulder rehabilitation, Injury-psychological readiness to return to sport scale (I-PRRS), Shoulder pain and disability index (SPADI)
Full-Text [PDF 382 kb]
(1118 Downloads)
| Abstract (HTML) (2001 Views)
Full-Text: (177 Views)
Introduction
Shoulder injuries are particularly prevalent among fast bowlers in cricket, largely due to the high-velocity and repetitive arm movements involved in bowling. These motions place significant stress on the glenohumeral joint, often resulting in pathologies, such as rotator cuff tears and superior labrum anteriorposterior (SLAP) lesions [1, 2]. This case study examines a 30-year-old male fast bowler who sustained a Grade 2C rotator cuff tear, an associated SLAP tear, and shoulder impingement, diagnosed via magnetic resonance imaging (MRI) and subsequently underwent arthroscopic surgical repair.
Persistent pain, reduced shoulder stability and performance decline prompted surgical intervention followed by a carefully tailored rehabilitation program focusing on pain management, restoration of range of motion (ROM), progressive strengthening and sport-specific reconditioning.
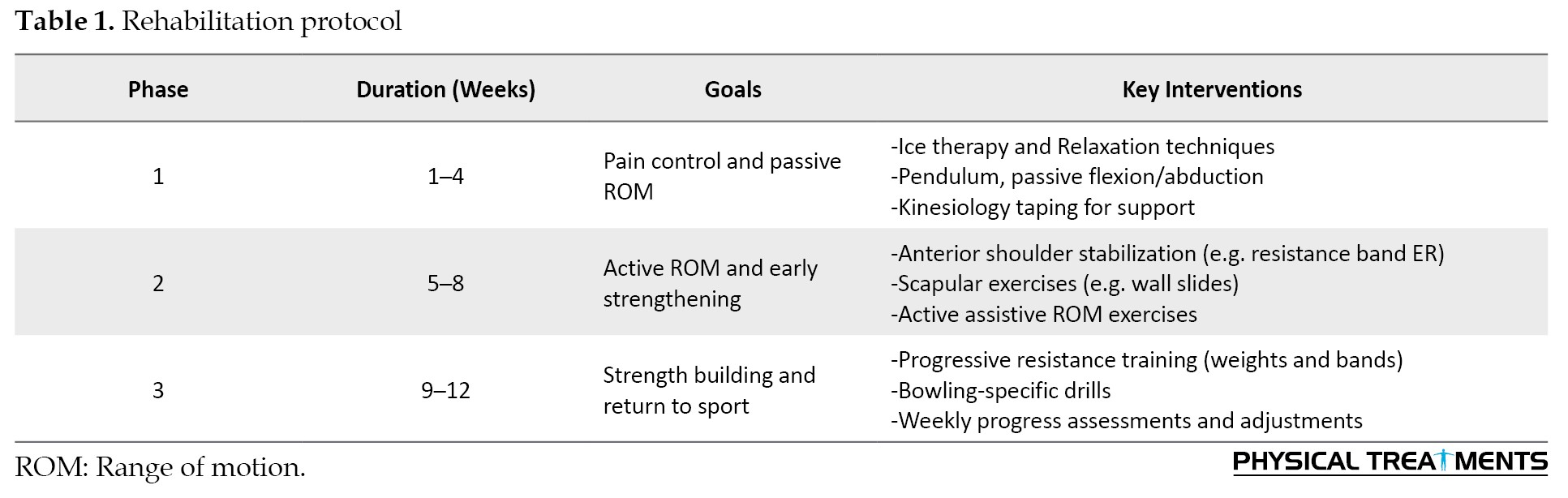
In addition to physical deficits, shoulder injuries significantly impact an athlete’s psychological readiness. Fear of re-injury and anxiety about returning to competitive play are well-documented among athletes engaging in overhead sports, highlighting the need for psychological strategies within rehabilitation protocols (Table 1) [2, 3].
This case study aimed to outline a multidimensional rehabilitation approach that integrates both physical and psychological components to maximize return-to-sport outcomes.
The fast-bowling action involves a kinetic sequence, including wind-up, delivery stride, and follow through, which place substantial repetitive multi-planar load on the shoulder joint, contributing to microtrauma over time and increasing the risk of injury. Systematic surveillance data suggest that shoulder injuries constitute approximately 10% of injuries in fast bowlers and up to 16.7% in spin bowlers. The prevalence varies between about 0.9–1.1% depending on playing level and match conditions [4].
A cross-sectional analysis of 100 state and district level fast bowlers in India found significant shoulder disability scores, as measured by shoulder pain and disability index (SPADI) and constant-murley assessments, reinforcing the relationship between bowling mechanics and shoulder dysfunction [1]. Research conducted in elite cricketers identified altered glenohumeral rotational patterns specifically decreased internal rotation and increased external rotation on the dominant side. This suggests adaptive tissue changes, such as internal rotation deficits, which are implicated in labral pathology and rotator cuff injuries [5].
Biomechanical studies indicate front-on bowling actions may predispose bowlers to shoulder pathology through increased shear stresses and rotator cuff muscle imbalance, particularly external/internal strength ratios linked to a greater injury risk [6]. Scapular kinematic alterations and posterior capsule tightness have also been observed in asymptomatic bowlers and may serve as precursors to SLAP lesions and rotator cuff tears [7].
SLAP lesions are commonly reported in overhead athletes and are frequently caused by chronic overuse or acute traction injuries, with symptoms including catching, shoulder instability, and decreased throwing velocity [2]. Rotator cuff tears, especially partial thickness tears, such as Grade 2C, often emerge from repetitive deceleration forces and compromised tendon integrity, further affecting shoulder function and athletic performance.
When conservative management fails, arthroscopic repair is often required. Surgical outcomes in overhead athletes improve when combined with structured rehabilitation incorporating progressive ROM exercises, rotator cuff and scapular strengthening, proprioception and sports specific drills alongside psychological support to address fear of re-injury and ensure optimal return-to-play readiness [2, 3, 8].
This case study documents the application of a comprehensive, evidence-informed rehabilitation strategy for a professional fast bowler with complex shoulder injuries, aligning with current best practices in sports medicine and physiotherapy.
The shoulder rehabilitation effects evaluated by a combination of subjective and objective measures provide a comprehensive picture of recovery. The visual analogue scale (VAS) is widely used for quantifying perceived pain levels and monitoring improvements over time [9]. The SPADI assesses both pain and functional limitations and is also sensitive to change following rotator cuff repair [10]. The injury-psychological readiness to return to sport scale (I-PRRS) captures athletes’ confidence and mental preparedness to resume sport, a crucial but often overlooked component of rehabilitation in overhead athletes [11]. Objective functional recovery is measured using ROM assessments and manual muscle testing (MMT), which together reflect structural healing, strength gains, and readiness for sport-specific activities [12, 13]. These outcome measures enable a multidimensional evaluation of post-operative progress and return to play decision making. Outcomes were measured by the treating therapist prior to initiating rehabilitation and subsequently documented.
Case Report
This case study included a 30-year-old male professional cricketer who presented with persistent right shoulder pain and functional limitation, particularly affecting his bowling performance. He had an extensive playing history as a fast bowler at the competitive level. MRI revealed a Grade 2C rotator cuff tear, a SLAP tear and signs of shoulder impingement. Given the functional demands of his sport, the injury had a significant impact on his ability to perform.
Surgical intervention
The athlete underwent arthroscopic surgery. Surgical procedures included rotator cuff repair, SLAP repair and subacromial decompression. Postoperatively, he was discharged with specific instructions regarding pain management, activity restrictions and an individualized rehabilitation plan to guide recovery.
Results
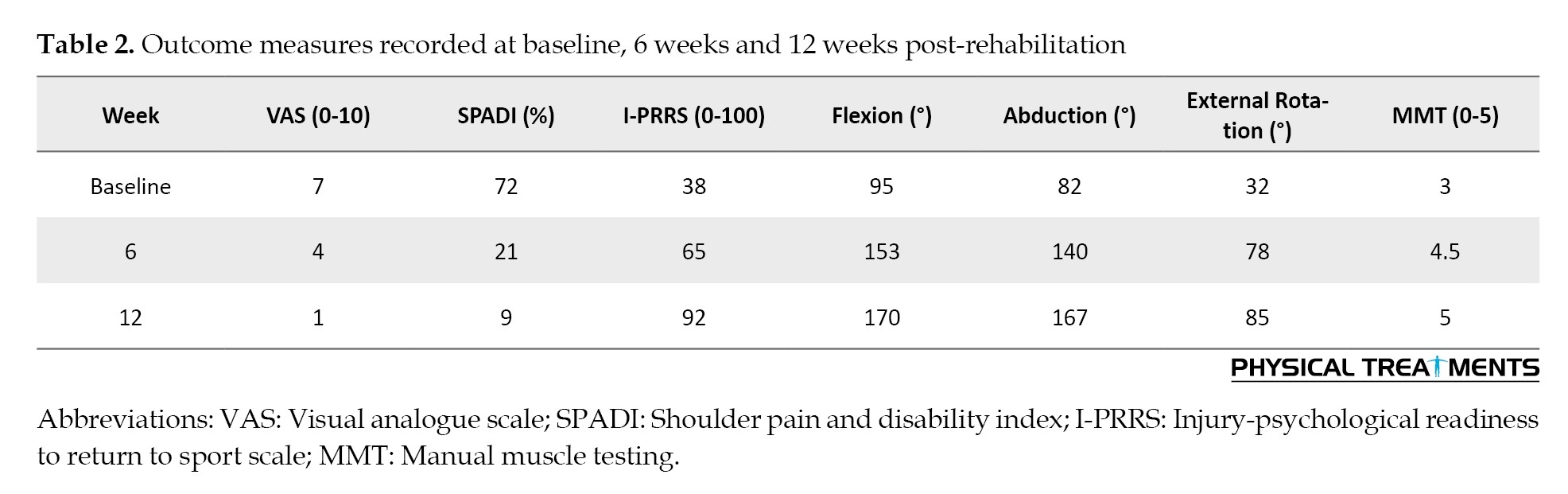
Over the 12-week rehabilitation program, the athlete demonstrated progressive improvement across all measured outcomes. Pain reduced by almost 85.7%. SPADI scores declined significantly from 72% to 9%, indicating marked improvement in shoulder function up to 87.5%. Psychological readiness (I-PRRS) increased by 54%, reflecting enhanced confidence in returning to sport. ROM improved substantially in all planes. Muscle strength (MMT) improved from Grade 3 to 5, indicating full recovery of rotator cuff strength. Table 2 presents the data.
Discussion
This case report highlights the successful rehabilitation of a professional fast bowler who underwent arthroscopic repair for a Grade 2C rotator cuff tear, SLAP lesion and subacromial decompression. The athlete’s structured 12-week rehabilitation program resulted in marked improvements in pain, function, ROM, muscle strength, and psychological readiness key domains necessary for a safe return to high-performance sport.
The patient experienced a significant reduction in pain and functional disability. These findings are consistent with evidence supporting early mobilization and progressive strengthening following rotator cuff and labral repair. Wilk et al. (2002) emphasized that early rehabilitation focusing on controlled motion and stability facilitates faster symptom resolution and functional gains in overhead athletes [14].
Notably, shoulder mobility improved across all planes of motion. This improvement supports established rehabilitation principles that emphasize gradual ROM restoration alongside neuromuscular control to ensure safe reintegration into sport-specific tasks [15].
Muscle strength also improved significantly, with MMT increasing from Grade 3 to Grade 5 by the end of the rehabilitation period. This finding supports the work of De Mey et al. (2013), who emphasized the importance of scapular-focused exercises in overhead athletes and demonstrated improvements in both SPADI scores and shoulder strength [16].
A crucial underappreciated component of rehabilitation is psychological readiness. The athlete’s I-PRRS score rose from 38 to 92, reflecting restored confidence and mental preparedness. These results align with studies highlighting psychological readiness as a critical predictor of return-to-sport success, especially in upper-limb injuries where fear of reinjury may linger [11].
The outcomes in this case support a rehabilitation model that integrates physical restoration and psychological readiness. A phased approach emphasizing pain control, joint mobility, muscular strength and mental resilience proved effective in enabling this fast bowler to return safely to competitive sport. While the single-case design limits generalizability, this case adds to the growing body of literature supporting individualized, sport-specific rehabilitation for overhead athletes.
Conclusion
This case illustrates the success of a structured, individualized rehabilitation program in restoring both physical function and psychological readiness in a professional fast bowler following shoulder surgery. The integration of pain control, progressive mobility, strength training and mental conditioning was crucial in facilitating a timely and safe return to sport.
Ethical Considerations
Compliance with ethical guidelines
Compliance with ethical guidelines all procedures were performed according to the Helsinki declaration of 1975 and its modifications. Informed consent has been obtained from the patient for the publication of this case report.
Funding
This research did not receive any specific grants from public, commercial, or not-for-profit funding agencies.
Authors' contributions
Study design and drafting of the manuscript: Geethapriya Vadamalai; Data collection and literature review: Karthika Ramalingam; Rehabilitation protocol supervision: Kamalakannan M; Clinical management and revisions: Karthik Tamildasan; Data analysis and final editing: Suriya N, and Kavitha K.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors sincerely thank the athlete for his consent and cooperation, and the medical and rehabilitation team for their valuable support throughout the recovery process.
Shoulder injuries are particularly prevalent among fast bowlers in cricket, largely due to the high-velocity and repetitive arm movements involved in bowling. These motions place significant stress on the glenohumeral joint, often resulting in pathologies, such as rotator cuff tears and superior labrum anteriorposterior (SLAP) lesions [1, 2]. This case study examines a 30-year-old male fast bowler who sustained a Grade 2C rotator cuff tear, an associated SLAP tear, and shoulder impingement, diagnosed via magnetic resonance imaging (MRI) and subsequently underwent arthroscopic surgical repair.
Persistent pain, reduced shoulder stability and performance decline prompted surgical intervention followed by a carefully tailored rehabilitation program focusing on pain management, restoration of range of motion (ROM), progressive strengthening and sport-specific reconditioning.
In addition to physical deficits, shoulder injuries significantly impact an athlete’s psychological readiness. Fear of re-injury and anxiety about returning to competitive play are well-documented among athletes engaging in overhead sports, highlighting the need for psychological strategies within rehabilitation protocols (Table 1) [2, 3].
This case study aimed to outline a multidimensional rehabilitation approach that integrates both physical and psychological components to maximize return-to-sport outcomes.
The fast-bowling action involves a kinetic sequence, including wind-up, delivery stride, and follow through, which place substantial repetitive multi-planar load on the shoulder joint, contributing to microtrauma over time and increasing the risk of injury. Systematic surveillance data suggest that shoulder injuries constitute approximately 10% of injuries in fast bowlers and up to 16.7% in spin bowlers. The prevalence varies between about 0.9–1.1% depending on playing level and match conditions [4].
A cross-sectional analysis of 100 state and district level fast bowlers in India found significant shoulder disability scores, as measured by shoulder pain and disability index (SPADI) and constant-murley assessments, reinforcing the relationship between bowling mechanics and shoulder dysfunction [1]. Research conducted in elite cricketers identified altered glenohumeral rotational patterns specifically decreased internal rotation and increased external rotation on the dominant side. This suggests adaptive tissue changes, such as internal rotation deficits, which are implicated in labral pathology and rotator cuff injuries [5].
Biomechanical studies indicate front-on bowling actions may predispose bowlers to shoulder pathology through increased shear stresses and rotator cuff muscle imbalance, particularly external/internal strength ratios linked to a greater injury risk [6]. Scapular kinematic alterations and posterior capsule tightness have also been observed in asymptomatic bowlers and may serve as precursors to SLAP lesions and rotator cuff tears [7].
SLAP lesions are commonly reported in overhead athletes and are frequently caused by chronic overuse or acute traction injuries, with symptoms including catching, shoulder instability, and decreased throwing velocity [2]. Rotator cuff tears, especially partial thickness tears, such as Grade 2C, often emerge from repetitive deceleration forces and compromised tendon integrity, further affecting shoulder function and athletic performance.
When conservative management fails, arthroscopic repair is often required. Surgical outcomes in overhead athletes improve when combined with structured rehabilitation incorporating progressive ROM exercises, rotator cuff and scapular strengthening, proprioception and sports specific drills alongside psychological support to address fear of re-injury and ensure optimal return-to-play readiness [2, 3, 8].
This case study documents the application of a comprehensive, evidence-informed rehabilitation strategy for a professional fast bowler with complex shoulder injuries, aligning with current best practices in sports medicine and physiotherapy.
The shoulder rehabilitation effects evaluated by a combination of subjective and objective measures provide a comprehensive picture of recovery. The visual analogue scale (VAS) is widely used for quantifying perceived pain levels and monitoring improvements over time [9]. The SPADI assesses both pain and functional limitations and is also sensitive to change following rotator cuff repair [10]. The injury-psychological readiness to return to sport scale (I-PRRS) captures athletes’ confidence and mental preparedness to resume sport, a crucial but often overlooked component of rehabilitation in overhead athletes [11]. Objective functional recovery is measured using ROM assessments and manual muscle testing (MMT), which together reflect structural healing, strength gains, and readiness for sport-specific activities [12, 13]. These outcome measures enable a multidimensional evaluation of post-operative progress and return to play decision making. Outcomes were measured by the treating therapist prior to initiating rehabilitation and subsequently documented.
Case Report
This case study included a 30-year-old male professional cricketer who presented with persistent right shoulder pain and functional limitation, particularly affecting his bowling performance. He had an extensive playing history as a fast bowler at the competitive level. MRI revealed a Grade 2C rotator cuff tear, a SLAP tear and signs of shoulder impingement. Given the functional demands of his sport, the injury had a significant impact on his ability to perform.
Surgical intervention
The athlete underwent arthroscopic surgery. Surgical procedures included rotator cuff repair, SLAP repair and subacromial decompression. Postoperatively, he was discharged with specific instructions regarding pain management, activity restrictions and an individualized rehabilitation plan to guide recovery.
Results
Over the 12-week rehabilitation program, the athlete demonstrated progressive improvement across all measured outcomes. Pain reduced by almost 85.7%. SPADI scores declined significantly from 72% to 9%, indicating marked improvement in shoulder function up to 87.5%. Psychological readiness (I-PRRS) increased by 54%, reflecting enhanced confidence in returning to sport. ROM improved substantially in all planes. Muscle strength (MMT) improved from Grade 3 to 5, indicating full recovery of rotator cuff strength. Table 2 presents the data.
Discussion
This case report highlights the successful rehabilitation of a professional fast bowler who underwent arthroscopic repair for a Grade 2C rotator cuff tear, SLAP lesion and subacromial decompression. The athlete’s structured 12-week rehabilitation program resulted in marked improvements in pain, function, ROM, muscle strength, and psychological readiness key domains necessary for a safe return to high-performance sport.
The patient experienced a significant reduction in pain and functional disability. These findings are consistent with evidence supporting early mobilization and progressive strengthening following rotator cuff and labral repair. Wilk et al. (2002) emphasized that early rehabilitation focusing on controlled motion and stability facilitates faster symptom resolution and functional gains in overhead athletes [14].
Notably, shoulder mobility improved across all planes of motion. This improvement supports established rehabilitation principles that emphasize gradual ROM restoration alongside neuromuscular control to ensure safe reintegration into sport-specific tasks [15].
Muscle strength also improved significantly, with MMT increasing from Grade 3 to Grade 5 by the end of the rehabilitation period. This finding supports the work of De Mey et al. (2013), who emphasized the importance of scapular-focused exercises in overhead athletes and demonstrated improvements in both SPADI scores and shoulder strength [16].
A crucial underappreciated component of rehabilitation is psychological readiness. The athlete’s I-PRRS score rose from 38 to 92, reflecting restored confidence and mental preparedness. These results align with studies highlighting psychological readiness as a critical predictor of return-to-sport success, especially in upper-limb injuries where fear of reinjury may linger [11].
The outcomes in this case support a rehabilitation model that integrates physical restoration and psychological readiness. A phased approach emphasizing pain control, joint mobility, muscular strength and mental resilience proved effective in enabling this fast bowler to return safely to competitive sport. While the single-case design limits generalizability, this case adds to the growing body of literature supporting individualized, sport-specific rehabilitation for overhead athletes.
Conclusion
This case illustrates the success of a structured, individualized rehabilitation program in restoring both physical function and psychological readiness in a professional fast bowler following shoulder surgery. The integration of pain control, progressive mobility, strength training and mental conditioning was crucial in facilitating a timely and safe return to sport.
Ethical Considerations
Compliance with ethical guidelines
Compliance with ethical guidelines all procedures were performed according to the Helsinki declaration of 1975 and its modifications. Informed consent has been obtained from the patient for the publication of this case report.
Funding
This research did not receive any specific grants from public, commercial, or not-for-profit funding agencies.
Authors' contributions
Study design and drafting of the manuscript: Geethapriya Vadamalai; Data collection and literature review: Karthika Ramalingam; Rehabilitation protocol supervision: Kamalakannan M; Clinical management and revisions: Karthik Tamildasan; Data analysis and final editing: Suriya N, and Kavitha K.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors sincerely thank the athlete for his consent and cooperation, and the medical and rehabilitation team for their valuable support throughout the recovery process.
References
- Dhakate Darshana S, Yeole U, Mhatre S, Khatri S. Incidence of shoulder injuries amongst fast bowlers. International Journal of Research and Analytical Reviews. 2019; 6(1):42–5. [Link]
- Sundaram B, Bhargava SK, Karuppannan S. Glenohumeral rotational range of motion differences between fast bowlers and spin bowlers in elite cricketers. International Journal of Sports Physical Therapy. 2012; 7(6):576. [PMID]
- Zaremski JL, Wasser JG, Vincent HK. Mechanisms and treatments for shoulder injuries in overhead throwing athletes. Current Sports Medicine Reports. 2017; 16(3):179-88. [DOI:10.1249/JSR.0000000000000361]
- Boycott S, Petersen C. Cricket pace bowlers shoulder injuries: a systematic literature review and suggestions for prevention. Paper presented at: 5th World Congress of Science and Medicine in Cricket (WCSMC). 27March 2015; Sydney, Australia. [Link]
- Mansingh A. shoulder injuries in modern cricket: should an increase be anticipated?. Indian Journal of Orthopaedics. 2023; 57(10):1561-4. [DOI:10.1007/s43465-023-00963-x]
- Aginsky KD, Lategan L, Stretch RA. Shoulder injuries in provincial male fast bowlers-predisposing factors. South African Journal of Sports Medicine. 2004; 16(1):25-8. [Link]
- Tendulkar SS, Mehta N. Incidence of alteration of scapula position in bowlers. International Journal of Physical Education, Sports and Health. 2020; 7(4):81–4. [Link]
- Burkhart SS, Morgan CD, Kibler WB. Shoulder injuries in overhead athletes: The “dead arm” revisited. Clinics in Sports Medicine. 2000; 19(1):125-58. [DOI:10.1016/S0278-5919(05)70300-8] [PMID]
- Hawker GA, Mian S, Kendzerska T, French M. Measures of adult pain: Visual analog scale for pain (vas pain), numeric rating scale for pain (nrs pain), mcgill pain questionnaire (mpq), short-form mcgill pain questionnaire (sf-mpq), chronic pain grade scale (cpgs), short form-36 bodily pain scale (sf-36 bps), and measure of intermittent and constant osteoarthritis pain (icoap). Arthritis Care & Research. 2011; 63(S11):S240-52. [DOI:10.1002/acr.20543]
- MacDermid JC, Solomon P, Prkachin K. The shoulder pain and disability index demonstrates factor, construct and longitudinal validity. BMC Musculoskeletal Disorders. 2006; 7:12. [DOI:10.1186/1471-2474-7-12]
- Glazer DD. Development and preliminary validation of the injury-psychological readiness to return to sport (I-PRRS) scale. Journal of Athletic Training. 2009; 44(2):185–9. [DOI:10.4085/1062-6050-44.2.185]
- Wilk KE, Bagwell MS, Davies GJ, Arrigo CA. Return to sport participation criteria following shoulder injury: A clinical commentary. International Journal of Sports Physical Therapy. 2020; 15(4):624–42. [PMID]
- Ellenbecker TS, Cools A. Rehabilitation of shoulder impingement syndrome and rotator cuff injuries: An evidence-based review. British Journal of Sports Medicine. 2010; 44(5):319–27. [DOI:10.1136/bjsm.2009.058875]
- Wilk KE, Meister K, Andrews JR. Current concepts in the rehabilitation of the overhead throwing athlete. The American Journal of Sports Medicine. 2002; 30(1):136-51. [PMID]
- Wilk KE, Arrigo CA, Hooks TR, Andrews JR. Rehabilitation of the overhead throwing athlete: there is more to it than just external rotation/internal rotation strengthening. Pm&R. 2016; 8(3):S78-90. [DOI:10.1016/j.pmrj.2015.12.005]
- De Mey K, Danneels L, Cagnie B, Huyghe L, Seyns E, Cools AM. Conscious correction of scapular orientation in overhead athletes performing selected shoulder rehabilitation exercises: The effect on trapezius muscle activation measured by surface electromyography. Journal of Orthopaedic & Sports Physical Therapy. 2013; 43(1):3-10. [PMID]
Type of Study: case report |
Subject:
Sport injury and corrective exercises
Received: 2025/08/23 | Accepted: 2025/09/15 | Published: 2026/04/1
Received: 2025/08/23 | Accepted: 2025/09/15 | Published: 2026/04/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
