Wed, Jul 15, 2026
Volume 16, Issue 1 (Winter 2026)
PTJ 2026, 16(1): 73-82 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Ebrahimi E, Tabatabaee S M, Dadarkhah A, Najafi S. NASM-based Core Stability Training Using Taekwondo Movements in Male Individuals With Hyperlordosis. PTJ 2026; 16 (1) :73-82
URL: http://ptj.uswr.ac.ir/article-1-733-en.html
URL: http://ptj.uswr.ac.ir/article-1-733-en.html



1- Clinical Biomechanics and Ergonomics Research Center, Aja University of Medical Sciences, Tehran, Iran.
Full-Text [PDF 1113 kb]
(948 Downloads)
| Abstract (HTML) (1772 Views)
Full-Text: (1677 Views)
Introduction
ordosis refers to the natural anterior curvature found in the cervical and lumbar regions of the human spine [1]. Excessive inward curvature of the lumbar spine is known as lumbar hyperlordosis [2]. It is estimated that the prevalence ranges from approximately 10% to 30%, depending on age, activity level, and contributing biomechanical factors [3]. Lumbar hyperlordosis occurs due to imbalances in the muscles and soft tissues of the core regions, including the pelvis, abdomen, and spine, caused by a combination of weakness and tightness [4]. The kinesiopathology model suggests that functional alterations in one part of the movement system can gradually contribute to musculoskeletal disorders [5]. In individuals with lumbar hyperlordosis, muscle imbalances in the lumbopelvic region often result in an anterior pelvic tilt, an exaggerated lumbar curve, and reduced core stability [6]. Therefore, stabilizing the core of the lumbar spine is considered essential for ensuring proper lower extremity movement [7], as it enhances spinal stability and helps prevent injuries in the lumbopelvic region [8].
In this context, a study examining the effectiveness of an 8-week intervention in non-athletic men with hyperlordosis found that corrective exercises improved performance, demonstrating a significant positive impact on this condition [9]. In another study conducted by Rahmani et al. it was revealed that the core stability-based corrective program not only improved the curvature of lumbar hyperlordosis but also enhanced functional movement patterns [10].
Taekwondo (TKD), a martial art emphasizing precise movements, balance, and control, notably affects postural alignment [11]. Its dynamic and static techniques incorporate core stabilization, flexibility, and strength, collectively contributing to improved posture [12]. TKD movements consist of a series of effective actions designed for specific activities in both sports and therapeutic contexts [13], where the correct and timely execution of movements holds significant importance [14]. In this regard, a study demonstrated that a training program incorporating basic TKD movements is an effective tool for correcting body posture, including pelvic inclination [15]. The national academy of sports medicine (NASM) asserts that incorporating exercises aligned with its approach— which emphasizes self-myofascial release and integration— can enhance training effectiveness [16]. Various studies have shown that corrective exercises following the NASM approach improve postural abnormalities in both the upper and lower extremities [17-19].
Despite the increasing interest in core stability training to address postural abnormalities, such as hyperlordosis, there is still a lack of studies integrating sport-specific movements, like TKD, into these programs. Recent research primarily focuses on traditional exercise interventions, neglecting the potential benefits of martial arts’ dynamic, functional movements that simultaneously promote core activation, flexibility, and neuromuscular control. Furthermore, although the NASM approach is well-recognized for its systematic and evidence-based methods in corrective exercise, its application alongside TKD movements remains unexplored. Additionally, most studies on hyperlordosis have concentrated on mixed-gender samples or female participants, creating a gap in understanding how targeted interventions may specifically influence postural alignment and functional outcomes in men. Thus, this study aimed to investigate NASM-based core stability training using TKD movements in male individuals with hyperlordosis.
Materials and Methods
The present study was quasi-experimental with a pre-posttest design. The study population comprised soldiers from the AJA University of Medical Sciences in Tehran. They were selected using convenience sampling and divided into the TKD (n=16) and non-TKD (n=15) groups. According to a previous study [20], considering a significance level of 0.05, a statistical power of 0.80, and an effect size of 0.78, the sample size calculated using G*Power software, version 3.1 included 15 participants in each group.
The inclusion criteria were as follows: male participants aged 18-25 years with lumbar lordosis greater than 51 degrees [21], and without physical disorders, mental illnesses, a history of surgery, or the use of specific medications. The exclusion criteria included any medical condition limiting physical activity, inability to complete the test, current lower limb pain during the test, and any lower limb injury within the past six months that necessitated changes to the individual’s training regimen or a break from sports participation for a minimum of one week.
Initially, for ethical considerations based on the Declaration of Helsinki, all stages of the study were explained to the subjects, and written informed consent was obtained. The subjects were instructed on how to perform each test. It is worth mentioning that all tests were conducted at the 501 Army Hospital under the supervision of the researcher, who is an official coach of the TKD Federation.
Procedure
In the first step, the demographic information of the participants was recorded. Subsequently, the lumbar lordosis angle was measured using a spinal mouse (SM) device, pain levels were assessed through the visual analogue scale (VAS), and abdominal muscle endurance was evaluated via a sit-up test. The data collected at this stage were recorded as pre-test results for each individual. The experimental group then participated in an 8-week core stability program based on the NASM approach, incorporating TKD movements. Simultaneously, the control group participated in standard corrective hyperlordosis exercises based on the NASM approach for the same duration as the experimental group [16]. After completing the 8-week program, the lumbar lordosis angle, pain levels, and abdominal muscle endurance were re-assessed, and the results at this stage were recorded as post-test data.
Assessment of hyperlordosis
The SM is a non-invasive, handheld device used to assess spinal curvature, including lumbar lordosis, with high reliability (r=0.94) [22]. Initially, the examiner thoroughly briefed all participants on the procedure and the correct handling of the SM device to prevent errors and inaccurate results. Detailed instructions on how to use the software were also provided. Each participant removed his shirt and stood facing away from the examiner, with his arm hanging naturally at his sides. The software on a portable laptop or computer was prepared for the assessment. Participants were instructed to focus on a fixed point in front of them to maintain a stable posture [23]. To assess spinal curvature, each rater began by identifying and marking the spinous process of C7 (the starting point) and the vertebrae sacral support (S3) as the endpoint on the skin using palpation and a pencil. To find the C7 vertebra, he was asked to bend his head forward while standing, and his most prominent vertebra, which was the C7 vertebra, was found and marked [23]. To find the S3, the examiner first locates the posterior superior iliac spines (PSIS) by palpating the bony prominences at the lower back near the iliac crest. These landmarks are at the level of the S2 vertebra. From the PSIS, the examiner moves their fingers slightly downward and medially along the midline to locate the sacral spinous processes. The S3 spinous process is generally found just below the level of S2, in the midline of the sacrum [23]. The device was moved slowly and steadily, ensuring both wheels remained in contact with the skin throughout the recording process [23]. At the end of the measurement, the examiner stopped the recording by pressing the left button on the device. A confirmation tone indicated that the data had been successfully transferred to the computer. Also, as the SM is rolled along the spine, data points are collected at intervals of 1.3 mm, resulting in a sampling rate of roughly 150 Hz.
Assessment of pain
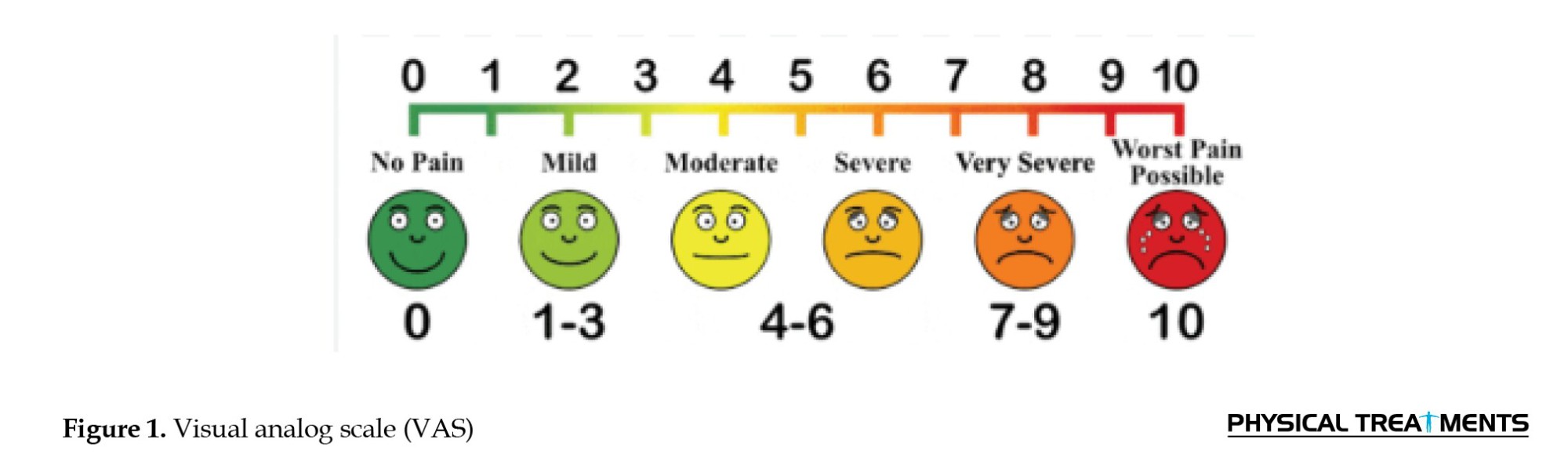
The VAS was employed to assess the pain level in participants during both pre-test and post-test. The VAS is recognized as the most reliable pain-rating system for comparing pain levels across different periods [24], with a high-reliability coefficient of ICC=0.99 [25]. Participants were asked to evaluate their pain level by marking a point on a graded line ranging from 0 (no pain) to 10 (the worst imaginable pain). It is important to note that all participants reported experiencing pain. The value obtained was recorded as the participant’s pain level (Figure 1).
Assessment of abdominal muscle endurance
The one-minute sit-up test was employed to assess participants’ abdominal muscle endurance. Before starting the test, participants completed a 15-minute standardized warm-up to ensure physical and mental preparedness. The procedure and test protocol were thoroughly explained to all participants to ensure familiarity. During the test, participants lay on their backs with knees bent at approximately 90 degrees and feet flat on the ground. Their arms were crossed over their chest throughout the exercise (Figure 2). An assistant secured the participants’ feet to maintain stability. Each participant performed sit-ups by raising their torso until their elbows touched their knees and then returned to the starting position on the floor [26]. This motion was repeated as many times as possible within one minute. The assistant provided time updates and recorded the number of correctly performed sit-ups. To minimize the impact of fatigue, the test was conducted only once.

Training programs of TKD and non-TKD groups
The training program for the TKD group is presented in Table 1. These exercises were performed using TKD movements for 8 weeks, with three weekly sessions lasting 30-45 minutes each, including 5-10 minutes of warm-up and cool-down at the beginning and end of each session.
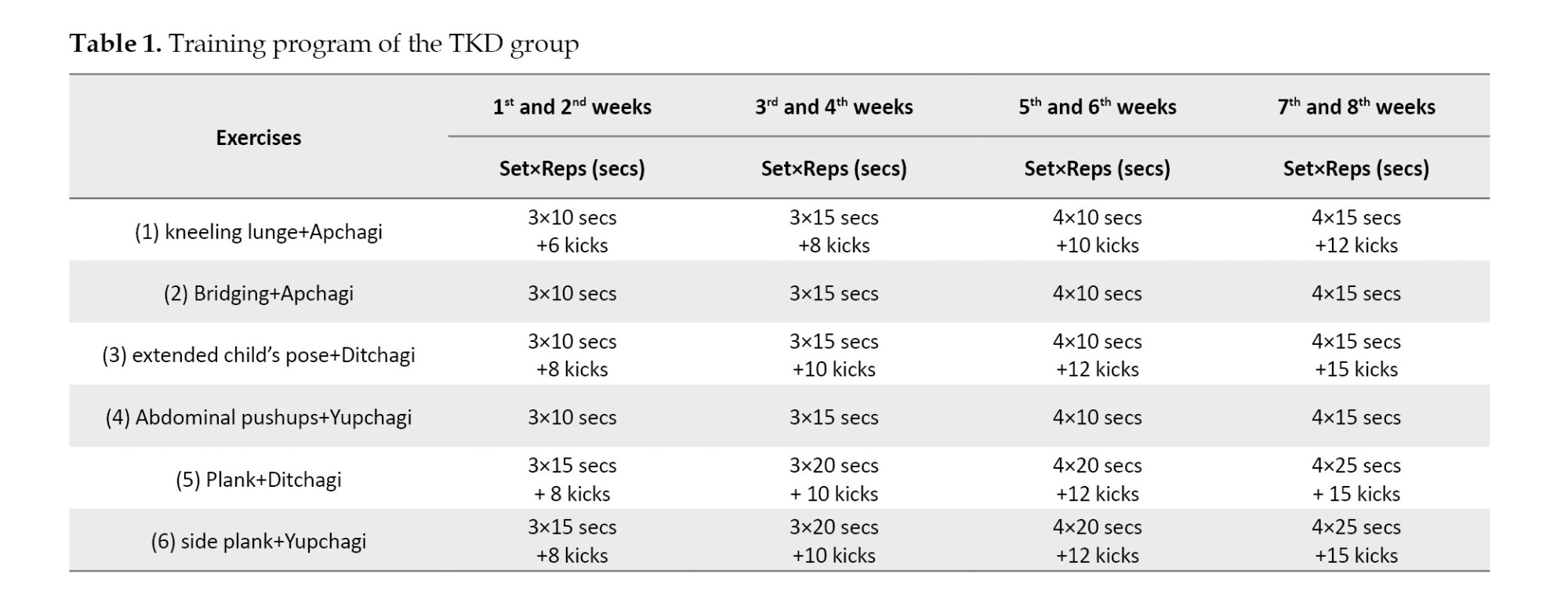
In this program, designed by an official federation coach based on the NASM approach, participants underwent core muscle stability exercises using TKD movements (PALCHAGI [kicks]), specifically targeting the lower limbs (Figure 3). The exercises followed the principles of overload and gradual progression, with increases in repetitions, sets, and duration over time. The exercises were implemented in a circuit format, and intensity was adjusted for each participant based on previous findings and individual tolerance thresholds [27]. The coach initially demonstrated all exercises practically to ensure proper execution. In the training program, some exercises require holding a position for a specified duration, measured in seconds (secs). In contrast, others involve repeating a movement, measured by the number of repetitions (reps).

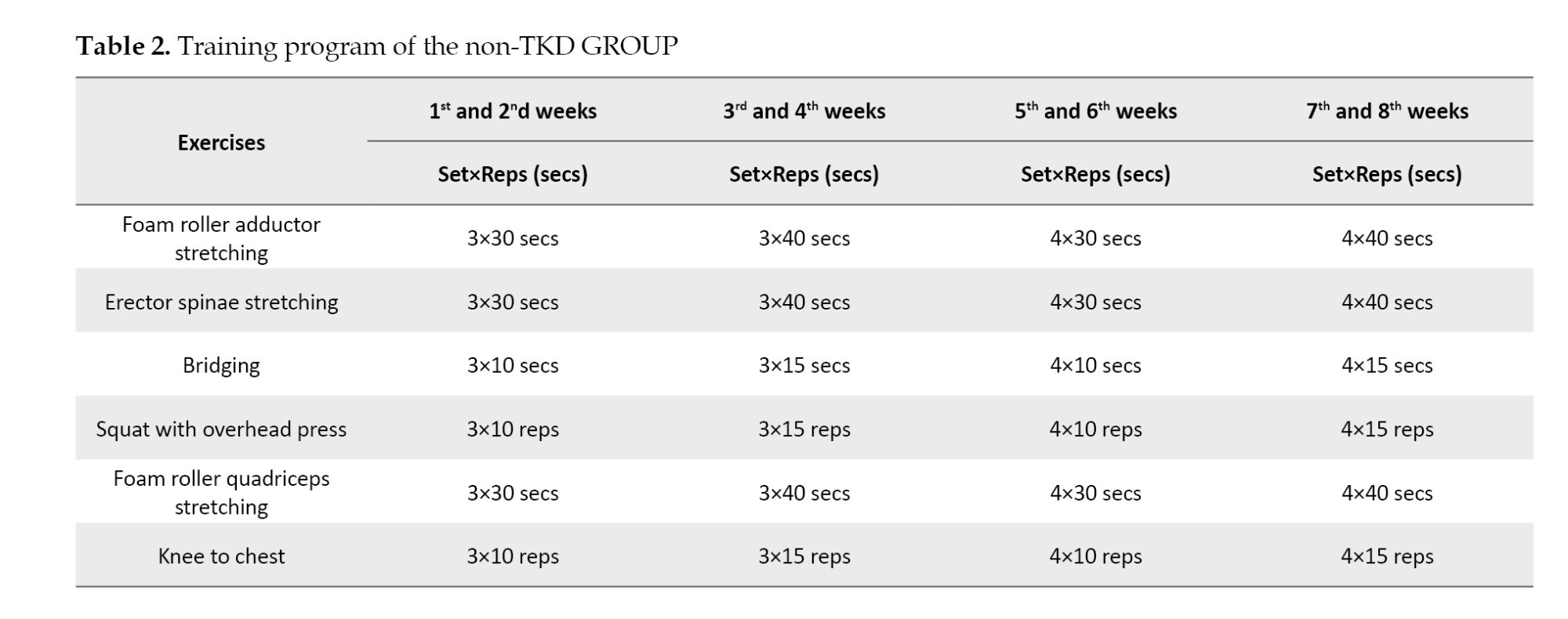
Table 2 presents the training program for the non-TKD group. The program consisted of standard exercises for the hyperlordosis condition based on the NASM approach. Similar to the TKD group, this program was conducted over 8 weeks, with three weekly sessions lasting 30-45 minutes each, including 5-10 minutes of warm-up and cool-down at the beginning and end of each session. The exercises followed the principles of overload and gradual progression, with increases in repetitions, sets, and duration over time.
Data analysis
The Shapiro-Wilk test was utilized to evaluate the normality of the data distribution. Inferential statistics were analyzed using ANCOVA with a significance level of P<0.05. Additionally, paired t-tests were conducted for within-group comparisons. All statistical analyses were performed using SPSS software, version 26.
Results
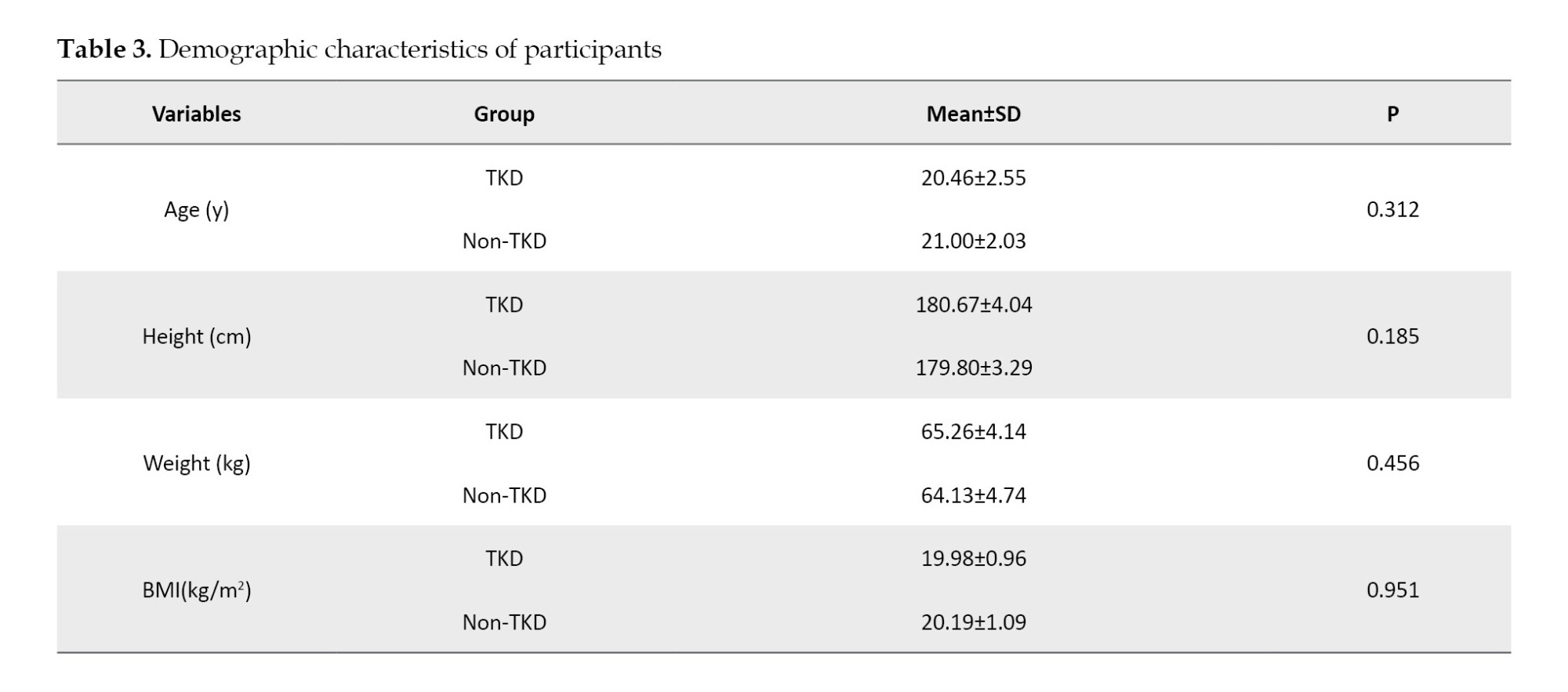
Table 3 displays the demographic characteristics of participants in both groups. There were no significant differences between the study groups in demographic data. The Shapiro-Wilk test results indicated that the data followed a normal distribution.
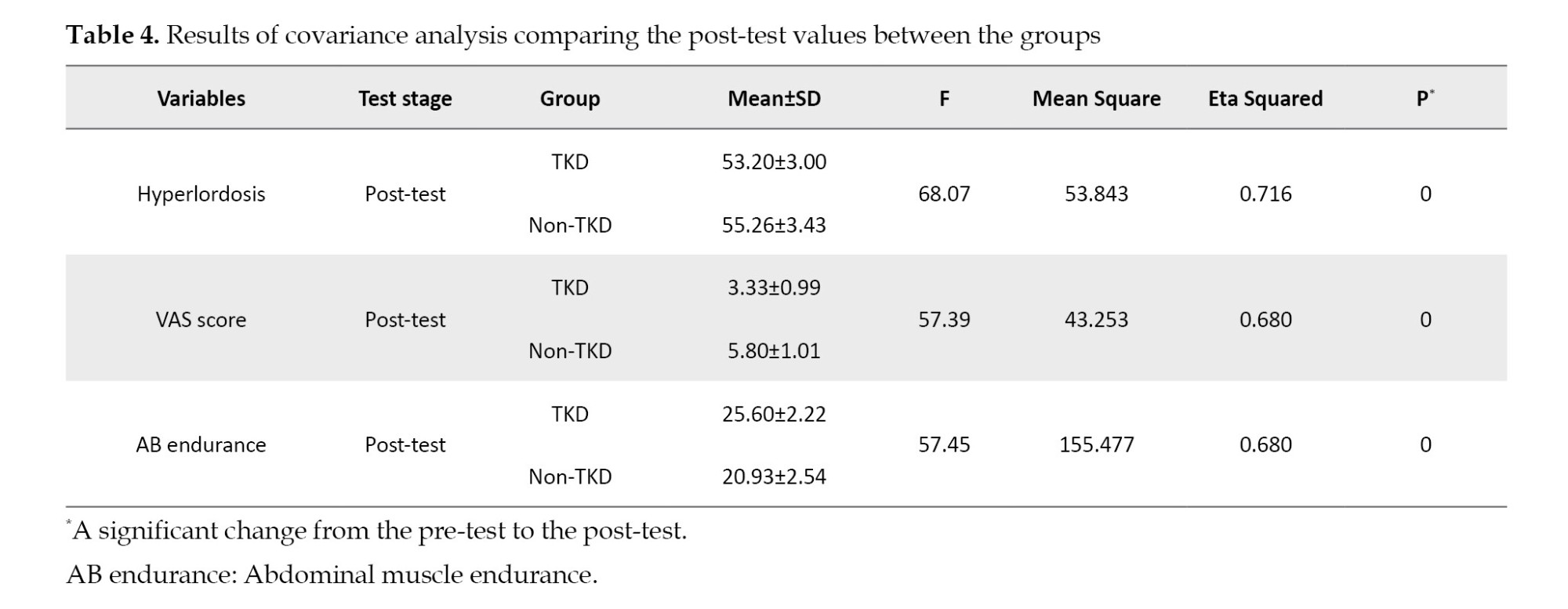
There was a significant difference between the two groups in hyperlordosis degree (P<0.000), VAS score (P<0.000), and abdominal muscle endurance test score (P<0.000), even when the pre-test effect was taken into account (covariate). This shows that incorporating TKD movements with core stability exercises had a significant effect (Table 4).
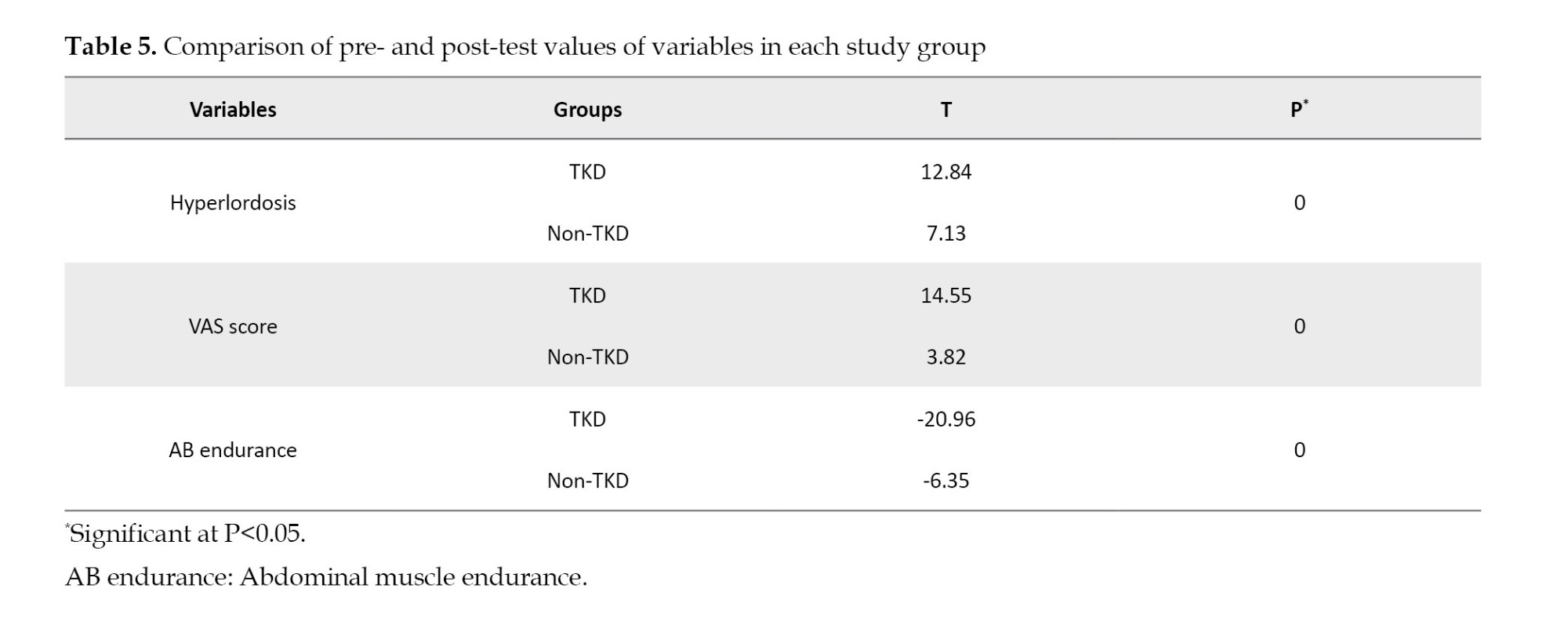
The results of the paired t-test (Table 5) showed that in both TKD and non-TKD groups, the training program significantly affected all variables (P<0.05).
Discussion
The present study found that hyperlordosis, VAS score, and abdominal muscle endurance test score were affected by incorporating TKD into core stability exercises between the two groups. TKD training, when practiced comprehensively, contributes significantly to overall health enhancement by cultivating vital motor skills and physical capabilities. TKD is an effective modality for improving physical fitness and addressing postural and musculoskeletal imbalances, such as lower limb abnormalities and body alignment issues, through its diverse techniques and exercises.
In this regard, Tomenko et al. investigated the effect of recreational TKD training on children’s musculoskeletal systems, and the findings indicated that participants experienced improvements in specific abnormalities, such as foot alignment, which is in line with our results [28]. Similarly, another study demonstrated that integrating core stability exercises into TKD training enhanced the performance of the Wing kick [29]. This aligns with the current findings, highlighting that core stability facilitates effective coordination among muscle groups, reduces unwanted oscillations during movements, and promotes more efficient motor performance [30].
Moreover, another study found that the Apkoobi position had a significant positive effect on correcting pelvic inclination and hyperlordosis angles [15], which is in line with our results. Additionally, another study revealed that TKD training improves leg length, leg inclination, and trunk slope by strengthening the muscles supporting the lower limbs and spine [31].
It can be interpreted that a training regimen incorporating fundamental TKD movements can effectively correct postural deformities. The possible mechanism involves the activation of lower limb movements during TKD, such as Juchumseogi, which elicits eccentric contractions of the gluteus maximus, semimembranosus, semitendinosus, and adductor magnus muscles [32]. Concurrently, this movement triggers concentric contractions in the quadratus lumborum, pectineus, tensor fasciae latae, adductor brevis, adductor longus, adductor magnus, rectus femoris, and sartorius muscles. During the Apkoobi position, front-leg movements primarily activate the semimembranosus and semitendinosus muscles [33]. These findings collectively suggest that TKD movements can strengthen muscles that contribute to correcting abnormal body alignments.
Lower limb muscles are essential for executing explosive movements, jumping, and maintaining proper posture. A study reported a significant increase in the average number of push-ups performed in 30 seconds after 17 weeks of TKD training, indicating improvements in muscular endurance [34]. Similarly, Fong et al. identified TKD as a practical exercise modality for enhancing physical fitness and muscular strength endurance [35]. Furthermore, research indicates that TKD can effectively maintain health and improve physical strength in older adults [36]. These findings are consistent with the present study, underscoring the critical role of proprioception and motor control in TKD. The complex and diverse movements inherent to TKD, which continuously involve new postures and movement patterns, may enhance neuromuscular coordination and muscular activation beyond what is achieved through traditional core exercises [37]. While traditional and TKD-based training methods improve abdominal endurance, the more significant improvements observed in the TKD group suggest that dynamic, full-body exercises may enhance muscular endurance and functional core stability. This approach appears particularly beneficial for individuals with hyperlordosis, as TKD training offers superior outcomes in addressing such conditions [38].
Hyperlordosis is often accompanied by musculoskeletal pain [39]. Previous studies have demonstrated that strengthening core muscles can alleviate pain by improving posture and reducing mechanical stress on the spine [10, 40]. The NASM protocol, which typically emphasizes stabilizing exercises aimed at enhancing postural control and isolating specific core muscles, is beneficial for overall strength [41]. However, it may not fully address the complex dynamic needs of individuals with hyperlordosis. In contrast, a study highlighted that TKD exercises involve dynamic movements that engage the core muscles and the back, hip flexors, and other muscles critical to posture and balance [42]. Additionally, another study suggested that the focus of TKD on motor control and neuromuscular coordination may positively impact pain relief by reinforcing better movement patterns and reducing compensatory actions, often exacerbating discomfort in individuals with postural issues [13]. Finally, the nature of TKD training, which emphasizes flexibility, coordination, and functional movement patterns, may provide a more holistic approach to correcting muscular imbalances associated with hyperlordosis and reducing pain.
This study has several limitations that should be acknowledged. First, the sample size was limited to male participants, which restricts the generalizability of the findings to females or other populations with hyperlordosis, such as older adults or individuals with comorbid conditions. Second, while the NASM-based protocol combined with TKD movements was designed to target core stability and address postural imbalances, variations in participants’ baseline physical fitness, proprioceptive ability, and adherence to the program may have influenced the outcomes. Third, the study primarily focused on short- to medium-term effects, and the long-term sustainability of improvements in posture, pain reduction, and functional mobility remains uncertain. Future research should incorporate objective imaging techniques, such as kinematic analysis or electromyography (EMG), to provide deeper insights into muscular activation patterns and movement efficiency. Lastly, cultural and skill-related factors inherent to TKD may limit its applicability to individuals unfamiliar with martial arts. Exploring alternative movement-based approaches or modifications could help broaden the relevance of the findings. Addressing these limitations in future research will enhance the robustness of interventions to manage hyperlordosis through dynamic and core stability-focused training programs.
Conclusion
TKD, with its dynamic, full-body movements, may prove more effective than isolated core- strengthening exercises in reducing pain, lumbar lordotic angles, and improving abdominal muscle endurance in individuals with hyperlordosis. The enhanced efficacy of TKD in these variables can likely be attributed to its ability to engage multiple muscle groups, improve neuromuscular coordination, and address the complex postural and muscular imbalances associated with hyperlordosis.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Research Ethics Committees of AJA University of Medical Sciences, Tehran, Iran (Code: IR.AJAUMS.REC.1403.225).
Funding
This research was financially supported by AJA Medical Sciences, Tehran, Iran.
Authors' contributions
Study design and data collection: Ebrahim Ebrahimi; Writing: Ebrahim Ebrahimi and Seyed Morteza Tabatabaee; Final approval: All authors.
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgments
The authors would like to thank the grant administrators and program officers at AJA Medical Sciences for their guidance and assistance throughout the grant application and management process.
References
ordosis refers to the natural anterior curvature found in the cervical and lumbar regions of the human spine [1]. Excessive inward curvature of the lumbar spine is known as lumbar hyperlordosis [2]. It is estimated that the prevalence ranges from approximately 10% to 30%, depending on age, activity level, and contributing biomechanical factors [3]. Lumbar hyperlordosis occurs due to imbalances in the muscles and soft tissues of the core regions, including the pelvis, abdomen, and spine, caused by a combination of weakness and tightness [4]. The kinesiopathology model suggests that functional alterations in one part of the movement system can gradually contribute to musculoskeletal disorders [5]. In individuals with lumbar hyperlordosis, muscle imbalances in the lumbopelvic region often result in an anterior pelvic tilt, an exaggerated lumbar curve, and reduced core stability [6]. Therefore, stabilizing the core of the lumbar spine is considered essential for ensuring proper lower extremity movement [7], as it enhances spinal stability and helps prevent injuries in the lumbopelvic region [8].
In this context, a study examining the effectiveness of an 8-week intervention in non-athletic men with hyperlordosis found that corrective exercises improved performance, demonstrating a significant positive impact on this condition [9]. In another study conducted by Rahmani et al. it was revealed that the core stability-based corrective program not only improved the curvature of lumbar hyperlordosis but also enhanced functional movement patterns [10].
Taekwondo (TKD), a martial art emphasizing precise movements, balance, and control, notably affects postural alignment [11]. Its dynamic and static techniques incorporate core stabilization, flexibility, and strength, collectively contributing to improved posture [12]. TKD movements consist of a series of effective actions designed for specific activities in both sports and therapeutic contexts [13], where the correct and timely execution of movements holds significant importance [14]. In this regard, a study demonstrated that a training program incorporating basic TKD movements is an effective tool for correcting body posture, including pelvic inclination [15]. The national academy of sports medicine (NASM) asserts that incorporating exercises aligned with its approach— which emphasizes self-myofascial release and integration— can enhance training effectiveness [16]. Various studies have shown that corrective exercises following the NASM approach improve postural abnormalities in both the upper and lower extremities [17-19].
Despite the increasing interest in core stability training to address postural abnormalities, such as hyperlordosis, there is still a lack of studies integrating sport-specific movements, like TKD, into these programs. Recent research primarily focuses on traditional exercise interventions, neglecting the potential benefits of martial arts’ dynamic, functional movements that simultaneously promote core activation, flexibility, and neuromuscular control. Furthermore, although the NASM approach is well-recognized for its systematic and evidence-based methods in corrective exercise, its application alongside TKD movements remains unexplored. Additionally, most studies on hyperlordosis have concentrated on mixed-gender samples or female participants, creating a gap in understanding how targeted interventions may specifically influence postural alignment and functional outcomes in men. Thus, this study aimed to investigate NASM-based core stability training using TKD movements in male individuals with hyperlordosis.
Materials and Methods
The present study was quasi-experimental with a pre-posttest design. The study population comprised soldiers from the AJA University of Medical Sciences in Tehran. They were selected using convenience sampling and divided into the TKD (n=16) and non-TKD (n=15) groups. According to a previous study [20], considering a significance level of 0.05, a statistical power of 0.80, and an effect size of 0.78, the sample size calculated using G*Power software, version 3.1 included 15 participants in each group.
The inclusion criteria were as follows: male participants aged 18-25 years with lumbar lordosis greater than 51 degrees [21], and without physical disorders, mental illnesses, a history of surgery, or the use of specific medications. The exclusion criteria included any medical condition limiting physical activity, inability to complete the test, current lower limb pain during the test, and any lower limb injury within the past six months that necessitated changes to the individual’s training regimen or a break from sports participation for a minimum of one week.
Initially, for ethical considerations based on the Declaration of Helsinki, all stages of the study were explained to the subjects, and written informed consent was obtained. The subjects were instructed on how to perform each test. It is worth mentioning that all tests were conducted at the 501 Army Hospital under the supervision of the researcher, who is an official coach of the TKD Federation.
Procedure
In the first step, the demographic information of the participants was recorded. Subsequently, the lumbar lordosis angle was measured using a spinal mouse (SM) device, pain levels were assessed through the visual analogue scale (VAS), and abdominal muscle endurance was evaluated via a sit-up test. The data collected at this stage were recorded as pre-test results for each individual. The experimental group then participated in an 8-week core stability program based on the NASM approach, incorporating TKD movements. Simultaneously, the control group participated in standard corrective hyperlordosis exercises based on the NASM approach for the same duration as the experimental group [16]. After completing the 8-week program, the lumbar lordosis angle, pain levels, and abdominal muscle endurance were re-assessed, and the results at this stage were recorded as post-test data.
Assessment of hyperlordosis
The SM is a non-invasive, handheld device used to assess spinal curvature, including lumbar lordosis, with high reliability (r=0.94) [22]. Initially, the examiner thoroughly briefed all participants on the procedure and the correct handling of the SM device to prevent errors and inaccurate results. Detailed instructions on how to use the software were also provided. Each participant removed his shirt and stood facing away from the examiner, with his arm hanging naturally at his sides. The software on a portable laptop or computer was prepared for the assessment. Participants were instructed to focus on a fixed point in front of them to maintain a stable posture [23]. To assess spinal curvature, each rater began by identifying and marking the spinous process of C7 (the starting point) and the vertebrae sacral support (S3) as the endpoint on the skin using palpation and a pencil. To find the C7 vertebra, he was asked to bend his head forward while standing, and his most prominent vertebra, which was the C7 vertebra, was found and marked [23]. To find the S3, the examiner first locates the posterior superior iliac spines (PSIS) by palpating the bony prominences at the lower back near the iliac crest. These landmarks are at the level of the S2 vertebra. From the PSIS, the examiner moves their fingers slightly downward and medially along the midline to locate the sacral spinous processes. The S3 spinous process is generally found just below the level of S2, in the midline of the sacrum [23]. The device was moved slowly and steadily, ensuring both wheels remained in contact with the skin throughout the recording process [23]. At the end of the measurement, the examiner stopped the recording by pressing the left button on the device. A confirmation tone indicated that the data had been successfully transferred to the computer. Also, as the SM is rolled along the spine, data points are collected at intervals of 1.3 mm, resulting in a sampling rate of roughly 150 Hz.
Assessment of pain
The VAS was employed to assess the pain level in participants during both pre-test and post-test. The VAS is recognized as the most reliable pain-rating system for comparing pain levels across different periods [24], with a high-reliability coefficient of ICC=0.99 [25]. Participants were asked to evaluate their pain level by marking a point on a graded line ranging from 0 (no pain) to 10 (the worst imaginable pain). It is important to note that all participants reported experiencing pain. The value obtained was recorded as the participant’s pain level (Figure 1).
Assessment of abdominal muscle endurance
The one-minute sit-up test was employed to assess participants’ abdominal muscle endurance. Before starting the test, participants completed a 15-minute standardized warm-up to ensure physical and mental preparedness. The procedure and test protocol were thoroughly explained to all participants to ensure familiarity. During the test, participants lay on their backs with knees bent at approximately 90 degrees and feet flat on the ground. Their arms were crossed over their chest throughout the exercise (Figure 2). An assistant secured the participants’ feet to maintain stability. Each participant performed sit-ups by raising their torso until their elbows touched their knees and then returned to the starting position on the floor [26]. This motion was repeated as many times as possible within one minute. The assistant provided time updates and recorded the number of correctly performed sit-ups. To minimize the impact of fatigue, the test was conducted only once.
Training programs of TKD and non-TKD groups
The training program for the TKD group is presented in Table 1. These exercises were performed using TKD movements for 8 weeks, with three weekly sessions lasting 30-45 minutes each, including 5-10 minutes of warm-up and cool-down at the beginning and end of each session.
In this program, designed by an official federation coach based on the NASM approach, participants underwent core muscle stability exercises using TKD movements (PALCHAGI [kicks]), specifically targeting the lower limbs (Figure 3). The exercises followed the principles of overload and gradual progression, with increases in repetitions, sets, and duration over time. The exercises were implemented in a circuit format, and intensity was adjusted for each participant based on previous findings and individual tolerance thresholds [27]. The coach initially demonstrated all exercises practically to ensure proper execution. In the training program, some exercises require holding a position for a specified duration, measured in seconds (secs). In contrast, others involve repeating a movement, measured by the number of repetitions (reps).
Table 2 presents the training program for the non-TKD group. The program consisted of standard exercises for the hyperlordosis condition based on the NASM approach. Similar to the TKD group, this program was conducted over 8 weeks, with three weekly sessions lasting 30-45 minutes each, including 5-10 minutes of warm-up and cool-down at the beginning and end of each session. The exercises followed the principles of overload and gradual progression, with increases in repetitions, sets, and duration over time.
Data analysis
The Shapiro-Wilk test was utilized to evaluate the normality of the data distribution. Inferential statistics were analyzed using ANCOVA with a significance level of P<0.05. Additionally, paired t-tests were conducted for within-group comparisons. All statistical analyses were performed using SPSS software, version 26.
Results
Table 3 displays the demographic characteristics of participants in both groups. There were no significant differences between the study groups in demographic data. The Shapiro-Wilk test results indicated that the data followed a normal distribution.
There was a significant difference between the two groups in hyperlordosis degree (P<0.000), VAS score (P<0.000), and abdominal muscle endurance test score (P<0.000), even when the pre-test effect was taken into account (covariate). This shows that incorporating TKD movements with core stability exercises had a significant effect (Table 4).
The results of the paired t-test (Table 5) showed that in both TKD and non-TKD groups, the training program significantly affected all variables (P<0.05).
Discussion
The present study found that hyperlordosis, VAS score, and abdominal muscle endurance test score were affected by incorporating TKD into core stability exercises between the two groups. TKD training, when practiced comprehensively, contributes significantly to overall health enhancement by cultivating vital motor skills and physical capabilities. TKD is an effective modality for improving physical fitness and addressing postural and musculoskeletal imbalances, such as lower limb abnormalities and body alignment issues, through its diverse techniques and exercises.
In this regard, Tomenko et al. investigated the effect of recreational TKD training on children’s musculoskeletal systems, and the findings indicated that participants experienced improvements in specific abnormalities, such as foot alignment, which is in line with our results [28]. Similarly, another study demonstrated that integrating core stability exercises into TKD training enhanced the performance of the Wing kick [29]. This aligns with the current findings, highlighting that core stability facilitates effective coordination among muscle groups, reduces unwanted oscillations during movements, and promotes more efficient motor performance [30].
Moreover, another study found that the Apkoobi position had a significant positive effect on correcting pelvic inclination and hyperlordosis angles [15], which is in line with our results. Additionally, another study revealed that TKD training improves leg length, leg inclination, and trunk slope by strengthening the muscles supporting the lower limbs and spine [31].
It can be interpreted that a training regimen incorporating fundamental TKD movements can effectively correct postural deformities. The possible mechanism involves the activation of lower limb movements during TKD, such as Juchumseogi, which elicits eccentric contractions of the gluteus maximus, semimembranosus, semitendinosus, and adductor magnus muscles [32]. Concurrently, this movement triggers concentric contractions in the quadratus lumborum, pectineus, tensor fasciae latae, adductor brevis, adductor longus, adductor magnus, rectus femoris, and sartorius muscles. During the Apkoobi position, front-leg movements primarily activate the semimembranosus and semitendinosus muscles [33]. These findings collectively suggest that TKD movements can strengthen muscles that contribute to correcting abnormal body alignments.
Lower limb muscles are essential for executing explosive movements, jumping, and maintaining proper posture. A study reported a significant increase in the average number of push-ups performed in 30 seconds after 17 weeks of TKD training, indicating improvements in muscular endurance [34]. Similarly, Fong et al. identified TKD as a practical exercise modality for enhancing physical fitness and muscular strength endurance [35]. Furthermore, research indicates that TKD can effectively maintain health and improve physical strength in older adults [36]. These findings are consistent with the present study, underscoring the critical role of proprioception and motor control in TKD. The complex and diverse movements inherent to TKD, which continuously involve new postures and movement patterns, may enhance neuromuscular coordination and muscular activation beyond what is achieved through traditional core exercises [37]. While traditional and TKD-based training methods improve abdominal endurance, the more significant improvements observed in the TKD group suggest that dynamic, full-body exercises may enhance muscular endurance and functional core stability. This approach appears particularly beneficial for individuals with hyperlordosis, as TKD training offers superior outcomes in addressing such conditions [38].
Hyperlordosis is often accompanied by musculoskeletal pain [39]. Previous studies have demonstrated that strengthening core muscles can alleviate pain by improving posture and reducing mechanical stress on the spine [10, 40]. The NASM protocol, which typically emphasizes stabilizing exercises aimed at enhancing postural control and isolating specific core muscles, is beneficial for overall strength [41]. However, it may not fully address the complex dynamic needs of individuals with hyperlordosis. In contrast, a study highlighted that TKD exercises involve dynamic movements that engage the core muscles and the back, hip flexors, and other muscles critical to posture and balance [42]. Additionally, another study suggested that the focus of TKD on motor control and neuromuscular coordination may positively impact pain relief by reinforcing better movement patterns and reducing compensatory actions, often exacerbating discomfort in individuals with postural issues [13]. Finally, the nature of TKD training, which emphasizes flexibility, coordination, and functional movement patterns, may provide a more holistic approach to correcting muscular imbalances associated with hyperlordosis and reducing pain.
This study has several limitations that should be acknowledged. First, the sample size was limited to male participants, which restricts the generalizability of the findings to females or other populations with hyperlordosis, such as older adults or individuals with comorbid conditions. Second, while the NASM-based protocol combined with TKD movements was designed to target core stability and address postural imbalances, variations in participants’ baseline physical fitness, proprioceptive ability, and adherence to the program may have influenced the outcomes. Third, the study primarily focused on short- to medium-term effects, and the long-term sustainability of improvements in posture, pain reduction, and functional mobility remains uncertain. Future research should incorporate objective imaging techniques, such as kinematic analysis or electromyography (EMG), to provide deeper insights into muscular activation patterns and movement efficiency. Lastly, cultural and skill-related factors inherent to TKD may limit its applicability to individuals unfamiliar with martial arts. Exploring alternative movement-based approaches or modifications could help broaden the relevance of the findings. Addressing these limitations in future research will enhance the robustness of interventions to manage hyperlordosis through dynamic and core stability-focused training programs.
Conclusion
TKD, with its dynamic, full-body movements, may prove more effective than isolated core- strengthening exercises in reducing pain, lumbar lordotic angles, and improving abdominal muscle endurance in individuals with hyperlordosis. The enhanced efficacy of TKD in these variables can likely be attributed to its ability to engage multiple muscle groups, improve neuromuscular coordination, and address the complex postural and muscular imbalances associated with hyperlordosis.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Research Ethics Committees of AJA University of Medical Sciences, Tehran, Iran (Code: IR.AJAUMS.REC.1403.225).
Funding
This research was financially supported by AJA Medical Sciences, Tehran, Iran.
Authors' contributions
Study design and data collection: Ebrahim Ebrahimi; Writing: Ebrahim Ebrahimi and Seyed Morteza Tabatabaee; Final approval: All authors.
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgments
The authors would like to thank the grant administrators and program officers at AJA Medical Sciences for their guidance and assistance throughout the grant application and management process.
References
- Hyun AH, Cho JY, Hyun AH, Cho JY. Effect of 8 weeks un-tact pilates home training on body composition, abdominal obesity, pelvic tilt and strength, back pain in overweight women after childbirth. Exercise Science. 2021; 30(1):61-9. [DOI:10.15857/ksep.2021.30.1.61]
- Pesenti S, Prost S, McCausland AM, Farah K, Tropiano P, Fuentes S, et al. Optimal correction of adult spinal deformities requires restoration of distal lumbar lordosis. Advances in Orthopedics. 2021; 2021:5572181. [DOI:10.1155/2021/5572181] [PMID]
- Sergeenko OM, Savin DM, Diachkov KA. Association of spinal cord abnormalities with vertebral anomalies: An embryological perspective. Child’s Nervous System. 2024; 40(5):1415-25. [DOI:10.1007/s00381-024-06336-5] [PMID]
- Czaprowski D, Stoliński Ł, Tyrakowski M, Kozinoga M, Kotwicki T. Non-structural misalignments of body posture in the sagittal plane. Scoliosis and Spinal Disorders. 2018; 13:1-14. [DOI:10.1186/s13013-018-0151-5] [PMID]
- Sahrmann S, Azevedo DC, Van Dillen L. Diagnosis and treatment of movement system impairment syndromes. Brazilian Journal of Physical Therapy. 2017; 21(6):391-9. [DOI:10.1016/j.bjpt.2017.08.001] [PMID]
- Shalamzari MH, Henteh MA, Shamsoddini A, Ghanjal A. Comparison of the effects of core stability and whole-body electromyostimulation exercises on lumbar lordosis angle and dynamic balance of sedentary people with hyperlordosis: A randomized controlled trial. BMC Sports Science, Medicine and Rehabilitation. 2024; 16(1):91. [DOI:10.1186/s13102-024-00879-5] [PMID]
- Willson JD, Ireland ML, Davis I. Core strength and lower extremity alignment during single leg squats. Medicine and Science in Sports and Exercise. 2006; 38(5):945. [DOI:10.1249/01.mss.0000218140.05074.fa] [PMID]
- Hodges PW, Moseley GL. Pain and motor control of the lumbopelvic region: Effect and possible mechanisms. Journal of Electromyography and Kinesiology. 2003; 13(4):361-70. [DOI:10.1016/S1050-6411(03)00042-7] [PMID]
- Elahi AR, Seidi F, Ardakani MK. Effect of 8 weeks of corrective exercises on the lumbar lordosis angle and lower limb function in Non-Athlete Men with lumbar Hyperlordosis. Journal of Safety Promotion and Injury Prevention. 2022; 9(4):304-14. [Link]
- Rahmani M, Zandi S, Minoonejad H. Core stability based corrective exercise program on improving and functional movement patterns in male adults with lumbar hyper-lordosis. International Journal of Musculoskeletal Pain Prevention. 2022; 7(4):794-802. [DOI:10.22034/ijmpp.7.4.794]
- Fong SS, Fu SN, Ng GY. Taekwondo training speeds up the development of balance and sensory functions in young adolescents. Journal of Science and Medicine in Sport. 2012; 15(1):64-8. [DOI:10.1016/j.jsams.2011.06.001] [PMID]
- Lu W, Lin X. Application and analysis of taekwondo techniques, tactics, and movement trajectories based on multi‐intelligent decision making. Mathematical Problems in Engineering. 2022; 2022(1):8411550. [DOI:10.1155/2022/8411550]
- Kim HG, Jung JH, Bae SU. Effects of the three-direction movement control focus complex pain program and neurodynamic focus complex pain program on pain, mechanosensitivity, and body function in taekwondo athletes with non-specific low back pain: A preliminary study. Healthcare. 2024; 12(4):422. [DOI:10.3390/healthcare12040422] [PMID]
- Ebrahimi E, Rashidi P, Tabatabaei N, Soleymani N. [The effectiveness of six weeks of core stability exercises on q angle and flatfoot in female taekwondo athletes (Persian)]. Journal of Sport Biomechanics. 2024; 10(3):216-28. [DOI:10.61186/JSportBiomech.10.3.216]
- Byun S, An C, Kim M, Han D. The effects of an exercise program consisting of taekwondo basic movements on posture correction. Journal of Physical Therapy Science. 2014; 26(10):1585-8. [DOI:10.1589/jpts.26.1585] [PMID]
- Clark M, Lucett S. NASM essentials of corrective exercise training. Philadelphia: Lippincott Williams & Wilkins; 2010. [Link]
- Samadi A, Hajilou B. The effect of 8 weeks of corrective exercises using the NASM approach on movement disorders, lumbar lordosis, and genu valgum in girls aged 12-15. Journal of Sport Biomechanics. 2024; 10(1):2-16. [DOI:10.61186/JSportBiomech.10.1.2]
- Abdolahzadeh M, Daneshmandi H. The effect of an 8-week NASM corrective exercise program on upper crossed syndrome. Journal of Sport Biomechanics. 2019; 5(3):156-67. [DOI:10.32598/biomechanics.5.3.3]
- Kamali M, Ghasemi B, Moradi MR, Bagherian-Dehkordi S. [Comparing the effect of two kinds of the traditional and the NASM corrcetive exercises training protocols on the correction of hyperlordosis in female students (Persian)]. Journal of Research in Rehabilitation Sciences. 2015; 11(2):155-63. [DOI:10.22122/jrrs.v1i2.2279]
- Javadi Mr, Miri H, Letafatkar A. Effects of six weeks of agility exercises on maximum ground reaction force, knee proprioception, balance, and performance in taekwondo athletes of alborz province league. The Scientific Journal of Rehabilitation Medicine. 2020; 9(1):74-87. [DOI:10.22037/jrm.2019.111339.1927]
- Babagoltabar Samakoush H, Norasteh A. Prevalence of postural abnormalities of spine and shoulder girdle in sanda professionals. Annals of Applied Sport Science. 2017; 5(4):31-8. [DOI:10.29252/aassjournal.5.4.31]
- Ripani M, Di Cesare A, Giombini A, Agnello L, Fagnani F, Pigozzi F. Spinal curvature: Comparison of frontal measurements with the spinal mouse and radiographic assessment. The Journal of Sports Medicine and Physical Fitness. 2008; 48(4):488-94. [PMID]
- Ghorbani L, Ghasemi G. Effects of eight weeks corrective exercises on lumbar lordosis. Journal of Research in Rehabilitation Sciences. 2007; 3(2):59-70. [DOI:10.22122/jrrs.v3i2.88]
- Ghasemi B, Ghasemi M, Aazamian A. Compare the effects of massage therapy and hydrotherapy in the pain and motor function in middle-age men (30-55) with choronic low back pain. Shahrekord: Shahrekord University; 2016. [Link]
- Bijur PE, Silver W, Gallagher EJ. Reliability of the visual analog scale for measurement of acute pain. Academic Emergency Medicine. 2001; 8(12):1153-7. [DOI:10.1111/j.1553-2712.2001.tb01132.x] [PMID]
- Noguchi T, Demura S, Takahashi K. Relationships between sit-ups and abdominal flexion strength tests and the thickness of each abdominal muscle. Advances in Physical Education. 2013; 3(2):84-8. [DOI:10.4236/ape.2013.32014]
- Daneshmandi H, Mogharrabi Manzari M. [The effect of eight weeks comprehensive corrective exercises on upper crossed syndrome (Persian)]. Research in Sport Medicine and Technology. 2014; 12(7):75-86. [Link]
- Tomenko O, Kirichenko L, Skripka I, Kopytina Y, Burla A. Effect of recreational taekwondo training on musculoskeletal system of primary school age children. Journal of Physical Education and Sport. 2017; 17(3):1095-100. [DOI:10.22514/jomh.2024.118]
- Guan L, Li K, Li H, Kim Y, Kim S. Effects of core muscle stability on kicking performance during the aerial phase of taekwondo wing kicks. Journal of Men’s Health. 2024; 20(7):138-48. [DOI:10.7752/JPES.2017.03168]
- Barrio ED, Ramirez-Campillo R, Garcia de Alcaraz Serrano A, RaquelHernandez-Garcia R. Effects of core training on dynamic balance stability: A systematic review and meta-analysis. Journal of Sports Sciences. 2022; 40(16):1815-23. [DOI:10.1080/02640414.2022.2110203] [PMID]
- Lee JS, Shin KO. The effects of Taekwondo training of foot angle application on pelvic stabilization and trunk tilt ability. Exercise Science. 2019; 28(3):240-7. [DOI:10.15857/ksep.2019.28.3.240]
- Myers TW. Anatomy trains posters. London: Churchill Livingstone; 2003. [Link]
- Florence Peterson Kendall. Testing and function with posture and pain. Philadelphia: Lippincott Williams & Wilkins; 2005. [Link]
- Brudnak M, Dundero D, Van Hecke F. Are thehard’martial arts, such as the Korean martial art, taekwon-do, of benefit to senior citizens? Medical Hypotheses. 2002; 59(4):485-91. [DOI:10.1016/S0306-9877(02)00203-7] [PMID]
- Fong SS, Ng GY. Does Taekwondo training improve physical fitness? Physical Therapy in Sport. 2011; 12(2):100-6. [DOI:10.1016/j.ptsp.2010.07.001] [PMID]
- Linhares DG, dos Santos AB, dos Santos LL, Pardo PJM, de Souza Cordeiro L, de Castro JBP, et al. Effects of taekwondo on health in older people: A systematic review. Retos. 2022; 46(2022):36-42. [DOI:10.47197/retos.v46.93336]
- Chiodo S, Tessitore A, Cortis C, Lupo C, Ammendolia A, Iona T, et al. Effects of official taekwondo competitions on all-out performances of elite athletes. The Journal of Strength & Conditioning Research. 2011; 25(2):334-9. [DOI:10.1519/JSC.0b013e3182027288] [PMID]
- Xinyue W. Physical fitness improvements and psychological benefits of taekwondo among student athletes in the university. Social Science and Humanities Journal. 2024; 8(10):5582-609. [DOI:10.18535/sshj.v8i10.1404]
- Chun SW, Lim CY, Kim K, Hwang J, Chung SG. The relationships between low back pain and lumbar lordosis: A systematic review and meta-analysis. The Spine Journal. 2017; 17(8):1180-91. [DOI:10.1016/j.spinee.2017.04.034] [PMID]
- Skundric G, Vukicevic V, Lukic N. Effects of core stability exercises, lumbar lordosis and low-back pain: A systematic review. Journal of Anthropology of Sport and Physical Education. 2021; 5(1):17-23. [DOI:10.26773/jaspe.210104]
- Okhli H, Hojjati H, Akhoundzadeh G. Comparing the effect of the corrective exercises of America’s National academy of sports medicine and Pilates on the correction of lordosis among female high school students in Golestan Province in 2018. International Journal of School Health. 2019; 6(4):1-6. [DOI:10.30476/intjsh.2019.45883]
- Fong SSM, Tsang WWN, Ng GYF. Lower limb joint sense, muscle strength and postural stability in adolescent taekwondo practitioners. International SportMed Journal. 2013; 14(2):44-52. [Link]
Type of Study: Research |
Subject:
Sport injury and corrective exercises
Received: 2025/01/28 | Accepted: 2025/05/24 | Published: 2026/01/1
Received: 2025/01/28 | Accepted: 2025/05/24 | Published: 2026/01/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
