Tue, Jul 28, 2026
Volume 16, Issue 2 (Spring 2026)
PTJ 2026, 16(2): 201-220 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Ahmadpour N, Mohammadi B, Rabiei M. Effects of Plyometric, Balance, PNF and Combined Trainings on Basketball Players Ankle Muscle Activation. PTJ 2026; 16 (2) :201-220
URL: http://ptj.uswr.ac.ir/article-1-774-en.html
URL: http://ptj.uswr.ac.ir/article-1-774-en.html



1- Department of Sport Sciences, Faculty of Literature and Humanities, Shahrekord University, Shahrekord, Iran.
Keywords: Ankle muscle activation, Jump phase analysis, Basketball injury prevention, Combined training
Full-Text [PDF 730 kb]
(635 Downloads)
| Abstract (HTML) (1661 Views)
Full-Text: (89 Views)
Introduction
Basketball, a sport that has captivated millions around the world, has a rich and fascinating history [1]. Injuries are an inevitable aspect of sports, and basketball is no exception [2]. The physical demands and high-intensity nature of the game make basketball players susceptible to various types of injuries [3]. Ankle twists are a common occurrence in basketball, often resulting in significant pain and functional limitations for players [4]. Understanding the mechanism behind ankle twists is crucial for developing effective preventive measures and rehabilitation strategies [5]. Ankle injuries are common among basketball players and can lead to various problems for basketball players, affecting their performance, playing time, and long-term health [4]. Poor ankle stability is a significant risk factor for ankle injuries. Basketball players with weaker ankle muscles and ligaments are more prone to ankle sprains found that players with decreased ankle stability had a higher incidence of ankle injuries and players with a history of ankle sprains are more likely to experience recurrent ankle injuries [6]. Athletes have an increased risk of subsequent sprains [7]. Certain movement patterns, such as sudden changes in direction, jumping, and landing, can put stress on the ankle joint and increase the risk of injury [8]. Ankle injury prevention is crucial for basketball players to maintain their performance and reduce the risk of long-term complications and some trainings, such as plyometric and balance and proprioceptive neuromuscular facilitation (PNF), are effective [9]. Balance and proprioception exercises can improve ankle stability and reduce the risk of ankle injuries [10]. Board training program significantly reduced the incidence of ankle sprains among basketball players [11]. Strengthening the muscles around the ankle joint, including the calves, can provide better support and stability [12]. Strengthening exercises can be effective in reducing ankle injuries in basketball players [13]. PNF exercises include stretching exercises that are effective for improving range of motion, reducing spasms and accelerating recovery, designed based on natural patterns [14]. However, the same study indicated that PNF exercises do not have a significant effect on stimulus feedback time or ankle dorsiflexion strength [14]. A thorough warm-up routine that includes dynamic stretching exercises can help enhance flexibility and prepare the muscles for the demands of basketball [15]. Neglected or mismanaged ankle injuries can lead to long-term joint damage, such as osteoarthritis and continued stress, and instability in the ankle joint can accelerate joint degeneration, also ankle sprains were associated with an increased risk of developing ankle osteoarthritis in later life [16]. Ankle injuries can have psychological consequences, including fear of reinjury, decreased confidence, and psychological distress. Athletes may develop anxiety or apprehension related to returning to play after an ankle injury [17]. Given this, basketball is a sport with high risk of ankle injury, a com-parative training program is necessary to prevent ankle injury. This study aimed to investigate the electrical ac- tivity of the ankle muscles of basketball players between groups in the jumping test.
Objectives
This study evaluated the effectiveness of plyometric, balance, and PNF training protocols in preventing ankle injuries among 75 competitive basketball players, using electromyographic (EMG) analysis during single-leg jumps. The key findings demonstrated that plyometric training significantly reduced muscle activation in ankle stabilizers (particularly tibialis anterior (TA) and gastrocnemius) during critical jump phases. Balance training showed specific benefits, while PNF training exhibited no measurable effects. Crucially, the data revealed that a combined training protocol integrating all three methods produced superior outcomes in optimizing neuromuscular control and reducing injury-risk activation patterns across all jump phases. These results suggest that multimodal training interventions may offer the most effective strategy for ankle injury prevention in basketball. However, further longitudinal research is needed to validate these findings and establish optimal implementation protocols.
Materials and Methods
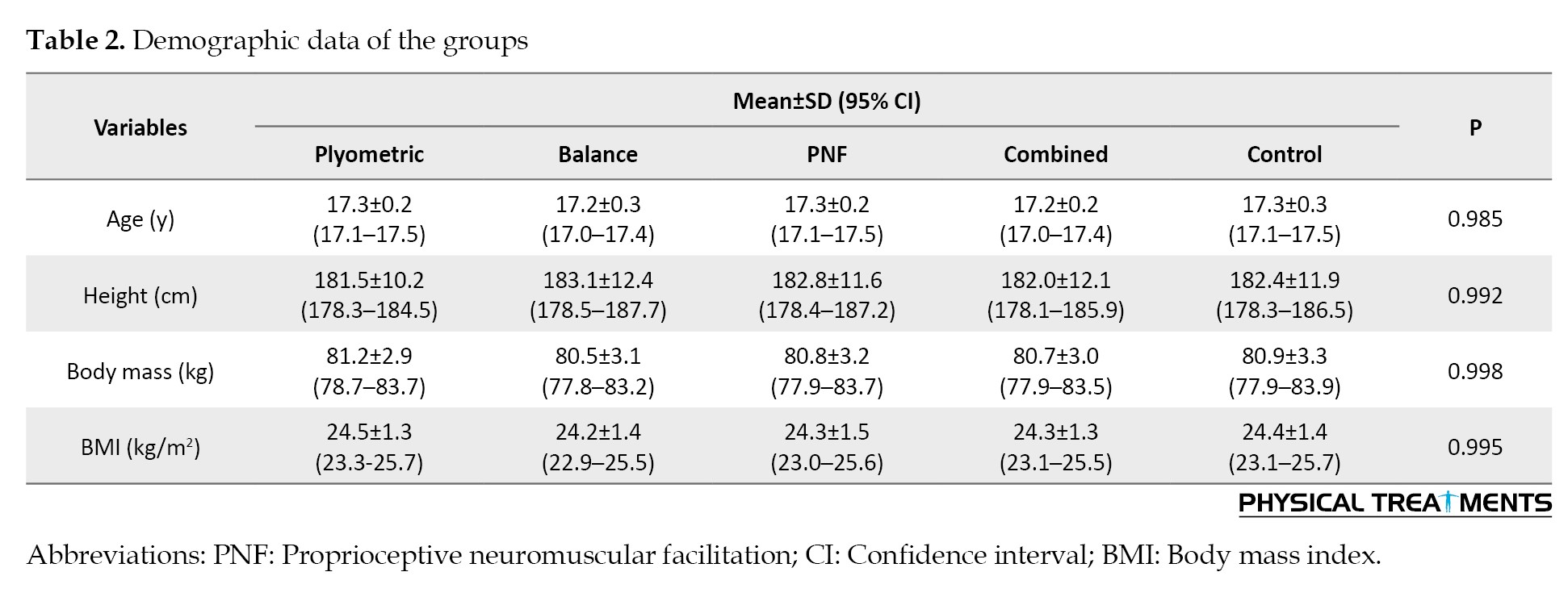
This study included 75 young male basketball players (aged 16-18 years) with at least two years of competitive basketball experience and no history of ankle injury. The participants (mean age 17.26±0.24 years; mean height 182.38±11.7 cm; mean body mass 80.82±3.04 kg; mean BMI 24.38±1.36 kg/m²) were from Shahrekord City, southwest Iran. All participants were right-hand and dominant-foot. They were randomly assigned to one of five training groups (n=15 per group): Plyometric, balance, PNF, combined (plyometric, balance, and PNF), and a control group (Table 1).
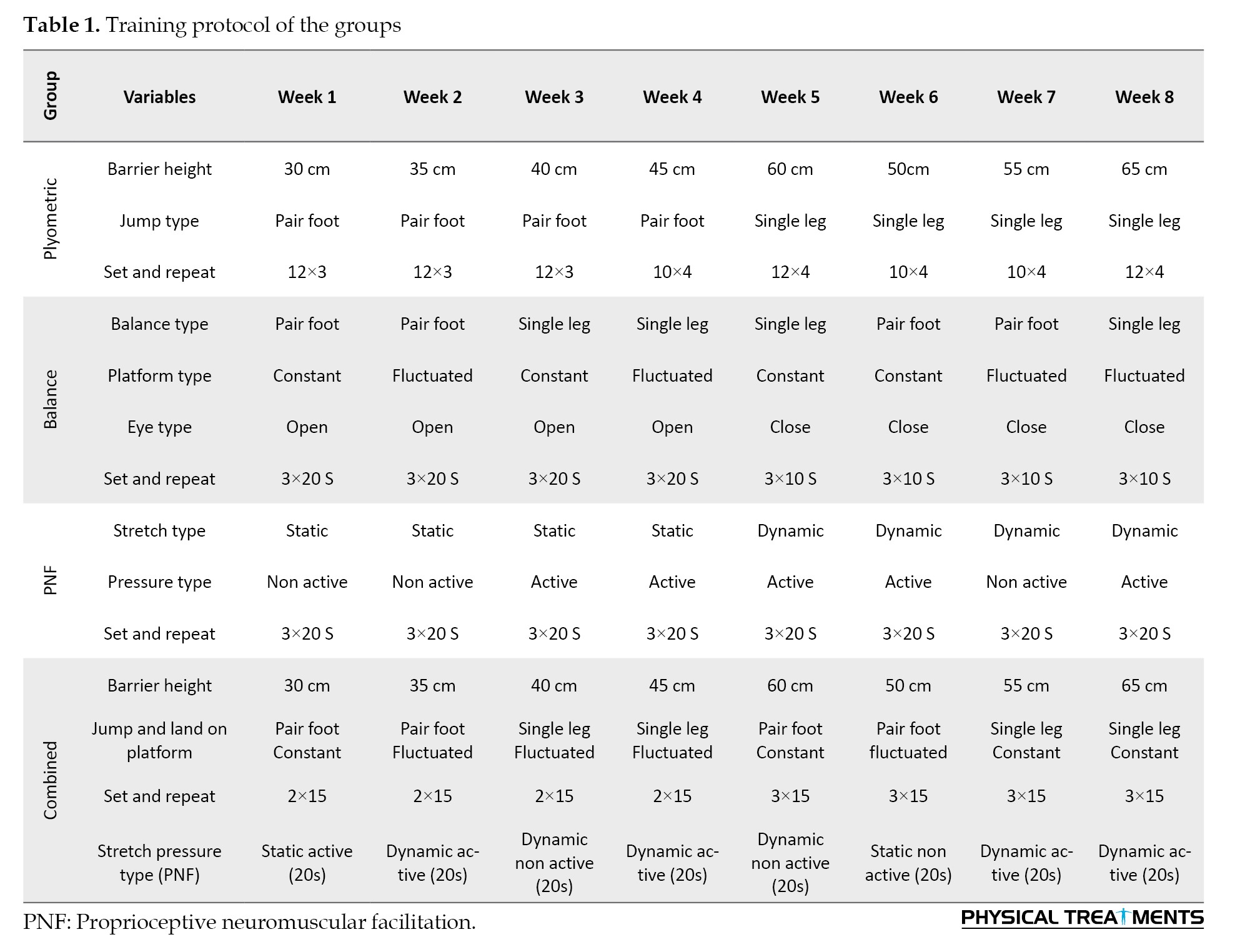
One-way analysis of variance (ANOVA) confirmed no significant baseline differences in demographic characteristics between the groups (P>0.05), ensuring group comparability at study initiation. The control group continued their standard basketball practice without any additional warm-up training. In contrast, the experimental groups incorporated their specific training protocols into their warm-up period before basketball training. These protocol trainings were applied consistently across the experimental groups and were optimized over the 8-week period [18] (Table 2).
Before the study commenced, the aims and procedures were explained to the participants. All participants voluntarily signed informed consent forms. The participants were also assured they could withdraw from the study whenever they wished. Following anthropometric measurements (age, height, weight, BMI), the researcher measured functional factors, including strength, endurance, power and range of motion as pre-tests. The experimental groups then performed one of the four training methods (plyometric, balance, PNF, or combination) for 30-45 minutes per session, alongside their regular skill exercises. These sessions took place three times per week for eight weeks. The researcher directly supervised the groups. The exercise program for the experimental groups adhered to the principle of overload with gradual increases in the duration and repetition of each exercise. According to the training program, plyometric exercises included double-leg and single-leg jumping exercises in length and height, and balance exercises included exercises for maintaining balance in pair-leg and single-leg positions with stable and unstable surfaces and with open eyes and close eyes positions also PNF training included stretching and pressure exercises at different levels and also combination training included plyometric, balance and PNF exercises. Exercises are progressed from an easy level to a hard level of intensity over the eight weeks according to the principle of overload. The control group performed their usual training sessions concurrently. Following the training period, the researcher measured functional factors in experimental and control groups as post-tests. This research recorded the muscle electrical activity using an 8-channel biofeedback electromyography device (pro-comp infiniti, canada) with a sampling rate of 2000 Hz [19]. The targeted muscles encompassed the TA, peroneus longus (PL), gastrocnemius medialis (GM), and soleus (SL) [20]. Before measuring the electrical activity of muscles, the following actions were taken (according to the SENIAM protocol): To capture muscle activity accurately, surface EMG electrodes were strategically placed over the targeted muscles. Common electrode placement protocols were followed, aligning with established guidelines for each muscle group. The muscles assessed included: TA, PL, gastrocnemius (media land lateral) and SL. Prior to electrode application, the skin was prepared to minimize impedance. This typically involved gentle abrasion and cleansing to ensure optimal electrode-skin contact, as recommended in literature on EMG procedures. Before initiating the test protocols, the EMG system underwent calibration procedures to establish a baseline for muscle activity. This step is crucial for accurate interpretation of EMG signals and is aligned with the standard practices in electromyography research. Participants were familiarized with the testing environment, and anthropometric measurements were taken to guide electrode placement. Informed consent was obtained, and ethical considerations were upheld throughout the study, in accordance with ethical guidelines. After preparation and setup of the measurement equipment, maximal voluntary isometric contractions (MVIC) of the ankle muscles were measured. Subsequently, subjects performed the single jump test with their dominant (right) foot from a 30 cm box [21]. Following the After the pre-test assessment, the experimental groups performed plyometric, balance, PNF and combined exercises (plyometric and balance and PNF) in addition to basketball exercises. The control group continued with only basketball exercises [22]. For a more accurate assessment, the jump test was divided into four different phases. The activity of each muscle in each phase was examined between five training groups. These phases are defined as follows [23]: The first phase of jumping refers to the distance between maintaining balance and the command of the examinee until the first contraction of the target muscles before jumping; the second phase of jumping is the interval between the first contraction of the ankle muscles before jumping and the separation of the toe and heel from the ground; the third phase of jumping or the swing phase is the distance between the separation of the toe and heel from the ground to the first contact of the foot with the surface after jumping; and the fourth phase of jumping is the distance between the first contact of the foot with the surface and the complete landing and maintaining balance [24]. Following the jump tests, the root mean square (RMS) value for each muscle’s activity during each phase was calculated for both pre-test and post-test. These RMS values were normalized to the MVIC of each respective muscle, expressed as a percentage. This allowed for the examination and measurement of muscle activation percentages across all four phases in both pre-test and post-test conditions [25]. Participants performed the single-leg jump-and-land task, replicating real-world scenarios and the EMG system recorded muscle activity throughout the task, capturing data on the targeted muscles during takeoff, flight, and landing phases [26]. The single-leg box jump test was systematically analyzed across four biomechanically defined phases: 1) Initial contact phase (0–100 ms after ground contact), characterized by rapid impact absorption with eccentric muscle activation; 2) Braking phase (from initial contact to peak knee flexion, typically 100–300 ms), where muscles decelerate downward momentum; 3) Propulsion phase (from peak knee flexion to toe-off, 300–500 ms), dominated by concentric activation for upward acceleration; and 4) Stabilization phase (first 200 ms after landing on the box), requiring dynamic control to maintain balance. EMG signals were segmented into these phases using kinematic (motion capture) and kinetic (force plate) triggers, with RMS amplitude calculated for each phase to quantify phase-specific neuromuscular adaptations [26]. EMG signals were continuously recorded during the entire test using a synchronized data acquisition system. Signal processing techniques, such as filtering and normalization, were applied to enhance the accuracy of the recorded [27]. Collected data underwent rigorous analysis using established algorithms. Muscle activation patterns, onset, and offset times were extracted for each targeted muscle, allowing for a detailed examination of neuromuscular responses [28]. Statistical methods, including paired t-tests or ANOVA, were employed to assess significant differences in muscle activation patterns between pre-test and post-test conditions [29]. This analytical approach aligns with recommended statistical practices in EMG research.
Results
In this part, research hypotheses were tested using statistics and SPSS software, version 21. A paired t-test was used to compare the pre-test and post-test scores of each group, and the ANOVA statistical test was used to compare the changes across the five training groups over the intervention period. Differences in muscle electrical activity in the jumping phases were analyzed based on the absolute value of the normalized differences (Figures 1, 2, 3, 4 and 5).
Basketball, a sport that has captivated millions around the world, has a rich and fascinating history [1]. Injuries are an inevitable aspect of sports, and basketball is no exception [2]. The physical demands and high-intensity nature of the game make basketball players susceptible to various types of injuries [3]. Ankle twists are a common occurrence in basketball, often resulting in significant pain and functional limitations for players [4]. Understanding the mechanism behind ankle twists is crucial for developing effective preventive measures and rehabilitation strategies [5]. Ankle injuries are common among basketball players and can lead to various problems for basketball players, affecting their performance, playing time, and long-term health [4]. Poor ankle stability is a significant risk factor for ankle injuries. Basketball players with weaker ankle muscles and ligaments are more prone to ankle sprains found that players with decreased ankle stability had a higher incidence of ankle injuries and players with a history of ankle sprains are more likely to experience recurrent ankle injuries [6]. Athletes have an increased risk of subsequent sprains [7]. Certain movement patterns, such as sudden changes in direction, jumping, and landing, can put stress on the ankle joint and increase the risk of injury [8]. Ankle injury prevention is crucial for basketball players to maintain their performance and reduce the risk of long-term complications and some trainings, such as plyometric and balance and proprioceptive neuromuscular facilitation (PNF), are effective [9]. Balance and proprioception exercises can improve ankle stability and reduce the risk of ankle injuries [10]. Board training program significantly reduced the incidence of ankle sprains among basketball players [11]. Strengthening the muscles around the ankle joint, including the calves, can provide better support and stability [12]. Strengthening exercises can be effective in reducing ankle injuries in basketball players [13]. PNF exercises include stretching exercises that are effective for improving range of motion, reducing spasms and accelerating recovery, designed based on natural patterns [14]. However, the same study indicated that PNF exercises do not have a significant effect on stimulus feedback time or ankle dorsiflexion strength [14]. A thorough warm-up routine that includes dynamic stretching exercises can help enhance flexibility and prepare the muscles for the demands of basketball [15]. Neglected or mismanaged ankle injuries can lead to long-term joint damage, such as osteoarthritis and continued stress, and instability in the ankle joint can accelerate joint degeneration, also ankle sprains were associated with an increased risk of developing ankle osteoarthritis in later life [16]. Ankle injuries can have psychological consequences, including fear of reinjury, decreased confidence, and psychological distress. Athletes may develop anxiety or apprehension related to returning to play after an ankle injury [17]. Given this, basketball is a sport with high risk of ankle injury, a com-parative training program is necessary to prevent ankle injury. This study aimed to investigate the electrical ac- tivity of the ankle muscles of basketball players between groups in the jumping test.
Objectives
This study evaluated the effectiveness of plyometric, balance, and PNF training protocols in preventing ankle injuries among 75 competitive basketball players, using electromyographic (EMG) analysis during single-leg jumps. The key findings demonstrated that plyometric training significantly reduced muscle activation in ankle stabilizers (particularly tibialis anterior (TA) and gastrocnemius) during critical jump phases. Balance training showed specific benefits, while PNF training exhibited no measurable effects. Crucially, the data revealed that a combined training protocol integrating all three methods produced superior outcomes in optimizing neuromuscular control and reducing injury-risk activation patterns across all jump phases. These results suggest that multimodal training interventions may offer the most effective strategy for ankle injury prevention in basketball. However, further longitudinal research is needed to validate these findings and establish optimal implementation protocols.
Materials and Methods
This study included 75 young male basketball players (aged 16-18 years) with at least two years of competitive basketball experience and no history of ankle injury. The participants (mean age 17.26±0.24 years; mean height 182.38±11.7 cm; mean body mass 80.82±3.04 kg; mean BMI 24.38±1.36 kg/m²) were from Shahrekord City, southwest Iran. All participants were right-hand and dominant-foot. They were randomly assigned to one of five training groups (n=15 per group): Plyometric, balance, PNF, combined (plyometric, balance, and PNF), and a control group (Table 1).
One-way analysis of variance (ANOVA) confirmed no significant baseline differences in demographic characteristics between the groups (P>0.05), ensuring group comparability at study initiation. The control group continued their standard basketball practice without any additional warm-up training. In contrast, the experimental groups incorporated their specific training protocols into their warm-up period before basketball training. These protocol trainings were applied consistently across the experimental groups and were optimized over the 8-week period [18] (Table 2).
Before the study commenced, the aims and procedures were explained to the participants. All participants voluntarily signed informed consent forms. The participants were also assured they could withdraw from the study whenever they wished. Following anthropometric measurements (age, height, weight, BMI), the researcher measured functional factors, including strength, endurance, power and range of motion as pre-tests. The experimental groups then performed one of the four training methods (plyometric, balance, PNF, or combination) for 30-45 minutes per session, alongside their regular skill exercises. These sessions took place three times per week for eight weeks. The researcher directly supervised the groups. The exercise program for the experimental groups adhered to the principle of overload with gradual increases in the duration and repetition of each exercise. According to the training program, plyometric exercises included double-leg and single-leg jumping exercises in length and height, and balance exercises included exercises for maintaining balance in pair-leg and single-leg positions with stable and unstable surfaces and with open eyes and close eyes positions also PNF training included stretching and pressure exercises at different levels and also combination training included plyometric, balance and PNF exercises. Exercises are progressed from an easy level to a hard level of intensity over the eight weeks according to the principle of overload. The control group performed their usual training sessions concurrently. Following the training period, the researcher measured functional factors in experimental and control groups as post-tests. This research recorded the muscle electrical activity using an 8-channel biofeedback electromyography device (pro-comp infiniti, canada) with a sampling rate of 2000 Hz [19]. The targeted muscles encompassed the TA, peroneus longus (PL), gastrocnemius medialis (GM), and soleus (SL) [20]. Before measuring the electrical activity of muscles, the following actions were taken (according to the SENIAM protocol): To capture muscle activity accurately, surface EMG electrodes were strategically placed over the targeted muscles. Common electrode placement protocols were followed, aligning with established guidelines for each muscle group. The muscles assessed included: TA, PL, gastrocnemius (media land lateral) and SL. Prior to electrode application, the skin was prepared to minimize impedance. This typically involved gentle abrasion and cleansing to ensure optimal electrode-skin contact, as recommended in literature on EMG procedures. Before initiating the test protocols, the EMG system underwent calibration procedures to establish a baseline for muscle activity. This step is crucial for accurate interpretation of EMG signals and is aligned with the standard practices in electromyography research. Participants were familiarized with the testing environment, and anthropometric measurements were taken to guide electrode placement. Informed consent was obtained, and ethical considerations were upheld throughout the study, in accordance with ethical guidelines. After preparation and setup of the measurement equipment, maximal voluntary isometric contractions (MVIC) of the ankle muscles were measured. Subsequently, subjects performed the single jump test with their dominant (right) foot from a 30 cm box [21]. Following the After the pre-test assessment, the experimental groups performed plyometric, balance, PNF and combined exercises (plyometric and balance and PNF) in addition to basketball exercises. The control group continued with only basketball exercises [22]. For a more accurate assessment, the jump test was divided into four different phases. The activity of each muscle in each phase was examined between five training groups. These phases are defined as follows [23]: The first phase of jumping refers to the distance between maintaining balance and the command of the examinee until the first contraction of the target muscles before jumping; the second phase of jumping is the interval between the first contraction of the ankle muscles before jumping and the separation of the toe and heel from the ground; the third phase of jumping or the swing phase is the distance between the separation of the toe and heel from the ground to the first contact of the foot with the surface after jumping; and the fourth phase of jumping is the distance between the first contact of the foot with the surface and the complete landing and maintaining balance [24]. Following the jump tests, the root mean square (RMS) value for each muscle’s activity during each phase was calculated for both pre-test and post-test. These RMS values were normalized to the MVIC of each respective muscle, expressed as a percentage. This allowed for the examination and measurement of muscle activation percentages across all four phases in both pre-test and post-test conditions [25]. Participants performed the single-leg jump-and-land task, replicating real-world scenarios and the EMG system recorded muscle activity throughout the task, capturing data on the targeted muscles during takeoff, flight, and landing phases [26]. The single-leg box jump test was systematically analyzed across four biomechanically defined phases: 1) Initial contact phase (0–100 ms after ground contact), characterized by rapid impact absorption with eccentric muscle activation; 2) Braking phase (from initial contact to peak knee flexion, typically 100–300 ms), where muscles decelerate downward momentum; 3) Propulsion phase (from peak knee flexion to toe-off, 300–500 ms), dominated by concentric activation for upward acceleration; and 4) Stabilization phase (first 200 ms after landing on the box), requiring dynamic control to maintain balance. EMG signals were segmented into these phases using kinematic (motion capture) and kinetic (force plate) triggers, with RMS amplitude calculated for each phase to quantify phase-specific neuromuscular adaptations [26]. EMG signals were continuously recorded during the entire test using a synchronized data acquisition system. Signal processing techniques, such as filtering and normalization, were applied to enhance the accuracy of the recorded [27]. Collected data underwent rigorous analysis using established algorithms. Muscle activation patterns, onset, and offset times were extracted for each targeted muscle, allowing for a detailed examination of neuromuscular responses [28]. Statistical methods, including paired t-tests or ANOVA, were employed to assess significant differences in muscle activation patterns between pre-test and post-test conditions [29]. This analytical approach aligns with recommended statistical practices in EMG research.
Results
In this part, research hypotheses were tested using statistics and SPSS software, version 21. A paired t-test was used to compare the pre-test and post-test scores of each group, and the ANOVA statistical test was used to compare the changes across the five training groups over the intervention period. Differences in muscle electrical activity in the jumping phases were analyzed based on the absolute value of the normalized differences (Figures 1, 2, 3, 4 and 5).
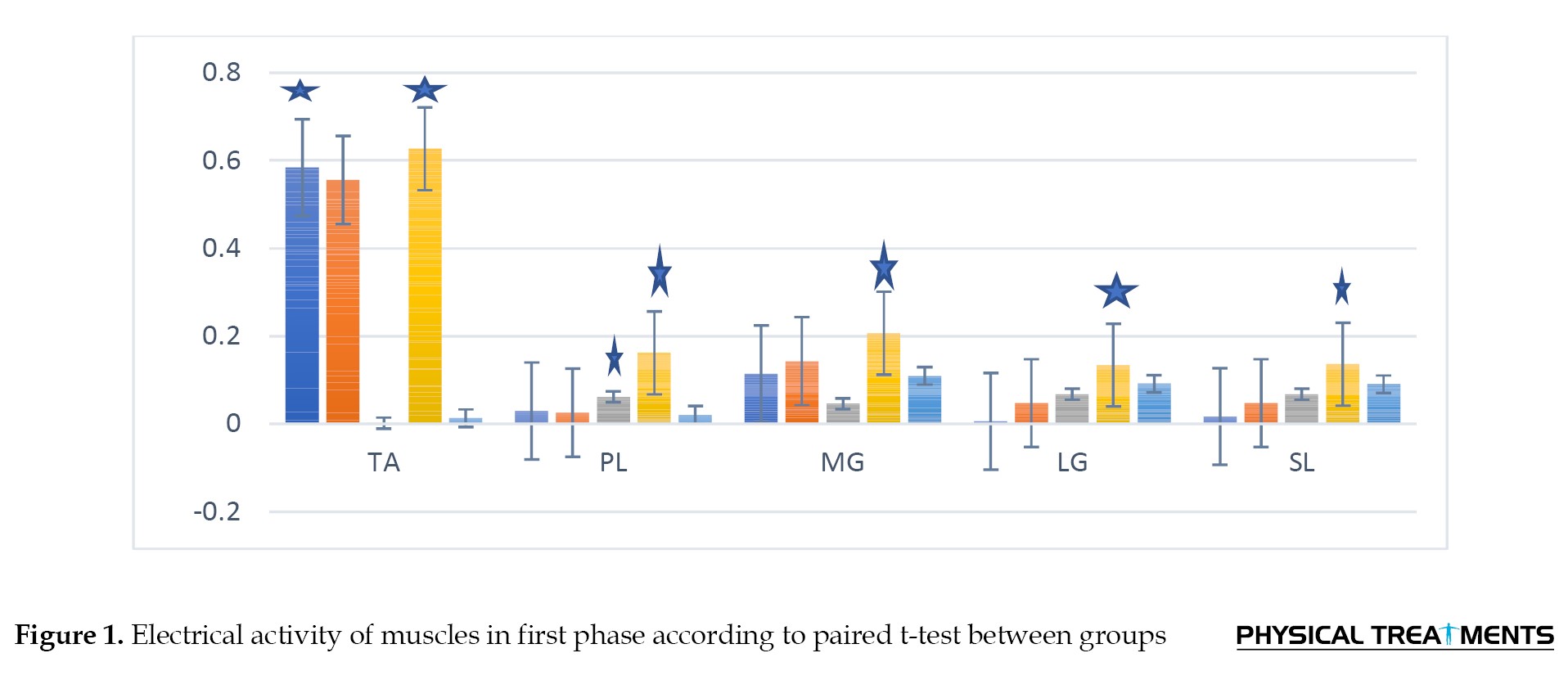
Paired t-test results indicated that combined training significantly affected the activity of TA, PL, medial and lateral GM, and SL muscles during the first jumping phase, demonstrating a more pronounced effect compared to other interventions. Exercise showed more and better effect in the first phase of jumping. In addition, plyometric training significantly affected TA muscle activity, and PNF training had a significant effect on PL muscle activity (Table 3) (P<0.05).
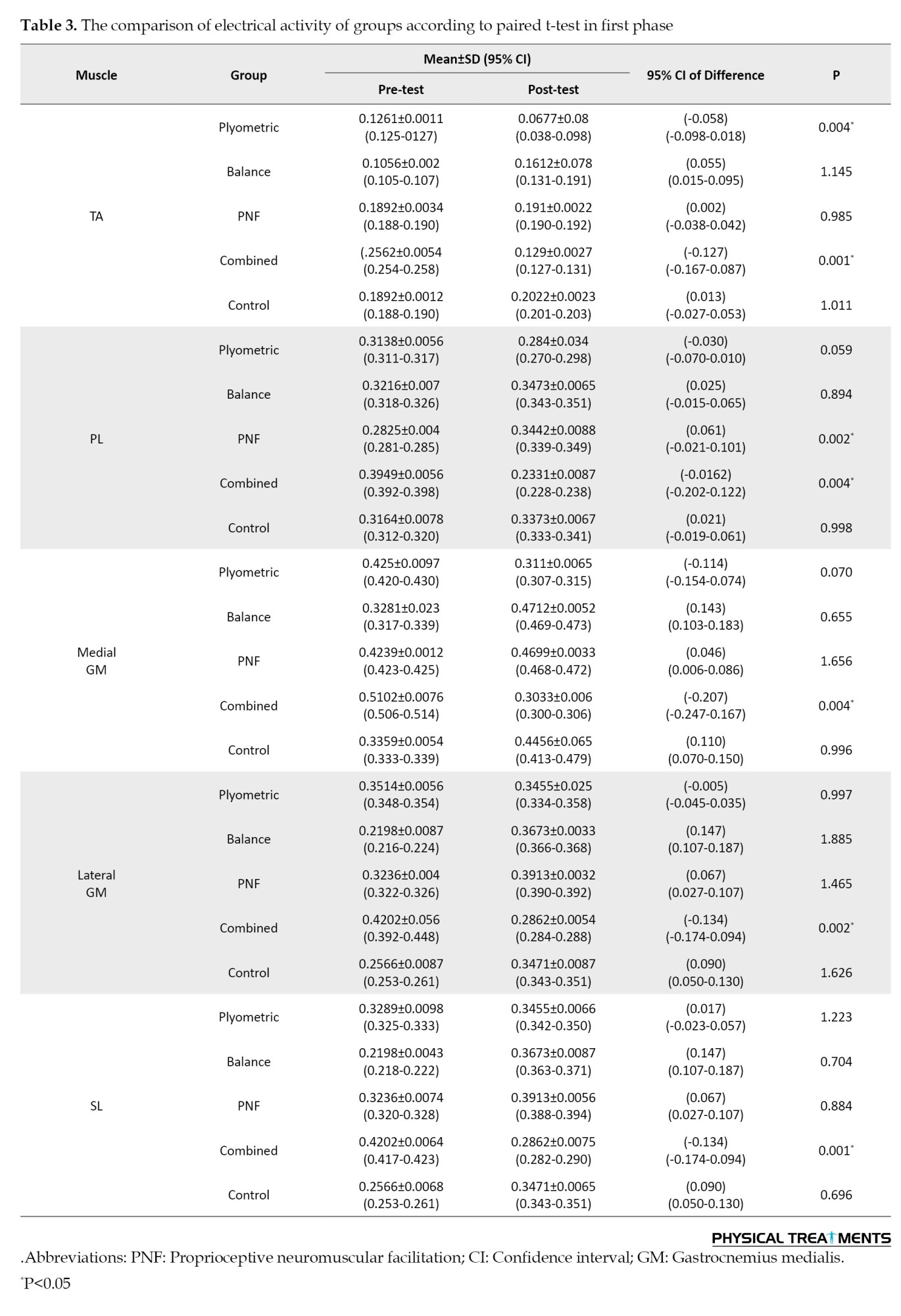
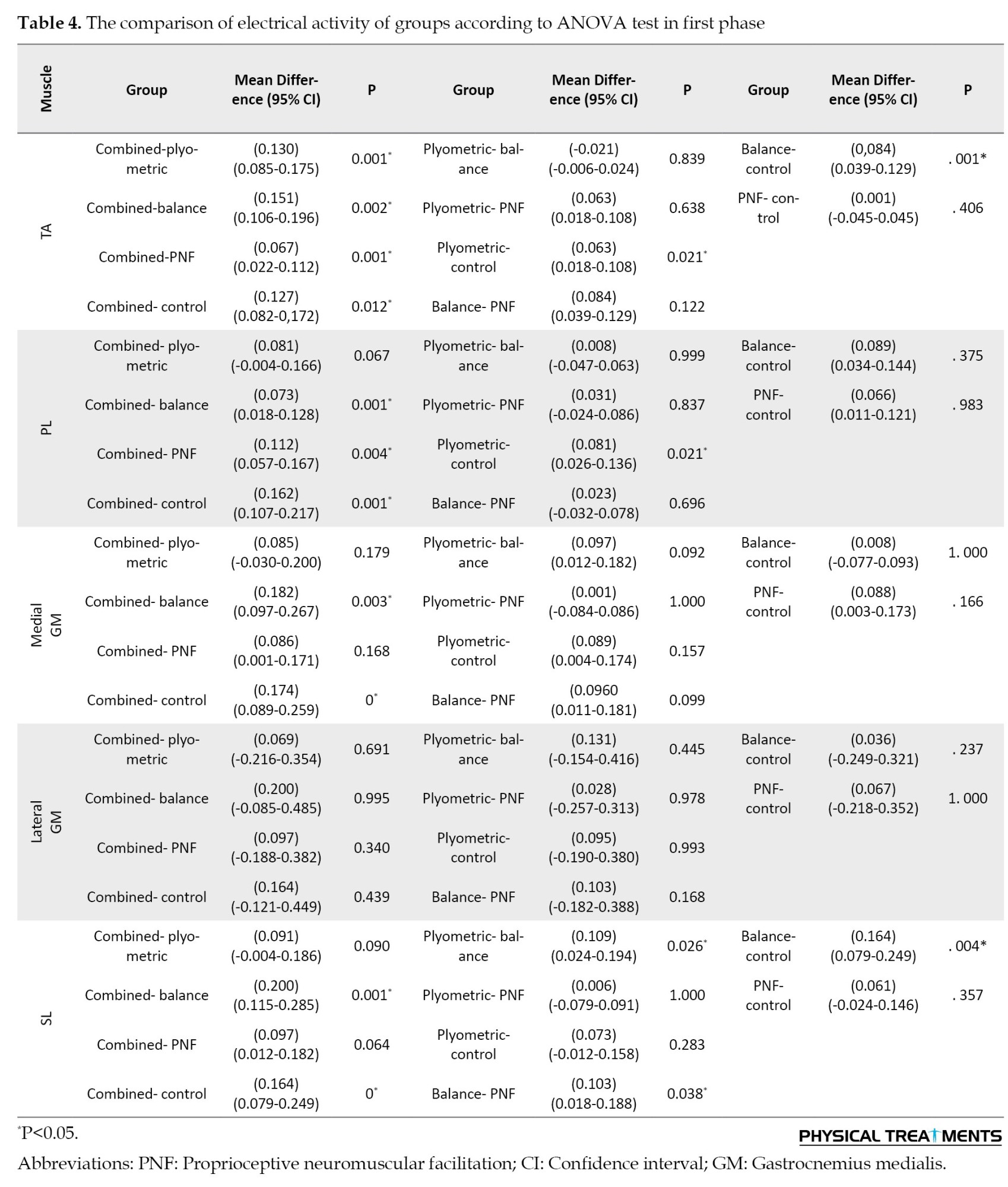
The results of ANOVA test showed significant differences in TA muscle activity during the first jumping phase between the plyometric, balance, and combined groups compared to the control group. In addition, significant differences were observed between combined training group with the plyometric, balance, and PNF groups. In the PL muscle, significant differences were observed between the plyometric and control group, and between the combined training group and both the balance and control groups. In the medial GM muscle, a significant difference was found between the combined with balance and control groups. No significant difference was observed in the lateral GM muscle between groups. In the SL muscle, significant differences were observed between balance with control and PNF groups. Additionally, differences were found between the plyometric group and both the balance and control group. Finally, a significant difference was observed between combined with balance and control groups (Table 4) (P<0.05).
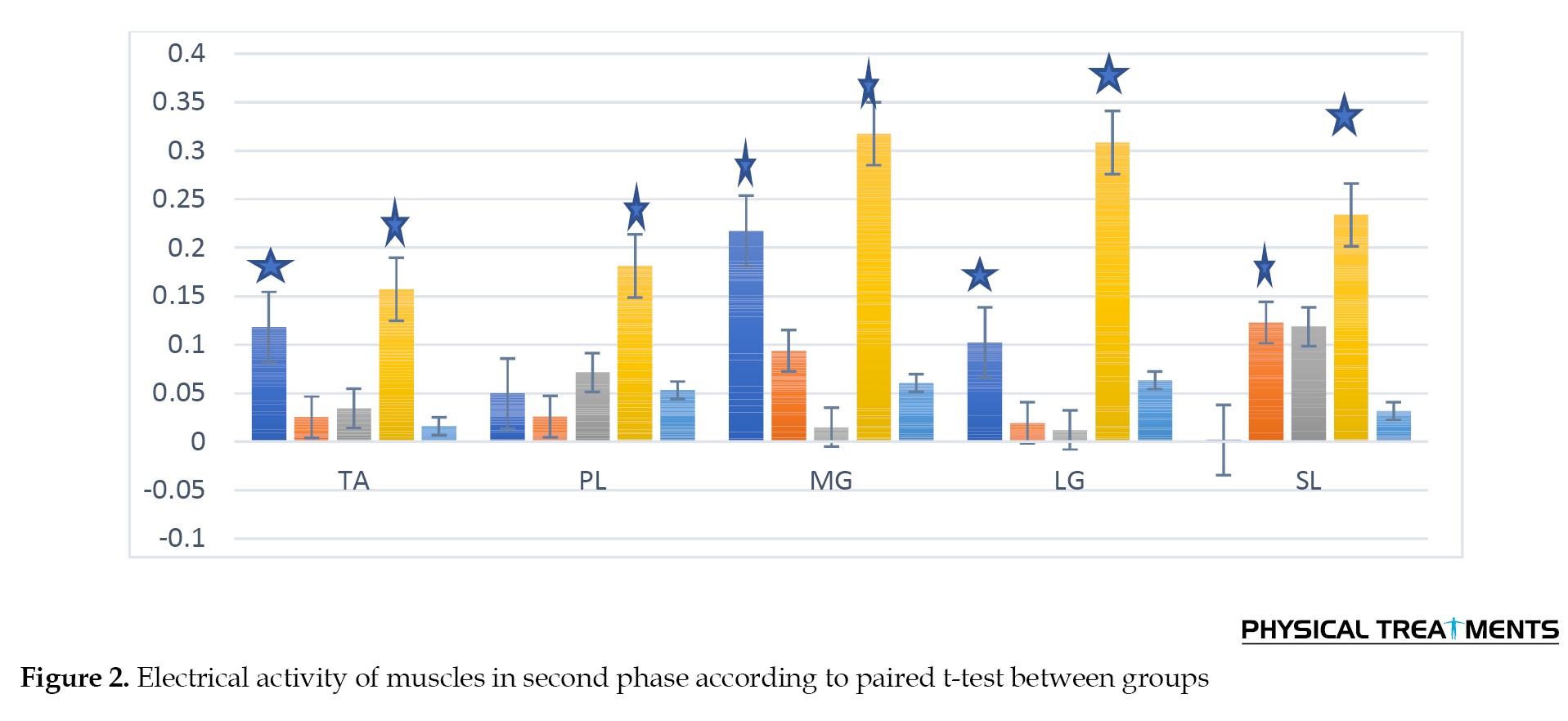
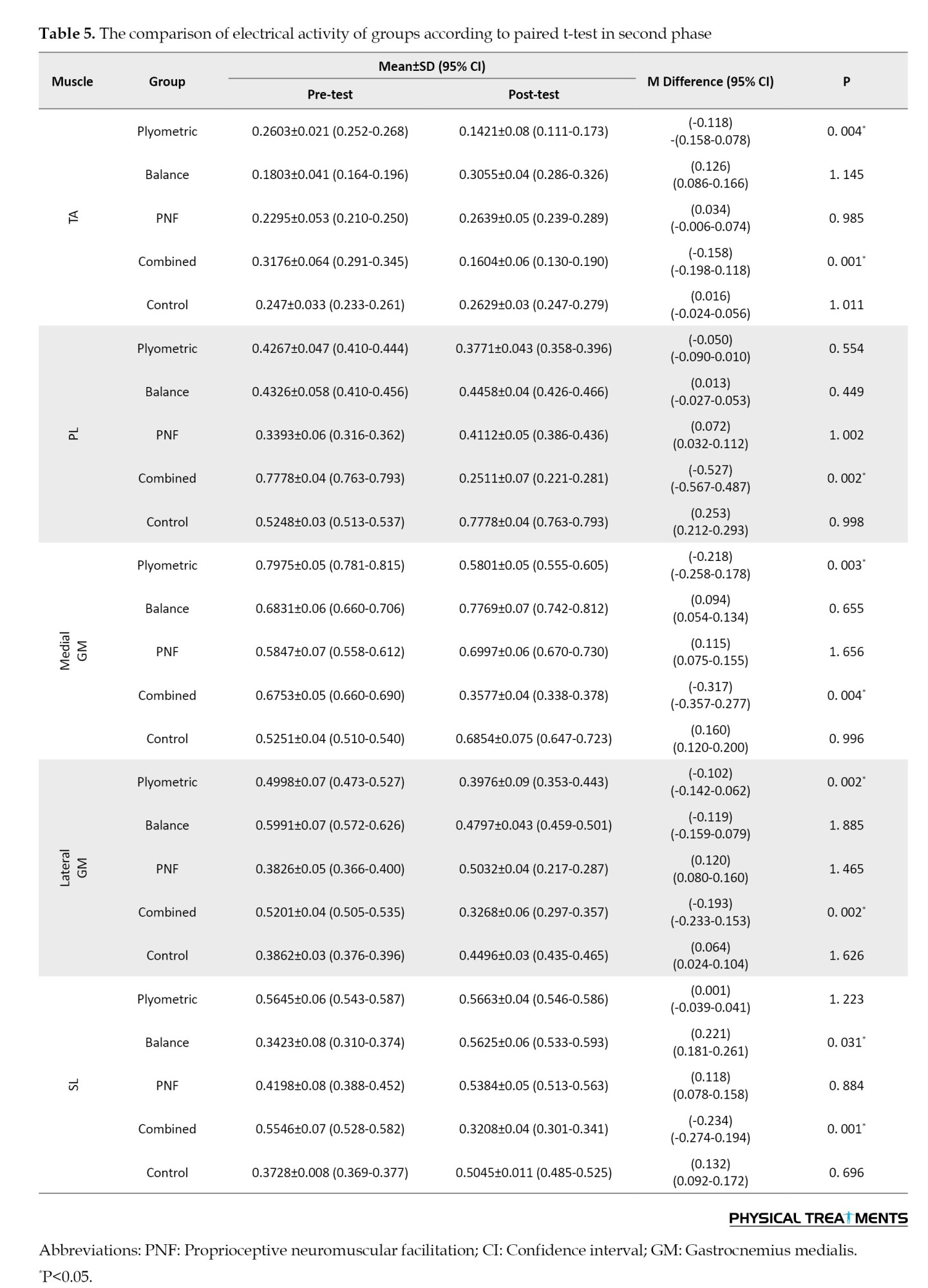
Paired t-test results indicated that combined exercises significantly affected all five ankle muscles during the second jumping phase. Furthermore, plyometric training significantly affected the TA and both medial and lateral GM muscles. Balance training significantly affected the SL muscle, whereas PNF training showed no significant effect on any of the studied muscles (Table 5) (P<0.05).
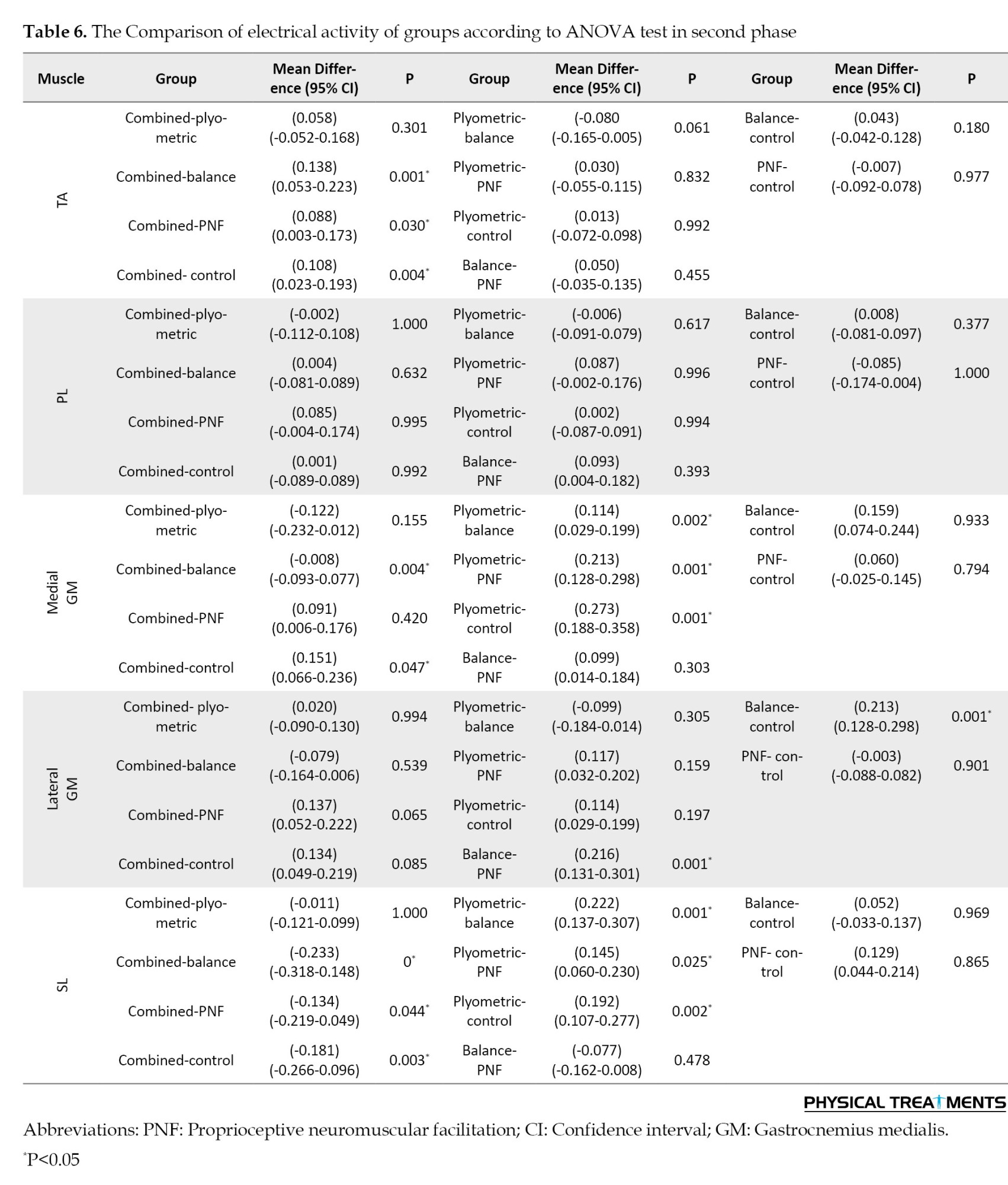
According to the ANOVA test, in the TA, differences were observed between the combined group and the balance, PNF, and control groups. No significant differences were observed in the PL muscle between any groups. In the medial GM muscle, significant differences were observed between the combined group and both the balance and control groups. Additionally, differences were observed between the plyometrics group and the balance, PNF, and control groups. In the lateral GM muscle, a difference was observed between the balance group and both the PNF and control groups. In the SL muscle, differences were observed between the combined group and the balance, PNF, and control groups. Furthermore, differences were observed between plyometrics training group and balance, PNF, and control groups (Table 6) (P<0.05).
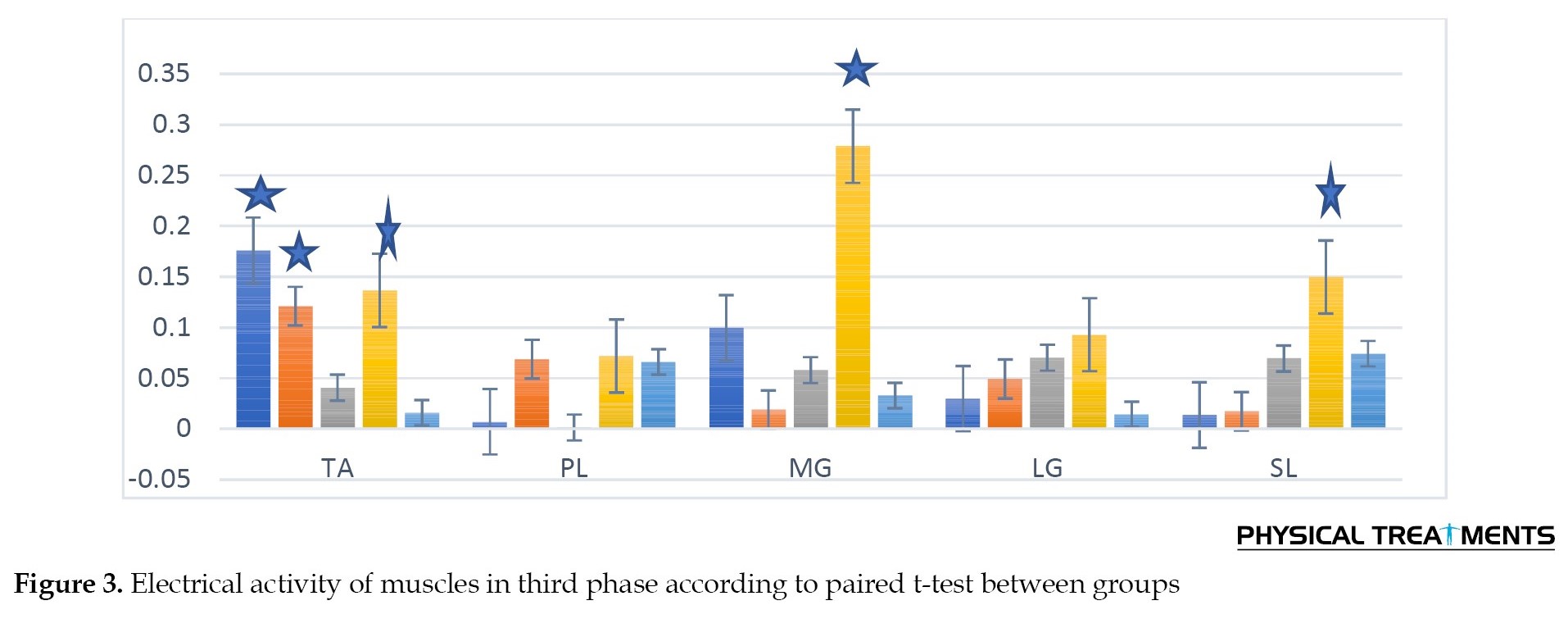
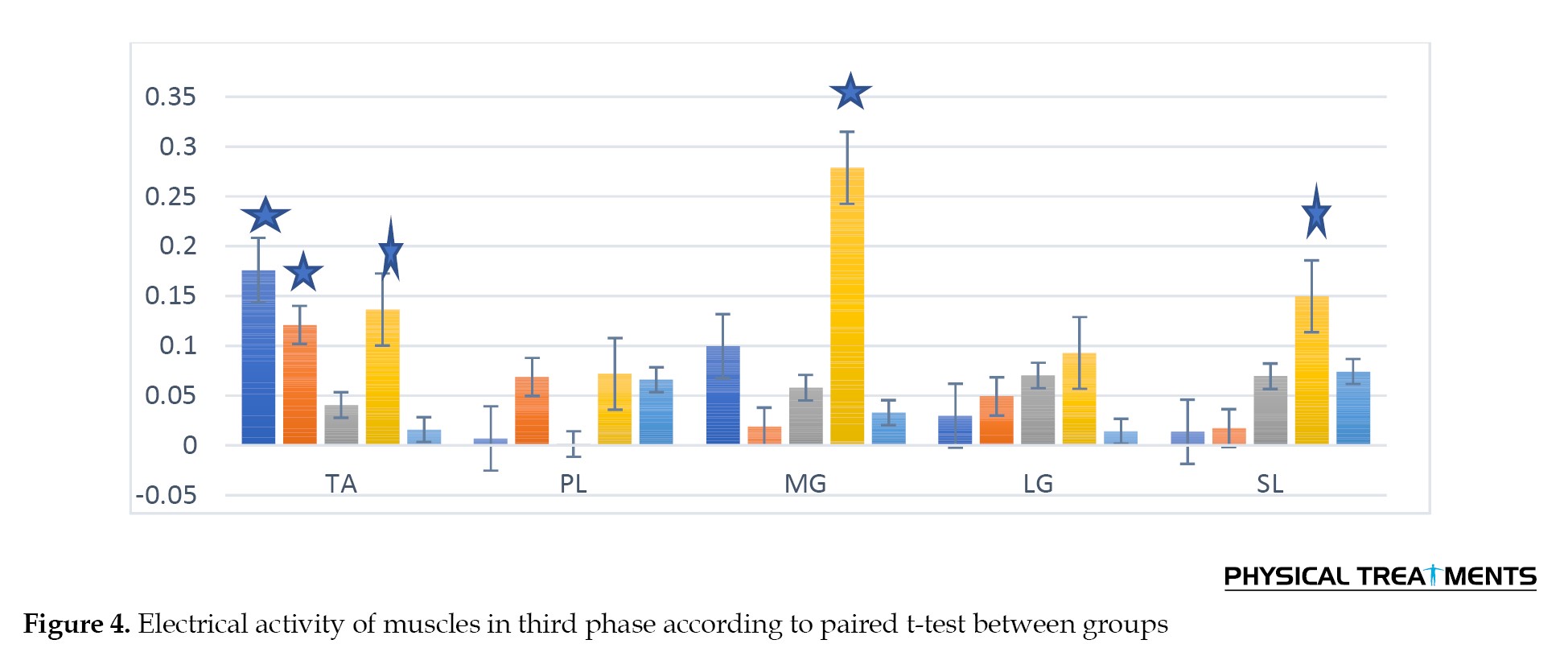
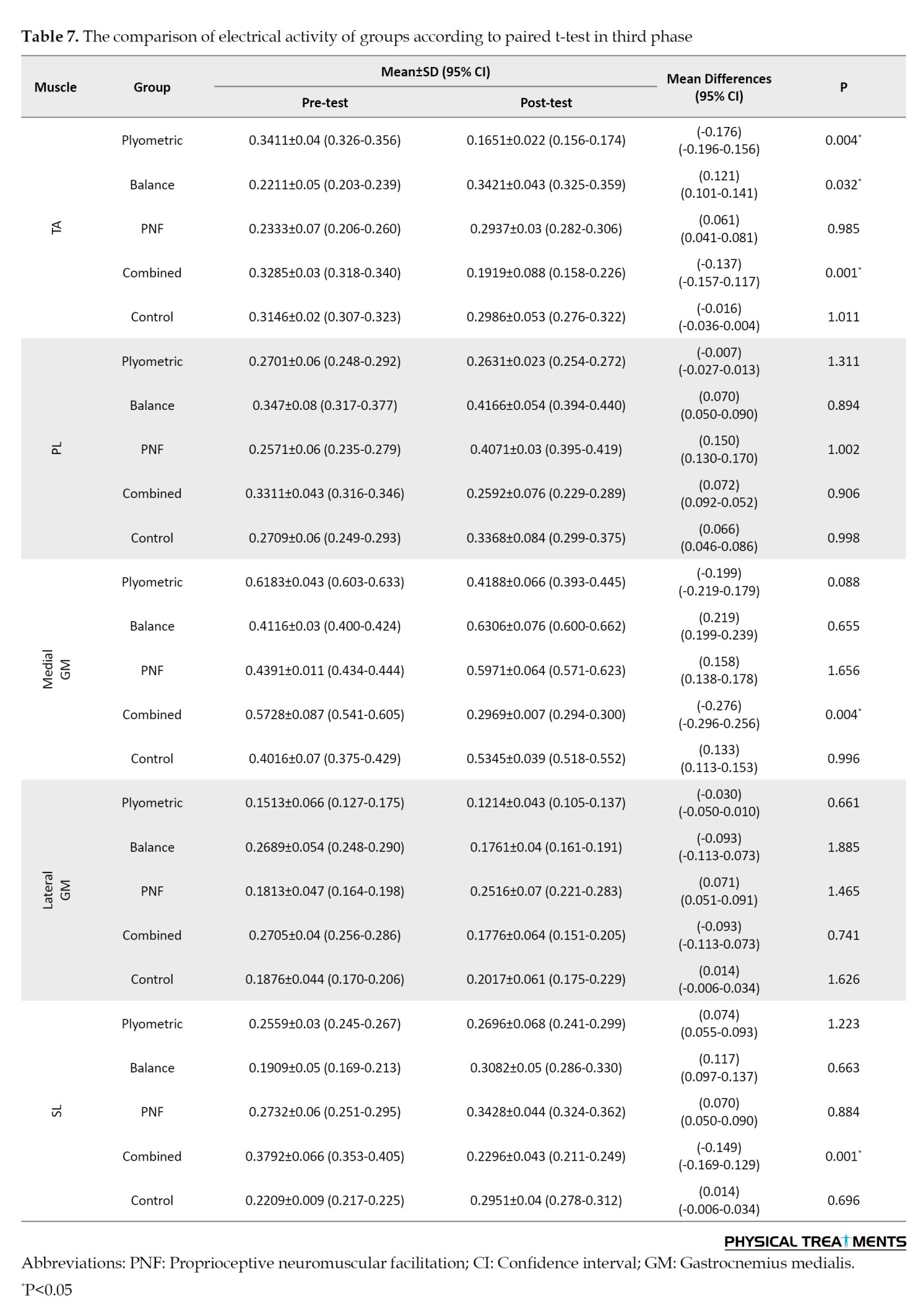
According to the results of the paired t-test for intra-group comparisons, it can be concluded that in the third phase of jumping, combined training had an effect on the TA, medial GM and SL muscles, as well as plyometric and balance trainings had significant effect on the TA muscle (Table 7) (P<0.05).
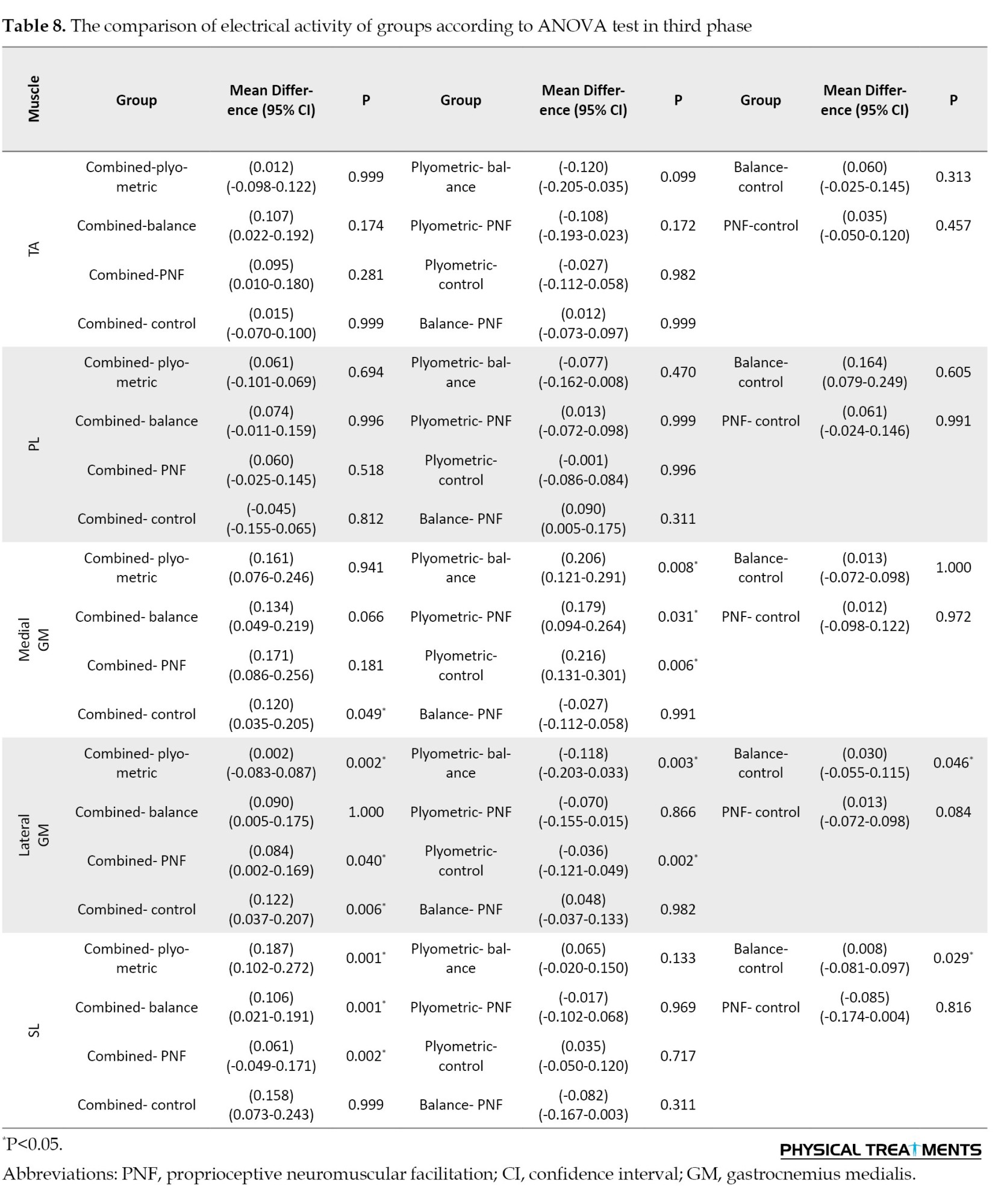
The results of ANOVA test showed a difference in the medial GM muscle between the plyometric with balance, PNF and control groups. Furthermore, a difference was observed between the combined group and the control group. The lateral GM muscle demonstrated a significant difference between the combined group and the plyometric, PNF, and control groups. A significant difference was observed between the balance group and the control group, as well as between the plyometric group and the control group. A significant difference was observed in the SL muscle between the combined group and all other groups (Table 8) (P<0.05).
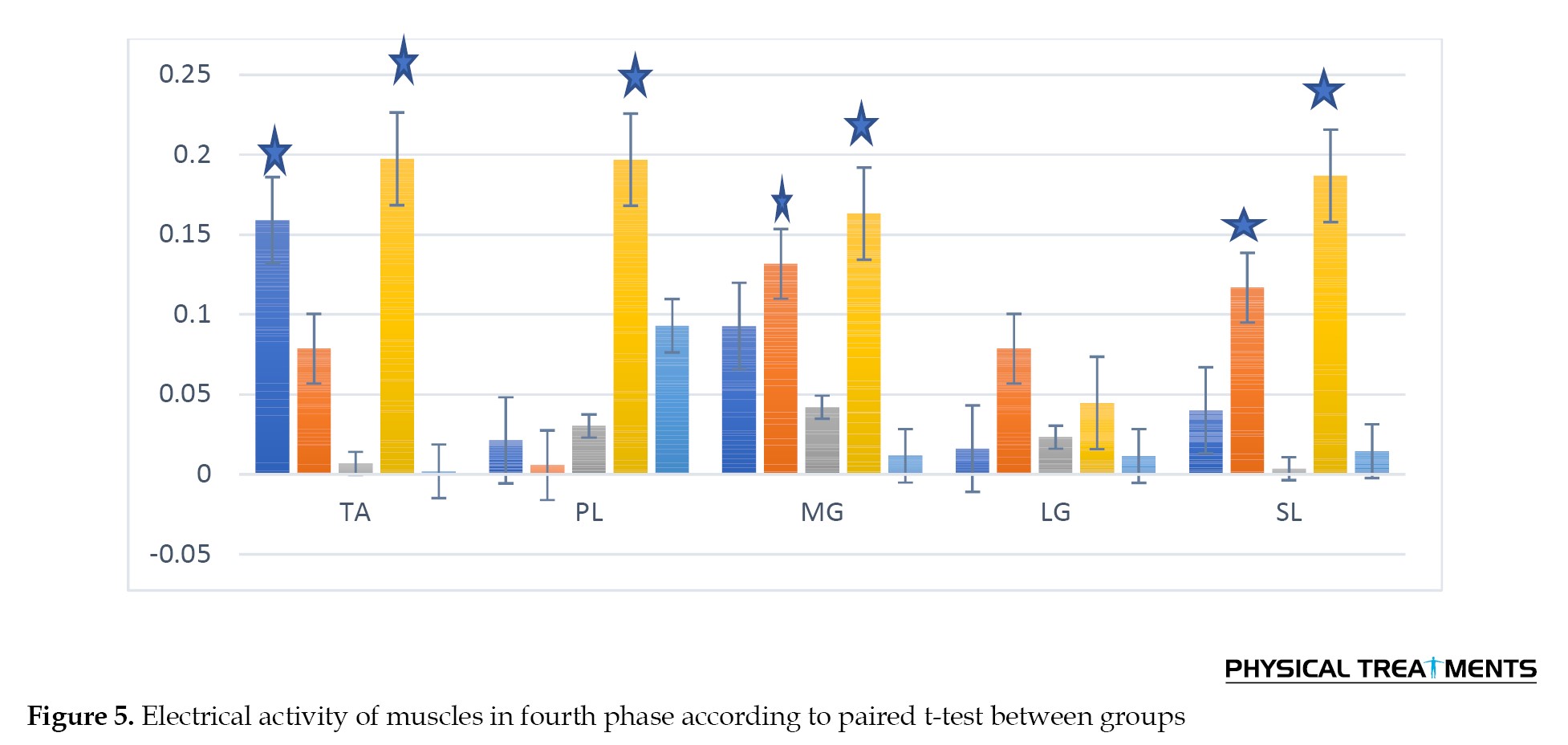
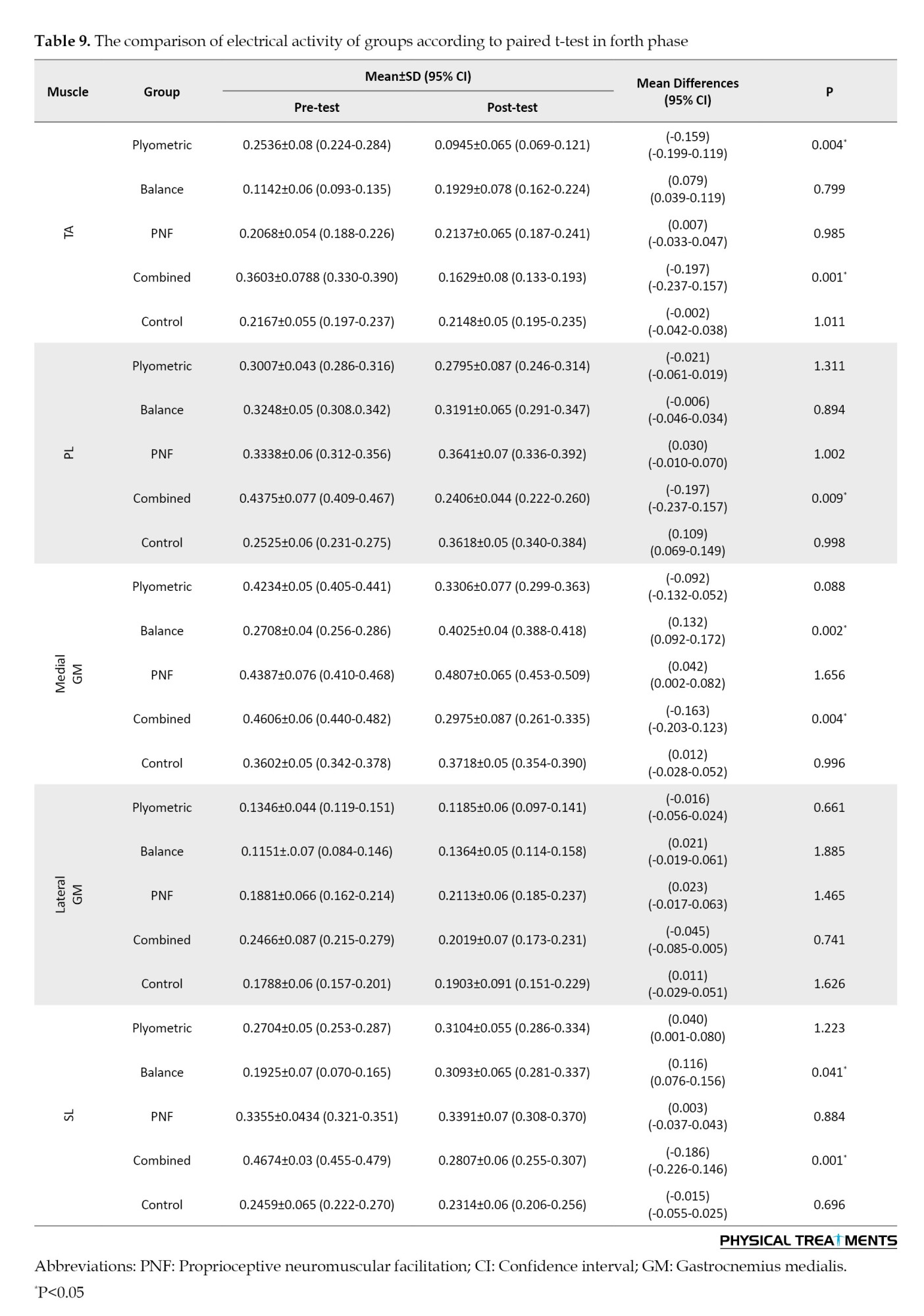
According to the results of the paired t-test for intra-group comparisons, combined training significantly affected the TA, PL, medial GM, and SL muscles during the fourth jumping phase. Additionally, plyometric training affected the TA muscle, and balance training impacted the medial GM and SL muscle (Table 9) (P<0.05).
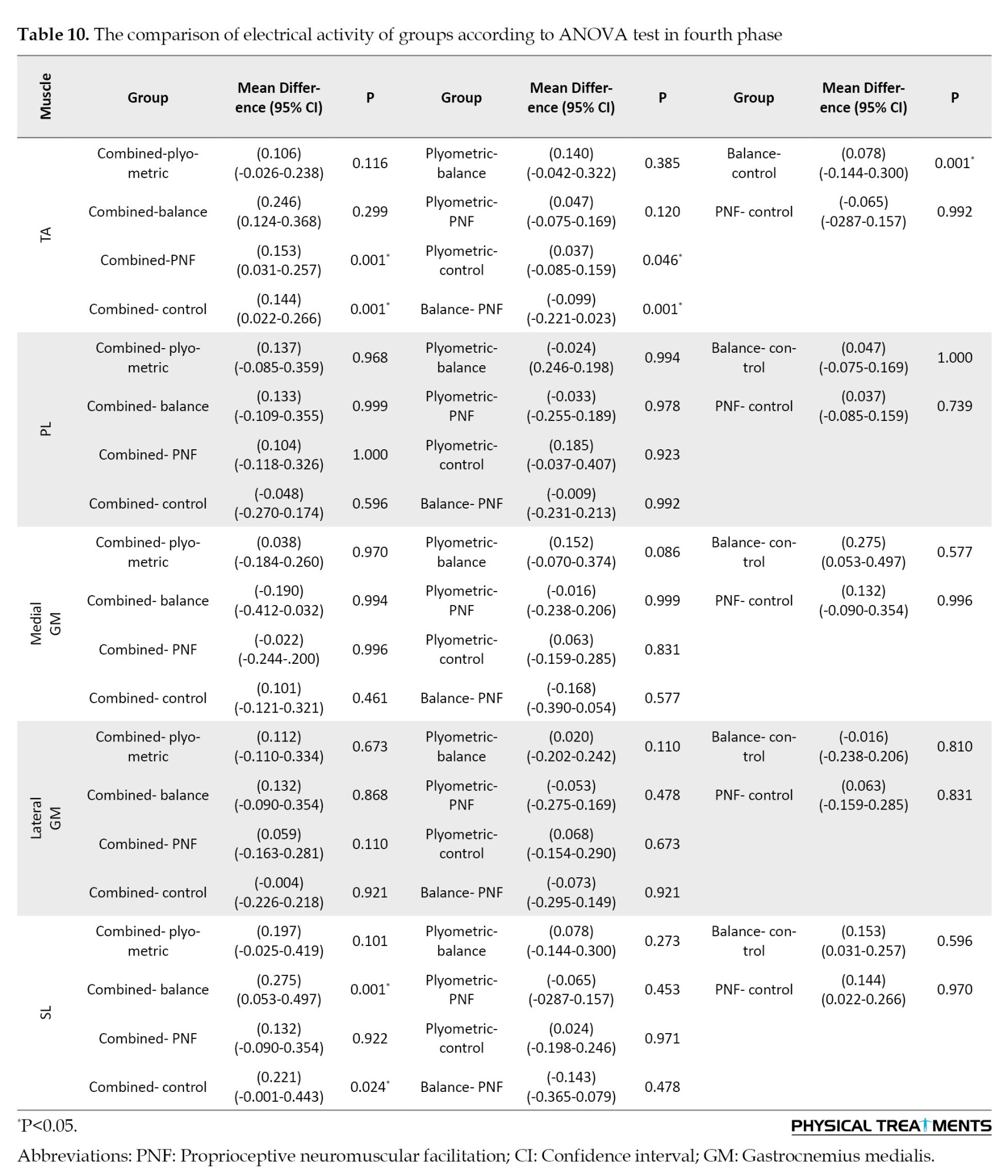
The results of ANOVA test showed a difference in the anterior large muscle between the combined group, and the PNF and control groups. Also, a significant difference was observed between plyometric group with control group. Differences were also found between the balance group and both the combined and control groups. In the SL muscle, a difference was observed between the combined group and the balance and control groups (Table 10) (P<0.05).
Discussion
This study showed that plyometric, balance and PNF trainings each had a positive impact on electromyography function of ankle muscles and reduced the rate of ankle injury. However, combined training (plyometric, balance and PNF) exhibited a greater impact on function muscles across four phases of jumping test. Plyometric training demonstrated considerable effectiveness in preventing ankle injuries among basketball players [30]. Studies have demonstrated that incorporating plyometric exercises into the training regimen of basketball players enhances ankle stability, muscular strength, and proprioception. These adaptations contribute to a reduced risk of ankle injuries during the dynamic movements involved in basketball [31]. Also, a targeted plyometric program significantly decreased the incidence of ankle sprains in basketball players, and plyometric interventions positively impacted neuromuscular control. The influence of plyometric training on neuromuscular performance and injury risk in young athletes has been investigated, highlighting it as a crucial factor in preventing ankle injuries [32]. Balance training has proven to be a valuable component in preventing ankle injuries among basketball players [33]. In addition, a significant reduction in the incidence of ankle sprains was observed among basketball players who underwent a targeted balance training program. These findings support the role of balance training in enhancing proprioception and reducing the risk of ankle injuries in sports, including basketball [34]. Also, a study incorporated balance training into the regimen of basketball players evaluated its effects using functional assessments, including the Jump on Step Test. The findings revealed improvements in ankle muscle function, enhanced proprioception, and a decreased risk of ankle injuries among those who underwent balance training [35]. PNF training has demonstrated positive effects on preventing ankle injuries among basketball players. Significant studies emphasize the efficacy of PNF techniques in enhancing proprioception and reducing the risk of ankle sprains [36]. Incorporating PNF exercises of basketball players has been shown to improve joint position sense and reduce the incidence of ankle injuries, emphasizing the role of PNF in enhancing neuromuscular control and decreasing the likelihood of ankle sprains in athletes [37]. Combined training, integrating plyometric and balance exercises, has been shown to be effective in reducing the rate of ankle injuries. Plyometric exercises focus on explosive movements, while balance training enhances proprioception and stability [38]. On the other hand, plyometric exercises focus on explosive movements that improve power and speed, while balance training helps improve proprioception and stability around the ankle joint. In addition, athletes who performed plyometric and balance exercises had better overall ankle stability and lower rates of injury compared to those who did not perform these combined interventions [39]. On the other hand, combined training, including plyometric and balance, improves ankle power and stability but showed no effect on the range of motion and coordination. Therefore, it is crucial to note that individual factors, such as range of motion, can influence the risk factors for ankle sprain in youth sports [40]. By combining plyometric and PNF exercises in a structured training program, athletes can benefit from the synergistic effects of both modalities. Plyometric training improves power and explosive strength, while PNF techniques enhance proprioception, coordination, and neuromuscular control. Together, these components can help athletes develop better ankle stability and reduce the risk of injuries [41]. While combined training with plyometric and PNF exercises can be beneficial, it is important to consider potential drawbacks and limitations. Several studies suggests that integrating these two training modalities can lead to improvements in muscle activation patterns, and functional performance, potentially contributing to a reduced risk of ankle injuries in athletes. However, this combined practice did not have a significant impact on balance and coordination [41]. Research supports the effectiveness of combined training involving balance and PNF exercises in reducing the rate of ankle injuries. These practices are also effective in neuromuscular and proprioceptive training program in preventing ankle ligament injuries in athletes. Furthermore, the positive impact of neuromuscular and proprioceptive training on injury prevention emphasizes the importance of balance exercises [42]. Balance training and PNF exercises improve proprioception, which is the body’s ability to sense its position, movement, and balance. By enhancing proprioception through targeted exercises, athletes can better control their movements and respond to lateral forces, reducing the risk of ankle injuries caused by instability or poor coordination. While combined training with balance and PNF exercises can be beneficial for reducing the rate of ankle injuries, it is crucial to consider potential drawbacks and limitations. It has been demonstrated that combined (balance and PNF) training improves the stability, coordination and range of motion, but it has insufficient impact on enhancing the strength and power [43]. This research showed that plyometric, balance exercises, and PNF individually affect ankle muscles during different phases of a box jump test. However, combined exercises demonstrated a superior and greater effect across all four jump phases in basketball players’ ankle muscles. In addition, combined exercises can be used to improve the electrical ankle muscle activity among basketball players or even to prevent ankle injuries. Since most ankle injuries occur during forward movement, the phasing of the test has significantly contributed to a more accurate examination of the ankle muscle activity. Moreover, in each examined phase, muscles undergo concentric and eccentric contractions. Weakness in each of the phases and muscles involved causes ankle injury under certain conditions [44]. Thus, it is concluded that a series of injury prevention exercises to strengthen and improve each of the muscles involved in different phases is necessary. The integration of plyometric, balance, and PNF training demonstrates a collective positive impact on preventing ankle injuries. Research consistently supports the individual efficacy of these methods, with studies highlighting improved strength, stability, and proprioception. However, the combining approach appears to yield a more comprehensive and heightened preventative effect. This amalgamation enhances neuromuscular control, addresses multiple facets of ankle stability, and fosters a more robust injury prevention strategy. The novel findings of this study provide a significant advancement in ankle injury prevention by offering the first detailed analysis of muscle activation patterns across all four critical phases of single-leg jumps in basketball players. Unlike previous research that examined general muscle activity, our phase-specific EMG data precisely identifies neuromuscular deficits during preparation, takeoff, flight, and landing phases. This granular understanding allows for targeted rehabilitation protocols that address phase-specific weaknesses, fundamentally changing how ankle stability training is approached in sports medicine. The demonstrated greater effectiveness of combined training underscores its potential as an evidence-based intervention, providing coaches and clinicians with actionable insights to reduce ankle injury rates among athletes. By connecting biomechanical evidence with practical training applications, this work establishes a new standard for injury prevention strategies in basketball and similar jumping sports.
Conclusion
The findings of this study demonstrate that while isolated plyometric, balance, and PNF training protocols each induce specific neuromuscular adaptations in the ankle stabilizers of young basketball players, their efficacy is limited to particular muscles and phases of a single-leg jump. The combined training protocol, integrating all three modalities, proved to be the most comprehensive and effective intervention. It elicited significant improvements in EMG activity across all four biomechanically defined phases of the jump (preparation, takeoff, flight, and landing), impacting the TA, PL, medial and lateral gastrocnemius, and SL muscles. This superior effect is likely due to the synergistic nature of combined training, which simultaneously enhances muscular strength, power, proprioceptive acuity, and dynamic neuromuscular control. Therefore, for clinicians and strength coaches aiming to optimize ankle stability and mitigate injury risk in basketball players, a multimodal training approach is strongly recommended over single-focus protocols. Implementing such a combined program as part of a regular warm-up or conditioning routine could provide a more robust defense against the high incidence of ankle sprains in this athletic population. Future research should investigate the long-term effects of this combined training on actual ankle injury rates and its applicability to other sports and demographic groups.
Research limitations
This research has several limitations. The study sample was limited to young male players (12–16 years old) with no history of ankle injury, which restricts the generalizability of the findings. The short, 8-week training duration may be insufficient to reveal long-term effects. The focus was also narrow, as EMG activity was measured only during single-leg jumps and not during more complex, game-like movements. Furthermore, the study design was unblinded, introducing potential bias since both participants and researchers were aware of group assignments. While muscle activity was measured, the actual incidence of injuries was not tracked. Consequently, these results may not be applicable to females, older athletes, or other sports.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Institute of Physical Education and Sport Sciences (Code: IR.SKU.REC.1400.075).
Funding
This research was financially supported by Shahrekord University, Shahrekord, Iran (Grant No.:141.1402.32).
Authors' contributions
Study design, training implementation data analysis, manuscript writing: Nayeb Ahmadpour; Supervision, data collection, manuscript review: Banafsheh Mohammadi; Methodology support, statistical analysis, manuscript editing: Mohammad Rabiei.
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgments
The authors appreciate all individuals who contributed to the completion of this manuscript.
The results of ANOVA test showed significant differences in TA muscle activity during the first jumping phase between the plyometric, balance, and combined groups compared to the control group. In addition, significant differences were observed between combined training group with the plyometric, balance, and PNF groups. In the PL muscle, significant differences were observed between the plyometric and control group, and between the combined training group and both the balance and control groups. In the medial GM muscle, a significant difference was found between the combined with balance and control groups. No significant difference was observed in the lateral GM muscle between groups. In the SL muscle, significant differences were observed between balance with control and PNF groups. Additionally, differences were found between the plyometric group and both the balance and control group. Finally, a significant difference was observed between combined with balance and control groups (Table 4) (P<0.05).
Paired t-test results indicated that combined exercises significantly affected all five ankle muscles during the second jumping phase. Furthermore, plyometric training significantly affected the TA and both medial and lateral GM muscles. Balance training significantly affected the SL muscle, whereas PNF training showed no significant effect on any of the studied muscles (Table 5) (P<0.05).
According to the ANOVA test, in the TA, differences were observed between the combined group and the balance, PNF, and control groups. No significant differences were observed in the PL muscle between any groups. In the medial GM muscle, significant differences were observed between the combined group and both the balance and control groups. Additionally, differences were observed between the plyometrics group and the balance, PNF, and control groups. In the lateral GM muscle, a difference was observed between the balance group and both the PNF and control groups. In the SL muscle, differences were observed between the combined group and the balance, PNF, and control groups. Furthermore, differences were observed between plyometrics training group and balance, PNF, and control groups (Table 6) (P<0.05).
According to the results of the paired t-test for intra-group comparisons, it can be concluded that in the third phase of jumping, combined training had an effect on the TA, medial GM and SL muscles, as well as plyometric and balance trainings had significant effect on the TA muscle (Table 7) (P<0.05).
The results of ANOVA test showed a difference in the medial GM muscle between the plyometric with balance, PNF and control groups. Furthermore, a difference was observed between the combined group and the control group. The lateral GM muscle demonstrated a significant difference between the combined group and the plyometric, PNF, and control groups. A significant difference was observed between the balance group and the control group, as well as between the plyometric group and the control group. A significant difference was observed in the SL muscle between the combined group and all other groups (Table 8) (P<0.05).
According to the results of the paired t-test for intra-group comparisons, combined training significantly affected the TA, PL, medial GM, and SL muscles during the fourth jumping phase. Additionally, plyometric training affected the TA muscle, and balance training impacted the medial GM and SL muscle (Table 9) (P<0.05).
The results of ANOVA test showed a difference in the anterior large muscle between the combined group, and the PNF and control groups. Also, a significant difference was observed between plyometric group with control group. Differences were also found between the balance group and both the combined and control groups. In the SL muscle, a difference was observed between the combined group and the balance and control groups (Table 10) (P<0.05).
Discussion
This study showed that plyometric, balance and PNF trainings each had a positive impact on electromyography function of ankle muscles and reduced the rate of ankle injury. However, combined training (plyometric, balance and PNF) exhibited a greater impact on function muscles across four phases of jumping test. Plyometric training demonstrated considerable effectiveness in preventing ankle injuries among basketball players [30]. Studies have demonstrated that incorporating plyometric exercises into the training regimen of basketball players enhances ankle stability, muscular strength, and proprioception. These adaptations contribute to a reduced risk of ankle injuries during the dynamic movements involved in basketball [31]. Also, a targeted plyometric program significantly decreased the incidence of ankle sprains in basketball players, and plyometric interventions positively impacted neuromuscular control. The influence of plyometric training on neuromuscular performance and injury risk in young athletes has been investigated, highlighting it as a crucial factor in preventing ankle injuries [32]. Balance training has proven to be a valuable component in preventing ankle injuries among basketball players [33]. In addition, a significant reduction in the incidence of ankle sprains was observed among basketball players who underwent a targeted balance training program. These findings support the role of balance training in enhancing proprioception and reducing the risk of ankle injuries in sports, including basketball [34]. Also, a study incorporated balance training into the regimen of basketball players evaluated its effects using functional assessments, including the Jump on Step Test. The findings revealed improvements in ankle muscle function, enhanced proprioception, and a decreased risk of ankle injuries among those who underwent balance training [35]. PNF training has demonstrated positive effects on preventing ankle injuries among basketball players. Significant studies emphasize the efficacy of PNF techniques in enhancing proprioception and reducing the risk of ankle sprains [36]. Incorporating PNF exercises of basketball players has been shown to improve joint position sense and reduce the incidence of ankle injuries, emphasizing the role of PNF in enhancing neuromuscular control and decreasing the likelihood of ankle sprains in athletes [37]. Combined training, integrating plyometric and balance exercises, has been shown to be effective in reducing the rate of ankle injuries. Plyometric exercises focus on explosive movements, while balance training enhances proprioception and stability [38]. On the other hand, plyometric exercises focus on explosive movements that improve power and speed, while balance training helps improve proprioception and stability around the ankle joint. In addition, athletes who performed plyometric and balance exercises had better overall ankle stability and lower rates of injury compared to those who did not perform these combined interventions [39]. On the other hand, combined training, including plyometric and balance, improves ankle power and stability but showed no effect on the range of motion and coordination. Therefore, it is crucial to note that individual factors, such as range of motion, can influence the risk factors for ankle sprain in youth sports [40]. By combining plyometric and PNF exercises in a structured training program, athletes can benefit from the synergistic effects of both modalities. Plyometric training improves power and explosive strength, while PNF techniques enhance proprioception, coordination, and neuromuscular control. Together, these components can help athletes develop better ankle stability and reduce the risk of injuries [41]. While combined training with plyometric and PNF exercises can be beneficial, it is important to consider potential drawbacks and limitations. Several studies suggests that integrating these two training modalities can lead to improvements in muscle activation patterns, and functional performance, potentially contributing to a reduced risk of ankle injuries in athletes. However, this combined practice did not have a significant impact on balance and coordination [41]. Research supports the effectiveness of combined training involving balance and PNF exercises in reducing the rate of ankle injuries. These practices are also effective in neuromuscular and proprioceptive training program in preventing ankle ligament injuries in athletes. Furthermore, the positive impact of neuromuscular and proprioceptive training on injury prevention emphasizes the importance of balance exercises [42]. Balance training and PNF exercises improve proprioception, which is the body’s ability to sense its position, movement, and balance. By enhancing proprioception through targeted exercises, athletes can better control their movements and respond to lateral forces, reducing the risk of ankle injuries caused by instability or poor coordination. While combined training with balance and PNF exercises can be beneficial for reducing the rate of ankle injuries, it is crucial to consider potential drawbacks and limitations. It has been demonstrated that combined (balance and PNF) training improves the stability, coordination and range of motion, but it has insufficient impact on enhancing the strength and power [43]. This research showed that plyometric, balance exercises, and PNF individually affect ankle muscles during different phases of a box jump test. However, combined exercises demonstrated a superior and greater effect across all four jump phases in basketball players’ ankle muscles. In addition, combined exercises can be used to improve the electrical ankle muscle activity among basketball players or even to prevent ankle injuries. Since most ankle injuries occur during forward movement, the phasing of the test has significantly contributed to a more accurate examination of the ankle muscle activity. Moreover, in each examined phase, muscles undergo concentric and eccentric contractions. Weakness in each of the phases and muscles involved causes ankle injury under certain conditions [44]. Thus, it is concluded that a series of injury prevention exercises to strengthen and improve each of the muscles involved in different phases is necessary. The integration of plyometric, balance, and PNF training demonstrates a collective positive impact on preventing ankle injuries. Research consistently supports the individual efficacy of these methods, with studies highlighting improved strength, stability, and proprioception. However, the combining approach appears to yield a more comprehensive and heightened preventative effect. This amalgamation enhances neuromuscular control, addresses multiple facets of ankle stability, and fosters a more robust injury prevention strategy. The novel findings of this study provide a significant advancement in ankle injury prevention by offering the first detailed analysis of muscle activation patterns across all four critical phases of single-leg jumps in basketball players. Unlike previous research that examined general muscle activity, our phase-specific EMG data precisely identifies neuromuscular deficits during preparation, takeoff, flight, and landing phases. This granular understanding allows for targeted rehabilitation protocols that address phase-specific weaknesses, fundamentally changing how ankle stability training is approached in sports medicine. The demonstrated greater effectiveness of combined training underscores its potential as an evidence-based intervention, providing coaches and clinicians with actionable insights to reduce ankle injury rates among athletes. By connecting biomechanical evidence with practical training applications, this work establishes a new standard for injury prevention strategies in basketball and similar jumping sports.
Conclusion
The findings of this study demonstrate that while isolated plyometric, balance, and PNF training protocols each induce specific neuromuscular adaptations in the ankle stabilizers of young basketball players, their efficacy is limited to particular muscles and phases of a single-leg jump. The combined training protocol, integrating all three modalities, proved to be the most comprehensive and effective intervention. It elicited significant improvements in EMG activity across all four biomechanically defined phases of the jump (preparation, takeoff, flight, and landing), impacting the TA, PL, medial and lateral gastrocnemius, and SL muscles. This superior effect is likely due to the synergistic nature of combined training, which simultaneously enhances muscular strength, power, proprioceptive acuity, and dynamic neuromuscular control. Therefore, for clinicians and strength coaches aiming to optimize ankle stability and mitigate injury risk in basketball players, a multimodal training approach is strongly recommended over single-focus protocols. Implementing such a combined program as part of a regular warm-up or conditioning routine could provide a more robust defense against the high incidence of ankle sprains in this athletic population. Future research should investigate the long-term effects of this combined training on actual ankle injury rates and its applicability to other sports and demographic groups.
Research limitations
This research has several limitations. The study sample was limited to young male players (12–16 years old) with no history of ankle injury, which restricts the generalizability of the findings. The short, 8-week training duration may be insufficient to reveal long-term effects. The focus was also narrow, as EMG activity was measured only during single-leg jumps and not during more complex, game-like movements. Furthermore, the study design was unblinded, introducing potential bias since both participants and researchers were aware of group assignments. While muscle activity was measured, the actual incidence of injuries was not tracked. Consequently, these results may not be applicable to females, older athletes, or other sports.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Institute of Physical Education and Sport Sciences (Code: IR.SKU.REC.1400.075).
Funding
This research was financially supported by Shahrekord University, Shahrekord, Iran (Grant No.:141.1402.32).
Authors' contributions
Study design, training implementation data analysis, manuscript writing: Nayeb Ahmadpour; Supervision, data collection, manuscript review: Banafsheh Mohammadi; Methodology support, statistical analysis, manuscript editing: Mohammad Rabiei.
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgments
The authors appreciate all individuals who contributed to the completion of this manuscript.
References
- Taylor JB, Ford KR, Nguyen AD, Terry LN, Hegedus EJ. Prevention of lower extremity injuries in basketball:A systematic review and meta-analysis. Sports Health. 2015; 7(5):392-8. [DOI:10.1177/1941738115593441] [PMID]
- Harmer PA. Basketball injuries. Medicine and Sport Science. 2005; 49:31-61. [Link]
- Newman JS, Newberg AH. Basketball injuries. Radiologic Clinics. 2010; 48(6):1095-111. [Link]
- Leanderson J, Nemeth G, Eriksson E. Ankle injuries in basketball players. Knee Surgery, Sports Traumatology, Arthroscopy. 1993; 1(3-4):200-2. [Link]
- McKay GD, Goldie P, Payne WR, Oakes B. Ankle injuries in basketball: injury rate and risk factors. British Journal of Sports Medicine. 2001; 35(2):103-8. [DOI:10.1136/bjsm.35.2.103]
- Faraji E, Daneshmandi H, Atri AE, Onvani V, Namjoo FR. Effects of prefabricated ankle orthoses on postural stability in basketball players with chronic ankle instability. Asian Journal of Sports Medicine. 2012; 3(4):274. [PMID]
- Owoeye OB, Palacios-Derflingher LM, Emery CA. Prevention of ankle sprain injuries in youth soccer and basketball: effectiveness of a neuromuscular training program and examining risk factors. Clinical Journal of Sport Medicine. 2018; 28(4):325-31. [DOI:10.1097/JSM.0000000000000462]
- Sacco IdC, Takahasi HY, Vasconcellos ÂA, Suda EY, Bacarin TdA, Pereira CS, et al. Influence of ankle devices in the jump and landing biomechanical responses in basketball. Revista Brasileira de Medicina do Esporte. 2004; 10:447-52. [Link]
- Herzog MM, Mack CD, Dreyer NA, Wikstrom EA, Padua DA, Kocher MS, et al. Ankle sprains in the national basketball association, 2013-2014 through 2016-2017. The American Journal of Sports Medicine. 2019; 47(11):2651-8. [Link]
- Cumps E, Verhagen E, Meeusen R. Efficacy of a sports specific balance training programme on the incidence of ankle sprains in basketball. Journal of Sports Science & Medicine. 2007; 6(2):212. [PMID]
- Riva D, Bianchi R, Rocca F, Mamo C. Proprioceptive training and injury prevention in a professional men’s basketball team: a six-year prospective study. The Journal of Strength & Conditioning Research. 2016; 30(2):461-75. [DOI:10.1519/JSC.0000000000001097]
- Schiftan GS, Ross LA, Hahne AJ. The effectiveness of proprioceptive training in preventing ankle sprains in sporting populations: A systematic review and meta-analysis. Journal of Science and Medicine in Sport. 2015; 18(3):238-44. [DOI:10.1016/j.jsams.2014.04.005]
- Van Reijen M, Vriend I, Zuidema V, Van Mechelen W, Verhagen E. Increasing compliance with neuromuscular training to prevent ankle sprain in sport: does the ‘Strengthen your ankle’mobile App make a difference? A randomised controlled trial. British Journal of Sports Medicine. 2016; 50(19):1200-5. [DOI:10.1136/bjsports-2015-095290]
- Mohammadi B, Ahmadpour ND, Rabiei M. The effect of four types of training: Plyometric, balance, pnf and combination training on physical performance and ankle injury prevention in basketball players: A clinical trial. Journal of Advanced Sport Technology. 2024; 8(2):14-26. [Link]
- Padua E, D’Amico AG, Alashram A, Campoli F, Romagnoli C, Lombardo M, et al. Effectiveness of warm-up routine on the ankle injuries prevention in young female basketball players: A randomized controlled trial. Medicina. 2019;55(10):690. [PMID]
- Sushko R, Vysochina N, Vorobiova A, Doroshenko E, Pastuhova V, Vysochin F. Psychological selection in game sports on the basketball example. Journal of Physical Education and Sport. 2019; 19(7):1708-14. [Link]
- Díaz-Martínez AS, Vaquero-Cristóbal R, Albaladejo-Saura M, Esparza-Ros F. Effect of pre-season and in-season training on anthropometric variables, somatotype, body composition and body proportion in elite basketball players. Scientific Reports. 2024; 14(1):7537. [DOI:10.1038/s41598-024-58222-4]
- Al Attar WSA, Khaledi EH, Bakhsh JM, Faude O, Ghulam H, Sanders RH. Injury prevention programs that include balance training exercises reduce ankle injury rates among soccer players: A systematic review. Journal of Physiotherapy. 2022; 68(3):165-73. [PMID]
- Maleki B, Mantashloo Z, Salehi S. Effect of ankle sprain on postural control and electrical activity of selected muscles after single-leg jump landing task. Novelty in Biomedicine. 2019;7(4):218-24. [Link]
- İlbak İ, Acak M. The effect of plyometric training combined with electrical muscle stimulation on sports performance parameters in basketball players. Spor ve Performans Araştırmaları Dergisi. 2022; 13(2):189-200. [Link]
- Pechlivanos RG, Amiridis IG, Anastasiadis N, Kannas T, Sahinis C, Duchateau J, et al. Effects of plyometric training techniques on vertical jump performance of basketball players. European Journal of Sport Science. 2024. [PMID]
- Yeste-Fabregat M, Baraja-Vegas L, Vicente-Mampel J, Pérez-Bermejo M, Bautista González IJ, Barrios C. Acute effects of tecar therapy on skin temperature, ankle mobility and hyperalgesia in myofascial pain syndrome in professional basketball players: A pilot study. International Journal of Environmental Research and Public Health. 2021; 18(16):8756. [PMID]
- Gulick DT, Castel JC, Palermo FX, Draper DO. Effect of patterned electrical neuromuscular stimulation on vertical jump in collegiate athletes. Sports Health. 2011; 3(2):152-7. [PMID]
- Yoshida M, Taniguchi K, Katayose M. Analysis of muscle activity and ankle joint movement during the side-hop test. The Journal of Strength & Conditioning Research. 2011; 25(8):2255-64. [PMID]
- Labanca L, Mosca M, Ghislieri M, Agostini V, Knaflitz M, Benedetti MG. Muscle activations during functional tasks in individuals with chronic ankle instability: A systematic review of electromyographical studies. Gait & Posture. 2021;90:340-73. [PMID]
- Mendes PG, Pereira AA, Abreu PHA, Campos MR, Lins C, Felicio LR. Electromiographic activity during single leg jump in adolescent athletes with chronic ankle instability: A pilot study. Journal of Bodywork and Movement Therapies. 2021; 28:238-45. [PMID]
- Allet L, Zumstein F, Eichelberger P, Armand S, Punt IM. Neuromuscular control mechanisms during single-leg jump landing in subacute ankle sprain patients: A case control study. Pm&r. 2017; 9(3):241-50. [PMID]
- Llurda-Almuzara L, Perez-Bellmunt A, Labata-Lezaun N, López-de-Celis C, Canet-Vintró M, Cadellans-Arroniz A, et al. Relationship between lower limb EMG activity and knee frontal plane projection angle during a single-legged drop jump. Physical Therapy in Sport. 2021; 52:13-20. [PMID]
- Thain PK, Hughes GTG, Mitchell ACS. The effect of repetitive ankle perturbations on muscle reaction time and muscle activity. Journal of Electromyography and Kinesiology. 2016; 30:184-90. [PMID]
- Asadi A, de Villarreal ES, Arazi H. The effects of plyometric type neuromuscular training on postural control performance of male team basketball players. The Journal of Strength & Conditioning Research. 2015; 29(7):1870-5. [PMID]
- Bal BS, Kaur PJ, Singh D. Effects of a short term plyometric training program of agility in young basketball players. Brazilian Journal of Biomotricity. 2011; 5(4):271-8. [Link]
- Huang PY, Jankaew A, Lin CF. Effects of plyometric and balance training on neuromuscular control of recreational athletes with functional ankle instability: A randomized controlled laboratory study. International Journal of Environmental Research and Public Health. 2021; 18(10):5269. [PMID]
- McGuine TA, Keene JS. The effect of a balance training program on the risk of ankle sprains in high school athletes. The American Journal of Sports Medicine. 2006;34(7):1103-11. [PMID]
- Borao O, Planas A, Beltran V, Corbi F. Effects of a 6-week neuromuscular ankle training program on the star excursion balance test for basketball players. Apunts Medicina de l’Esport. 2015; 50(187):95-102. [Link]
- Zemková E, Hamar D. The effect of 6-week combined agility-balance training on neuromuscular performance in basketball players. Journal of Sports Medicine and Physical Fitness. 2010; 50(3):262. [PMID]
- Daniel DC. Effects of ultrasound therapy with taping PNF training and PNF training with taping in treatment and rehabilitation of sports injuries of high ankle sprain. Journal of Dr NTR University of Health Sciences. 2017;6(2):92-7. [Link]
- Bhardwaj A, Kathayat L. Effectiveness of contract-relax PNF technique versus dynamic oscillatory stretching on active range of motion and balance in collegiate basketball players. Journal of Exercise Science & Physiotherapy. 2021; 17(2):1. [Link]
- Surakhamhaeng A, Bovonsunthonchai S, Vachalathiti R. Effects of balance and plyometric training on balance control among individuals with functional ankle instability. Physiotherapy Quarterly. 2020; 28(2):38-45. [Link]
- Villalba MM, Eltz GD, Fujita RA, Panhan AC, Cardozo AC, Gonçalves M. Effects of six weeks of plyometric training on the ground vs on a mini-trampoline on strength, jump performance, and balance in male basketball players—Randomized clinical trial. Sport Sciences for Health. 2023; 19(3):829-39. [Link]
- Kooroshfard N, Rahimi Z. The effect of the neuromuscular, strength, and combined training on balance and performance in female basketball players. Physical Treatments-Specific Physical Therapy Journal. 2022; 12(1):41-50. [DOI:10.32598/ptj.12.1.513.1]
- Singh S, Taneja D, Saharan A, Ranjieeta W, Mathur M. Low intensity plyometrics versus PNF stretching on vertical jump height and agility in collegiate basketball players. International Journal of Development Research. 2018; 8(3):19261-70. [Link]
- Lazarou L, Kofotolis N, Malliou P, Kellis E. Effects of two proprioceptive training programs on joint position sense, strength, activation and recurrent injuries after ankle sprains. Isokinetics and Exercise Science. 2017; 25(4):289-300. [DOI:10.3233/IES-171146]
- Hall EA, Chomistek AK, Kingma JJ, Docherty CL. Balance-and strength-training protocols to improve chronic ankle instability deficits, part I: Assessing clinical outcome measures. Journal of Athletic Training. 2018; 53(6):568-77. [Link]
- Garcia-Gil M, Torres-Unda J, Esain I, Duñabeitia I, Gil SM, Gil J, Irazusta J. Anthropometric parameters, age, and agility as performance predictors in elite female basketball players. The Journal of Strength & Conditioning Research. 2018; 32(6):1723-30. [DOI:10.1519/JSC.0000000000002043]
Type of Study: Research |
Subject:
General
Received: 2025/05/9 | Accepted: 2025/09/12 | Published: 2026/04/1
Received: 2025/05/9 | Accepted: 2025/09/12 | Published: 2026/04/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
