Thu, Jul 30, 2026
Volume 16, Issue 2 (Spring 2026)
PTJ 2026, 16(2): 189-200 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Hovanloo F, Khoshniyat A R, Barati A H, Barzegar Bafrouei M. Effect of Six-week Corrective Exercises on Shoulder Stability in CrossFit Athletes With Scapular Dysfunction. PTJ 2026; 16 (2) :189-200
URL: http://ptj.uswr.ac.ir/article-1-769-en.html
URL: http://ptj.uswr.ac.ir/article-1-769-en.html



1- Department of Sports Health and Rehabilitation, Faculty of Sports and Health Sciences, Shahid Beheshti University, Tehran, Iran.
Full-Text [PDF 1649 kb]
(988 Downloads)
| Abstract (HTML) (1570 Views)
Full-Text: (111 Views)
Introduction
CrossFit, first introduced in the early 2000s, is a type of high-intensity functional training that combines aerobic workouts, gymnastics, and Olympic weightlifting to enhance overall physical performance [1, 2]. It is designed to improve various aspects of fitness, including aerobic capacity, muscular strength and endurance, flexibility, coordination, agility, speed, and balance. CrossFit workouts are typically performed in a high-intensity circuit format, characterized by short durations, minimal rest, and high repetitions, aiming to simultaneously develop strength and endurance [3-5].
The increasing popularity of high-intensity training modalities, such as CrossFit, reflects a broader trend in sports science favoring such approaches over traditional methods, due to their greater time-efficiency and effectiveness in improving health and fitness [6, 7]. Due to its adaptability to different fitness levels, motivational nature, and group setting, CrossFit has gained global popularity since its inception [8, 9].
Despite its benefits, research reports a wide range of injury rates in CrossFit, from 3.3% to 73.5%, with approximately 9.18 cases occurring per 1,000 training hours [10]. Approximately 67% of injuries occur among beginner to intermediate athletes [11]. The most common injury sites in CrossFit athletes are the shoulder (26%), spine (24%), and knee (18%) [12]. Shoulder injuries are particularly frequent, mainly associated with overhead activities that decrease the subacromial space [13] and with gymnastic movements, which represent about 41% of such injuries [14, 15]. In Iran, the incidence has been estimated at 4.421 cases per 1,000 training hours, with the shoulder and knee reported as the most vulnerable areas. Overall, men experience higher injury rates than women, likely because of less supervision and fewer consultations with professional coaches [14, 16].
One of the major biomechanical contributors to shoulder injuries in CrossFit is scapular dyskinesis, which refers to non-functional or altered scapular motion patterns [17, 18].
Scapular dyskinesis is defined as an alteration in the normal position or motion of the scapula during coordinated scapulohumeral movements [19]. It is commonly observed among overhead athletes and individuals with shoulder pathologies, with prevalence rates reported between 61% to 100% depending on the population and assessment methods [20, 21]. Kibler et al. categorized scapular dyskinesis into three main types: Type I (prominence of the inferomedial border), type II (prominence of the entire medial border), and type III (excessive elevation and shrugging during arm elevation), each reflecting specific muscular imbalances, such as serratus anterior weakness or upper trapezius overactivity [22]. The etiology of scapular dyskinesis is multifactorial, including neuromuscular imbalance, poor posture, nerve injury (e.g. long thoracic nerve palsy), and repetitive overhead movements [23]. These alterations disrupt scapulohumeral rhythm and glenohumeral joint mechanics, increasing the risk of subacromial impingement, labral injuries, and rotator cuff pathology [24]. Clinically, it can be identified using tests, such as the scapular dyskinesis test (SDT), Scapular Assistance Test, and Lateral Scapular Slide Test, which are reliable tools for detection and functional evaluation [25]. Treatment typically focuses on neuromuscular re-education, strengthening of stabilizing muscles (particularly lower trapezius and serratus anterior), and postural correction strategies [26]. Consequently, early recognition and correction of scapular dyskinesis are crucial in restoring optimal shoulder biomechanics and preventing secondary injuries [27].
The scapula plays a crucial role in maintaining glenohumeral stability and ensuring the efficient transmission of kinetic energy from the lower extremities to the upper limbs [28, 29]. Dyskinesis is associated with disrupted scapulohumeral rhythm, leading to compromised shoulder mechanics and increased injury risk [30]. It is typically characterized by abrupt or exaggerated protraction and elevation during arm lifting, as well as accelerated downward rotation when the arm is lowered [25, 31].
Contributing factors include abnormal recruitment patterns in stabilizing muscles, skeletal malalignment, structural joint instability, and altered soft tissue or neural input [30, 31]. Scapular dysfunction may result in a winged scapula, seen as the prominence of the medial border or inferior angle detaching from the thoracic wall, often due to delayed activation or weakness in the serratus anterior and lower trapezius muscles [25, 31-33]. Furthermore, limited flexibility of the pectoralis minor and the short head of the biceps brachii has been associated with excessive anterior tilting and forward movement of the scapula [34].
Muscle imbalance frequently observed in overhead athletes with overuse pain syndromes can inhibit proper scapular stabilizer activation, further contributing to dysfunctional scapular motion [24, 35-37]. These neuromuscular and biomechanical disturbances may lead to increased stress on the anterior shoulder capsule, rotator cuff compression, and reduced functional performance. Imbalances among key muscles such as the serratus anterior, trapezius, pectoralis minor, rhomboids, and levator scapulae negatively affect scapulohumeral rhythm and shoulder joint function [38].
Considering the high prevalence of shoulder and scapular dysfunction in CrossFit athletes and the lack of sufficient research on corrective interventions in this population, this study aimed to evaluate the effects of a six-week corrective exercise program on shoulder stability in male CrossFit athletes with scapular dyskinesis, in order to improve movement mechanics, musculoskeletal alignment, and reduce the risk of injury.
Materials and Methods
A total of 24 male CrossFit athletes, aged between 25 and 30 years, who had a minimum of two years of continuous training experience and a clinical diagnosis of scapular movement dysfunction, participated in this study. The sample size was determined with G*Power software, version 3.1, drawing on earlier clinical trials that examined scapular stabilization programs. The calculation was performed using the following parameters: effect size=0.54, α=0.05, and statistical power=80% (1−β=0.80), which yielded a minimum of 24 participants (12 per group). To allow for a potential 10% dropout, the final sample size was increased to 26.
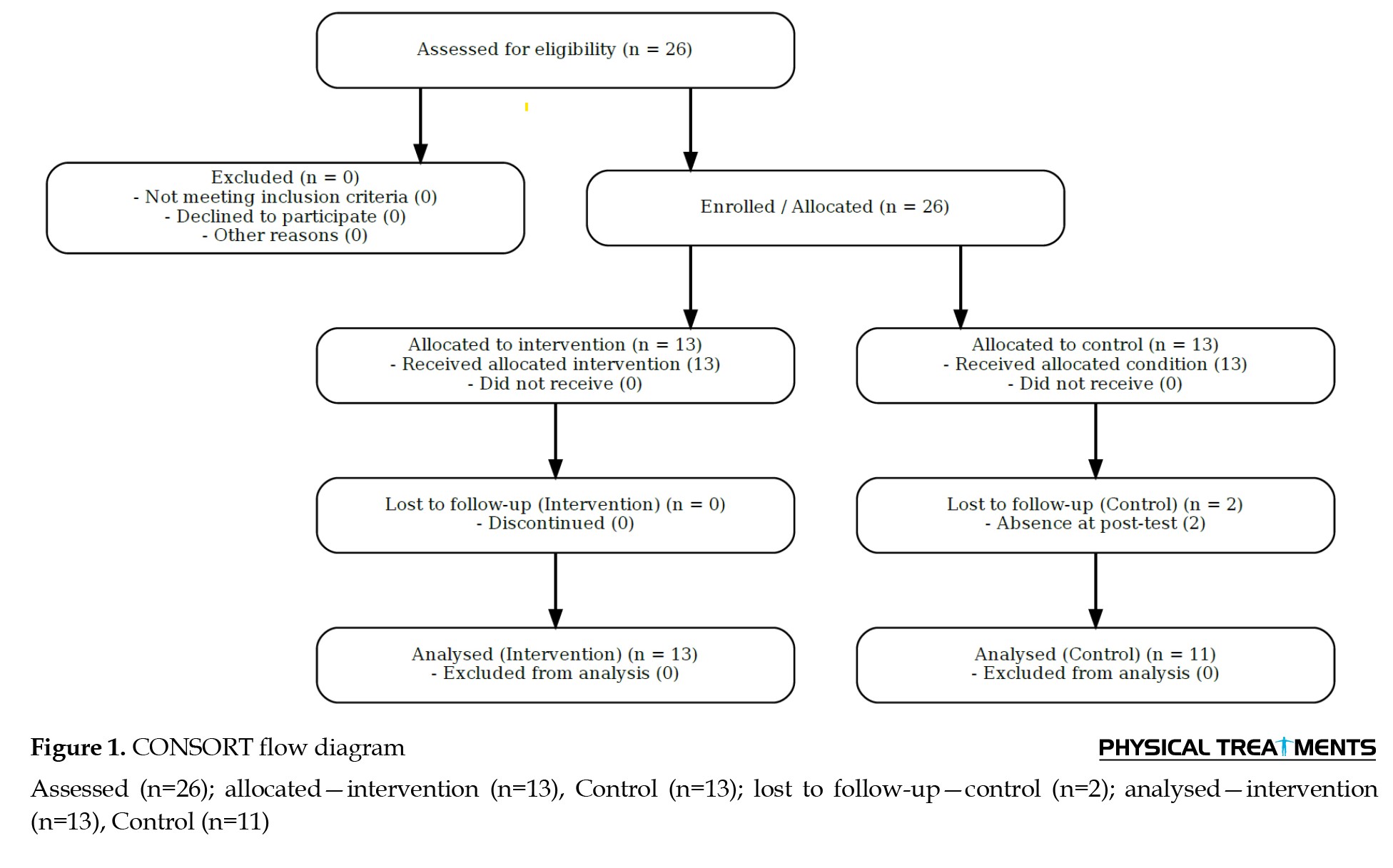
To clarify the recruitment and allocation process, a CONSORT-style flow diagram was provided (Figure 1).
CrossFit, first introduced in the early 2000s, is a type of high-intensity functional training that combines aerobic workouts, gymnastics, and Olympic weightlifting to enhance overall physical performance [1, 2]. It is designed to improve various aspects of fitness, including aerobic capacity, muscular strength and endurance, flexibility, coordination, agility, speed, and balance. CrossFit workouts are typically performed in a high-intensity circuit format, characterized by short durations, minimal rest, and high repetitions, aiming to simultaneously develop strength and endurance [3-5].
The increasing popularity of high-intensity training modalities, such as CrossFit, reflects a broader trend in sports science favoring such approaches over traditional methods, due to their greater time-efficiency and effectiveness in improving health and fitness [6, 7]. Due to its adaptability to different fitness levels, motivational nature, and group setting, CrossFit has gained global popularity since its inception [8, 9].
Despite its benefits, research reports a wide range of injury rates in CrossFit, from 3.3% to 73.5%, with approximately 9.18 cases occurring per 1,000 training hours [10]. Approximately 67% of injuries occur among beginner to intermediate athletes [11]. The most common injury sites in CrossFit athletes are the shoulder (26%), spine (24%), and knee (18%) [12]. Shoulder injuries are particularly frequent, mainly associated with overhead activities that decrease the subacromial space [13] and with gymnastic movements, which represent about 41% of such injuries [14, 15]. In Iran, the incidence has been estimated at 4.421 cases per 1,000 training hours, with the shoulder and knee reported as the most vulnerable areas. Overall, men experience higher injury rates than women, likely because of less supervision and fewer consultations with professional coaches [14, 16].
One of the major biomechanical contributors to shoulder injuries in CrossFit is scapular dyskinesis, which refers to non-functional or altered scapular motion patterns [17, 18].
Scapular dyskinesis is defined as an alteration in the normal position or motion of the scapula during coordinated scapulohumeral movements [19]. It is commonly observed among overhead athletes and individuals with shoulder pathologies, with prevalence rates reported between 61% to 100% depending on the population and assessment methods [20, 21]. Kibler et al. categorized scapular dyskinesis into three main types: Type I (prominence of the inferomedial border), type II (prominence of the entire medial border), and type III (excessive elevation and shrugging during arm elevation), each reflecting specific muscular imbalances, such as serratus anterior weakness or upper trapezius overactivity [22]. The etiology of scapular dyskinesis is multifactorial, including neuromuscular imbalance, poor posture, nerve injury (e.g. long thoracic nerve palsy), and repetitive overhead movements [23]. These alterations disrupt scapulohumeral rhythm and glenohumeral joint mechanics, increasing the risk of subacromial impingement, labral injuries, and rotator cuff pathology [24]. Clinically, it can be identified using tests, such as the scapular dyskinesis test (SDT), Scapular Assistance Test, and Lateral Scapular Slide Test, which are reliable tools for detection and functional evaluation [25]. Treatment typically focuses on neuromuscular re-education, strengthening of stabilizing muscles (particularly lower trapezius and serratus anterior), and postural correction strategies [26]. Consequently, early recognition and correction of scapular dyskinesis are crucial in restoring optimal shoulder biomechanics and preventing secondary injuries [27].
The scapula plays a crucial role in maintaining glenohumeral stability and ensuring the efficient transmission of kinetic energy from the lower extremities to the upper limbs [28, 29]. Dyskinesis is associated with disrupted scapulohumeral rhythm, leading to compromised shoulder mechanics and increased injury risk [30]. It is typically characterized by abrupt or exaggerated protraction and elevation during arm lifting, as well as accelerated downward rotation when the arm is lowered [25, 31].
Contributing factors include abnormal recruitment patterns in stabilizing muscles, skeletal malalignment, structural joint instability, and altered soft tissue or neural input [30, 31]. Scapular dysfunction may result in a winged scapula, seen as the prominence of the medial border or inferior angle detaching from the thoracic wall, often due to delayed activation or weakness in the serratus anterior and lower trapezius muscles [25, 31-33]. Furthermore, limited flexibility of the pectoralis minor and the short head of the biceps brachii has been associated with excessive anterior tilting and forward movement of the scapula [34].
Muscle imbalance frequently observed in overhead athletes with overuse pain syndromes can inhibit proper scapular stabilizer activation, further contributing to dysfunctional scapular motion [24, 35-37]. These neuromuscular and biomechanical disturbances may lead to increased stress on the anterior shoulder capsule, rotator cuff compression, and reduced functional performance. Imbalances among key muscles such as the serratus anterior, trapezius, pectoralis minor, rhomboids, and levator scapulae negatively affect scapulohumeral rhythm and shoulder joint function [38].
Considering the high prevalence of shoulder and scapular dysfunction in CrossFit athletes and the lack of sufficient research on corrective interventions in this population, this study aimed to evaluate the effects of a six-week corrective exercise program on shoulder stability in male CrossFit athletes with scapular dyskinesis, in order to improve movement mechanics, musculoskeletal alignment, and reduce the risk of injury.
Materials and Methods
A total of 24 male CrossFit athletes, aged between 25 and 30 years, who had a minimum of two years of continuous training experience and a clinical diagnosis of scapular movement dysfunction, participated in this study. The sample size was determined with G*Power software, version 3.1, drawing on earlier clinical trials that examined scapular stabilization programs. The calculation was performed using the following parameters: effect size=0.54, α=0.05, and statistical power=80% (1−β=0.80), which yielded a minimum of 24 participants (12 per group). To allow for a potential 10% dropout, the final sample size was increased to 26.
To clarify the recruitment and allocation process, a CONSORT-style flow diagram was provided (Figure 1).
Initially, 26 CrossFit athletes were assessed for eligibility, all of whom met the inclusion criteria and were randomized into intervention (n=13) and control (n=13) groups. During the study, two participants from the control group were lost to follow-up due to absence in the post-test phase. Therefore, the final analysis included 24 participants (intervention=13, control=11).
The chosen sample size aligns with previous intervention-based research. For instance, Turgut et al. (2017) performed a randomized controlled study on scapular stabilization exercises in individuals with subacromial pain syndrome, involving 30 participants divided equally into two groups of 15 [39]. Similarly, Buttagat et al. (2023) investigated posture correction and mobility improvements using scapular-based interventions, involving 48 participants (24 per group) [40].
The eligibility requirements included being male, an age range of 25–30 years, a minimum of two years of prior CrossFit training, regular attendance in training sessions (at least three times per week), and a clinical diagnosis of scapular movement dysfunction. The exclusion criteria included unwillingness to participate in training or assessment, absence from at least three consecutive sessions, shoulder pain affecting functional task execution, engagement in other professional sports, history of cardiopulmonary, orthopedic, or neuromuscular disorders (based on informed consent, observation, and coach input), and thoracic kyphosis greater than 45°.
Scapular movement dysfunction was assessed using a standardized clinical protocol. Participants performed bilateral shoulder flexion and abduction with 5 kg dumbbells, with each task was performed five times, each phase lasting 3 s. Two independent kinesiologists evaluated scapular rhythm, symmetry, winging, and tilting. If abnormal movement was present in three or more of fiverepetitions, the result was recorded as positive [41, 42].
The outcome of the test was dichotomized as “positive” (indicating observed changes in rhythm or scapular winging) or “negative.” Correspondingly, “Yes” or “No” was recorded for each participant [42].
Scapular dysfunction diagnosis
Scapular dysfunction was diagnosed using the SDT. This test involved assessing scapular movement patterns during shoulder flexion and abduction exercises. Participants performed five repetitions for each movement, with each phase of the movement lasting approximately 3 s. The scoring method was as follows: A) Normal movement: No observable abnormal scapular movement. B) Mildly abnormal movement: Slightly abnormal or suspicious scapular movement. C) Clearly abnormal movement: Evident abnormal scapular movement in at least 3 out of 5 repetitions.
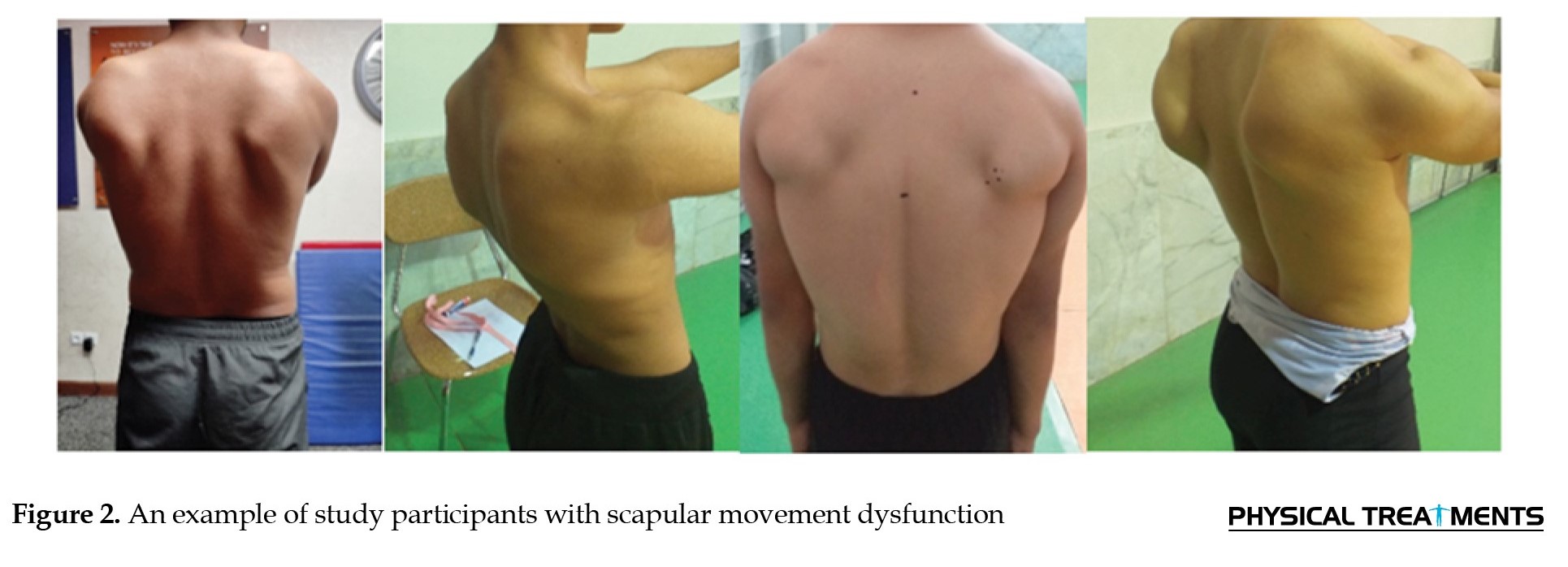
The final score was determined based on a combination of the flexion and abduction tests: Normal: Both tests are normal, or one test is mildly abnormal. 1) Suspiciously abnormal: Both tests are mildly abnormal. 2) Clearly abnormal: One or both tests are clearly abnormal. 3) Of the participants, 25% showed “clearly abnormal” scapular movement patterns. Figure 2 shows an example of a participant with scapular movement dysfunction.
The chosen sample size aligns with previous intervention-based research. For instance, Turgut et al. (2017) performed a randomized controlled study on scapular stabilization exercises in individuals with subacromial pain syndrome, involving 30 participants divided equally into two groups of 15 [39]. Similarly, Buttagat et al. (2023) investigated posture correction and mobility improvements using scapular-based interventions, involving 48 participants (24 per group) [40].
The eligibility requirements included being male, an age range of 25–30 years, a minimum of two years of prior CrossFit training, regular attendance in training sessions (at least three times per week), and a clinical diagnosis of scapular movement dysfunction. The exclusion criteria included unwillingness to participate in training or assessment, absence from at least three consecutive sessions, shoulder pain affecting functional task execution, engagement in other professional sports, history of cardiopulmonary, orthopedic, or neuromuscular disorders (based on informed consent, observation, and coach input), and thoracic kyphosis greater than 45°.
Scapular movement dysfunction was assessed using a standardized clinical protocol. Participants performed bilateral shoulder flexion and abduction with 5 kg dumbbells, with each task was performed five times, each phase lasting 3 s. Two independent kinesiologists evaluated scapular rhythm, symmetry, winging, and tilting. If abnormal movement was present in three or more of fiverepetitions, the result was recorded as positive [41, 42].
The outcome of the test was dichotomized as “positive” (indicating observed changes in rhythm or scapular winging) or “negative.” Correspondingly, “Yes” or “No” was recorded for each participant [42].
Scapular dysfunction diagnosis
Scapular dysfunction was diagnosed using the SDT. This test involved assessing scapular movement patterns during shoulder flexion and abduction exercises. Participants performed five repetitions for each movement, with each phase of the movement lasting approximately 3 s. The scoring method was as follows: A) Normal movement: No observable abnormal scapular movement. B) Mildly abnormal movement: Slightly abnormal or suspicious scapular movement. C) Clearly abnormal movement: Evident abnormal scapular movement in at least 3 out of 5 repetitions.
The final score was determined based on a combination of the flexion and abduction tests: Normal: Both tests are normal, or one test is mildly abnormal. 1) Suspiciously abnormal: Both tests are mildly abnormal. 2) Clearly abnormal: One or both tests are clearly abnormal. 3) Of the participants, 25% showed “clearly abnormal” scapular movement patterns. Figure 2 shows an example of a participant with scapular movement dysfunction.
This diagnostic method has demonstrated moderate to good levels of validity and reliability, with reported coefficients ranging from approximately 0.57 [25, 33, 41].
Scapular dyskinesis and stability assessment
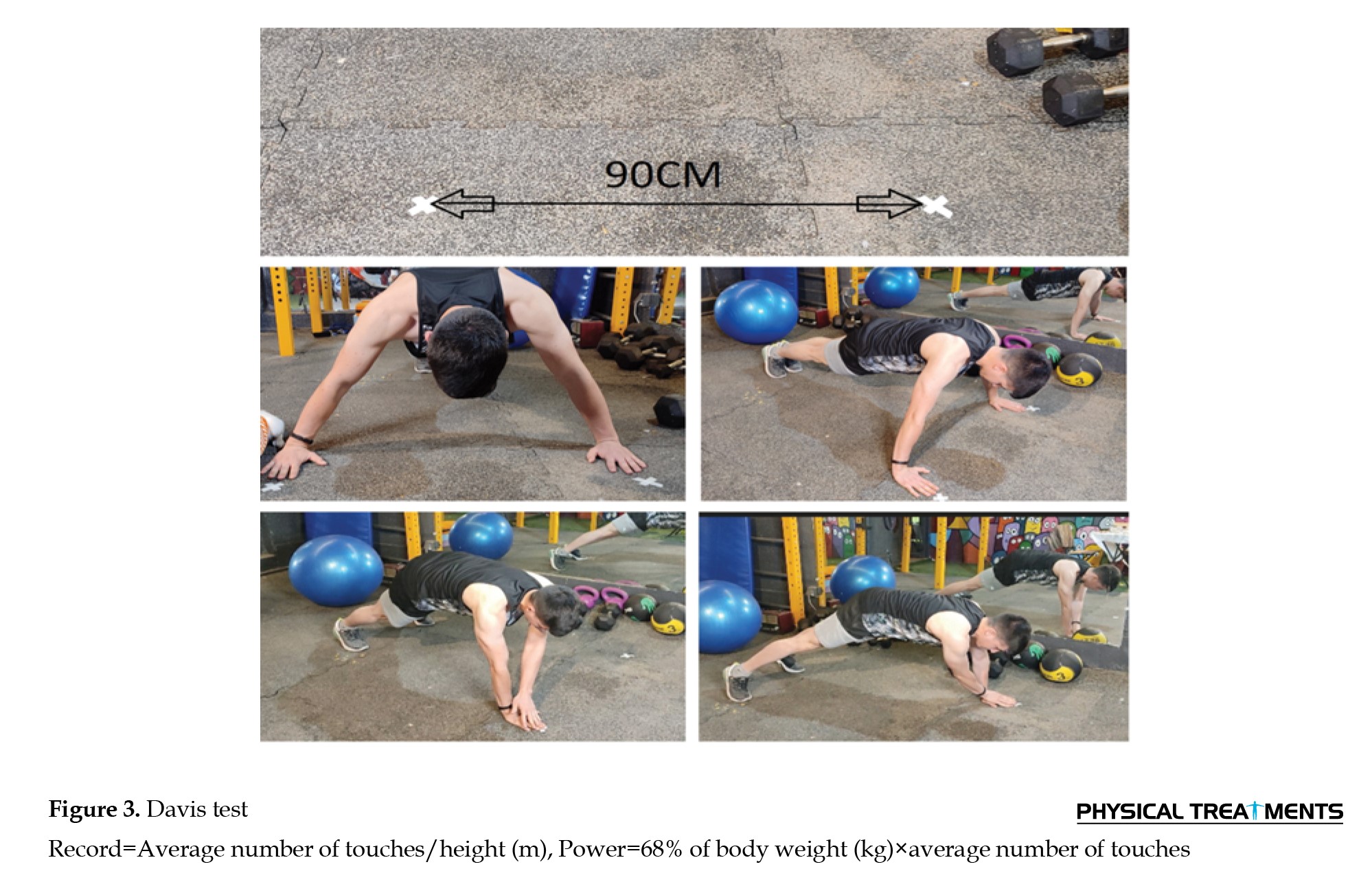
The Davis Test for scapular stability was employed to assess the effectiveness of the intervention. The Davis test setup and power calculation are illustrated in Figure 3.
Scapular dyskinesis and stability assessment
The Davis Test for scapular stability was employed to assess the effectiveness of the intervention. The Davis test setup and power calculation are illustrated in Figure 3.
This test involves calculating power output using 68% of the participant’s body weight. This method has been validated in previous studies for shoulder stability assessments [43], and is widely accepted because it provides an accurate measure of relative power output, particularly when compared to methods using fixed loads.
For the test administration, participants assumed a stable stance, similar to a push-up position, with their hands placed 90 cm (36 inches) apart. Each trial lasted 15 seconds, during which they alternately touched one hand to the other, followed by a 45-second recovery. This procedure was performed three times per participant. Results for performance and power output were calculated through established formulas. Previous studies have confirmed the Davis test as a highly valid and reliable assessment, with reliability coefficients reported between 0.90 and 0.92 [44-48].
For scapular dyskinesis assessment, the SDT was used to evaluate the severity of scapular dysfunction. This test assesses scapular movement patterns during shoulder flexion and abduction exercises. The scoring method involves categorizing movement as normal, mildly abnormal, or clearly abnormal, based on observable deviations in at least three out of five repetitions. Participants who demonstrated clearly abnormal movement in at least 3 out of 5 repetitions were diagnosed with scapular dyskinesis. In the current study, 25% of the participants showed “clearly abnormal” scapular movement patterns.[49, 50].
While the reliability coefficient for the SDT (κ=0.57) is considered moderate, it suggests the potential for measurement error due to factors such as inter-rater variability and the subjective nature of scapular movement evaluations. To minimize these errors, future studies could benefit from incorporating more standardized protocols and more reliable methods. Despite this, the SDT remains a valuable tool for assessing scapular dyskinesis in both clinical and athletic settings [51].
Training protocol
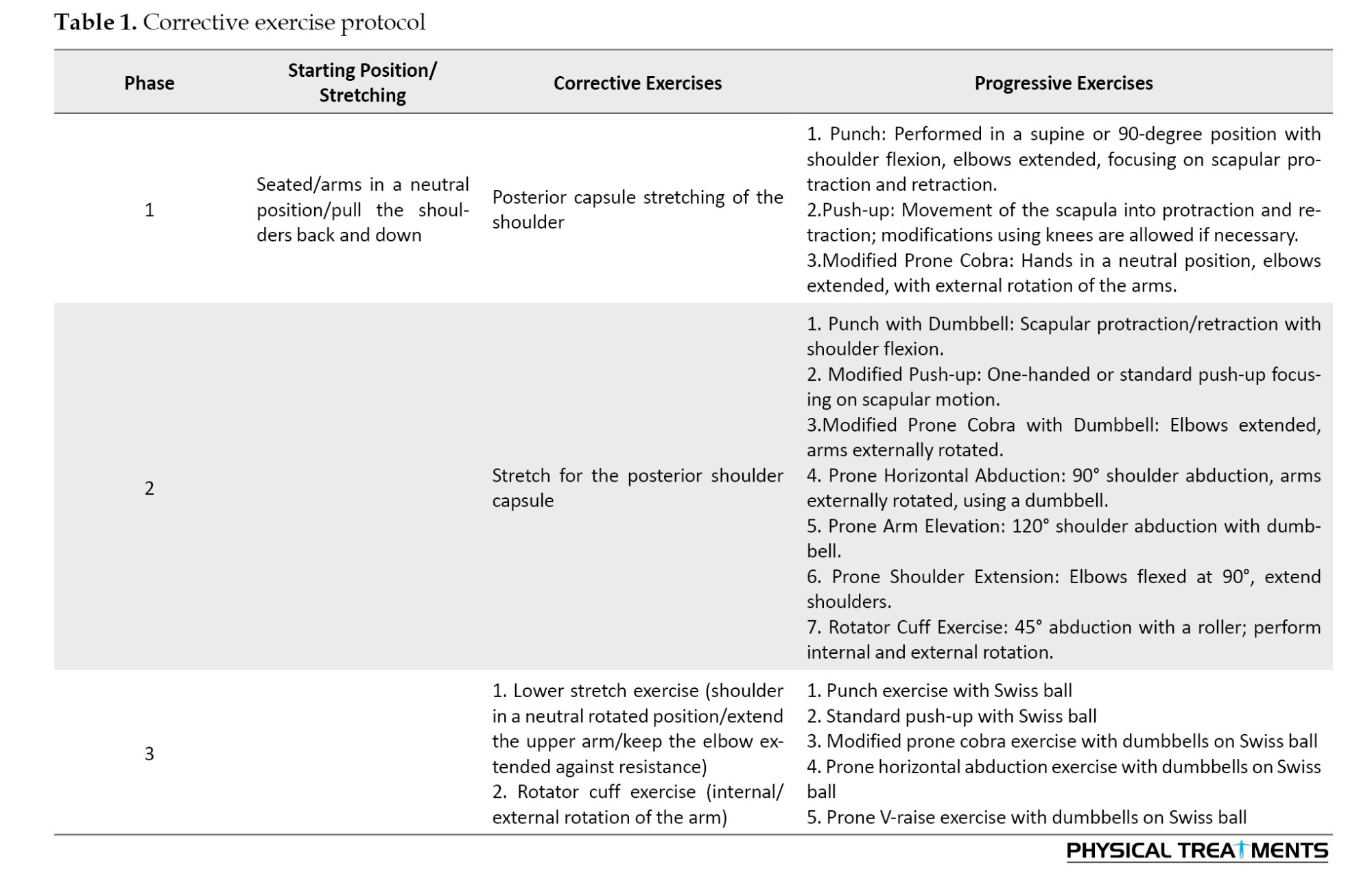
The selected training program was adapted from Mora et al. [52, 53] and modified for participants with movement dysfunction. It included three phases: exercises to increase range of motion and teach scapular control, exercises targeting scapular muscles, and advanced sensorimotor exercises emphasizing scapular stability and alignment [24, 41, 54]. All exercises were performed in three sets of 15 repetitions, while stretching exercises were held for 20–30 seconds in three sets. The intervention was conducted over a six-week period, during which the experimental group trained three times each week. The detailed corrective exercise protocol is presented in Table 1.
The intervention protocol was designed to progressively improve scapular stability through targeted corrective exercises. Intensity was regulated using the Borg Rating of Perceived Exertion scale, with a targeted range of 12–15 on the scale [55]. This range was chosen to ensure that participants experienced moderate to vigorous intensity without overexertion.
Progression of resistance/loads was structured as follows: 1) Week 1–2: Participants performed exercises at low resistance (e.g. bodyweight or light resistance bands). 2) Week 3–4: Resistance was gradually increased by 10–15% each week based on participants’ ability to complete the prescribed sets and repetitions with proper form. 3) Week 5–6: Resistance was further increased, with weekly adjustments based on individual progress, aiming for moderate to heavy resistance (e.g. dumbbells, resistance bands) [56].
The control group maintained their regular CrossFit training schedule throughout the study, which included their typical exercises (e.g. weightlifting, metabolic conditioning). The potential confounding effects of this were considered, and although both groups underwent similar training schedules, it was ensured that the intervention group received additional specific corrective exercises designed to target scapular stability. The impact of the control group’s regular training was analyzed, and it was found that any changes observed in the intervention group were not attributable to CrossFit training alone but rather to the additional exercises.
Statistical method
Data were analyzed using SPSS software, version 26. The Shapiro–Wilk test was applied to assess data distribution. Since the results confirmed normality, between-group comparisons were conducted using analysis of covariance (ANCOVA), and within-group changes were evaluated with paired t-tests. Statistical significance was set at P<0.05.
Ethical considerations
All individuals participated in the study voluntarily and signed written informed consent forms. Before the research began, the procedures, testing protocols, and possible risks were fully explained to them. Participants were guaranteed complete confidentiality of their personal data, which was accessible only to the main investigator.
Results
A total of 26 male CrossFit athletes initially participated in the study (13 in each group). However, due to the absence of two participants from the control group in the post-test phase, the final analysis was conducted on 24 participants: 13 in the training group and 11 in the control group.
Table 2 presents the anthropometric characteristics of the participants, including age, height, weight, and body mass index (BMI).
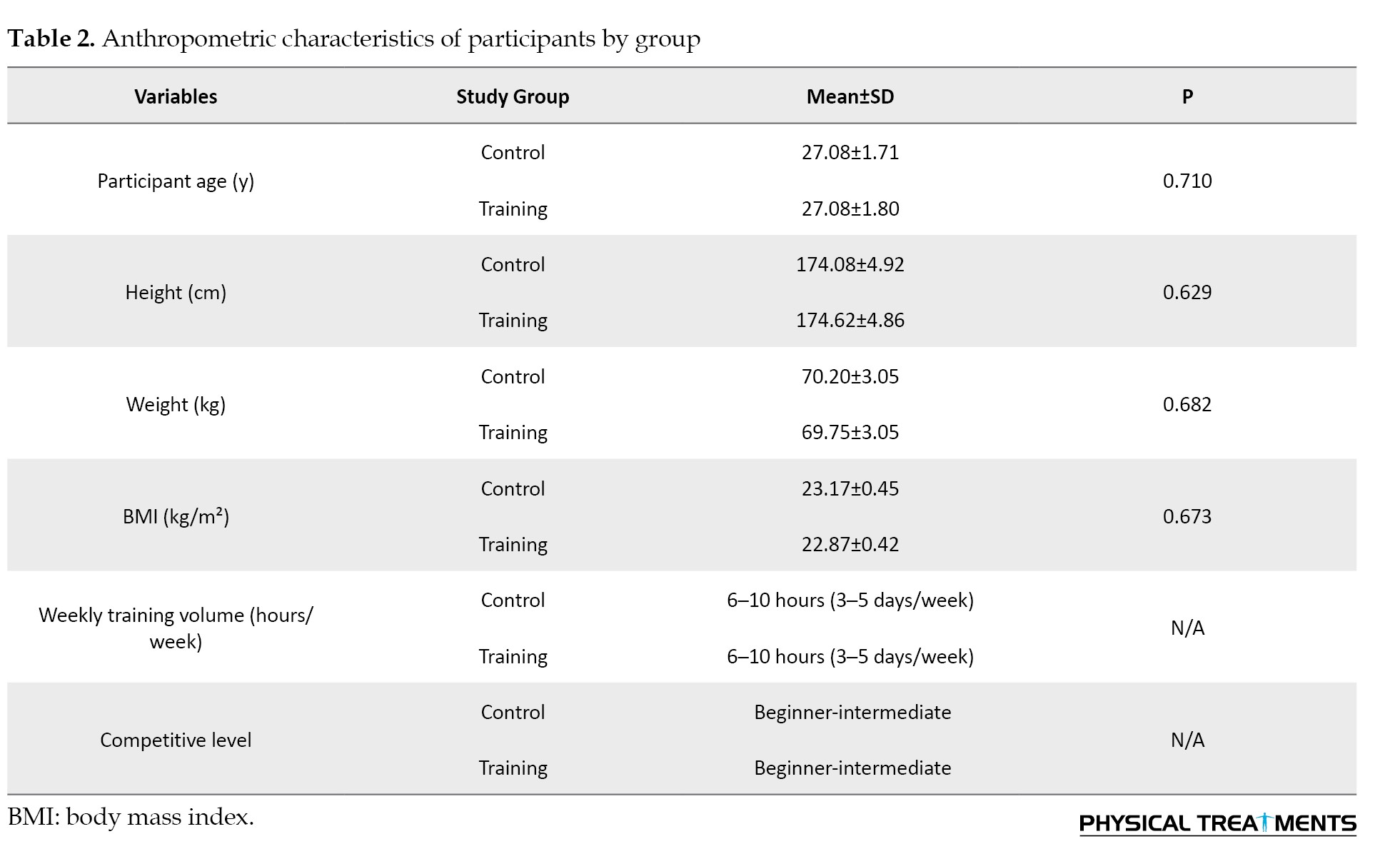
Independent t-tests revealed no statistically significant differences between the groups in any of the measured variables (P>0.05), confirming baseline homogeneity. Table 2 also includes participants’ characteristics regarding weekly training volume and competitive level.
Normality of the dependent variables was examined using the Shapiro–Wilk test, which indicated that all variables were normally distributed (P>0.05). This verified the assumptions required for applying parametric methods. To further check the appropriateness of these analyses, Levene’s test was used to evaluate variance homogeneity between the intervention and control groups. The findings for both outcomes (Davis test record and power output) showed non-significant results (P>0.05), confirming equal variances and thus allowing the use of ANCOVA.
Following confirmation of these assumptions, paired sample t-tests were used to analyze within-group differences, while ANCOVA was applied to compare between-group differences, adjusting for pre-test scores. This approach ensured that any observed differences between groups could be attributed to the intervention, rather than baseline differences or random variations.
Paired sample t-test analyses demonstrated significant improvements in the training group across all scapular stability measures, such as test record and power output (P<0.01). Conversely, the control group did not exhibit any meaningful differences between pre and post-test assessments (P>0.05) (Table 3).
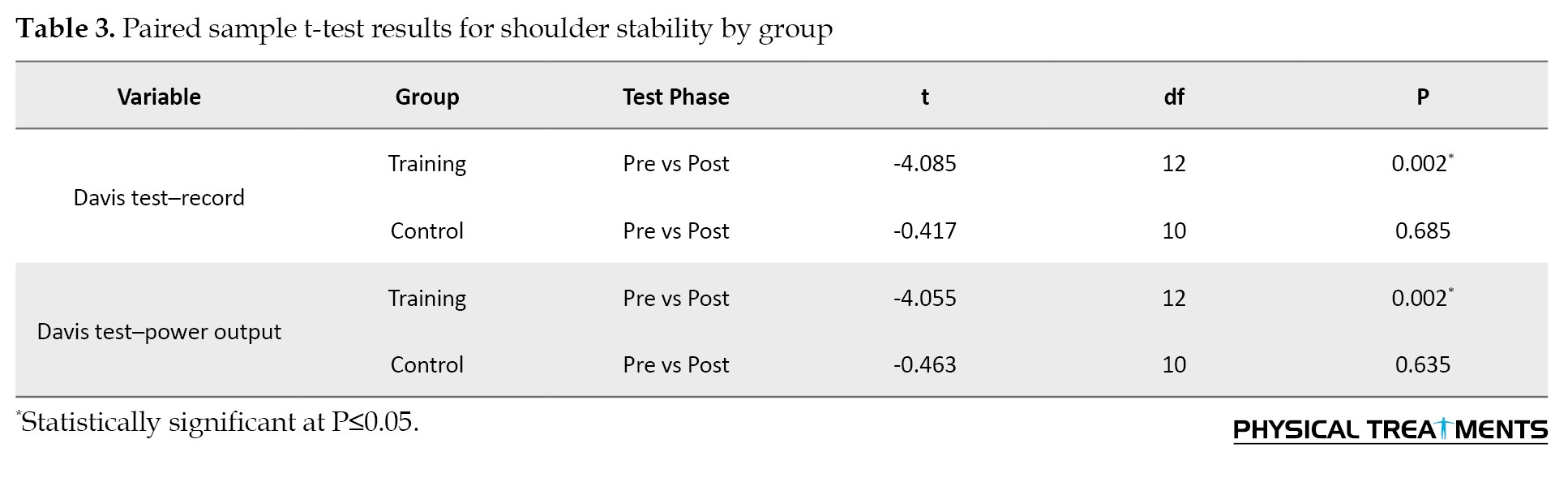
The paired sample t-test results revealed that the training group showed statistically significant improvements in both shoulder performance indicators, test record and power output, following the six-week corrective exercise program (P=0.002 for both variables).
These findings indicate that the intervention effectively enhanced shoulder stability among male CrossFit athletes diagnosed with scapular movement dysfunction.
In contrast, the control group did not exhibit any significant changes in either metric (P=0.685 for record; P=0.635 for power output), suggesting that the observed improvements in the training group were attributable to the intervention rather than natural progression or external factors.
These findings support the first research hypothesis, demonstrating that targeted corrective exercises can meaningfully improve dynamic shoulder stability in athletes with scapular dyskinesis. Prior to conducting the ANCOVA, Levene’s test was performed to assess the assumption of homogeneity of variances between the training and control groups. The results of Levene’s test for both outcome variables, Davis Test record (P=0.51) and Power Output (P=0.54), indicated that the assumption of equal variances was met (P>0.05). Therefore, it was appropriate to proceed with the ANCOVA analysis under the assumption of homogeneity of variances.
To assess the effectiveness of the corrective exercise program on shoulder stability between the two groups, an ANCOVA was conducted. This test compared the post-test values of the Davis test variables (record and power output) between the training and control groups while adjusting for pre-test scores as covariates. Table 4 presents the results.
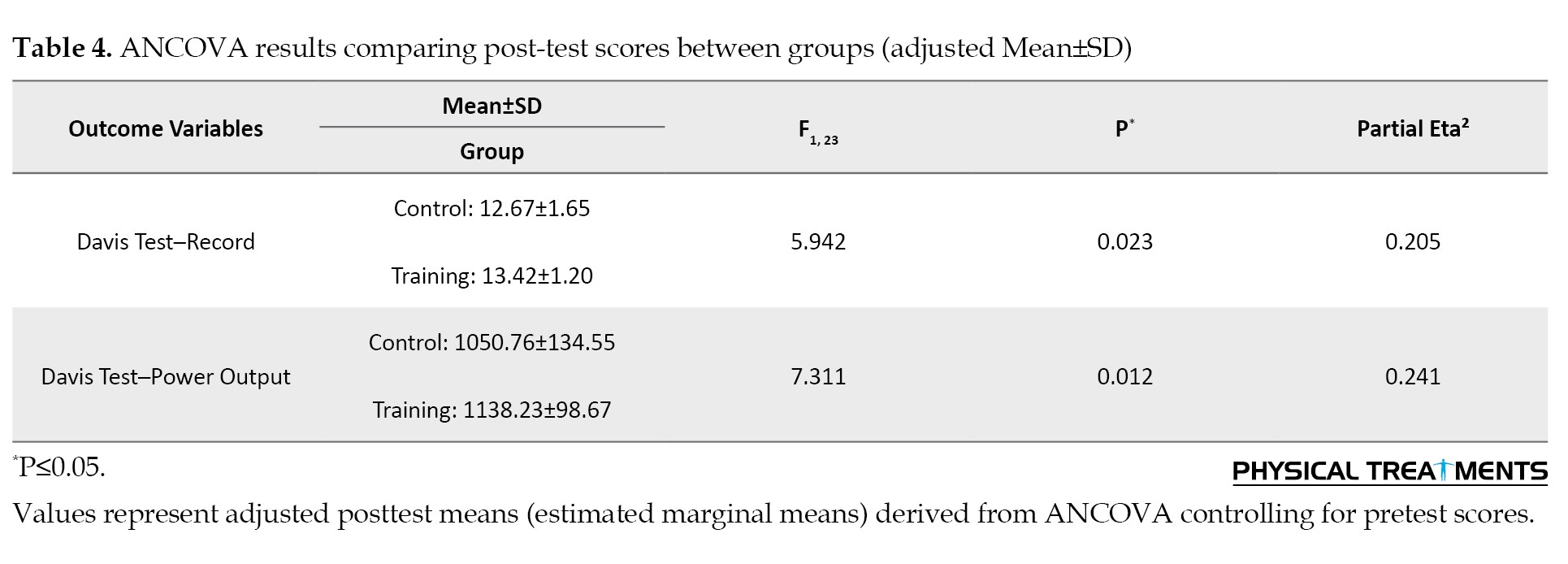
The ANCOVA results demonstrated statistically significant differences between the training and control groups for both key performance indicators. For Davis test record, the adjusted mean scores differed significantly (F1, 23=5.942, P=0.023), with a moderate effect size (η²=0.205). For power output, the difference was greater (F1,23=7.311, P=0.012), reflecting a strong effect size (η²=0.241).
These findings align with the within-group t-test results and confirm that the six-week corrective exercise program produced meaningful improvements in scapular stability among male CrossFit athletes with scapular dyskinesis. The combination of statistical significance and moderate-to-strong effect sizes indicates both clinical relevance and robustness of the intervention’s impact.
Discussion
This study aimed to examine the effect of a six-week corrective exercise program on shoulder stability in male CrossFit athletes with scapular movement dysfunction. The findings demonstrated a statistically significant improvement in shoulder stability in the intervention group following the training period, indicating that the applied protocol effectively enhanced neuromuscular control and functional stabilization of the glenohumeral joint.
Shoulder stability, especially in overhead athletes, depends largely on the dynamic regulation of the scapulohumeral complex. Given the inherent structural mobility and shallow socket of the glenohumeral joint, its functional integrity is critically reliant on the coordinated activation of stabilizing muscles. Scapular dyskinesis, characterized by altered scapular positioning and motion, often disrupts this coordination, leading to abnormal loading patterns, increased posterior capsule stress, and compromised dynamic centralization of the humeral head [19, 57].
The exercise protocol used in this study specifically targeted key stabilizers of the scapula, including the serratus anterior and lower trapezius, while aiming to reduce the overactivity of the upper trapezius. By promoting balanced muscle activation patterns and enhancing proprioceptive feedback, the intervention contributed to restoring scapular control and shoulder joint stability. These outcomes are consistent with findings by Pashaei (2022), Eyvazi (2020), and Haji Hosseini (2019), who reported that targeted corrective training improved dynamic shoulder function in overhead athletes [58-60].
From a biomechanical perspective, improving the eccentric function of the rotator cuff muscles is essential to maintaining central humeral head alignment during deceleration and overhead movements. Ellenbecker and Cools (2010) highlighted that deficits in eccentric control can contribute to cumulative microtrauma and instability, and emphasized the importance of exercise-based rehabilitation for injury prevention [61].
Clinically, Owens et al. (2007) reported that over 85% of shoulder instability cases in overhead athletes stem from repetitive micro-subluxations caused by inadequate neuromuscular control [62]. This finding further supports the necessity of implementing structured corrective exercise protocols, particularly in high-demand sports such as CrossFit, which impose considerable mechanical stress on the shoulder complex. Thus, the present results validate the first hypothesis of the study and highlight the potential of functionally oriented exercise programs to improve shoulder stability and reduce injury risk in athletes with scapular dysfunction.
Conclusion
The findings of this study revealed that a six-week targeted corrective exercise program significantly improved shoulder stability in male CrossFit athletes exhibiting scapular movement dysfunction. These results suggest that incorporating corrective exercises can effectively enhance scapular control and reduce dysfunctional movement patterns. Strengthening both dynamic and static stabilizers of the shoulder joint appears to play a critical role in maintaining scapular stability under various loading conditions and across a range of motion and postural demands.
Research suggestions
Based on the findings of this study, it is recommended that sports therapists and rehabilitation specialists utilize these results to design targeted corrective and therapeutic programs aimed at improving scapular rhythm, positioning, and shoulder stability in athletes with scapular dyskinesis. Preventive training programs should also emphasize the correction of functional deficits and enhancement of proper movement patterns. Coaches are advised to evaluate and adjust technical execution in CrossFit athletes to reduce the risk of injury and improve performance. At the foundational level, proper movement education and early identification of dysfunctions—along with timely referral to specialists—are essential. Future research should expand the age range of participants and utilize more advanced biomechanical assessment tools. It is also suggested to investigate the effects of the corrective exercises on additional variables such as arm rotation and neuromuscular control indices. Moreover, given the prevalence of other injuries, such as knee disorders in CrossFit athletes, similar research should be conducted on other musculoskeletal issues. Finally, the effectiveness of the corrective exercises should also be examined in female CrossFit athletes to determine their broader applicability.
Research limitations
One of the main limitations of this study was the relatively small sample size, which may reduce the generalizability of the findings to broader athletic populations. Outcome assessments were not blinded, which may introduce potential observer bias. The study focused exclusively on male CrossFit athletes aged 25–30 years, limiting the extrapolation of results to female athletes or older participants. Additionally, the specific type of scapular dyskinesis was not classified according to established categories, such as Kibler’s types; only its presence or absence was assessed, which may limit analytical depth and comparability with previous studies. The assessment relied on visual observation, which, although widely used in clinical and field settings, may lack the precision of advanced tools such as 3D motion analysis or imaging systems. Furthermore, no long-term follow-up was conducted, restricting the ability to evaluate the sustainability of intervention effects.
Ethical Considerations
Compliance with ethical guidelines
The research was approved by the Ethics Committee of Shahid Beheshti University of Medical Sciences, Tehran, Iran (Code: IR.SBU.REC.1401.063).
Funding
This research received no specific grant from any funding agency in the public commercial, or non-profit sectors.
Authors' contributions
All authors contributed equally to the conception and design of the study, data collection and analysis, interpretation of the results, and drafting of the manuscript. Each author approved the final version of the manuscript for submission.
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgments
The authors sincerely thank all individuals who contributed to the completion of this study, including the CrossFit athletes who participated in the research and the local CrossFit club that supported the execution of this project.
For the test administration, participants assumed a stable stance, similar to a push-up position, with their hands placed 90 cm (36 inches) apart. Each trial lasted 15 seconds, during which they alternately touched one hand to the other, followed by a 45-second recovery. This procedure was performed three times per participant. Results for performance and power output were calculated through established formulas. Previous studies have confirmed the Davis test as a highly valid and reliable assessment, with reliability coefficients reported between 0.90 and 0.92 [44-48].
For scapular dyskinesis assessment, the SDT was used to evaluate the severity of scapular dysfunction. This test assesses scapular movement patterns during shoulder flexion and abduction exercises. The scoring method involves categorizing movement as normal, mildly abnormal, or clearly abnormal, based on observable deviations in at least three out of five repetitions. Participants who demonstrated clearly abnormal movement in at least 3 out of 5 repetitions were diagnosed with scapular dyskinesis. In the current study, 25% of the participants showed “clearly abnormal” scapular movement patterns.[49, 50].
While the reliability coefficient for the SDT (κ=0.57) is considered moderate, it suggests the potential for measurement error due to factors such as inter-rater variability and the subjective nature of scapular movement evaluations. To minimize these errors, future studies could benefit from incorporating more standardized protocols and more reliable methods. Despite this, the SDT remains a valuable tool for assessing scapular dyskinesis in both clinical and athletic settings [51].
Training protocol
The selected training program was adapted from Mora et al. [52, 53] and modified for participants with movement dysfunction. It included three phases: exercises to increase range of motion and teach scapular control, exercises targeting scapular muscles, and advanced sensorimotor exercises emphasizing scapular stability and alignment [24, 41, 54]. All exercises were performed in three sets of 15 repetitions, while stretching exercises were held for 20–30 seconds in three sets. The intervention was conducted over a six-week period, during which the experimental group trained three times each week. The detailed corrective exercise protocol is presented in Table 1.
The intervention protocol was designed to progressively improve scapular stability through targeted corrective exercises. Intensity was regulated using the Borg Rating of Perceived Exertion scale, with a targeted range of 12–15 on the scale [55]. This range was chosen to ensure that participants experienced moderate to vigorous intensity without overexertion.
Progression of resistance/loads was structured as follows: 1) Week 1–2: Participants performed exercises at low resistance (e.g. bodyweight or light resistance bands). 2) Week 3–4: Resistance was gradually increased by 10–15% each week based on participants’ ability to complete the prescribed sets and repetitions with proper form. 3) Week 5–6: Resistance was further increased, with weekly adjustments based on individual progress, aiming for moderate to heavy resistance (e.g. dumbbells, resistance bands) [56].
The control group maintained their regular CrossFit training schedule throughout the study, which included their typical exercises (e.g. weightlifting, metabolic conditioning). The potential confounding effects of this were considered, and although both groups underwent similar training schedules, it was ensured that the intervention group received additional specific corrective exercises designed to target scapular stability. The impact of the control group’s regular training was analyzed, and it was found that any changes observed in the intervention group were not attributable to CrossFit training alone but rather to the additional exercises.
Statistical method
Data were analyzed using SPSS software, version 26. The Shapiro–Wilk test was applied to assess data distribution. Since the results confirmed normality, between-group comparisons were conducted using analysis of covariance (ANCOVA), and within-group changes were evaluated with paired t-tests. Statistical significance was set at P<0.05.
Ethical considerations
All individuals participated in the study voluntarily and signed written informed consent forms. Before the research began, the procedures, testing protocols, and possible risks were fully explained to them. Participants were guaranteed complete confidentiality of their personal data, which was accessible only to the main investigator.
Results
A total of 26 male CrossFit athletes initially participated in the study (13 in each group). However, due to the absence of two participants from the control group in the post-test phase, the final analysis was conducted on 24 participants: 13 in the training group and 11 in the control group.
Table 2 presents the anthropometric characteristics of the participants, including age, height, weight, and body mass index (BMI).
Independent t-tests revealed no statistically significant differences between the groups in any of the measured variables (P>0.05), confirming baseline homogeneity. Table 2 also includes participants’ characteristics regarding weekly training volume and competitive level.
Normality of the dependent variables was examined using the Shapiro–Wilk test, which indicated that all variables were normally distributed (P>0.05). This verified the assumptions required for applying parametric methods. To further check the appropriateness of these analyses, Levene’s test was used to evaluate variance homogeneity between the intervention and control groups. The findings for both outcomes (Davis test record and power output) showed non-significant results (P>0.05), confirming equal variances and thus allowing the use of ANCOVA.
Following confirmation of these assumptions, paired sample t-tests were used to analyze within-group differences, while ANCOVA was applied to compare between-group differences, adjusting for pre-test scores. This approach ensured that any observed differences between groups could be attributed to the intervention, rather than baseline differences or random variations.
Paired sample t-test analyses demonstrated significant improvements in the training group across all scapular stability measures, such as test record and power output (P<0.01). Conversely, the control group did not exhibit any meaningful differences between pre and post-test assessments (P>0.05) (Table 3).
The paired sample t-test results revealed that the training group showed statistically significant improvements in both shoulder performance indicators, test record and power output, following the six-week corrective exercise program (P=0.002 for both variables).
These findings indicate that the intervention effectively enhanced shoulder stability among male CrossFit athletes diagnosed with scapular movement dysfunction.
In contrast, the control group did not exhibit any significant changes in either metric (P=0.685 for record; P=0.635 for power output), suggesting that the observed improvements in the training group were attributable to the intervention rather than natural progression or external factors.
These findings support the first research hypothesis, demonstrating that targeted corrective exercises can meaningfully improve dynamic shoulder stability in athletes with scapular dyskinesis. Prior to conducting the ANCOVA, Levene’s test was performed to assess the assumption of homogeneity of variances between the training and control groups. The results of Levene’s test for both outcome variables, Davis Test record (P=0.51) and Power Output (P=0.54), indicated that the assumption of equal variances was met (P>0.05). Therefore, it was appropriate to proceed with the ANCOVA analysis under the assumption of homogeneity of variances.
To assess the effectiveness of the corrective exercise program on shoulder stability between the two groups, an ANCOVA was conducted. This test compared the post-test values of the Davis test variables (record and power output) between the training and control groups while adjusting for pre-test scores as covariates. Table 4 presents the results.
The ANCOVA results demonstrated statistically significant differences between the training and control groups for both key performance indicators. For Davis test record, the adjusted mean scores differed significantly (F1, 23=5.942, P=0.023), with a moderate effect size (η²=0.205). For power output, the difference was greater (F1,23=7.311, P=0.012), reflecting a strong effect size (η²=0.241).
These findings align with the within-group t-test results and confirm that the six-week corrective exercise program produced meaningful improvements in scapular stability among male CrossFit athletes with scapular dyskinesis. The combination of statistical significance and moderate-to-strong effect sizes indicates both clinical relevance and robustness of the intervention’s impact.
Discussion
This study aimed to examine the effect of a six-week corrective exercise program on shoulder stability in male CrossFit athletes with scapular movement dysfunction. The findings demonstrated a statistically significant improvement in shoulder stability in the intervention group following the training period, indicating that the applied protocol effectively enhanced neuromuscular control and functional stabilization of the glenohumeral joint.
Shoulder stability, especially in overhead athletes, depends largely on the dynamic regulation of the scapulohumeral complex. Given the inherent structural mobility and shallow socket of the glenohumeral joint, its functional integrity is critically reliant on the coordinated activation of stabilizing muscles. Scapular dyskinesis, characterized by altered scapular positioning and motion, often disrupts this coordination, leading to abnormal loading patterns, increased posterior capsule stress, and compromised dynamic centralization of the humeral head [19, 57].
The exercise protocol used in this study specifically targeted key stabilizers of the scapula, including the serratus anterior and lower trapezius, while aiming to reduce the overactivity of the upper trapezius. By promoting balanced muscle activation patterns and enhancing proprioceptive feedback, the intervention contributed to restoring scapular control and shoulder joint stability. These outcomes are consistent with findings by Pashaei (2022), Eyvazi (2020), and Haji Hosseini (2019), who reported that targeted corrective training improved dynamic shoulder function in overhead athletes [58-60].
From a biomechanical perspective, improving the eccentric function of the rotator cuff muscles is essential to maintaining central humeral head alignment during deceleration and overhead movements. Ellenbecker and Cools (2010) highlighted that deficits in eccentric control can contribute to cumulative microtrauma and instability, and emphasized the importance of exercise-based rehabilitation for injury prevention [61].
Clinically, Owens et al. (2007) reported that over 85% of shoulder instability cases in overhead athletes stem from repetitive micro-subluxations caused by inadequate neuromuscular control [62]. This finding further supports the necessity of implementing structured corrective exercise protocols, particularly in high-demand sports such as CrossFit, which impose considerable mechanical stress on the shoulder complex. Thus, the present results validate the first hypothesis of the study and highlight the potential of functionally oriented exercise programs to improve shoulder stability and reduce injury risk in athletes with scapular dysfunction.
Conclusion
The findings of this study revealed that a six-week targeted corrective exercise program significantly improved shoulder stability in male CrossFit athletes exhibiting scapular movement dysfunction. These results suggest that incorporating corrective exercises can effectively enhance scapular control and reduce dysfunctional movement patterns. Strengthening both dynamic and static stabilizers of the shoulder joint appears to play a critical role in maintaining scapular stability under various loading conditions and across a range of motion and postural demands.
Research suggestions
Based on the findings of this study, it is recommended that sports therapists and rehabilitation specialists utilize these results to design targeted corrective and therapeutic programs aimed at improving scapular rhythm, positioning, and shoulder stability in athletes with scapular dyskinesis. Preventive training programs should also emphasize the correction of functional deficits and enhancement of proper movement patterns. Coaches are advised to evaluate and adjust technical execution in CrossFit athletes to reduce the risk of injury and improve performance. At the foundational level, proper movement education and early identification of dysfunctions—along with timely referral to specialists—are essential. Future research should expand the age range of participants and utilize more advanced biomechanical assessment tools. It is also suggested to investigate the effects of the corrective exercises on additional variables such as arm rotation and neuromuscular control indices. Moreover, given the prevalence of other injuries, such as knee disorders in CrossFit athletes, similar research should be conducted on other musculoskeletal issues. Finally, the effectiveness of the corrective exercises should also be examined in female CrossFit athletes to determine their broader applicability.
Research limitations
One of the main limitations of this study was the relatively small sample size, which may reduce the generalizability of the findings to broader athletic populations. Outcome assessments were not blinded, which may introduce potential observer bias. The study focused exclusively on male CrossFit athletes aged 25–30 years, limiting the extrapolation of results to female athletes or older participants. Additionally, the specific type of scapular dyskinesis was not classified according to established categories, such as Kibler’s types; only its presence or absence was assessed, which may limit analytical depth and comparability with previous studies. The assessment relied on visual observation, which, although widely used in clinical and field settings, may lack the precision of advanced tools such as 3D motion analysis or imaging systems. Furthermore, no long-term follow-up was conducted, restricting the ability to evaluate the sustainability of intervention effects.
Ethical Considerations
Compliance with ethical guidelines
The research was approved by the Ethics Committee of Shahid Beheshti University of Medical Sciences, Tehran, Iran (Code: IR.SBU.REC.1401.063).
Funding
This research received no specific grant from any funding agency in the public commercial, or non-profit sectors.
Authors' contributions
All authors contributed equally to the conception and design of the study, data collection and analysis, interpretation of the results, and drafting of the manuscript. Each author approved the final version of the manuscript for submission.
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgments
The authors sincerely thank all individuals who contributed to the completion of this study, including the CrossFit athletes who participated in the research and the local CrossFit club that supported the execution of this project.
References
- Lichtenstein MB, Jensen TT. Exercise addiction in CrossFit: Prevalence and psychometric properties of the exercise addiction inventory. Addictive Behaviors Reports. 2016; 3:33–7. [DOI:10.1016/j.abrep.2016.02.002] [PMID]
- Tibana RA, de Farias DL, Nascimento DC, Da Silva-Grigoletto ME, Prestes J. Relação da força muscular com o desempenho no levantamento olímpico em praticantes de CrossFit®. Revista Andaluza de Medicina del Deporte. 2018; 11(2):84-8. [DOI:10.1016/j.ramd.2015.11.005]
- Butcher SJ, Neyedly TJ, Horvey KJ, Benko CR. Do physiological measures predict selected crossfit® benchmark performance?. Open Access Journal of Sports Medicine. 2015; 241-7. [PMID]
- Joondeph SA, Joondeph BC. Retinal detachment due to CrossFit training injury. Case Reports in Ophthalmological Medicine. 2013; 2013(1):189837. [DOI:10.1155/2013/189837]
- Williams S, Booton T, Watson M, Rowland D, Altini M. Heart rate variability is a moderating factor in the workload-injury relationship of competitive crossfit™ athletes. Journal of Sports Science & Medicine. 2017; 16(4):443. [PMID]
- Gillen JB, Gibala MJ. Is high-intensity interval training a time-efficient exercise strategy to improve health and fitness? Applied Physiology, Nutrition, and Metabolism. 2014; 39(3):409–12. [PMID]
- Skelly LE, Andrews PC, Gillen JB, Martin BJ, Percival ME, Gibala MJ. High-intensity interval exercise induces 24-h energy expenditure similar to traditional endurance exercise despite reduced time commitment. Applied Physiology, Nutrition, and Metabolism. 2014; 39(7):845-8. [PMID]
- Árok P, Szabo A. What makes CrossFit exercise unique? Addiction, passion, or motivation?. Sport Sciences for Health. 2025; 21(3):2167-83. [DOI:10.1007/s11332-025-01403-z]
- Heinrich KM, Patel PM, O’Neal JL, Heinrich BS. High-intensity compared to moderate-intensity training for exercise initiation, enjoyment, adherence, and intentions: An intervention study. BMC Public Health. 2014; 14(1):789. [DOI:10.1186/1471-2458-14-789]
- Ángel Rodríguez M, García-Calleja P, Terrados N, Crespo I, Del Valle M, Olmedillas H. Injury in crossfit®: A systematic review of epidemiology and risk factors. The Physician and Sportsmedicine. 2022; 50(1):3-10. [DOI:10.1080/00913847.2020.1864675]
- Vassis K, Siouras A, Kourkoulis N, Poulis IA, Meletiou G, Iliopoulou AM, Misiris I. Epidemiological Profile among Greek CrossFit Practitioners. International Journal of Environmental Research and Public Health. 2023; 20(3):2538. [DOI:10.3390/ijerph20032538] [PMID]
- Hülsmann M, Reinecke K, Barthel T, Reinsberger C. Musculoskeletal injuries in crossFit®: A systematic review and meta-analysis of injury rates and locations. Deutsche Zeitschrift Sportmed. 2021; 72:351-8. [DOI:10.5960/dzsm.2021.504]
- Wang H, Cochrane T. Mobility impairment, muscle imbalance, muscle weakness, scapular asymmetry and shoulder injury in elite volleyball athletes. Journal of Sports Medicine and Physical Fitness. 2001; 41(3):403–10. [Link]
- Claudino JG, Gabbett TJ, Bourgeois F, Souza HD, Miranda RC, Mezêncio B, et al. CrossFit overview: Systematic review and meta-analysis. Sports Medicine-Open. 2018; 4(1):11. [DOI:10.1186/s40798-018-0124-5]
- Weisenthal BM, Beck CA, Maloney MD, DeHaven KE, Giordano BD. Injury rate and patterns among CrossFit athletes. Orthopaedic Journal of Sports Medicine. 2014; 2(4):2325967114531177. [DOI:10.1177/2325967114531177]
- Toledo R, Dias MR, Souza D, Soares R, Toledo R, Lácio M, Vianna J. Joint and muscle injuries in men and women CrossFit® training participants. The Physician and Sportsmedicine. 2022; 50(3):205-11. [DOI:10.1080/00913847.2021.1892468]
- Uhl T, Sciascia A. Scapular summit 2009: Introduction. Journal of Orthopaedic & Sports Physical Therapy. 2009;39(11):a1. [PMID]
- Warner JJ, Micheli LJ, Arslanian LE, Kennedy J, Kennedy R. Scapulothoracic motion in normal shoulders and shoulders with glenohumeral instability and impingement syndrome a study using moire topographic analysis. Clinical Orthopaedics and Related Research. 1992; 285:191–9. [Link]
- Kibler WB, McMullen JO, Uhl TI. Shoulder rehabilitation strategies, guidelines, and practice. Orthopedic Clinics. 2001; 32(3):527-38. [Link]
- Struyf F, Nijs J, Baeyens JP, Mottram S, Meeusen R. Scapular positioning and movement in unimpaired shoulders, shoulder impingement syndrome, and glenohumeral instability. Scandinavian Journal of Medicine & Science in Sports. 2011; 21(3):352-8. [DOI:10.1111/j.1600-0838.2010.01274.x]
- Tate AR, McClure P, Kareha S, Irwin D. Effect of the scapula reposition test on shoulder impingement symptoms and elevation strength in overhead athletes. Journal of Orthopaedic & Sports Physical Therapy. 2008; 38(1):4–11. [DOI:10.2519/jospt.2008.2616]
- Kibler BW, Sciascia A, Wilkes T. Scapular dyskinesis and its relation to shoulder injury. JAAOS-Journal of the American Academy of Orthopaedic Surgeons. 2012; 20(6):364-72. [DOI:10.5435/JAAOS-20-06-364]
- Cools AM, Struyf F, De Mey K, Maenhout A, Castelein B, Cagnie B. Rehabilitation of scapular dyskinesis: From the office worker to the elite overhead athlete. British Journal of Sports Medicine. 2014; 48(8):692–7. [DOI:10.1136/bjsports-2013-092148]
- Ludewig PM, Reynolds JF. The association of scapular kinematics and glenohumeral joint pathologies. Journal of Orthopaedic & Sports Physical Therapy. 2009; 39(2):90–104. [DOI:10.2519/jospt.2009.2808]
- McClure P, Tate AR, Kareha S, Irwin D, Zlupko E. A clinical method for identifying scapular dyskinesis, part 1: Reliability. Journal of Athletic Training. 2009; 44(2):160–4. [Link]
- Cools AM, Witvrouw EE, Declercq GA, Danneels LA, Cambier DC. Scapular muscle recruitment patterns: Trapezius muscle latency with and without impingement symptoms. The American Journal of Sports Medicine. 2003; 31(4):542–9. [DOI:10.1177/03635465030310041101]
- Thomas SJ, Swanik KA, Swanik CB, Kelly IV JD. Internal rotation and scapular position differences: A comparison of collegiate and high school baseball players. Journal of Athletic Training. 2010; 45(1):44–50. [Link]
- Ben Kibler W, Sciascia A. Current concepts: Scapular dyskinesis. British Journal of Sports Medicine. 2010; 44(5):300–5. [DOI:10.1136/bjsm.2009.058834]
- Lugo R, Kung P, Ma CB. Shoulder biomechanics. European Journal of Radiology. 2008; 68(1):16–24. [DOI:10.1016/j.ejrad.2008.02.051]
- Kibler BW, McMullen J. Scapular dyskinesis and its relation to shoulder pain. JAAOS-Journal of the American Academy of Orthopaedic Surgeons. 2003; 11(2):142–51. [Link]
- Kibler WB, Ludewig PM, McClure PW, Michener LA, Bak K, Sciascia AD. Clinical implications of scapular dyskinesis in shoulder injury: The 2013 consensus statement from the ‘Scapular Summit’. British Journal of Sports Medicine. 2013; 47(14):877–85. [DOI:10.1136/bjsports-2013-092425]
- Ben Kibler W. The role of the scapula in athletic shoulder function. The American Journal of Sports Medicine. 1998; 26(2):325–37. [DOI:10.1177/03635465980260022801]
- Maor MB, Ronin T, Kalichman L. Scapular dyskinesis among competitive swimmers. Journal of Bodywork and Movement Therapies. 2017; 21(3):633–6. [DOI:10.1016/j.jbmt.2016.11.011]
- Borstad JD, Ludewig PM. The effect of long versus short pectoralis minor resting length on scapular kinematics in healthy individuals. Journal of Orthopaedic & Sports Physical Therapy. 2005; 35(4):227–38. [DOI:10.2519/jospt.2005.35.4.227]
- Bak K, Faunø P. Clinical findings in competitive swimmers with shoulder pain. The American Journal of Sports Medicine. 1997; 25(2):254–60. [DOI:10.1177/036354659702500221]
- Burkhart SS, Morgan CD, Kibler WB. The disabled throwing shoulder: Spectrum of pathology Part I: Pathoanatomy and biomechanics. Arthroscopy: The Journal of Arthroscopic & Related Surgery. 2003; 19(4):404–20. [DOI:10.1053/jars.2003.50128]
- Rupp S, Berninger K, Hopf T. Shoulder problems in high level swimmers-impingement, anterior instability, muscular imbalance? International Journal of Sports Medicine. 1995; 16(08):557–62. [DOI:10.1055/s-2007-973054]
- Allander E. Prevalence, incidence, and remission rates of some common rheumatic diseases or syndromes. Scandinavian Journal of Rheumatology. 1974; 3(3):145–53. [DOI:10.3109/03009747409097141]
- Turgut E, Duzgun I, Baltaci G. Effects of scapular stabilization exercise training on scapular kinematics, disability, and pain in subacromial impingement: A randomized controlled trial. Archives of Physical Medicine and Rehabilitation. 2017; 98(10):1915–23. e3. [DOI:10.1016/j.apmr.2017.05.023]
- Buttagat V, Kluayhomthong S, Areeudomwong P. Effects of the combination of traditional Thai massage, scapular stabilization exercise, and chest mobilization in subjects with forward head posture: A single-blinded randomized clinical trial. Chiropractic & Manual Therapies. 2023; 31(1):31. [DOI:10.1186/s12998-023-00506-z]
- Tate AR, McClure P, Kareha S, Irwin D, Barbe MF. A clinical method for identifying scapular dyskinesis, part 2: Validity. Journal of Athletic Training. 2009; 44(2):165-73. [Link]
- Uhl TL, Kibler WB, Gecewich B, Tripp BL. Evaluation of clinical assessment methods for scapular dyskinesis. Arthroscopy. 2009; 25(11):1240–8. [DOI:10.1016/j.arthro.2009.06.007]
- Fanning E, Daniels K, Cools A, Miles JJ, Falvey É. Biomechanical upper-extremity performance tests and isokinetic shoulder strength in collision and contact athletes. Journal of Sports Sciences. 2021; 39(16):1873–81. [DOI:10.1080/02640414.2021.1904694]
- Borms D, Cools A. Upper-extremity functional performance tests: Reference values for overhead athletes. International Journal of Sports Medicine. 2018; 39(06):433–41. [DOI:10.1055/a-0573-1388]
- de Oliveira VM, Pitangui AC, Nascimento VY, da Silva HA, Dos Passos MH, de Araújo RC. Test-retest reliability of the closed kinetic chain upper extremity stability test (CKCUEST) in adolescents: reliability of CKCUEST in adolescents. International Journal of Sports Physical Therapy. 2017; 12(1):125. [PMID]
- Goldbeck TG, Davies GJ. Test-retest reliability of the closed kinetic chain upper extremity stability test: A clinical field test. Journal of Sport Rehabilitation. 2000; 9(1):35–45. [PMID]
- Hollstadt K, Boland M, Mulligan I. Test-retest reliability of the closed kinetic chain upper extremity stability test (CKCUEST) in a modified test position in division I collegiate basketball players. International Journal of Sports Physical Therapy. 2020; 15(2):203. [PMID]
- Tucci HT, Martins J, Sposito GdC, Camarini PMF, De Oliveira AS. Closed kinetic chain upper extremity stability test (CKCUES test): A reliability study in persons with and without shoulder impingement syndrome. BMC Musculoskeletal Disorders. 2014; 15:1–9. [PMID]
- Ellenbecker TS, Davies GJ. Closed kinetic chain exercise: A comprehensive guide to multiple joint exercise. Champaign: Human Kinetics; 2001. [Link]
- Schilling DT, Elazzazi AM. Shoulder strength and closed kinetic chain upper extremity stability test performance in Division III collegiate baseball and softball players. International Journal of Sports Physical Therapy. 2021; 16(3):844. [PMID]
- Kim J, Kim YK. Palpation-based scapular dyskinesis test: Inter-and intra-rater reliability and clinical advantages. Journal of Back and Musculoskeletal Rehabilitation. 2025; 38(3):616–23. [DOI:10.1177/10538127241308969] [PMID]
- Greenfield B, Catlin PA, Coats PW, Green E, McDonald JJ, North C. Posture in patients with shoulder overuse injuries and healthy individuals. Journal of Orthopaedic & Sports Physical Therapy. 1995; 21(5):287–95. [PMID]
- Moura KF, Monteiro RL, Lucareli PR, Fukuda TY. Rehabilitation of subacromial pain syndrome emphasizing scapular dyskinesis in amateur athletes: A case series. International journal of sports physical therapy. 2016; 11(4):552. [PMID]
- T’Jonck L, Lysens R, Grasse G. Measurements of scapular position and rotation: A reliability study. Physiotherapy Research International. 1996; 1(3):148–58. [PMID]
- Buckley JP, Eston R. Ratings of perceived exertion. Sport and exercise physiology testing guidelines: Volume II-exercise and clinical testing. Oxfordshire: Routledge; 2022. [Link]
- Lewis J, Green A, Reichard Z, Wright C. Scapular position: The validity of skin surface palpation. Manual Therapy. 2002; 7(1):26–30. [PMID]
- Ludewig PM, Braman JP. Shoulder impingement: Biomechanical considerations in rehabilitation. Manual Therapy. 2011; 16(1):33–9. [PMID]
- Eyvazi Hazeh Baran A, Ghani Zadeh Hesar N, Mohammad Ali Nasasb Firouzjah E, Roshani S. [Effect of eight weeks of scapular stabilization exercises on shoulder proprioception and performance of archers with scapular dyskinesis (Persian)]. The Scientific Journal of Rehabilitation Medicine. 2020; 9(4):52-61. [DOI:10.22037/jrm.2020.112841.2266]
- Hajihosseini E, Norasteh AA, Daneshmandi H. Comparison of isometric strength and functional stability of shoulder girdle muscles in volleyball women players with and without scapular dyskinesia. Journal of Health Promotion Management. 2019; 8(5):24–32. [Link]
- Pashaei Z, Daneshmandi H, Norasteh A, Fatahi A. Effect of scapular movement impairment on functional stability of shoulder girdle and scapulohumeral rhythm in elite male volleyball players. The Scientific Journal of Rehabilitation Medicine. 2022; 11(1):64–77. [Link]
- Ellenbecker TS, Cools A. Rehabilitation of shoulder impingement syndrome and rotator cuff injuries: An evidence-based review. British Journal of Sports Medicine. 2010; 44(5):319-27. [DOI:10.1136/bjsm.2009.058875]
- Owens BD, Duffey ML, Nelson BJ, DeBerardino TM, Taylor DC, Mountcastle SB. The incidence and characteristics of shoulder instability at the United States Military Academy. The American Journal of Sports Medicine. 2007; 35(7):1168–73. [PMID]
- Eyvazi Hezebaran A, Ghani Zadeh Hesar N, Mohammad Ali Nasab Firouzjah E, Roshani S. Effect of eight weeks scapular stabilization exercises on shoulder pain of archer men with scapular dyskinesis: A clinical trial study. Journal of Gorgan University of Medical Sciences. 2021; 23(3):24–31. [Link]
- Pashaei Z, Daneshmandi H, Hosseini SM. Effect of eight weeks of corrective exercises on scapulohumeral rhythm, iso-metric strength of shoulder girdle muscles and functional stability in volleyball players with scapular downward rotation syndrome. Scientific Journal of Rehabilitation Medicine. 2022; 11(2):126–43. [DOI:10.32598/SJRM.11.14]
Type of Study: Research |
Subject:
General
Received: 2025/04/27 | Accepted: 2025/09/7 | Published: 2026/04/1
Received: 2025/04/27 | Accepted: 2025/09/7 | Published: 2026/04/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
