Thu, Jun 18, 2026
Volume 16, Issue 2 (Spring 2026)
PTJ 2026, 16(2): 181-188 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Norouziyan B, Yadollahzadeh M, Akbarzadeh Baghban A, Shamili A, Nakhostin Ansari N, Shamsoddini A. Pilot Study on the Effect of Respiratory Biofeedback on Anxiety and Fatigue in Patients With COVID-19: Use of Smartphone. PTJ 2026; 16 (2) :181-188
URL: http://ptj.uswr.ac.ir/article-1-760-en.html
URL: http://ptj.uswr.ac.ir/article-1-760-en.html
Bahman Norouziyan1 

 , Mahdi Yadollahzadeh2 , Alireza Akbarzadeh Baghban3 , Aryan Shamili4 , Noureddin Nakhostin Ansari5 , Alireza Shamsoddini *6
, Mahdi Yadollahzadeh2 , Alireza Akbarzadeh Baghban3 , Aryan Shamili4 , Noureddin Nakhostin Ansari5 , Alireza Shamsoddini *6
, Mahdi Yadollahzadeh2 , Alireza Akbarzadeh Baghban3 , Aryan Shamili4 , Noureddin Nakhostin Ansari5 , Alireza Shamsoddini *6
1- Department of Occupational Therapy, School of Rehabilitation, Shahid Beheshti University of Medical Science, Tehran, Iran.
2- Department of Internal Medicine, School of Medicine, Firoozgar General Hospital, Iran University of Medical Sciences, Tehran, Iran.
3- Department of Biostatistics,Proteomics Research Center, School of Allied Medical Sciences, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
4- Department of Occupational Therapy, Faculty of Rehabilitation, Tehran University of Medical Sciences, Tehran, Iran.
5- Sports Medicine Research Center, Tehran University of Medical Sciences, Tehran, Iran.
6- Exercise Physiology Research Center, Life Style Institute, Baqiyatallah University of Medical Sciences, Tehran, Iran.
2- Department of Internal Medicine, School of Medicine, Firoozgar General Hospital, Iran University of Medical Sciences, Tehran, Iran.
3- Department of Biostatistics,Proteomics Research Center, School of Allied Medical Sciences, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
4- Department of Occupational Therapy, Faculty of Rehabilitation, Tehran University of Medical Sciences, Tehran, Iran.
5- Sports Medicine Research Center, Tehran University of Medical Sciences, Tehran, Iran.
6- Exercise Physiology Research Center, Life Style Institute, Baqiyatallah University of Medical Sciences, Tehran, Iran.
Full-Text [PDF 576 kb]
(408 Downloads)
| Abstract (HTML) (1277 Views)
Full-Text: (24 Views)
Introduction
In late 2019, a novel coronavirus named COVID-19 emerged in Wuhan City, China, causing a new form of pneumonia that rapidly spread across the country and eventually worldwide, posing significant threats to global public health. The virus rapidly spread worldwide [1]. Studies indicate that approximately 80% of infected individuals are asymptomatic or experience mild symptoms, 15% develop severe symptoms requiring oxygen therapy, and 5% require mechanical ventilation and ventilatory support. This highly contagious disease not only endangers physical health and can lead to death but also exerts profound psychological impacts, including stress, depression, grief, post-traumatic stress disorder, anxiety, and fatigue due to its pandemic scale, high pathogenicity, transmission rate, and mortality [2].
Additionally, patients isolated in ICUs face challenging conditions, such as severe respiratory problems, strict quarantine measures, the absence of effective drug treatments, and the risk of mortality, all of which may adversely affect mental health [3]. Studies have shown that respiratory diseases, due to their serious physical complications and the resulting reduction in patients’ quality of life, can lead to anxiety and fatigue [4].
Anxiety and fatigue triggered by illness can be highly destructive and may lead to mental disorders. Initially, anxiety and fatigue activate the hypothalamus, which stimulates increased cortisol secretion from the adrenal cortex and activates the sympathetic nervous system. This acute stress response helps the body cope with short-term stressors. However, if this heightened state of fear, stress, and physiological activation—characterized by prolonged elevated cortisol levels and sympathetic stimulation—persists long-term, it can weaken the immune system and diminish the body’s ability to fight infections, such as COVID-19. Studies have demonstrated that higher anxiety and cortisol levels correlate with worse COVID-19 outcomes, suggesting that chronic stress compromises immune resilience and disease recovery [5]. Over the last decade, mobile technology—particularly smartphones—has offered diverse platforms for assessment and treatment support within the healthcare system [6, 7]. Methods for combating anxiety can be divided into two main categories: pharmacological treatments and psychological/behavioral therapies [8]. Biofeedback is a behavioral therapy technique used to manage anxiety [9].
Biofeedback is a mind-body therapy that teaches individuals to consciously regulate physiological functions by recognizing and modifying specific mental activities and physical responses. Through real-time feedback from sensors, people learn to control autonomic nervous system imbalances—such as sympathetic activation—and thereby reduce stress responses and enhance their healing process. This method enables patients to enhance selfregulation of stressrelated physiological reactions, thereby supporting faster recovery [10].
Respiratory biofeedback is one of the crucial biofeedback techniques. The respiratory system is unique in that it can be controlled both voluntary and involuntary. Many researchers suggest that certain physiological processes in respiratory disorders are linked to the coordination between respiratory rhythm and heartrate variability. Such coordination enhances vagal tone and stimulates baroreflex mechanisms, which regulate sympathetic and parasympathetic activity, thereby promoting autonomic balance [5].
However, several hospitalrelated factors—including a shortage of rehabilitation specialists, high stress among therapists, heat and discomfort associated with prolonged use of protective equipment, reduced staff performance, and heavy patient load—limit the team’s ability to fully address patients’ respiratory rehabilitation needs [11].
Studies have shown that following the outbreak of the severe acute respiratory syndrome (SARS) virus in 2003-2004, and in an effort to reduce direct contact between medical staff and patients, virtual health services—including remote medical consultations and technologyassisted treatment approaches such as mobilebased interventions—were introduced. As a result, smartphones became increasingly common in the medical sector [12]. In smartphonebased respiratory biofeedback, breathing patterns are presented to patients through applications or short instructional videos to guide them in performing structured breathing exercises. Diaphragmatic breathing is a key component of this approach [1]. Therefore, this study aimed to evaluate the effects of smartphonebased respiratory biofeedback on anxiety and fatigue in patients with COVID19 while reducing the need for direct therapist–patient interaction.
Materials and Methods
Experimental study design
A non-randomized clinical trial enrolled 67 patients with COVID-19 from Firouzgar Hospital’s intensive care unit (ICU) (Tehran Province, Iran). Patients were assigned to intervention and control groups based on inclusion criteria. The inclusion criteria included polymerase chain reaction (PCR)-confirmed SARS-CoV-2 infection, hemodynamic stability, Glasgow Coma Scale score >12, oxygen saturation (SpO2)≥85% on room air, absence of major comorbidities, and written informed consent for study participation. The exclusion criteria included hemodynamic instability, SpO2<85% despite oxygen therapy, cognitive impairment, visual impairment, and non-compliance with study protocol.
The vital signs of all patients, including heart rate, SpO2, and respiratory rate, were continuously monitored using medical devices throughout hospitalization. Before the intervention, all patients received instruction on the study procedures and were taught proper diaphragmatic breathing techniques. Each patient was asked to lie on their back, place their right hand on their chest, and their left hand on their abdomen. They were then instructed to breathe so that only the abdomen rises and falls during inhalation and exhalation, while keeping the right hand (on the chest) as still as possible to minimize chest movement. This technique allowed patients to feel the movement of the abdomen with their left hand, ensuring correct diaphragmatic breathing.
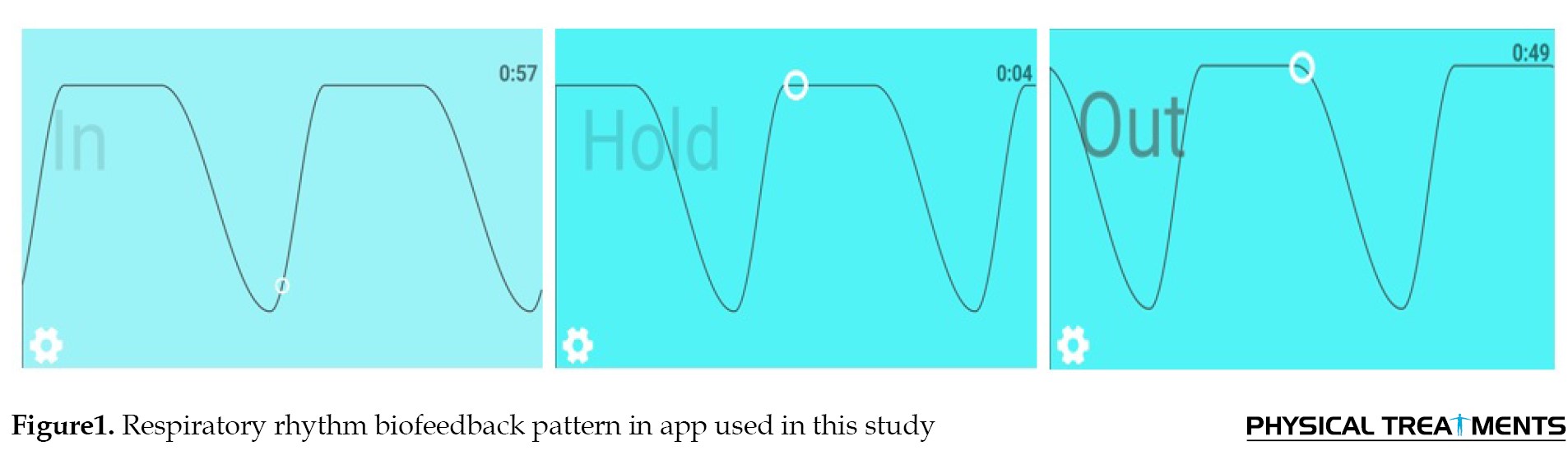
This diaphragmatic breathing exercise was practiced at the beginning of each session to ensure that patients could follow the biofeedback pattern accurately. After teaching the diaphragmatic breathing correctly, a visual diagram of the respiratory pattern was displayed to the patient by the Breathe application, which is installed on the therapist’s tablet. The Breathe app is a mobile application designed to support mindfulness and relaxation through guided breathing exercises. It helps users “watch their breath” by providing animations that signal inhales and exhales, allowing customization of breath length to promote intentional, calming breathing. This app aims to reduce anxiety, stress, and depression while enhancing cognitive functions, such as focus, memory, and decision-making [13]. In this software, the respiratory pattern is shown in the form of a three-part diagram, the ascending part of which represents inhalation, the smooth part of which represents holding the breath, and the descending part of which represents the exhalation. In this app, the respiratory pattern is shown in the form of a scheduled three-part diagram: 1) the ascending part of which represents the inhalation for 4 seconds (In) 2) the smooth part of which represents the retention of breath for 7 seconds (Hold) 3) the descending part of which represents the exhalation for 8 seconds (Out) (Figure 1).
In late 2019, a novel coronavirus named COVID-19 emerged in Wuhan City, China, causing a new form of pneumonia that rapidly spread across the country and eventually worldwide, posing significant threats to global public health. The virus rapidly spread worldwide [1]. Studies indicate that approximately 80% of infected individuals are asymptomatic or experience mild symptoms, 15% develop severe symptoms requiring oxygen therapy, and 5% require mechanical ventilation and ventilatory support. This highly contagious disease not only endangers physical health and can lead to death but also exerts profound psychological impacts, including stress, depression, grief, post-traumatic stress disorder, anxiety, and fatigue due to its pandemic scale, high pathogenicity, transmission rate, and mortality [2].
Additionally, patients isolated in ICUs face challenging conditions, such as severe respiratory problems, strict quarantine measures, the absence of effective drug treatments, and the risk of mortality, all of which may adversely affect mental health [3]. Studies have shown that respiratory diseases, due to their serious physical complications and the resulting reduction in patients’ quality of life, can lead to anxiety and fatigue [4].
Anxiety and fatigue triggered by illness can be highly destructive and may lead to mental disorders. Initially, anxiety and fatigue activate the hypothalamus, which stimulates increased cortisol secretion from the adrenal cortex and activates the sympathetic nervous system. This acute stress response helps the body cope with short-term stressors. However, if this heightened state of fear, stress, and physiological activation—characterized by prolonged elevated cortisol levels and sympathetic stimulation—persists long-term, it can weaken the immune system and diminish the body’s ability to fight infections, such as COVID-19. Studies have demonstrated that higher anxiety and cortisol levels correlate with worse COVID-19 outcomes, suggesting that chronic stress compromises immune resilience and disease recovery [5]. Over the last decade, mobile technology—particularly smartphones—has offered diverse platforms for assessment and treatment support within the healthcare system [6, 7]. Methods for combating anxiety can be divided into two main categories: pharmacological treatments and psychological/behavioral therapies [8]. Biofeedback is a behavioral therapy technique used to manage anxiety [9].
Biofeedback is a mind-body therapy that teaches individuals to consciously regulate physiological functions by recognizing and modifying specific mental activities and physical responses. Through real-time feedback from sensors, people learn to control autonomic nervous system imbalances—such as sympathetic activation—and thereby reduce stress responses and enhance their healing process. This method enables patients to enhance selfregulation of stressrelated physiological reactions, thereby supporting faster recovery [10].
Respiratory biofeedback is one of the crucial biofeedback techniques. The respiratory system is unique in that it can be controlled both voluntary and involuntary. Many researchers suggest that certain physiological processes in respiratory disorders are linked to the coordination between respiratory rhythm and heartrate variability. Such coordination enhances vagal tone and stimulates baroreflex mechanisms, which regulate sympathetic and parasympathetic activity, thereby promoting autonomic balance [5].
However, several hospitalrelated factors—including a shortage of rehabilitation specialists, high stress among therapists, heat and discomfort associated with prolonged use of protective equipment, reduced staff performance, and heavy patient load—limit the team’s ability to fully address patients’ respiratory rehabilitation needs [11].
Studies have shown that following the outbreak of the severe acute respiratory syndrome (SARS) virus in 2003-2004, and in an effort to reduce direct contact between medical staff and patients, virtual health services—including remote medical consultations and technologyassisted treatment approaches such as mobilebased interventions—were introduced. As a result, smartphones became increasingly common in the medical sector [12]. In smartphonebased respiratory biofeedback, breathing patterns are presented to patients through applications or short instructional videos to guide them in performing structured breathing exercises. Diaphragmatic breathing is a key component of this approach [1]. Therefore, this study aimed to evaluate the effects of smartphonebased respiratory biofeedback on anxiety and fatigue in patients with COVID19 while reducing the need for direct therapist–patient interaction.
Materials and Methods
Experimental study design
A non-randomized clinical trial enrolled 67 patients with COVID-19 from Firouzgar Hospital’s intensive care unit (ICU) (Tehran Province, Iran). Patients were assigned to intervention and control groups based on inclusion criteria. The inclusion criteria included polymerase chain reaction (PCR)-confirmed SARS-CoV-2 infection, hemodynamic stability, Glasgow Coma Scale score >12, oxygen saturation (SpO2)≥85% on room air, absence of major comorbidities, and written informed consent for study participation. The exclusion criteria included hemodynamic instability, SpO2<85% despite oxygen therapy, cognitive impairment, visual impairment, and non-compliance with study protocol.
The vital signs of all patients, including heart rate, SpO2, and respiratory rate, were continuously monitored using medical devices throughout hospitalization. Before the intervention, all patients received instruction on the study procedures and were taught proper diaphragmatic breathing techniques. Each patient was asked to lie on their back, place their right hand on their chest, and their left hand on their abdomen. They were then instructed to breathe so that only the abdomen rises and falls during inhalation and exhalation, while keeping the right hand (on the chest) as still as possible to minimize chest movement. This technique allowed patients to feel the movement of the abdomen with their left hand, ensuring correct diaphragmatic breathing.
This diaphragmatic breathing exercise was practiced at the beginning of each session to ensure that patients could follow the biofeedback pattern accurately. After teaching the diaphragmatic breathing correctly, a visual diagram of the respiratory pattern was displayed to the patient by the Breathe application, which is installed on the therapist’s tablet. The Breathe app is a mobile application designed to support mindfulness and relaxation through guided breathing exercises. It helps users “watch their breath” by providing animations that signal inhales and exhales, allowing customization of breath length to promote intentional, calming breathing. This app aims to reduce anxiety, stress, and depression while enhancing cognitive functions, such as focus, memory, and decision-making [13]. In this software, the respiratory pattern is shown in the form of a three-part diagram, the ascending part of which represents inhalation, the smooth part of which represents holding the breath, and the descending part of which represents the exhalation. In this app, the respiratory pattern is shown in the form of a scheduled three-part diagram: 1) the ascending part of which represents the inhalation for 4 seconds (In) 2) the smooth part of which represents the retention of breath for 7 seconds (Hold) 3) the descending part of which represents the exhalation for 8 seconds (Out) (Figure 1).
An attempt was made to match the patient’s diaphragmatic breathing pattern with the biofeedback pattern provided by the software. In the intervention group, the therapist guided the patient to synchronize their breathing rhythm with the visual breathing pattern displayed on the patient’s tablet. In addition to routine treatment, all patients in the intervention group followed a biofeedback-based breathing exercise protocol for five days, with two sessions per day lasting 30 minutes each. Every 5 minutes of breathing practice was followed by a 2-minute rest period. Additionally, non-verbal instrumental music integrated into the software was used to help calm patients and reduce their anxiety levels in the intervention group.
Patients in the control group received only standard medical care. Fatigue levels in both groups were assessed before and after the intervention using the multidimensional fatigue inventory. Additionally, anxiety levels were evaluated using the Spielberger questionnaire. To minimize assessment bias, the initial evaluation was conducted by one assessor, while the secondary assessment was performed independently by another assessor blinded to the initial results. This approach aimed to enhance objectivity, although complete blinding was not feasible.
Statistical analysis
Descriptive statistics methods, such as tables, graphs, and concentration and dispersion indices, were used to describe the results. The one-sample K-S test was used to examine the normality of the data distribution. If the data distribution was normal, parametric statistical methods, such as independent t-test, were used to compare between groups, paired t-test was used to compare within groups, repeated measures analysis of variance was used to examine the effect of time and intervention on the dependent variable, and analysis of variance was used to control for possible confounding variables.
Results
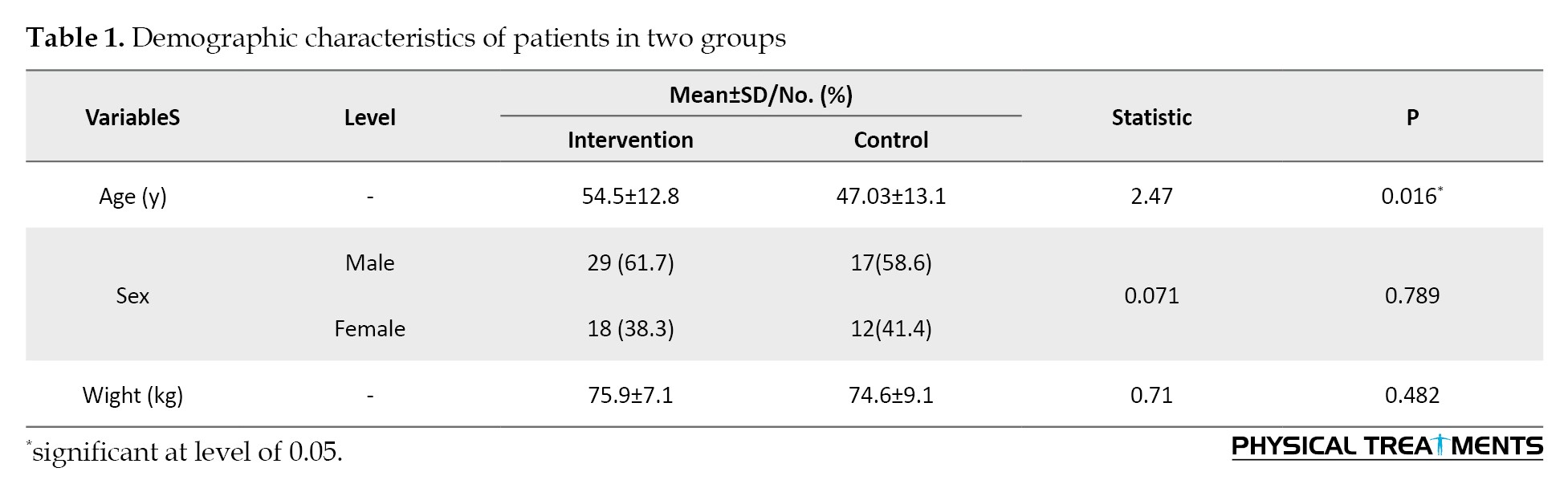
Seventy-six patients, including 47 men and 29 women, were allocated to the intervention and control groups. Table 1 presents the demographic characteristics of patients in both groups.
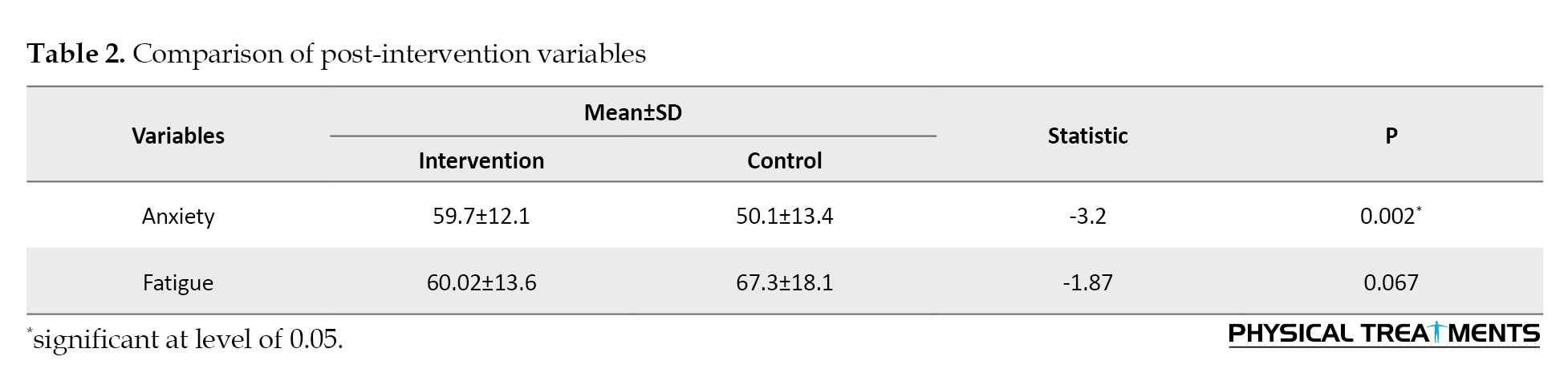
Compared to the control group, patients in the intervention group experienced a significant reduction in fatigue and anxiety following respiratory biofeedback therapy (P<0.05) (Table 2).
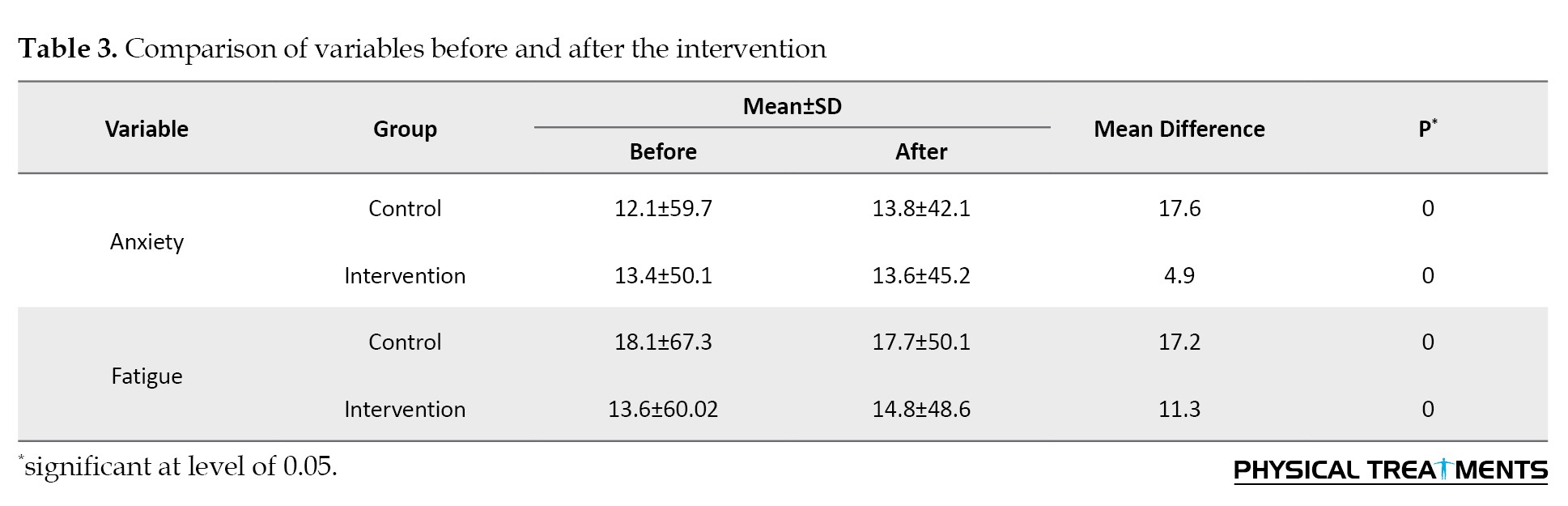
Although routine treatment also led to symptom improvement in the control group, both fatigue and anxiety levels improved significantly in both groups after the intervention (P<0.05), with a greater reduction observed in the intervention group (Table 3).
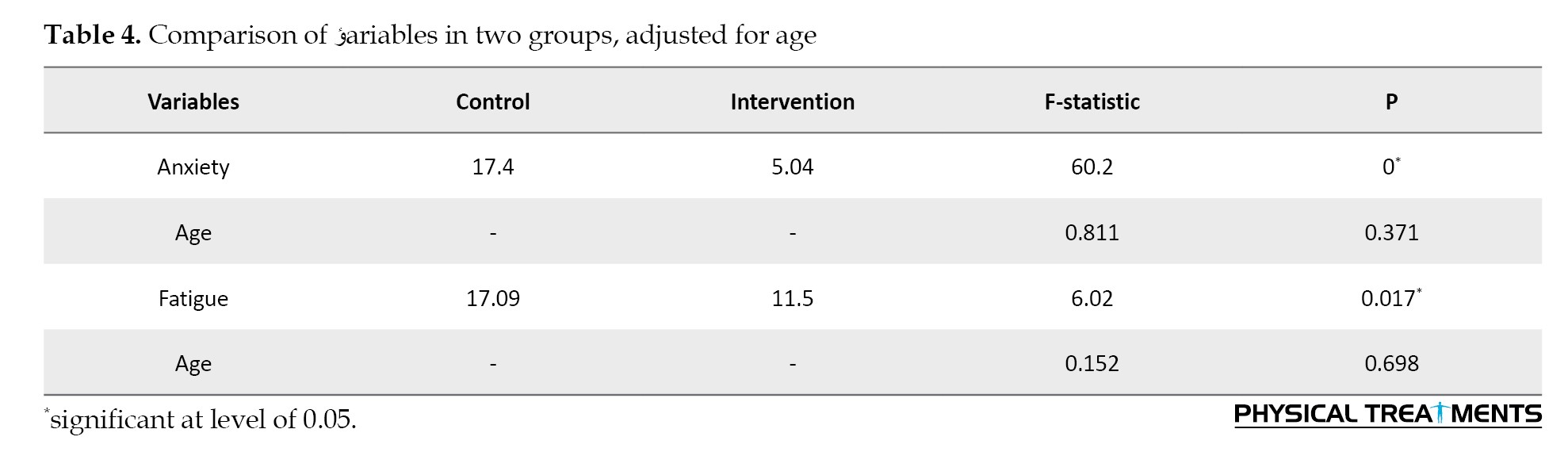
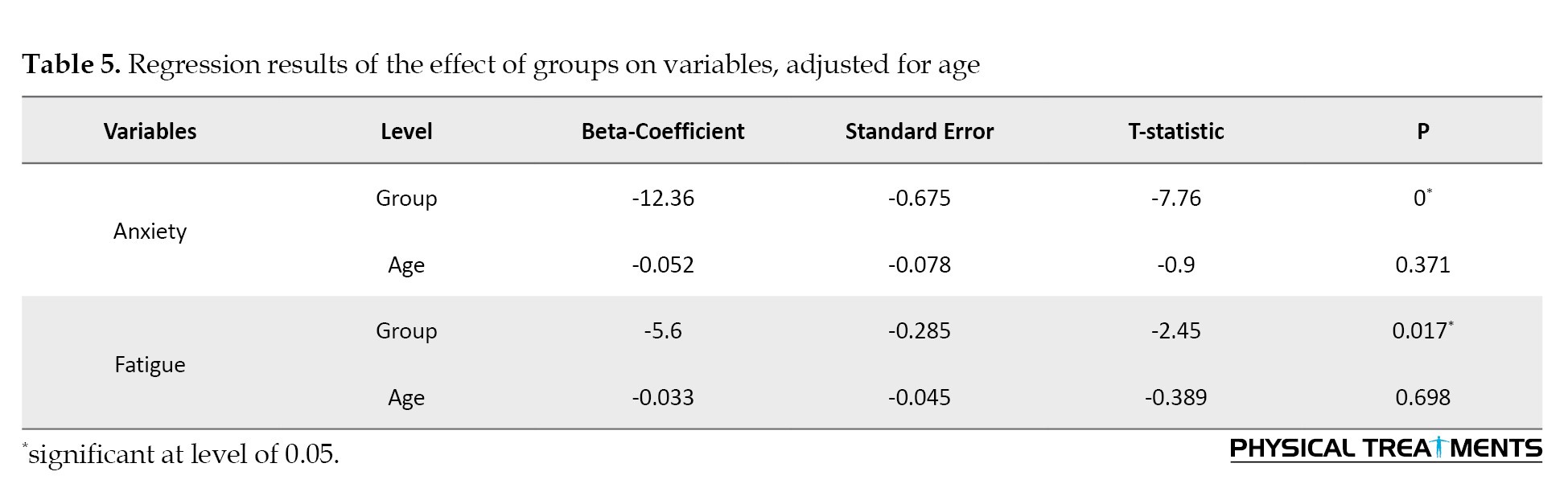
Furthermore, multivariate analysis of covariance (Table 4) and regression analysis (Table 5), adjusted for patient age, confirmed that respiratory biofeedback significantly improved fatigue and anxiety in the intervention group compared to the control group.
Discussion
Respiratory problems in patients with COVID-19 and their struggle for better breathing lead to anxiety and fatigue, which are therefore common symptoms associated with the disease. The results of the present study showed that biofeedback, using a researcher-made device, reduced the symptoms of anxiety and fatigue in people with COVID-19 [5]. The present findings demonstrate that respiratory biofeedback improves anxiety and fatigue in patients with COVID-19. Although the control group also showed symptom improvement, the degree of improvement in the intervention group was greater and statistically significant. Research indicates that respiratory biofeedback promotes self-organized improvement in psychological harm [14, 15].
At the psychological level, it uses cognitive and behavioral strategies to reduce stress, promote relaxation, and enhance self-efficacy, thereby improving fatigue and lowering anxiety levels [16]. In addition to its psychological effects, another reason for using biofeedback is to minimize therapist contact with COVID-19 patients. Therefore, this study aimed to apply an indirect biofeedback technique via patients’ smartphones to investigate its impact on reducing anxiety and fatigue while minimizing therapist-patient interaction.
In a study, Liu evaluated respiratory rehabilitation in patients with COVID-19. The results showed that six weeks of respiratory rehabilitation improved respiratory function, quality of life, and anxiety in patients, but had no significant effect on depression [17]. Based on the results of previous research, following the outbreak of the SARS virus in 2003-2004, virtual health services—such as medical consultations and the use of smartphones in treatment—became popular to reduce contact between medical staff and patients.
Peter and Lim showed that the self-care tools used by medical staff acted not only as physical barriers but also as psychological barriers to human communication during treatment. Additionally, the contagious nature of the virus negatively impacted all rehabilitation activities for these patients. Therefore, based on the study’s findings, it is important to consider rehabilitation approaches that align with infection control principles and support the health of medical staff [18]. Furthermore, the results of Simpson’s study indicated that innovative care approaches, such as virtual rehabilitation, are likely to become more prevalent in this context [18].
Consistent with the present study, Robert Reiner et al. investigated the effect of using a biofeedback device in clinical interventions for patients with anxiety disorders. Their results indicate that many physical and mental disorders stem from an imbalance between physiological systems. Specifically, increased sympathetic arousal and decreased parasympathetic activity—which normally promotes relaxation—lead to bodily disharmony. By promoting oscillation of heart rate and respiration, biofeedback helps restore autonomic balance between the sympathetic and parasympathetic nervous systems. The biofeedback system indirectly influences these systems by coordinating respiratory rhythm, thereby facilitating autonomic regulation and subsequently reducing anxiety and fatigue [19].
In the study by Kai Liu, muscle relaxation techniques reduced anxiety levels, improved sleep quality, and minimized patients’ reliance on anxiolytic and hypnotic medications. Based on this research, rehabilitation interventions were effective in controlling secondary symptoms [20]. Liu also indicated that progressive muscle relaxation improved sleep quality and reduced anxiety in patients with COVID-19. Therefore, it was recommended that patients receive progressive muscle relaxation training [20]. Building upon the effectiveness of biofeedback devices in reducing anxiety symptoms, it is evident that biofeedback assists individuals in behavioral modification by providing feedback on their physiological responses [21]. Biofeedback can enhance a person’s awareness of visceral events [22]. These perceptions enable individuals to achieve deeper self-regulation of these processes. In psychophysiology, respiration is primarily measured as a dependent variable that reflects an individual’s state [23].
Respiration is the only vital function that can be consciously controlled and modified. An individual can voluntarily adjust their breathing pattern to alter their state of physical tension. The parasympathetic nervous system functions in contrast to the sympathetic nervous system, which is responsible for the fight-or-flight response. The parasympathetic system promotes optimal respiration by regulating gas exchange and maintaining blood pH, thereby mitigating symptoms of rapid, abnormal breathing (hyperventilation), such as palpitations [24].
Symptoms, such as irregular heartbeat, precordial pain (chest, cardiac, and lower thoracic regions), epigastric discomfort, bloating, xerostomia (dry mouth/throat), diaphoresis (sweating), general malaise, dyspnea (shortness of breath), a sensation of suffocation, and impaired concentration, may occur. The decrease in anxiety can be attributed to a reduction in sympathetic activity or an increase in parasympathetic activity [25].
Our study has four primary limitations. First, the small sample size limits the generalizability of our findings. Due to the COVID-19 pandemic, recruiting a larger cohort was not feasible. Second, owing to pandemic-related constraints, the study was designed as a non-randomized clinical trial. Third, patient cooperation was limited, largely driven by fear of virus transmission in a clinical setting. Finally, because random assignment was not practicable under these circumstances, we conducted a quasi-experimental, non-randomized study.
Conclusion
The results indicate that a smartphone-based respiratory biofeedback intervention significantly improved anxiety and fatigue in patients with COVID-19. Given these positive findings, this approach is recommended as a therapeutic strategy to alleviate these symptoms, which may, in turn, facilitate earlier hospital discharge during the inpatient phase.
Ethical Considerations
Compliance with ethical guidelines
The study was approved by the Ethics Committee of Baqiyatallah University of Medical Sciences, Tehran, Iran (Code: IR.BMSU.REC.1399.483). All participants were informed of the study objectives, and written informed consent was obtained from those who agreed to participate.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors contributed to the preparation of this manuscript.
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgments
The authors thank the patients who participated in this study.
Patients in the control group received only standard medical care. Fatigue levels in both groups were assessed before and after the intervention using the multidimensional fatigue inventory. Additionally, anxiety levels were evaluated using the Spielberger questionnaire. To minimize assessment bias, the initial evaluation was conducted by one assessor, while the secondary assessment was performed independently by another assessor blinded to the initial results. This approach aimed to enhance objectivity, although complete blinding was not feasible.
Statistical analysis
Descriptive statistics methods, such as tables, graphs, and concentration and dispersion indices, were used to describe the results. The one-sample K-S test was used to examine the normality of the data distribution. If the data distribution was normal, parametric statistical methods, such as independent t-test, were used to compare between groups, paired t-test was used to compare within groups, repeated measures analysis of variance was used to examine the effect of time and intervention on the dependent variable, and analysis of variance was used to control for possible confounding variables.
Results
Seventy-six patients, including 47 men and 29 women, were allocated to the intervention and control groups. Table 1 presents the demographic characteristics of patients in both groups.
Compared to the control group, patients in the intervention group experienced a significant reduction in fatigue and anxiety following respiratory biofeedback therapy (P<0.05) (Table 2).
Although routine treatment also led to symptom improvement in the control group, both fatigue and anxiety levels improved significantly in both groups after the intervention (P<0.05), with a greater reduction observed in the intervention group (Table 3).
Furthermore, multivariate analysis of covariance (Table 4) and regression analysis (Table 5), adjusted for patient age, confirmed that respiratory biofeedback significantly improved fatigue and anxiety in the intervention group compared to the control group.
Discussion
Respiratory problems in patients with COVID-19 and their struggle for better breathing lead to anxiety and fatigue, which are therefore common symptoms associated with the disease. The results of the present study showed that biofeedback, using a researcher-made device, reduced the symptoms of anxiety and fatigue in people with COVID-19 [5]. The present findings demonstrate that respiratory biofeedback improves anxiety and fatigue in patients with COVID-19. Although the control group also showed symptom improvement, the degree of improvement in the intervention group was greater and statistically significant. Research indicates that respiratory biofeedback promotes self-organized improvement in psychological harm [14, 15].
At the psychological level, it uses cognitive and behavioral strategies to reduce stress, promote relaxation, and enhance self-efficacy, thereby improving fatigue and lowering anxiety levels [16]. In addition to its psychological effects, another reason for using biofeedback is to minimize therapist contact with COVID-19 patients. Therefore, this study aimed to apply an indirect biofeedback technique via patients’ smartphones to investigate its impact on reducing anxiety and fatigue while minimizing therapist-patient interaction.
In a study, Liu evaluated respiratory rehabilitation in patients with COVID-19. The results showed that six weeks of respiratory rehabilitation improved respiratory function, quality of life, and anxiety in patients, but had no significant effect on depression [17]. Based on the results of previous research, following the outbreak of the SARS virus in 2003-2004, virtual health services—such as medical consultations and the use of smartphones in treatment—became popular to reduce contact between medical staff and patients.
Peter and Lim showed that the self-care tools used by medical staff acted not only as physical barriers but also as psychological barriers to human communication during treatment. Additionally, the contagious nature of the virus negatively impacted all rehabilitation activities for these patients. Therefore, based on the study’s findings, it is important to consider rehabilitation approaches that align with infection control principles and support the health of medical staff [18]. Furthermore, the results of Simpson’s study indicated that innovative care approaches, such as virtual rehabilitation, are likely to become more prevalent in this context [18].
Consistent with the present study, Robert Reiner et al. investigated the effect of using a biofeedback device in clinical interventions for patients with anxiety disorders. Their results indicate that many physical and mental disorders stem from an imbalance between physiological systems. Specifically, increased sympathetic arousal and decreased parasympathetic activity—which normally promotes relaxation—lead to bodily disharmony. By promoting oscillation of heart rate and respiration, biofeedback helps restore autonomic balance between the sympathetic and parasympathetic nervous systems. The biofeedback system indirectly influences these systems by coordinating respiratory rhythm, thereby facilitating autonomic regulation and subsequently reducing anxiety and fatigue [19].
In the study by Kai Liu, muscle relaxation techniques reduced anxiety levels, improved sleep quality, and minimized patients’ reliance on anxiolytic and hypnotic medications. Based on this research, rehabilitation interventions were effective in controlling secondary symptoms [20]. Liu also indicated that progressive muscle relaxation improved sleep quality and reduced anxiety in patients with COVID-19. Therefore, it was recommended that patients receive progressive muscle relaxation training [20]. Building upon the effectiveness of biofeedback devices in reducing anxiety symptoms, it is evident that biofeedback assists individuals in behavioral modification by providing feedback on their physiological responses [21]. Biofeedback can enhance a person’s awareness of visceral events [22]. These perceptions enable individuals to achieve deeper self-regulation of these processes. In psychophysiology, respiration is primarily measured as a dependent variable that reflects an individual’s state [23].
Respiration is the only vital function that can be consciously controlled and modified. An individual can voluntarily adjust their breathing pattern to alter their state of physical tension. The parasympathetic nervous system functions in contrast to the sympathetic nervous system, which is responsible for the fight-or-flight response. The parasympathetic system promotes optimal respiration by regulating gas exchange and maintaining blood pH, thereby mitigating symptoms of rapid, abnormal breathing (hyperventilation), such as palpitations [24].
Symptoms, such as irregular heartbeat, precordial pain (chest, cardiac, and lower thoracic regions), epigastric discomfort, bloating, xerostomia (dry mouth/throat), diaphoresis (sweating), general malaise, dyspnea (shortness of breath), a sensation of suffocation, and impaired concentration, may occur. The decrease in anxiety can be attributed to a reduction in sympathetic activity or an increase in parasympathetic activity [25].
Our study has four primary limitations. First, the small sample size limits the generalizability of our findings. Due to the COVID-19 pandemic, recruiting a larger cohort was not feasible. Second, owing to pandemic-related constraints, the study was designed as a non-randomized clinical trial. Third, patient cooperation was limited, largely driven by fear of virus transmission in a clinical setting. Finally, because random assignment was not practicable under these circumstances, we conducted a quasi-experimental, non-randomized study.
Conclusion
The results indicate that a smartphone-based respiratory biofeedback intervention significantly improved anxiety and fatigue in patients with COVID-19. Given these positive findings, this approach is recommended as a therapeutic strategy to alleviate these symptoms, which may, in turn, facilitate earlier hospital discharge during the inpatient phase.
Ethical Considerations
Compliance with ethical guidelines
The study was approved by the Ethics Committee of Baqiyatallah University of Medical Sciences, Tehran, Iran (Code: IR.BMSU.REC.1399.483). All participants were informed of the study objectives, and written informed consent was obtained from those who agreed to participate.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors contributed to the preparation of this manuscript.
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgments
The authors thank the patients who participated in this study.
Reference
- Velavan TP, Meyer. The COVID‐19 epidemic. 2020; 25(3):278. [DOI:10.1111/tmi.13383] [PMID]
- Arden MA, Chilcot JJBjohp. Health psychology and the coronavirus (COVID‐19) global pandemic: A call for research. British Journal of Health Psychology. 2020; 25(2):231. [PMID]
- Pfefferbaum B, North CSJNEjom. Mental health and the Covid-19 pandemic. The New England Journal of Medicine. 2020; 383(6):510-2. [DOI:10.1056/NEJMp2008017] [PMID]
- Usher K, Durkin J, Bhullar NJ. The COVID‐19 pandemic and mental health impacts. International Journal of Mental Health Nursing. Journal of Medical Internet Research. 2020; 29(3):315. [DOI:10.1111/inm.12726] [PMID]
- Alneyadi M, Drissi N, Almeqbaali M, Ouhbi SJJm, uHealth. Biofeedback-based connected mental health interventions for anxiety: Systematic literature review. JMIR Mhealth Uhealth. 2021; 9(4):e26038. [DOI:10.2196/26038] [PMID]
- Martínez-Pérez B, De La Torre-Díez I, López-Coronado MJJomIr. Mobile health applications for the most prevalent conditions by the World Health Organization: Review and analysis. 2013; 15(6):e120. [DOI:10.2196/jmir.2600] [PMID]
- Pourahmadi M, Momeni E, Mohseni N, Hesarikia H, Ghanjal A, Shamsoddini AJPT, et al. The reliability and concurrent validity of a new iPhone® application for measuring active lumbar spine flexion and extension range of motion in patients with low back pain. An International Journal of Physical Therapy. 2021; 37(1):204-17. [DOI:10.1080/09593985.2019.1616017]
- Gerogianni G, Babatsikou F, Polikandrioti M, Grapsa EJ. Management of anxiety and depression in haemodialysis patients: The role of non-pharmacological methods. International Urology and Nephrology. 2019; 51(1):113-8. [DOI:10.1007/s11255-018-2022-7]
- Goessl VC, Curtiss JE, Hofmann SG. The effect of heart rate variability biofeedback training on stress and anxiety: A meta-analysis. Psychological Medicine. 2017; 47(15):2578-86. [DOI:10.1017/S0033291717001003]
- Tolin DF, Davies CD, Moskow DM, Hofmann SG. Biofeedback and neurofeedback for anxiety disorders: A quantitative and qualitative systematic review. In: Yong-Ku K, editor. Anxiety disorders: Rethinking and understanding recent discoveries. Berlin: Springer; 2020. [DOI:10.1007/978-981-32-9705-0_16]
- Medica EM. First impact on services and their preparation.“Instant paper from the field” on rehabilitation answers to the Covid-19 emergency. European Journal of Physical and Rehabilitation Medicine. 2020; 1-8. [DOI:10.23736/S1973-9087.20.06303-0]
- Zhao H, Liu F, Xie W, Zhou TC, OuYang J, Jin L, et al. Ultrasensitive supersandwich-type electrochemical sensor for SARS-CoV-2 from the infected COVID-19 patients using a smartphone. Sensors and Actuators B: Chemical. 2021; 327:128899. [DOI:10.1016/j.snb.2020.128899]
- Chittaro L, Sioni R. Evaluating mobile apps for breathing training: the effectiveness of visualization. Computers in Human Behavior. 2014; 40:56-63. [DOI:10.1016/j.chb.2014.07.049]
- Hillsman D, inventor. Respiratory biofeedback and performance evaluation system. Alexandria: United States patent US; 1976. [Link]
- Schwerdtfeger AR, Schwarz G, Pfurtscheller K, Thayer JF, Jarczok MN, Pfurtscheller G. Heart rate variability (HRV): From brain death to resonance breathing at 6 breaths per minute. Clinical Neurophysiology. 2020; 131(3):676-93. [DOI:10.1016/j.clinph.2019.11.013]
- Henriques G, Keffer S, Abrahamson C, Jeanne Horst S. Exploring the effectiveness of a computer-based heart rate variability biofeedback program in reducing anxiety in college students. Applied Psychophysiology and Biofeedback. 2011; 36(2):101-12. [DOI:10.1007/s10484-011-9151-4]
- Liu K, Zhang W, Yang Y, Zhang J, Li Y, Chen Y. Respiratory rehabilitation in elderly patients with COVID-19: A randomized controlled study. Complementary Therapies in Clinical Practice. 2020; 39:101166. [DOI:10.1016/j.ctcp.2020.101166]
- Lim PA, Ng YS, Tay BK. Impact of a viral respiratory epidemic on the practice of medicine and rehabilitation: Severe acute respiratory syndrome. Archives of Physical Medicine and Rehabilitation. 2004; 85(8):1365-70. [DOI:10.1016/j.apmr.2004.01.022]
- Reiner R. Integrating a portable biofeedback device into clinical practice for patients with anxiety disorders: Results of a pilot study. Applied Psychophysiology and Biofeedback. 2008; 33(1):55-61. [DOI:10.1007/s10484-007-9046-6]
- Liu K, Chen Y, Wu D, Lin R, Wang Z, Pan L. Effects of progressive muscle relaxation on anxiety and sleep quality in patients with COVID-19. Complementary Therapies in Clinical Practice. 2020; 39:101132. [DOI:10.1016/j.ctcp.2020.101132]
- Rosenberg A, Hamiel D. Reducing test anxiety and related symptoms using a biofeedback respiratory practice device: A randomized control trial. Applied Psychophysiology and Biofeedback. 2021; 46(1):69-82. [DOI:10.1007/s10484-020-09494-9]
- Cho Y, Kim H, Seong S, Park K, Choi J, Kim MJ, et al. Effect of virtual reality-based biofeedback for depressive and anxiety symptoms: Randomized controlled study. Journal of Affective Disorders. 2024; 361:392-8. [DOI:10.1016/j.jad.2024.06.031]
- Aranberri-Ruiz A, Aritzeta A, Olarza A, Soroa G, Mindeguia R. Reducing anxiety and social stress in primary education: A breath-focused heart rate variability biofeedback intervention. International Journal of Environmental Research and Public Health. 2022; 19(16):10181. [Link]
- Alves DG, Rocha SG, Andrade EV, Mendes AZ, Cunha ÂG. The positive impact of physical activity on the reduction of anxiety scores: A pilot study. Revista da Associação Médica Brasileira. 2019; 65:434-40. [Link]
- Tomasi J, Zai CC, Zai G, Herbert D, Richter MA, Mohiuddin AG, et al Investigating the association of anxiety disorders with heart rate variability measured using a wearable device. Journal of Affective Disorders. 2024; 351:569-78. [DOI:10.1016/j.jad.2024.01.137]
Type of Study: Research |
Subject:
General
Received: 2025/04/8 | Accepted: 2025/08/26 | Published: 2026/04/1
Received: 2025/04/8 | Accepted: 2025/08/26 | Published: 2026/04/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
