Tue, Jul 28, 2026
Volume 16, Issue 2 (Spring 2026)
PTJ 2026, 16(2): 127-132 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Piri E, Jafarnezhadgero A. Walking and Running Mechanics After Anterior Cruciate Ligament Reconstruction: An Editorial Review. PTJ 2026; 16 (2) :127-132
URL: http://ptj.uswr.ac.ir/article-1-804-en.html
URL: http://ptj.uswr.ac.ir/article-1-804-en.html



1- Department of Sports Biomechanics, Faculty of Educational Sciences and Psychology, University of Mohaghegh Ardabili, Ardabil, Iran.
Keywords: Anterior cruciate ligament reconstruction, Walking mechanics, Running mechanics, Gait analysis, Biomechanics
Full-Text [PDF 459 kb]
(599 Downloads)
| Abstract (HTML) (1634 Views)
Full-Text: (152 Views)
Introduction
Anterior cruciate ligament (ACL) reconstruction is one of the most common orthopedic procedures performed worldwide, aimed at restoring knee stability and enabling a return to functional activities, including walking and running [1]. Despite surgical success in anatomical repair, persistent biomechanical alterations in gait and running patterns are frequently observed during the post-operative recovery period [2]. Understanding the temporal evolution of these biomechanical adaptations, particularly at key milestones, such as 6, 12, and 18 months post-surgery, is critical for optimizing rehabilitation protocols and improving long-term outcomes [2, 3]. This editorial review synthesizes current evidence on the interplay between ACL reconstruction and locomotor mechanics, with a focus on spatiotemporal, kinematic, and kinetic changes during walking and running across the mid- to late-recovery phases. While many patients are cleared for return to sport (RTS) by 9–12 months, emerging data suggest that biomechanical symmetry and neuromuscular control may lag behind clinical milestones, raising concerns about reinjury risk and long-term joint health [4].
Biomechanical recovery at 6 months: the early functional phase
At 6 months post-surgery, most patients have completed the initial phases of rehabilitation and may begin to introduce running and sport-specific drills. However, biomechanical studies consistently report asymmetries in gait and running mechanics between the reconstructed and contralateral limbs [2, 3].
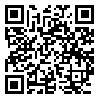
Walking: Patients often exhibit reduced knee flexion angle, lower peak knee extensor moment, and decreased ground reaction forces (GRFs) on the surgical side. These compensatory strategies are thought to protect the healing graft; however, they may contribute to abnormal joint loading over time [3-5].
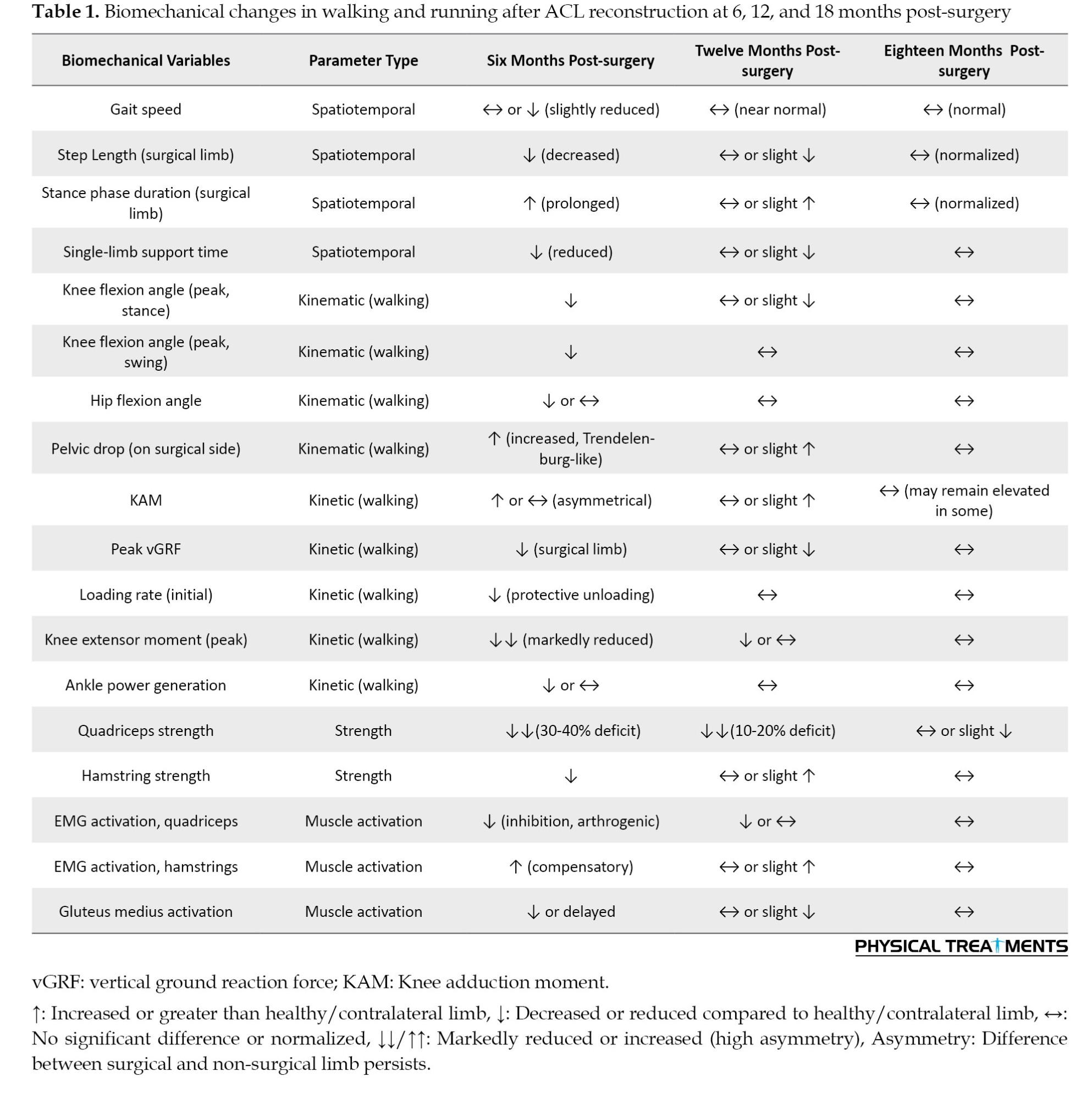
Running: Asymmetries are more pronounced during running. Studies using 3D motion analysis have shown reduced stride length, increased stance time on the non-operated limb, and diminished hip and knee power generation on the reconstructed side. Notably, even when patients report subjective readiness, objective biomechanical deficits persist in 60–70% of cases. These findings underscore a critical gap: clinical readiness does not necessarily equate to biomechanical readiness. Rehabilitation at this stage should emphasize neuromuscular re-education, dynamic stability, and progressive loading, rather than relying solely on time-based criteria [4]. The spatiotemporal, kinematic, and kinetic alterations observed at 6 months post-surgery are summarized in Table 1.
The 12-month milestone: Toward functional symmetry?
By 12 months, many athletes are cleared for RTS. However, meta-analyses and longitudinal cohort studies have revealed that true biomechanical symmetry is achieved in only a minority of patients [6]. Kinematic and kinetic asymmetries in both walking and running persist, particularly in knee abduction moments and hip control factors strongly associated with re-injury risk. Muscle activation patterns often remain altered, with persistent quadriceps inhibition and compensatory hamstring or gluteal dominance [7]. Loading rates during running are frequently higher in the non-operated limb, suggesting ongoing protective mechanisms and potential overuse injury risk in the contralateral knee [8]. Key running-specific biomechanical parameters observed after ACL reconstruction are presented in Table 2.
Importantly, psychological factors, such as fear of movement (kinesiophobia), may also contribute to altered mechanics independent of physical capacity [9]. Thus, a multidimensional assessment including biomechanical, strength, and psychosocial metrics is essential before RTS clearance.
Eighteen months and beyond: the long-term picture
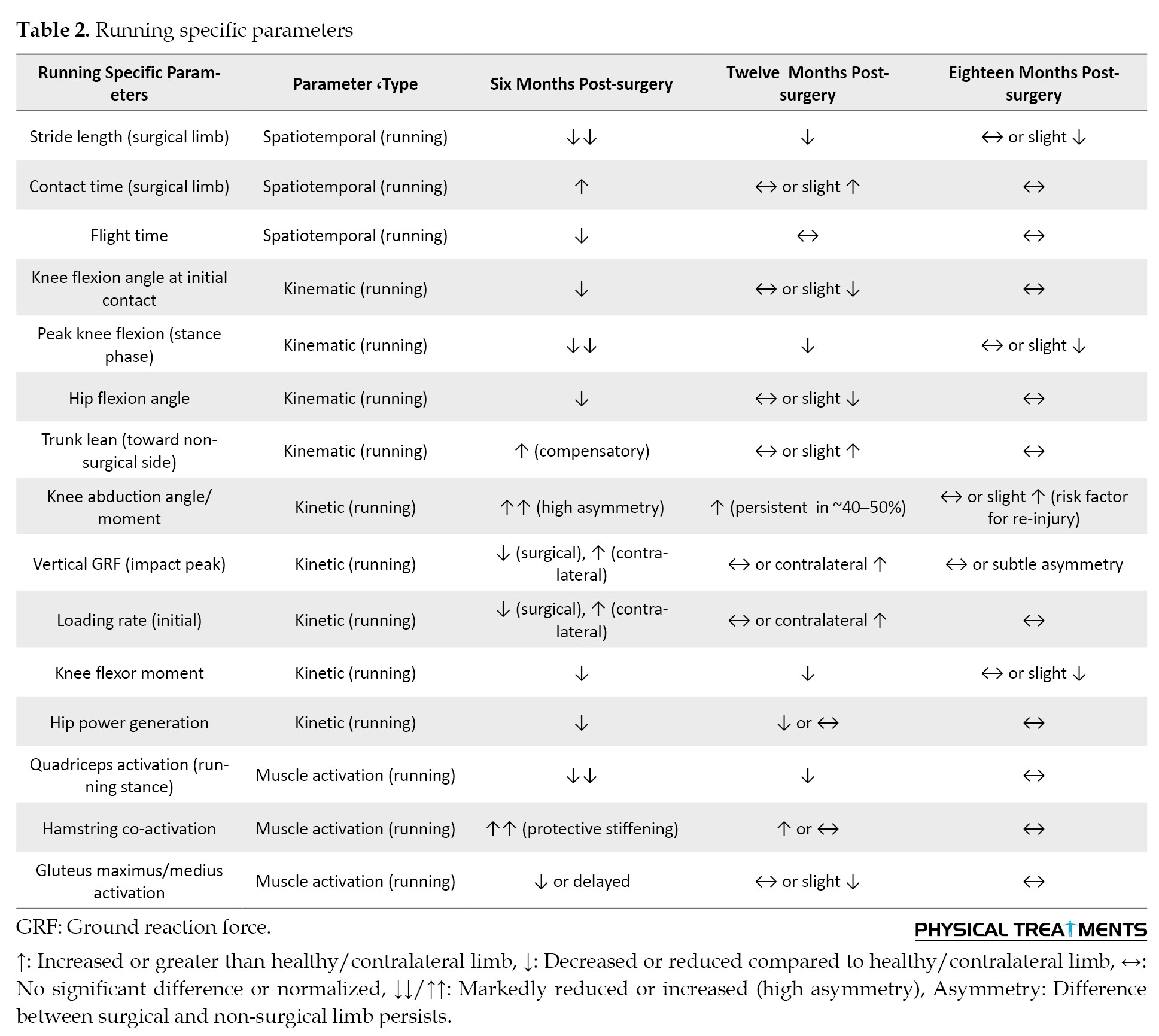
Emerging evidence suggests that biomechanical normalization may extend beyond 12 months, with some patients showing improvements as late as 18–24 months post-surgery [10]. At 18 months, gait patterns during walking often approach normal; however, running mechanics may still exhibit subtle asymmetries, particularly during cutting, deceleration, or high-speed tasks [5]. Longitudinal data indicate that patients who continue neuromuscular training and sport-specific conditioning beyond 12 months demonstrate better biomechanical outcomes and lower reinjury rates [11]. The temporal trends in walking and running mechanics following ACL reconstruction are summarized in Table 3.
There is also growing concern about the early onset of post-traumatic osteoarthritis (PTOA), potentially linked to persistent abnormal joint loading patterns, even in the absence of re-injury [12]. This delayed recovery trajectory challenges the conventional 9–12 month RTS timeline and calls for extended monitoring and individualized rehabilitation.
A comprehensive, evidence-based table summarizing biomechanical variables associated with walking and running after ACL reconstruction, evaluated at 6, 12, and 18 months post-surgery is presented below. The table includes key spatiotemporal, kinematic, kinetic, and muscle activation parameters, along with their direction of change (e.g. decreased, increased, asymmetrical, or normalized) relative to the contralateral limb or pre-injury norms, as per the current literature.
Clinical implications and future directions
The interplay between ACL reconstruction and locomotor mechanics is dynamic and multifactorial. The key takeaways for clinicians and researchers include:
1) Time-based return-to-sport criteria are insufficient. Objective biomechanical assessments (e.g. motion analysis, force plates, and wearable sensors) should be integrated into clinical decision-making. 2) Running mechanics are more sensitive than walking to residual deficits and should be specifically evaluated during rehabilitation. 3) Rehabilitation must extend beyond strength restoration to include neuromuscular control, proprioception, and psychological readiness. 4) Long-term follow-up is essential. Biomechanical recovery may continue beyond 18 months, and joint health monitoring should be prioritized to prevent PTOA.
Future research should focus on
Future research should focus on developing accessible tools for biomechanical screening in clinical settings, identifying predictors of persistent asymmetry, evaluating the impact of extended rehabilitation programs on long-term outcomes.
Suggestions for future research
1. Develop and validate accessible biomechanical assessment tools (e.g. wearable sensors, smartphone-based motion analysis) for routine clinical use to objectively evaluate gait and running symmetry before RTS clearance.
2. Investigate predictors of persistent biomechanical asymmetry, including neuromuscular, psychological (e.g., kinesiophobia), and graft-related factors, to enable early identification of high-risk patients. 3. Conduct longitudinal studies beyond 18 months to better understand the natural progression of biomechanical recovery and its relationship with early-onset PTOA. 4. Evaluate the effectiveness of extended, individualized rehabilitation programs incorporating neuromuscular training, sport-specific drills, and psychological support on long-term biomechanical outcomes and reinjury rates. 5. Compare different graft types and surgical techniques in terms of their impact on locomotor mechanics during walking and running across the recovery timeline.
Conclusion
ACL reconstruction is not merely a surgical intervention; rather, it is the beginning of a prolonged biomechanical recalibration process. While patients may appear functionally recovered by 12 months, subtle yet clinically significant alterations in walking and running mechanics often persist, evolving gradually up to 18 months and beyond. Recognizing this delayed recovery timeline is essential for minimizing reinjury risk, optimizing performance, and preserving joint health. As we move toward more personalized and evidence-based rehabilitation, the integration of longitudinal biomechanical assessments is paramount. However, biomechanical recovery after ACL reconstruction extends well beyond the conventional 9–12 month return-to-sport timeline, with running mechanics revealing residual asymmetries in knee control and loading that may increase reinjury risk and contribute to long-term joint degeneration.
Ethical Considerations
Compliance with ethical guidelines
There were no ethical considerations to be considered in this research.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Methodology, investigation, resources, visualization, project administration, and writing the original draft: Ebrahim Piri; Supervision: AmirAli Jafarnezhadgero; Conceptualization, validation, review and editing: All authors.
Conflict of interest
The authors declared no conflicts of interest.
Anterior cruciate ligament (ACL) reconstruction is one of the most common orthopedic procedures performed worldwide, aimed at restoring knee stability and enabling a return to functional activities, including walking and running [1]. Despite surgical success in anatomical repair, persistent biomechanical alterations in gait and running patterns are frequently observed during the post-operative recovery period [2]. Understanding the temporal evolution of these biomechanical adaptations, particularly at key milestones, such as 6, 12, and 18 months post-surgery, is critical for optimizing rehabilitation protocols and improving long-term outcomes [2, 3]. This editorial review synthesizes current evidence on the interplay between ACL reconstruction and locomotor mechanics, with a focus on spatiotemporal, kinematic, and kinetic changes during walking and running across the mid- to late-recovery phases. While many patients are cleared for return to sport (RTS) by 9–12 months, emerging data suggest that biomechanical symmetry and neuromuscular control may lag behind clinical milestones, raising concerns about reinjury risk and long-term joint health [4].
Biomechanical recovery at 6 months: the early functional phase
At 6 months post-surgery, most patients have completed the initial phases of rehabilitation and may begin to introduce running and sport-specific drills. However, biomechanical studies consistently report asymmetries in gait and running mechanics between the reconstructed and contralateral limbs [2, 3].
Walking: Patients often exhibit reduced knee flexion angle, lower peak knee extensor moment, and decreased ground reaction forces (GRFs) on the surgical side. These compensatory strategies are thought to protect the healing graft; however, they may contribute to abnormal joint loading over time [3-5].
Running: Asymmetries are more pronounced during running. Studies using 3D motion analysis have shown reduced stride length, increased stance time on the non-operated limb, and diminished hip and knee power generation on the reconstructed side. Notably, even when patients report subjective readiness, objective biomechanical deficits persist in 60–70% of cases. These findings underscore a critical gap: clinical readiness does not necessarily equate to biomechanical readiness. Rehabilitation at this stage should emphasize neuromuscular re-education, dynamic stability, and progressive loading, rather than relying solely on time-based criteria [4]. The spatiotemporal, kinematic, and kinetic alterations observed at 6 months post-surgery are summarized in Table 1.
The 12-month milestone: Toward functional symmetry?
By 12 months, many athletes are cleared for RTS. However, meta-analyses and longitudinal cohort studies have revealed that true biomechanical symmetry is achieved in only a minority of patients [6]. Kinematic and kinetic asymmetries in both walking and running persist, particularly in knee abduction moments and hip control factors strongly associated with re-injury risk. Muscle activation patterns often remain altered, with persistent quadriceps inhibition and compensatory hamstring or gluteal dominance [7]. Loading rates during running are frequently higher in the non-operated limb, suggesting ongoing protective mechanisms and potential overuse injury risk in the contralateral knee [8]. Key running-specific biomechanical parameters observed after ACL reconstruction are presented in Table 2.
Importantly, psychological factors, such as fear of movement (kinesiophobia), may also contribute to altered mechanics independent of physical capacity [9]. Thus, a multidimensional assessment including biomechanical, strength, and psychosocial metrics is essential before RTS clearance.
Eighteen months and beyond: the long-term picture
Emerging evidence suggests that biomechanical normalization may extend beyond 12 months, with some patients showing improvements as late as 18–24 months post-surgery [10]. At 18 months, gait patterns during walking often approach normal; however, running mechanics may still exhibit subtle asymmetries, particularly during cutting, deceleration, or high-speed tasks [5]. Longitudinal data indicate that patients who continue neuromuscular training and sport-specific conditioning beyond 12 months demonstrate better biomechanical outcomes and lower reinjury rates [11]. The temporal trends in walking and running mechanics following ACL reconstruction are summarized in Table 3.
There is also growing concern about the early onset of post-traumatic osteoarthritis (PTOA), potentially linked to persistent abnormal joint loading patterns, even in the absence of re-injury [12]. This delayed recovery trajectory challenges the conventional 9–12 month RTS timeline and calls for extended monitoring and individualized rehabilitation.
A comprehensive, evidence-based table summarizing biomechanical variables associated with walking and running after ACL reconstruction, evaluated at 6, 12, and 18 months post-surgery is presented below. The table includes key spatiotemporal, kinematic, kinetic, and muscle activation parameters, along with their direction of change (e.g. decreased, increased, asymmetrical, or normalized) relative to the contralateral limb or pre-injury norms, as per the current literature.
Clinical implications and future directions
The interplay between ACL reconstruction and locomotor mechanics is dynamic and multifactorial. The key takeaways for clinicians and researchers include:
1) Time-based return-to-sport criteria are insufficient. Objective biomechanical assessments (e.g. motion analysis, force plates, and wearable sensors) should be integrated into clinical decision-making. 2) Running mechanics are more sensitive than walking to residual deficits and should be specifically evaluated during rehabilitation. 3) Rehabilitation must extend beyond strength restoration to include neuromuscular control, proprioception, and psychological readiness. 4) Long-term follow-up is essential. Biomechanical recovery may continue beyond 18 months, and joint health monitoring should be prioritized to prevent PTOA.
Future research should focus on
Future research should focus on developing accessible tools for biomechanical screening in clinical settings, identifying predictors of persistent asymmetry, evaluating the impact of extended rehabilitation programs on long-term outcomes.
Suggestions for future research
1. Develop and validate accessible biomechanical assessment tools (e.g. wearable sensors, smartphone-based motion analysis) for routine clinical use to objectively evaluate gait and running symmetry before RTS clearance.
2. Investigate predictors of persistent biomechanical asymmetry, including neuromuscular, psychological (e.g., kinesiophobia), and graft-related factors, to enable early identification of high-risk patients. 3. Conduct longitudinal studies beyond 18 months to better understand the natural progression of biomechanical recovery and its relationship with early-onset PTOA. 4. Evaluate the effectiveness of extended, individualized rehabilitation programs incorporating neuromuscular training, sport-specific drills, and psychological support on long-term biomechanical outcomes and reinjury rates. 5. Compare different graft types and surgical techniques in terms of their impact on locomotor mechanics during walking and running across the recovery timeline.
Conclusion
ACL reconstruction is not merely a surgical intervention; rather, it is the beginning of a prolonged biomechanical recalibration process. While patients may appear functionally recovered by 12 months, subtle yet clinically significant alterations in walking and running mechanics often persist, evolving gradually up to 18 months and beyond. Recognizing this delayed recovery timeline is essential for minimizing reinjury risk, optimizing performance, and preserving joint health. As we move toward more personalized and evidence-based rehabilitation, the integration of longitudinal biomechanical assessments is paramount. However, biomechanical recovery after ACL reconstruction extends well beyond the conventional 9–12 month return-to-sport timeline, with running mechanics revealing residual asymmetries in knee control and loading that may increase reinjury risk and contribute to long-term joint degeneration.
Ethical Considerations
Compliance with ethical guidelines
There were no ethical considerations to be considered in this research.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Methodology, investigation, resources, visualization, project administration, and writing the original draft: Ebrahim Piri; Supervision: AmirAli Jafarnezhadgero; Conceptualization, validation, review and editing: All authors.
Conflict of interest
The authors declared no conflicts of interest.
Reference
- Filbay SR, Bullock G, Russell S, Brown F, Hui W, Egerton T. No difference in return-to-sport rate or activity level in people with anterior cruciate ligament (ACL) injury managed with ACL reconstruction or rehabilitation alone: A systematic review and meta-analysis: SR Filbay et al. Sports Medicine. 2025; 1-15. [PMID]
- Lee H, Lisee C, Büttner C, Bjornsen E, Favoreto N, Creighton RA, et al. Lower extremity mechanical energetics during walking 6 months following anterior cruciate ligament reconstruction. Scandinavian Journal of Medicine & Science in Sports. 2025; 35(7):e70105. [PMID]
- Gao T, Huang H, Yu Y, Liu H, Ao Y. Effect of knee extension constraint training on walking biomechanics 6 months after anterior cruciate ligament reconstruction: A double-blind randomized controlled clinical trial. Journal of Orthopaedic Surgery and Research. 2025; 20(1):20. [PMID]
- Lu Y, Zhao F, Kuai S, Zhang S, Yu Y, Huang H, et al. Lower limb joint kinetics during level walking in patients two years after anterior cruciate ligament reconstruction. Sports Medicine and Health Science. 2025 [Unpublished]. [DOI:10.1016/j.smhs.2025.02.003]
- Pfile K, Prosser B, Slone H, McLeod M, Gregory C, Hunnicutt J. Walking gait biomechanics in individuals with quadriceps tendon autograft anterior cruciate ligament reconstruction. Frontiers in Sports and Active Living. 2025; 7:1546297. [PMID]
- Girdwood M, Culvenor AG, Rio EK, Patterson BE, Haberfield M, Couch J, et al. Tale of quadriceps and hamstring muscle strength after ACL reconstruction: A systematic review with longitudinal and multivariate meta-analysis. British Journal of Sports Medicine. 2025; 59(6):423-34. [PMID]
- Ferguson D, Palmer A, Khan S, Oduoza U, Atkinson H. Early or delayed anterior cruciate ligament reconstruction: Is one superior? A systematic review and meta-analysis. European Journal of Orthopaedic Surgery & Traumatology. 2019; 29(6):1277-89. [PMID]
- Cattano NM, Magee D, Clark KP, Smith J. Cartilage deformation, outcomes, and running force comparisons in females with and without knee injuries. Journal of Sport Rehabilitation. 2025; 1(aop):1-8. [PMID]
- Cozzi AL, Dunn KL, Harding JL, McLeod TCV, Bacon CEW. Kinesiophobia after anterior cruciate ligament reconstruction in physically active individuals. Journal of Sport Rehabilitation. 2015; 24(4):434-9. [PMID]
- Büttner C, Lisee C, Bjornsen E, Buck A, Favoreto N, Creighton A, et al. Bilateral waveform analysis of gait biomechanics presurgery to 12 months following ACL reconstruction compared to controls. Journal of Orthopaedic Research®. 2025; 43(2):322-36. [PMID]
- Li S, Lu B, Zhang Y, Liu J, Xu W, Li Q. The effect of neuromuscular electrical stimulation superimposed on quadriceps training on gait dynamics after anterior cruciate ligament reconstruction. Journal of Back and Musculoskeletal Rehabilitation. 2025;38(1):139-47. [PMID]
- Harkey MS, Driban JB, Todem D, Kuenze C, Mahmoudian A, Meiring R, et al. Evaluating criteria for symptoms suggestive of early osteoarthritis over two years post–anterior cruciate ligament reconstruction: Data from the New Zealand anterior cruciate ligament registry. Arthritis Care & Research. 2025; 77(4):475-83. [PMID]
Type of Study: Systematic Review |
Subject:
Sports biomechanics
Received: 2024/07/30 | Accepted: 2025/05/19 | Published: 2026/04/1
Received: 2024/07/30 | Accepted: 2025/05/19 | Published: 2026/04/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
