Thu, Jul 30, 2026
Volume 16, Issue 2 (Spring 2026)
PTJ 2026, 16(2): 221-232 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Alarab A, Abu Aker M. Core Stability Exercises With Conventional Therapy versus Conventional Therapy in the Management of Chronic Non-specific Low Back Pain: A Randomized Controlled Trial. PTJ 2026; 16 (2) :221-232
URL: http://ptj.uswr.ac.ir/article-1-728-en.html
URL: http://ptj.uswr.ac.ir/article-1-728-en.html



1- Department of Physiotherapy, Faculty of Postgraduate Studies and Research, Palestine Ahliya University, Bethlehem, Palestine.
Full-Text [PDF 513 kb]
(1993 Downloads)
| Abstract (HTML) (1536 Views)
Full-Text: (115 Views)
Introduction
Low back pain (LBP), the most prevalent global musculoskeletal disorder, is defined as pain from the lower rib to the gluteal area, with or without leg pain, lasting more than one day [1–4]. It is the leading cause of disability worldwide [1, 3], affecting 619 million people in 2020 and projected to rise to 843 million by 2050, rising strongly in Asia and Africa [3]. About 84% of people experience LBP at some point in their lifetime, typically with acute flare-ups [5–7]. LBP is classified based on duration of symptoms into acute (<6 weeks), subacute (6–12 weeks), and chronic (>12 weeks). Chronic represents approximately 10–40% of all LBP diagnoses, and is thus a major cause to long-term disability [8, 9].
LBP is a common musculoskeletal condition affecting a large proportion of the global population [1, 3]. It can be classified as specific, resulting from identifiable causes, or non-specific, where no clear cause is found. Nonspecific LBP accounts for most cases [6, 8]. Non-specific LBP is influenced by various factors, including genetics, psychological and social aspects, as well as structural abnormalities in the bones, ligaments, or muscles of the lower back [10, 11]. Common risk factors include smoking, excess body weight, and poor posture or ergonomics [3]. Chronic non-specific LBP, which persists for more than 12 weeks, is a common reason for medical visits and can significantly impact daily activities and work performance [7, 11]. Recently, core stability exercises (CSE) has become a crucial focus of treatment because weakness in key stabilizing muscles reduces spinal support and increases stress on the lower back [3]. Combining CSE with conventional therapies has demonstrated efficacy in reducing symptoms and improving functional outcomes [12].
A meta-analysis of 23 studies involving 1132 participants evaluated the effectiveness of stabilization exercises in reducing pain and decreasing disability in patients with persistent LBP. The results indicated that extended treatment durations (8-12 weeks) yielded the most significant effects on alleviating pain and enhancing disability. Non-specific low back pain (NSLBP) demonstrated greater responsiveness to treatment compared with specific LBP. CSE was more effective in alleviating pain and had more evidence to support improving impairment. Stabilization exercises show strong therapeutic potential and should be considered a key component of clinical treatment, particularly when delivered in supervised and extended programs [13].
Research on CSE versus conventional therapy for nonspecific LBP has several limitations. These limitations include the absence of direct comparisons within the same patient cohort and an overemphasis on shortterm rather than longterm outcomes. Crucial factors, such as patient diversity, psychosocial influences, and quality-of-life measures beyond pain and disability, are frequently overlooked. Furthermore, inconsistent therapy protocols and unclear mechanisms underlying symptom relief pose challenges to drawing definitive conclusions. These gaps highlight the need for more rigorous and comprehensive research to better understand and clarify the efficacy of treatments for non-specific LBP.
Materials and Methods
A randomized single-blind controlled trial was conducted from April to September 2024 at Celina Care Clinic and Al Shifa’ Specialized Complex in Bethlehem, Palestine. Sixty adult patients with chronic non-specific low back pain (CNLBP) lasting over three months, who consulted an orthopedic physician at Al Shifa’ before March 20, 2024, and required physiotherapy, were recruited. The centers were chosen for their accessibility and ability to recruit CNLBP patients referred for physiotherapy after orthopedic consultations at Al Shifa.
Patients were allocated randomly to two groups by an independent researcher using computer-generated randomization. Allocation concealment was ensured by using sealed, opaque, sequentially numbered envelopes opened only after baseline assessment. The first group received CSE combined with conventional treatment therapy (CTT), while the second group received CTT alone. Due to the nature of the interventions, therapists and participants were not blinded, which may introduce performance bias. However, outcome assessors were blinded to group assignments to minimize detection bias.
The entry criteria for the study were people aged between 18 and 60 years, both men and women, with nonspecific LBP that had been present for more than three months and which had been causing pain on more than half the days. Patients were to show pain in the region between the gluteal fold and lower rib, with a visual analog scale (VAS) of 40 mm or more but below 80 mm as recorded at the New Patient Examination Appointment.
The exclusion criteria listed individuals under 18 or over 60 years old, which contradicts the previously stated upper age limit of 60. Other exclusions included those with mental or neurological disorders, specific spinal conditions (e.g. herniated disc, spinal stenosis), systemic diseases, a history of spinal surgery or recent physical therapy, pregnant women, and individuals with upper limb injuries.
Tools
Visual Analogue Scale (VAS): This is a widely used, reliable, and accurate tool for assessing pain severity. It consists of a 100 mm line, with “0” representing no pain and “100” indicating the most severe pain. Patients mark the point that reflects their pain level [14, 15]. The Arabic version of the VAS, validated by El Meidany et al. (2003), is a valid self-report instrument to assess the pain intensity among Arabic-speaking patients, and has also been shown to be effective for patients with rheumatoid arthritis [16].
Oswestry disability index (ODI): This is a valid self-report 10-item survey that evaluates pain difficulty in numerous activities of daily living, including pain severity, personal care, lifting, and walking. Each item is scored on a 0 (no restriction) to 5 (complete restriction) scale, and the sum is calculated to derive a disability index percentage [17]. Scores range from 0–20% (indicating limited disability) to 81–100% (indicating severe disability or being bedbound). The Arabic ODI, validated in Saudi Arabia, is a reliable tool for measuring functional impairment among LBP patients [18].
Fear-avoidance belief questionnaire (FABQ): This is a validated measure of pain and fear of impairment in activities of daily living, specifically for patients with chronic LBP [19]. There are two subscales: One measuring beliefs related to work activities (7 items) and another measuring beliefs related to physical activity (4 items), with responses quantified on a 7-point Likert scale [20, 21]. High scores reflect more fear avoidance. The Arabic version of the FABQ is demonstrated to be reliable and valid for measuring fear-avoidance beliefs in Arab LBP patients [22].
Data Collection
Eligible patients with CNLBP were screened by a blinded researcher after providing informed consent. A previous sample size calculation had established that 60 participants would provide sufficient power to detect significant changes. Participants were randomly assigned using a computer-generated sequence into two groups: group 1 received CSE and usual treatment, while group 2 received usual treatment alone. The core stability program consisted of supervised classes held three times per week for four weeks, aimed at activating the transversus abdominis, lumbar multifidi, and pelvic floor muscles through a graduated progression. Control treatment consisted of heat packs, Transcutaneous Electrical Nerve Stimulation, and therapeutic massage, divided in 45-minute sessions, three times per week for four weeks each. Outcome measures, i.e. the VAS, ODI, and FABQ, were measured by an independent physiotherapist before and after treatment.
Statistical analysis
Data were analyzed using SPSS software, version 24.0, and G*Power, version 3.1.9.4 was used for the computation of test powers and effect sizes. Standard Excel tools were used for basic operations on the data. A paired sample t-test was performed to assess differences between pre- and post-measurements, and an independent t-test was used to compare the efficacy of the two treatment groups, CSE with CTT and CTT only. Effect sizes were calculated using G*Power software, version 3.1.9.4 to indicate the strength of the observed effects, typically categorized as small, medium, or large. All statistical tests were performed at a significance level of P<0.05.
Results
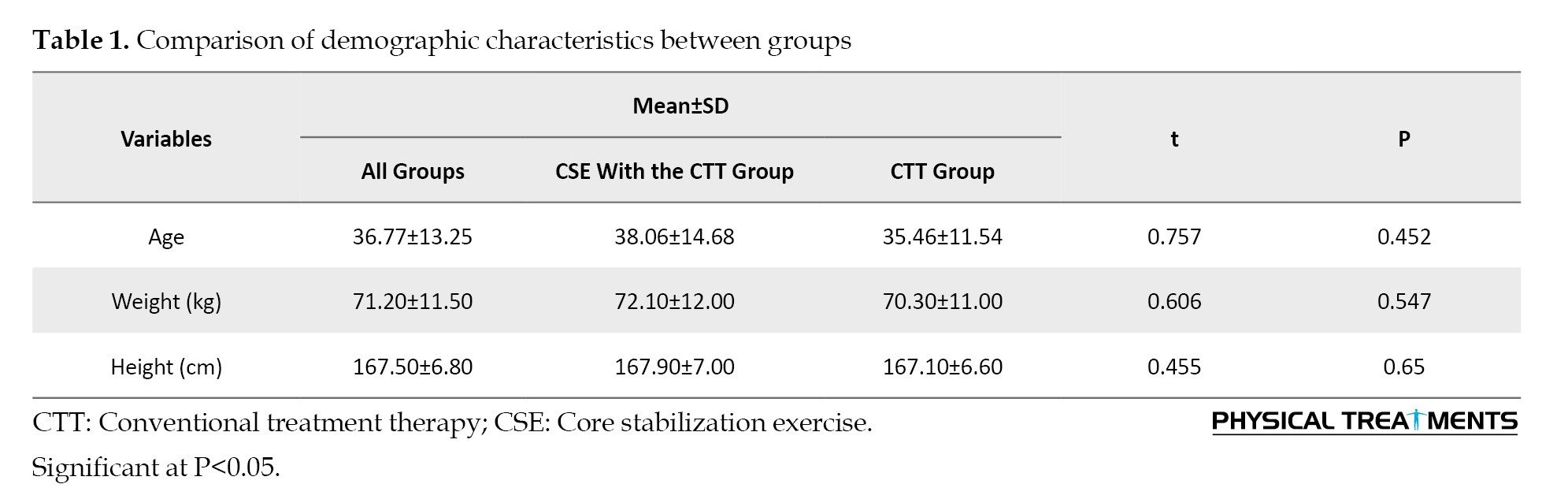
Sixty adult patients with CNLBP were randomized into two groups: 30 received CSE combined with CTT, and 30 received only CTT. The demographic analysis revealed that 46.7% of participants were male and 53.3% were female. The average age of the CSE+CTT group was 38.06 years, while the CTT-only group had an average age of 35.46 years. The baseline demographic comparison showed no statistically significant differences between the CSE+CTT group and the CTT-only group in terms of age, weight, or height (P>0.05 for all variables). Both groups were comparable at the start of the study, indicating that any differences observed in post-intervention outcomes are unlikely to be due to variations in these basic characteristics. Table 1 presents the results.
The results in Table 2 and Figure 1 show that CSE with CTT effectively reduces pain in adults with NSLBP.
Low back pain (LBP), the most prevalent global musculoskeletal disorder, is defined as pain from the lower rib to the gluteal area, with or without leg pain, lasting more than one day [1–4]. It is the leading cause of disability worldwide [1, 3], affecting 619 million people in 2020 and projected to rise to 843 million by 2050, rising strongly in Asia and Africa [3]. About 84% of people experience LBP at some point in their lifetime, typically with acute flare-ups [5–7]. LBP is classified based on duration of symptoms into acute (<6 weeks), subacute (6–12 weeks), and chronic (>12 weeks). Chronic represents approximately 10–40% of all LBP diagnoses, and is thus a major cause to long-term disability [8, 9].
LBP is a common musculoskeletal condition affecting a large proportion of the global population [1, 3]. It can be classified as specific, resulting from identifiable causes, or non-specific, where no clear cause is found. Nonspecific LBP accounts for most cases [6, 8]. Non-specific LBP is influenced by various factors, including genetics, psychological and social aspects, as well as structural abnormalities in the bones, ligaments, or muscles of the lower back [10, 11]. Common risk factors include smoking, excess body weight, and poor posture or ergonomics [3]. Chronic non-specific LBP, which persists for more than 12 weeks, is a common reason for medical visits and can significantly impact daily activities and work performance [7, 11]. Recently, core stability exercises (CSE) has become a crucial focus of treatment because weakness in key stabilizing muscles reduces spinal support and increases stress on the lower back [3]. Combining CSE with conventional therapies has demonstrated efficacy in reducing symptoms and improving functional outcomes [12].
A meta-analysis of 23 studies involving 1132 participants evaluated the effectiveness of stabilization exercises in reducing pain and decreasing disability in patients with persistent LBP. The results indicated that extended treatment durations (8-12 weeks) yielded the most significant effects on alleviating pain and enhancing disability. Non-specific low back pain (NSLBP) demonstrated greater responsiveness to treatment compared with specific LBP. CSE was more effective in alleviating pain and had more evidence to support improving impairment. Stabilization exercises show strong therapeutic potential and should be considered a key component of clinical treatment, particularly when delivered in supervised and extended programs [13].
Research on CSE versus conventional therapy for nonspecific LBP has several limitations. These limitations include the absence of direct comparisons within the same patient cohort and an overemphasis on shortterm rather than longterm outcomes. Crucial factors, such as patient diversity, psychosocial influences, and quality-of-life measures beyond pain and disability, are frequently overlooked. Furthermore, inconsistent therapy protocols and unclear mechanisms underlying symptom relief pose challenges to drawing definitive conclusions. These gaps highlight the need for more rigorous and comprehensive research to better understand and clarify the efficacy of treatments for non-specific LBP.
Materials and Methods
A randomized single-blind controlled trial was conducted from April to September 2024 at Celina Care Clinic and Al Shifa’ Specialized Complex in Bethlehem, Palestine. Sixty adult patients with chronic non-specific low back pain (CNLBP) lasting over three months, who consulted an orthopedic physician at Al Shifa’ before March 20, 2024, and required physiotherapy, were recruited. The centers were chosen for their accessibility and ability to recruit CNLBP patients referred for physiotherapy after orthopedic consultations at Al Shifa.
Patients were allocated randomly to two groups by an independent researcher using computer-generated randomization. Allocation concealment was ensured by using sealed, opaque, sequentially numbered envelopes opened only after baseline assessment. The first group received CSE combined with conventional treatment therapy (CTT), while the second group received CTT alone. Due to the nature of the interventions, therapists and participants were not blinded, which may introduce performance bias. However, outcome assessors were blinded to group assignments to minimize detection bias.
The entry criteria for the study were people aged between 18 and 60 years, both men and women, with nonspecific LBP that had been present for more than three months and which had been causing pain on more than half the days. Patients were to show pain in the region between the gluteal fold and lower rib, with a visual analog scale (VAS) of 40 mm or more but below 80 mm as recorded at the New Patient Examination Appointment.
The exclusion criteria listed individuals under 18 or over 60 years old, which contradicts the previously stated upper age limit of 60. Other exclusions included those with mental or neurological disorders, specific spinal conditions (e.g. herniated disc, spinal stenosis), systemic diseases, a history of spinal surgery or recent physical therapy, pregnant women, and individuals with upper limb injuries.
Tools
Visual Analogue Scale (VAS): This is a widely used, reliable, and accurate tool for assessing pain severity. It consists of a 100 mm line, with “0” representing no pain and “100” indicating the most severe pain. Patients mark the point that reflects their pain level [14, 15]. The Arabic version of the VAS, validated by El Meidany et al. (2003), is a valid self-report instrument to assess the pain intensity among Arabic-speaking patients, and has also been shown to be effective for patients with rheumatoid arthritis [16].
Oswestry disability index (ODI): This is a valid self-report 10-item survey that evaluates pain difficulty in numerous activities of daily living, including pain severity, personal care, lifting, and walking. Each item is scored on a 0 (no restriction) to 5 (complete restriction) scale, and the sum is calculated to derive a disability index percentage [17]. Scores range from 0–20% (indicating limited disability) to 81–100% (indicating severe disability or being bedbound). The Arabic ODI, validated in Saudi Arabia, is a reliable tool for measuring functional impairment among LBP patients [18].
Fear-avoidance belief questionnaire (FABQ): This is a validated measure of pain and fear of impairment in activities of daily living, specifically for patients with chronic LBP [19]. There are two subscales: One measuring beliefs related to work activities (7 items) and another measuring beliefs related to physical activity (4 items), with responses quantified on a 7-point Likert scale [20, 21]. High scores reflect more fear avoidance. The Arabic version of the FABQ is demonstrated to be reliable and valid for measuring fear-avoidance beliefs in Arab LBP patients [22].
Data Collection
Eligible patients with CNLBP were screened by a blinded researcher after providing informed consent. A previous sample size calculation had established that 60 participants would provide sufficient power to detect significant changes. Participants were randomly assigned using a computer-generated sequence into two groups: group 1 received CSE and usual treatment, while group 2 received usual treatment alone. The core stability program consisted of supervised classes held three times per week for four weeks, aimed at activating the transversus abdominis, lumbar multifidi, and pelvic floor muscles through a graduated progression. Control treatment consisted of heat packs, Transcutaneous Electrical Nerve Stimulation, and therapeutic massage, divided in 45-minute sessions, three times per week for four weeks each. Outcome measures, i.e. the VAS, ODI, and FABQ, were measured by an independent physiotherapist before and after treatment.
Statistical analysis
Data were analyzed using SPSS software, version 24.0, and G*Power, version 3.1.9.4 was used for the computation of test powers and effect sizes. Standard Excel tools were used for basic operations on the data. A paired sample t-test was performed to assess differences between pre- and post-measurements, and an independent t-test was used to compare the efficacy of the two treatment groups, CSE with CTT and CTT only. Effect sizes were calculated using G*Power software, version 3.1.9.4 to indicate the strength of the observed effects, typically categorized as small, medium, or large. All statistical tests were performed at a significance level of P<0.05.
Results
Sixty adult patients with CNLBP were randomized into two groups: 30 received CSE combined with CTT, and 30 received only CTT. The demographic analysis revealed that 46.7% of participants were male and 53.3% were female. The average age of the CSE+CTT group was 38.06 years, while the CTT-only group had an average age of 35.46 years. The baseline demographic comparison showed no statistically significant differences between the CSE+CTT group and the CTT-only group in terms of age, weight, or height (P>0.05 for all variables). Both groups were comparable at the start of the study, indicating that any differences observed in post-intervention outcomes are unlikely to be due to variations in these basic characteristics. Table 1 presents the results.
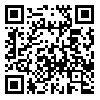
The results in Table 2 and Figure 1 show that CSE with CTT effectively reduces pain in adults with NSLBP.
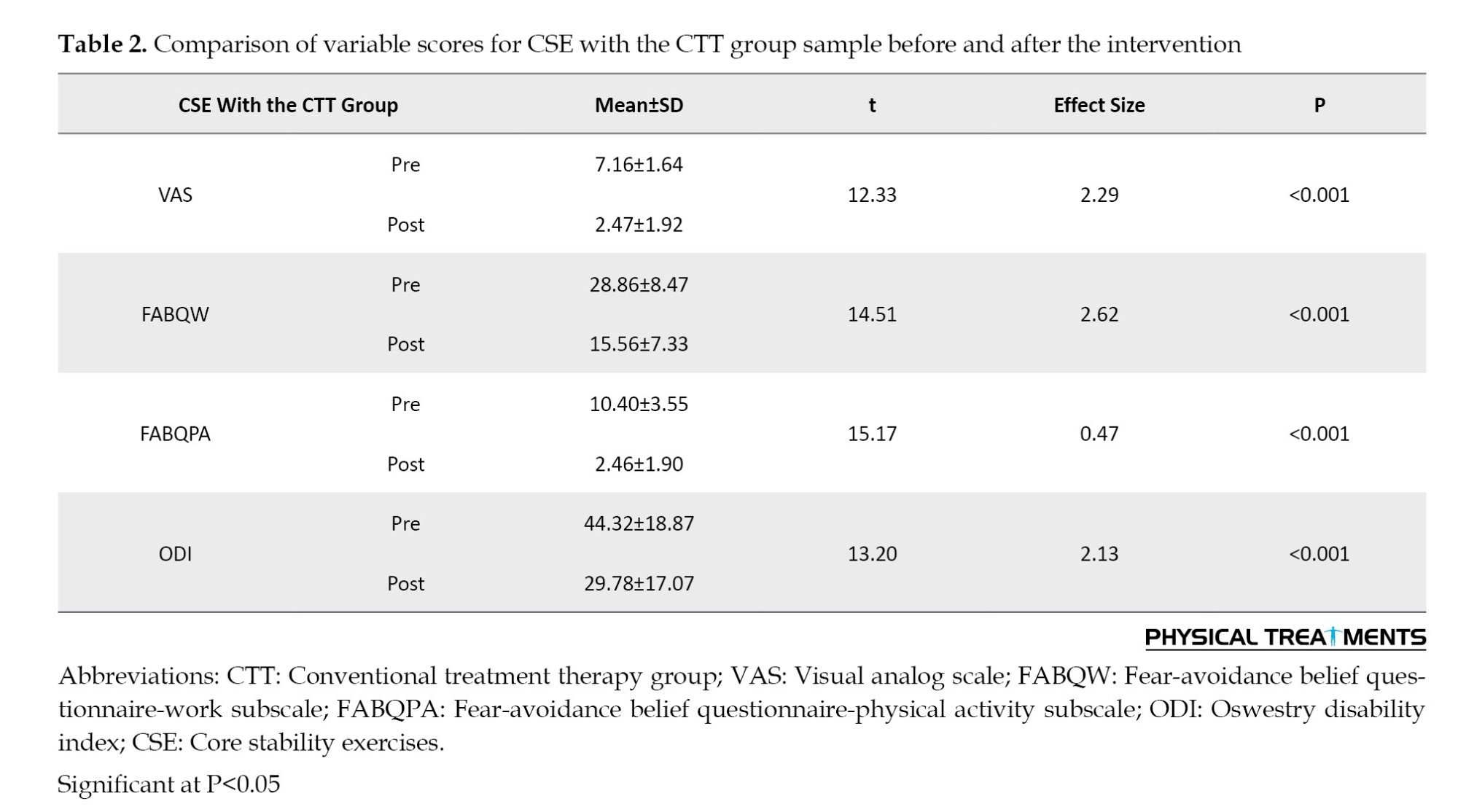
Paired sample t-tests revealed a significant reduction in pain, with the mean VAS score decreasing from 7.16±1.64 before treatment to 2.47±1.92 after treatment (P<0.05). The effect size was 2.29, indicating a substantial and clinically meaningful improvement, highlighting CTT as an effective treatment for NSLBP.
According to Table 2 and Figure 1, CSE with CTT significantly reduced fear-avoidance beliefs, as evidenced by the substantial decrease in both FABQ-work subscale (FABQW) (from 28.86±8.47 to 15.56±7.33, P<0.001) and FABQ-physical activity subscale (FABQPA) (from 10.40±3.55 to 2.46±1.90, P<0.001). CSE with CTT helps manage NSLBP by reducing fear-avoidance beliefs. Additionally, the ODI showed a significant reduction in disability from 44.32±18.87% to 29.78±17.07%, with an effect size of 2.13, indicating improved functional status following the intervention.
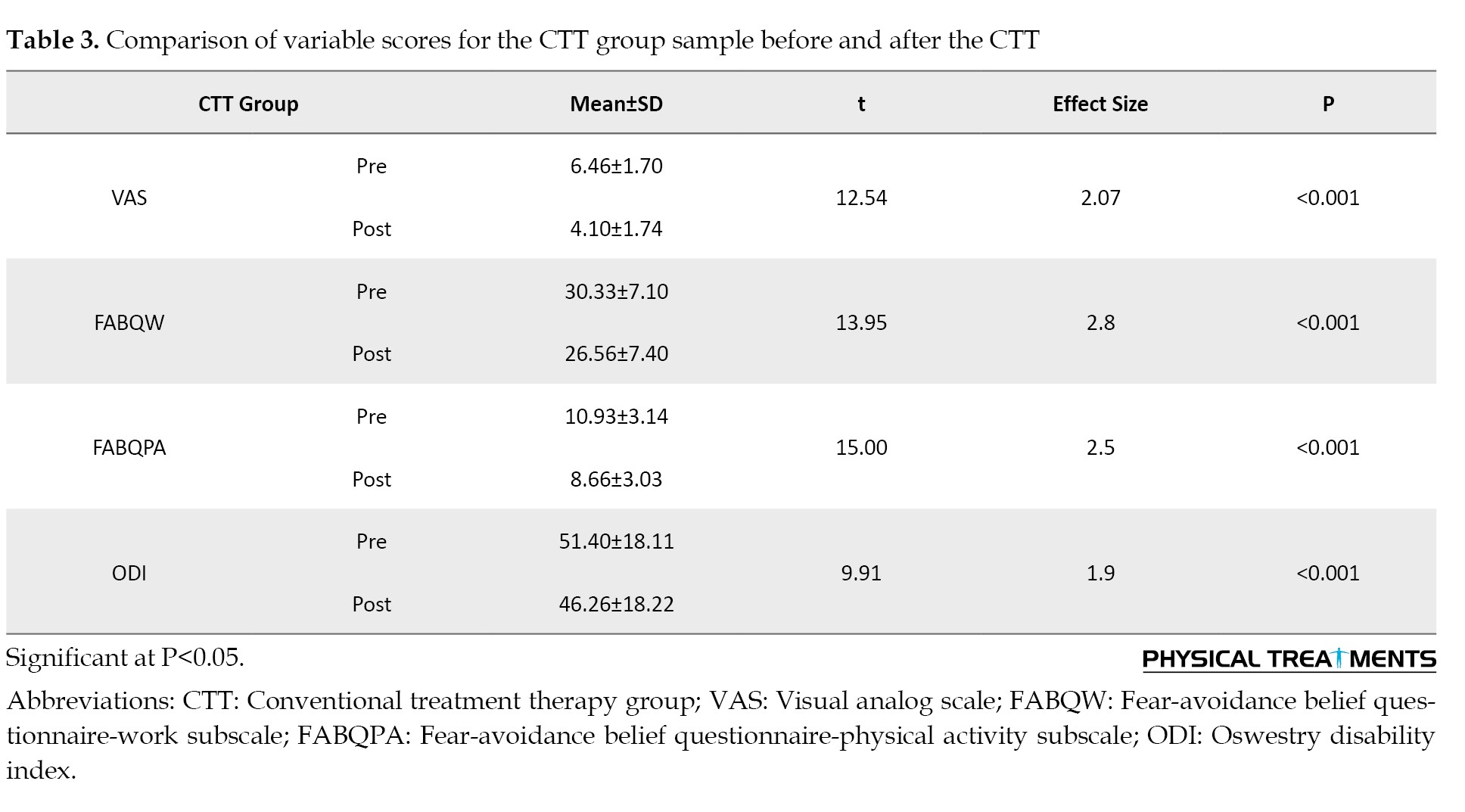
According to Table 3 and Figure 2, the study found that CTT alone significantly reduced pain, fear-avoidance beliefs, and disability in adults with NSLBP.
According to Table 2 and Figure 1, CSE with CTT significantly reduced fear-avoidance beliefs, as evidenced by the substantial decrease in both FABQ-work subscale (FABQW) (from 28.86±8.47 to 15.56±7.33, P<0.001) and FABQ-physical activity subscale (FABQPA) (from 10.40±3.55 to 2.46±1.90, P<0.001). CSE with CTT helps manage NSLBP by reducing fear-avoidance beliefs. Additionally, the ODI showed a significant reduction in disability from 44.32±18.87% to 29.78±17.07%, with an effect size of 2.13, indicating improved functional status following the intervention.
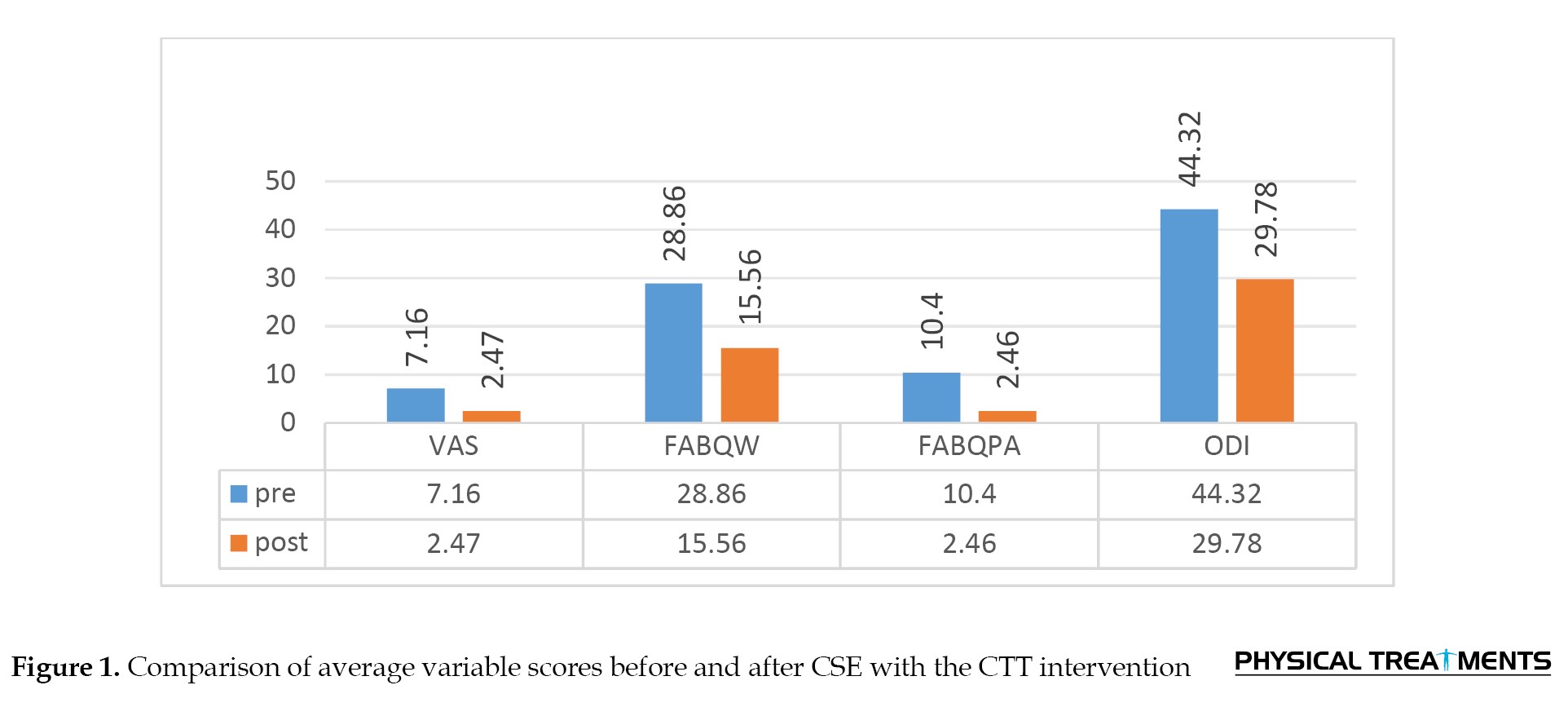
According to Table 3 and Figure 2, the study found that CTT alone significantly reduced pain, fear-avoidance beliefs, and disability in adults with NSLBP.
Pain decreased from 6.46±1.70 to 4.10±1.74 (P<0.05, effect size 2.07). Fear-avoidance beliefs also improved, with the FABQW score dropping from 30.33±7.10 to 26.56±7.40 (P<0.001, effect size 2.8) and the FABQPA score from 10.93±3.14 to 8.66±3.03 (P<0.001, effect size 2.5). Additionally, the ODI score decreased from 51.40±18.11% to 46.26±18.22% (P<0.001), indicating that CTT is effective in improving pain, fear-avoidance beliefs, and physical function in NSLBP patients.
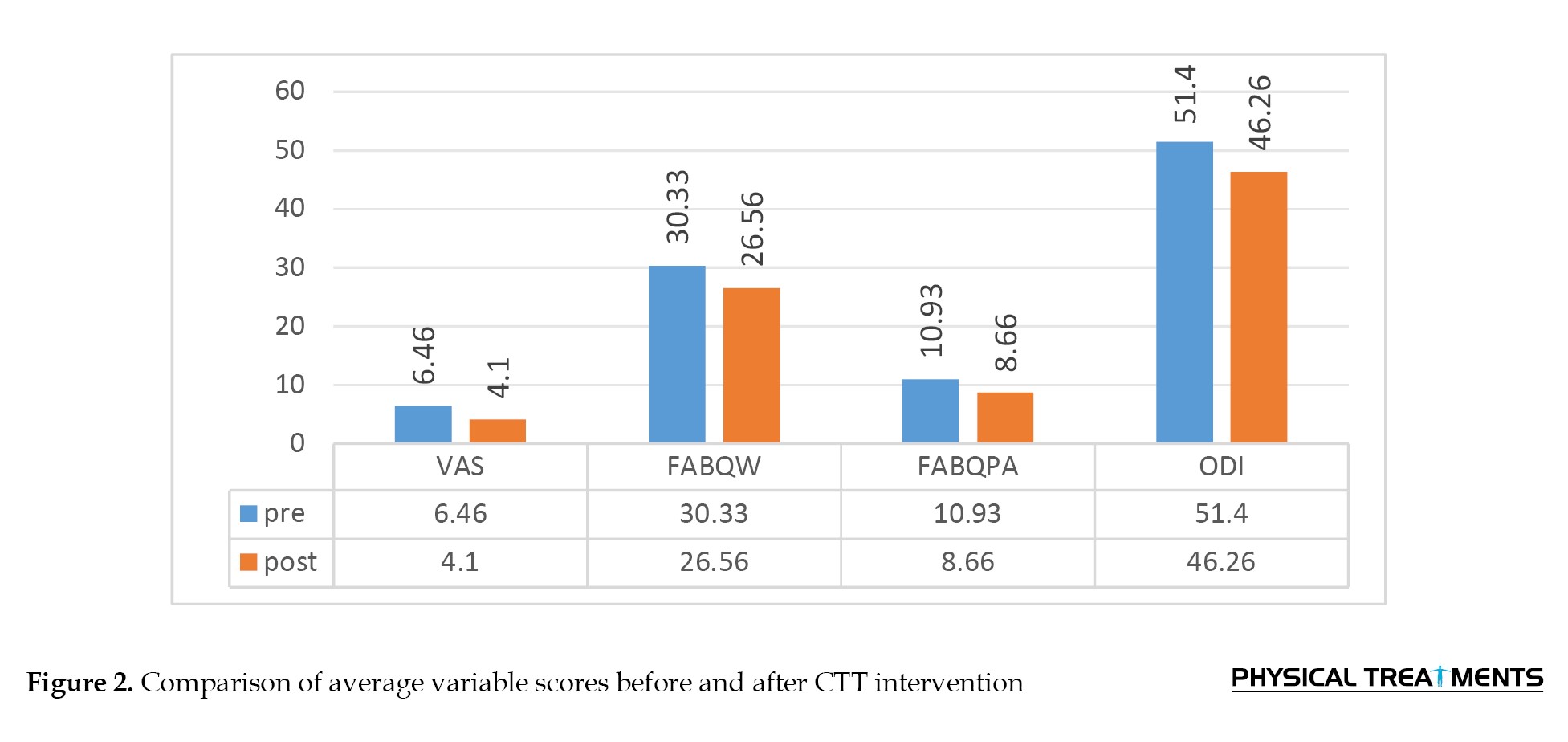
Table 4 and Figure 3 show that the CSE+CTT group had greater improvements than the CTT-only group across all outcome measures.
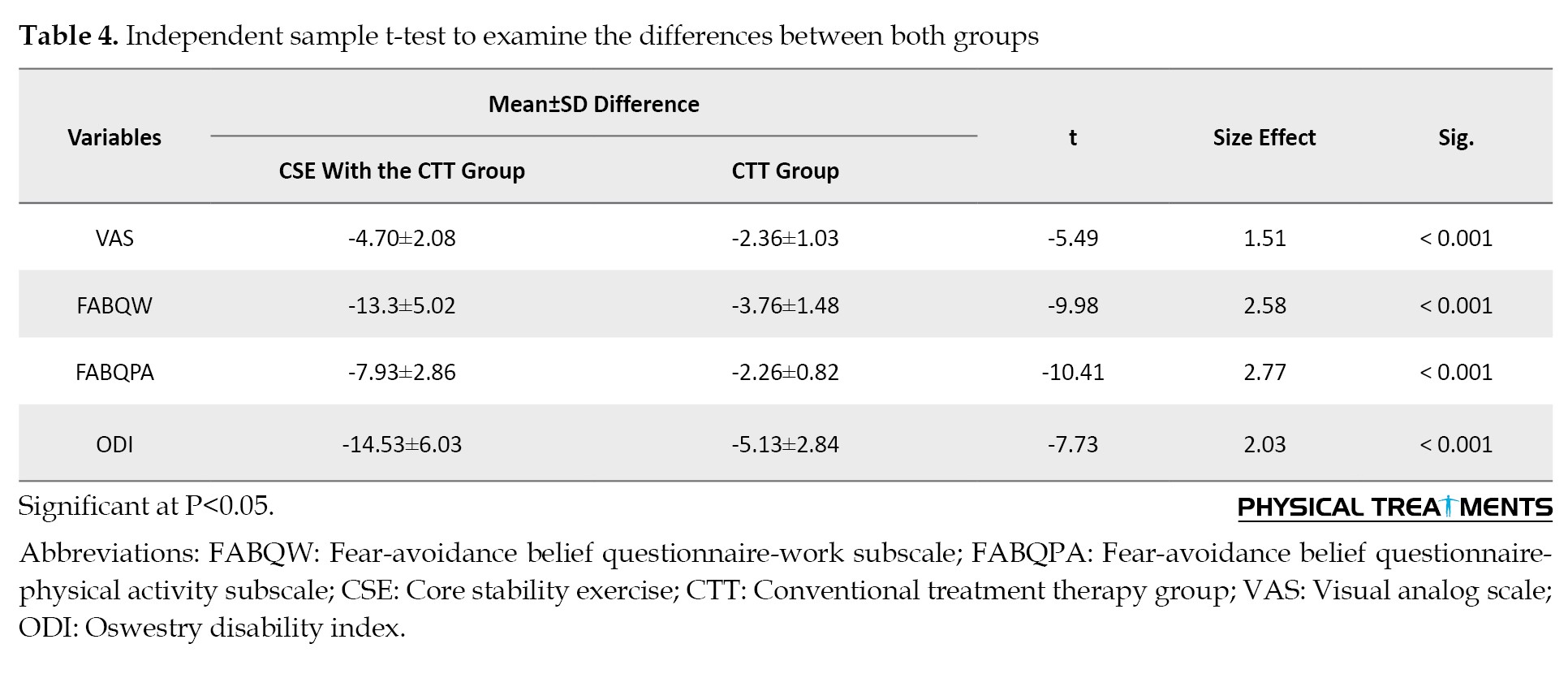
Table 4 and Figure 3 show that the CSE+CTT group had greater improvements than the CTT-only group across all outcome measures.
The CSE+CTT group exhibited a higher mean reduction in pain (VAS score difference of -4.70) compared to the CTT-only group (-2.36). This significant difference, with an effect size of 1.51 (P<0.001), indicates that CSE with CTT was more effective in reducing pain, fear-avoidance beliefs, and disability.
The CSE+CTT group showed significantly better results in fear-avoidance beliefs and disability reduction. The FABQW score decreased by -13.3 in the CSE+CTT group, compared to -3.76 in the CTT-only group (effect size 2.58, P<0.001). Similarly, the CSE+CTT group had greater reductions in FABQPA (-7.93 vs -2.26) and ODI (-14.53% vs -5.13%) compared to the CTT-only group, with a combined effect size of 2.03 (P<0.001). These findings indicate that combining CSE with CTT led to greater improvements in pain, fear-avoidance beliefs, and disability compared to CTT alone.
Discussion
CNLBP is a common condition that leads to chronic lower back pain, often related to biomechanical, psychological, and lifestyle issues. Poor posture, inactivity, and stress are the risk factors. Physical therapy, training core stability, treatment with drugs, and patient education form the treatment. Active patient involvement as part of a multidisciplinary approach is effective in relief of symptoms and improved well-being [6]. This study aimed to compare and evaluate the effectiveness of CTT and CSE with CTT in symptom reduction and improving function in patients with CNLBP. Sixty CNLBP patients were assessed according to inclusion and exclusion criteria established.
Adding CSE to routine treatment therapy (CTT) compared to the application of CTT alone was more effective in reducing pain, fear-avoidance beliefs, and disability in CNLBP patients. Specifically, the CSE+CTT group had significantly higher VAS, FABQW, FABQPA, and ODI score reductions (P<0.001). These results are consistent with those of Goswami et al. (2024), showing that CSE was superior to traditional physiotherapy in pain and disability reduction, again attesting its effectiveness in improving the outcome of rehabilitation for lower back pain patients [23]. Core strengthening exercises help mitigate back pain, improve function, and decrease fear-avoidance by increasing the muscles that stabilize the spine, facilitating optimal movement, pain alleviation, confidence, and overall stabilization of the body.
The study “review of core stability exercise versus conventional exercise in the management of chronic LBP” by Nwodo et al. (2022) confirms the effectiveness of CSE in the management of chronic LBP, with their most important advantages including spinal stability enhancement, reduction of pain, and functional mobility. Literature indicates that CSE causes greater gains in pain intensity and disability compared to conventional exercises, which justifies the inclusion of CSE within rehabilitation therapy. In this research, our findings confirm these observations in endorsing CSE administered in addition to CTT for the management of chronic LBP, but inviting further research into their combined efficacy [24].
Frizziero et al. (2021) demonstrated that CSE, including deep abdominal and back muscles, effectively reduce pain, functionality, and quality of life in CNLBP patients. The study advocates for the adoption of tailored rehabilitation programs incorporating these exercises for enhanced long-term recovery [3]. Our findings are consistent with the findings of Frizziero et al. (2021), highlighting enhanced pain relief and functional improvement achieved from the CSE and emphasizing their applicability in the rehabilitation of CNLBP as part of an individualized rehabilitation approach.
Koyuncu et al. (2024) compared core stabilization exercises performed on the Huber Motion Lab with conventional therapy for nonspecific LBP. Both groups experienced gains in disability, pain, mobility, and muscle endurance but greater gains in balance and core muscle activation in the Huber Motion Lab group. In contrast, this study determined that the incorporation of CSE as part of traditional treatment therapy yielded superior improvements in pain and disability as measured by the VAS and ODI compared with traditional treatment therapy alone [25]. These findings suggest that despite both being beneficial, CSE added to conventional therapy may bring about more significant improvement in pain relief and functional disability compared to either therapy in isolation [25].
Akhtar et al. (2017) compared core stabilization exercises with conventional therapy in CNLBP and found enhanced recovery in pain relief and functional capacity in the group that received core stabilization exercise. The study concluded that core stabilization exercises are more effective than traditional exercises in managing chronic LBP and validating their inclusion in rehabilitation [26]. Our study concurs with this, emphasizing the benefit of core stabilization exercises, particularly when complemented with CTT, on maximizing pain relief and functional capacity among patients with chronic LBP.
The Kumar et al. (2023) study contrasted core stabilization exercises with standard exercises in treating NSLBP. Findings showed that the core stabilization group had a greater degree of pain relief with a mean VAS score of 2.96 compared to 3.89 for the standard group (P<0.0001). The study concluded that core stabilization exercises were superior in improving pain in patients with NSLBP and recommended their inclusion in treatment protocols [27]. Both the present research and the Kumar et al. study aim to address chronic LBP through exercise therapy. While Kumar et al. compared standard exercises to core stabilization exercises, our study compares a combined CSE with CTT to CTT alone. Both studies highlight the effectiveness of exercise intervention in improving pain outcomes for patients with chronic LBP.
Londhe et al. (2020) investigated the effectiveness of core stabilization exercises in reducing LBP among nurses, identifying pain relief and functional capacity improvement among patients undergoing the exercise. The research highlighted the value of adding core stabilization to workplace wellness programs for physically demanding jobs, such as nursing [28]. Both studies support our findings by demonstrating the effectiveness of core stabilization exercises in reducing pain and improving functional capacity. While Londhe et al. highlighted the benefits to nurses, our research suggests that incorporating core stabilization into CTT further enhances pain and functional outcomes in patients with CNLBP.
Reddy, Jerome, and Kumar (2015) compared traditional physiotherapy with core stabilization exercises for chronic mechanical LBP. Both groups showed significant improvement in pain reduction, with the core stabilization group exhibiting more significant gains. The study found that core stabilization exercises were more effective in reducing pain and increasing functional mobility and recommended their implementation in rehabilitation of chronic LBP patients [29]. This finding is consistent with our study, as both indicate that incorporating core stabilization exercises enhances pain reduction and functional capacity. Notably, our study demonstrated greater improvements when CSE was combined with CTT.
Bibi and Shah (2023) conducted a randomized controlled trial to compare CSE versus conventional treatment for LBP. Both treatments reduced pain and improved function, but the group receiving CSE showed better results in VAS and ODI scores. The study suggests that CSE is superior and should be incorporated in rehabilitation programs to enhance recovery and quality of life [30]. Our study confirms these findings, highlighting the increased pain relief and functional gain with CSE compared to standard therapy, supporting their inclusion in existing therapeutic practice.
This study examined the impact of combining CSE with conventional therapy versus conventional therapy alone on fear avoidance beliefs. The results indicated that the combination of stability exercises and conventional therapy had a greater positive effect on fear avoidance. This research is unique in applying this scale to evaluate the combined treatment, as no prior studies have explored this topic.
Adding CSE to CTT for CNLBP led to greater improvements in pain, disability, and fear-avoidance beliefs than CTT alone. This is likely because of several mechanisms: CSE increases the activation of deep trunk muscles (such as the transversus abdominis and multifidus), improves segmental spinal control, and restores proprioception. This leads to better movement accuracy and less abnormal loading. Furthermore, CSE may modulate pain perception in the central nervous system, facilitate cortical reorganization, and reduce fear avoidance through gradual exposure to movement. CTT provides temporary pain relief that makes it easier to exercise, but it does not address underlying motor control or mental health issues. Previous studies have shown that motor control exercises yield better short-term results, particularly when combined with passive modalities and educational components.
To ensure the reliability of analytical results, researchers must control for age variation in their studies. Furthermore, to enhance participant comprehension across diverse backgrounds, it is crucial to validate outcome measures, such as the ODI and FABQ, using culturally relevant Arabic versions. Employing authentic Arabic translations of these instruments minimize confusion and lead to more dependable study.
This research possesses several strengths, including its randomized controlled trial design, which enhances reliability, and the use of allocation concealment via sealed envelopes to minimize selection bias. The study utilized validated outcome measures—VAS, ODI, and FABQ—which are suitable for assessing the multifaceted, biopsychosocial nature of CNLBP. Additionally, the incorporation of effect sizes alongside P-values strengthens the statistical rigor of the findings. Moreover, the research is distinguished by its inclusion of the fear-avoidance belief scale, a significant psychological variable often overlooked in related studies. This study has several limitations. The small sample size and short intervention duration significantly limit the generalizability and long-term applicability of the findings. Furthermore, including participants from only two clinical centers may restrict external validity. The lack of long-term follow-up also prevents the measurement of sustained benefits. Despite these limitations, the study makes a strong case for core stability training in CNLBP within the routine management.
However, this study is compromised by a small sample size, a short intervention time with lack of prolonged follow-up, and variability of therapist experience, all of which can provoke bias. Subsequent research should control for these confounds by using larger sample sizes, longer follow-up periods, and more homogeneous therapist training to confirm these results and guide their application.
Conclusion
The study conducted on adults with CNLBP in Bethlehem demonstrated that while CSE+CTT and CTT alone effectively reduced pain, disability, and fear-avoidance beliefs after four weeks, the combined approach yielded significantly greater improvements. These findings suggest that integrating CSE into conventional physiotherapy protocols can offer enhanced benefits for patients with CNLBP. Clinicians are encouraged to incorporate targeted core stability training alongside standard therapies to optimize patient outcomes. Further research is essential to determine the most effective long-term therapy options and to assess enduring benefits beyond the initial treatment phase.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of the University of Ahliyay, Bethlehem, Palestine (Code: CAMS/PTBR/3/145/2024). The Universal Trial Number assigned by the World Health Organization (WHO) (Code: U1111-1316-4673). Before any data collection, patients provided their informed consent, adhering to the Helsinki Declaration of 2008.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Formal analysis, project administration, supervision, resources, visualization and software, Writing, review and editing: Azzam Alarab; Writing the original draft: Maram Abu Aker; Conceptualization, validation, investigation, methodology and data collection: All authors.
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgments
The authors thank all the patients who participated in the study.
The CSE+CTT group showed significantly better results in fear-avoidance beliefs and disability reduction. The FABQW score decreased by -13.3 in the CSE+CTT group, compared to -3.76 in the CTT-only group (effect size 2.58, P<0.001). Similarly, the CSE+CTT group had greater reductions in FABQPA (-7.93 vs -2.26) and ODI (-14.53% vs -5.13%) compared to the CTT-only group, with a combined effect size of 2.03 (P<0.001). These findings indicate that combining CSE with CTT led to greater improvements in pain, fear-avoidance beliefs, and disability compared to CTT alone.
Discussion
CNLBP is a common condition that leads to chronic lower back pain, often related to biomechanical, psychological, and lifestyle issues. Poor posture, inactivity, and stress are the risk factors. Physical therapy, training core stability, treatment with drugs, and patient education form the treatment. Active patient involvement as part of a multidisciplinary approach is effective in relief of symptoms and improved well-being [6]. This study aimed to compare and evaluate the effectiveness of CTT and CSE with CTT in symptom reduction and improving function in patients with CNLBP. Sixty CNLBP patients were assessed according to inclusion and exclusion criteria established.
Adding CSE to routine treatment therapy (CTT) compared to the application of CTT alone was more effective in reducing pain, fear-avoidance beliefs, and disability in CNLBP patients. Specifically, the CSE+CTT group had significantly higher VAS, FABQW, FABQPA, and ODI score reductions (P<0.001). These results are consistent with those of Goswami et al. (2024), showing that CSE was superior to traditional physiotherapy in pain and disability reduction, again attesting its effectiveness in improving the outcome of rehabilitation for lower back pain patients [23]. Core strengthening exercises help mitigate back pain, improve function, and decrease fear-avoidance by increasing the muscles that stabilize the spine, facilitating optimal movement, pain alleviation, confidence, and overall stabilization of the body.
The study “review of core stability exercise versus conventional exercise in the management of chronic LBP” by Nwodo et al. (2022) confirms the effectiveness of CSE in the management of chronic LBP, with their most important advantages including spinal stability enhancement, reduction of pain, and functional mobility. Literature indicates that CSE causes greater gains in pain intensity and disability compared to conventional exercises, which justifies the inclusion of CSE within rehabilitation therapy. In this research, our findings confirm these observations in endorsing CSE administered in addition to CTT for the management of chronic LBP, but inviting further research into their combined efficacy [24].
Frizziero et al. (2021) demonstrated that CSE, including deep abdominal and back muscles, effectively reduce pain, functionality, and quality of life in CNLBP patients. The study advocates for the adoption of tailored rehabilitation programs incorporating these exercises for enhanced long-term recovery [3]. Our findings are consistent with the findings of Frizziero et al. (2021), highlighting enhanced pain relief and functional improvement achieved from the CSE and emphasizing their applicability in the rehabilitation of CNLBP as part of an individualized rehabilitation approach.
Koyuncu et al. (2024) compared core stabilization exercises performed on the Huber Motion Lab with conventional therapy for nonspecific LBP. Both groups experienced gains in disability, pain, mobility, and muscle endurance but greater gains in balance and core muscle activation in the Huber Motion Lab group. In contrast, this study determined that the incorporation of CSE as part of traditional treatment therapy yielded superior improvements in pain and disability as measured by the VAS and ODI compared with traditional treatment therapy alone [25]. These findings suggest that despite both being beneficial, CSE added to conventional therapy may bring about more significant improvement in pain relief and functional disability compared to either therapy in isolation [25].
Akhtar et al. (2017) compared core stabilization exercises with conventional therapy in CNLBP and found enhanced recovery in pain relief and functional capacity in the group that received core stabilization exercise. The study concluded that core stabilization exercises are more effective than traditional exercises in managing chronic LBP and validating their inclusion in rehabilitation [26]. Our study concurs with this, emphasizing the benefit of core stabilization exercises, particularly when complemented with CTT, on maximizing pain relief and functional capacity among patients with chronic LBP.
The Kumar et al. (2023) study contrasted core stabilization exercises with standard exercises in treating NSLBP. Findings showed that the core stabilization group had a greater degree of pain relief with a mean VAS score of 2.96 compared to 3.89 for the standard group (P<0.0001). The study concluded that core stabilization exercises were superior in improving pain in patients with NSLBP and recommended their inclusion in treatment protocols [27]. Both the present research and the Kumar et al. study aim to address chronic LBP through exercise therapy. While Kumar et al. compared standard exercises to core stabilization exercises, our study compares a combined CSE with CTT to CTT alone. Both studies highlight the effectiveness of exercise intervention in improving pain outcomes for patients with chronic LBP.
Londhe et al. (2020) investigated the effectiveness of core stabilization exercises in reducing LBP among nurses, identifying pain relief and functional capacity improvement among patients undergoing the exercise. The research highlighted the value of adding core stabilization to workplace wellness programs for physically demanding jobs, such as nursing [28]. Both studies support our findings by demonstrating the effectiveness of core stabilization exercises in reducing pain and improving functional capacity. While Londhe et al. highlighted the benefits to nurses, our research suggests that incorporating core stabilization into CTT further enhances pain and functional outcomes in patients with CNLBP.
Reddy, Jerome, and Kumar (2015) compared traditional physiotherapy with core stabilization exercises for chronic mechanical LBP. Both groups showed significant improvement in pain reduction, with the core stabilization group exhibiting more significant gains. The study found that core stabilization exercises were more effective in reducing pain and increasing functional mobility and recommended their implementation in rehabilitation of chronic LBP patients [29]. This finding is consistent with our study, as both indicate that incorporating core stabilization exercises enhances pain reduction and functional capacity. Notably, our study demonstrated greater improvements when CSE was combined with CTT.
Bibi and Shah (2023) conducted a randomized controlled trial to compare CSE versus conventional treatment for LBP. Both treatments reduced pain and improved function, but the group receiving CSE showed better results in VAS and ODI scores. The study suggests that CSE is superior and should be incorporated in rehabilitation programs to enhance recovery and quality of life [30]. Our study confirms these findings, highlighting the increased pain relief and functional gain with CSE compared to standard therapy, supporting their inclusion in existing therapeutic practice.
This study examined the impact of combining CSE with conventional therapy versus conventional therapy alone on fear avoidance beliefs. The results indicated that the combination of stability exercises and conventional therapy had a greater positive effect on fear avoidance. This research is unique in applying this scale to evaluate the combined treatment, as no prior studies have explored this topic.
Adding CSE to CTT for CNLBP led to greater improvements in pain, disability, and fear-avoidance beliefs than CTT alone. This is likely because of several mechanisms: CSE increases the activation of deep trunk muscles (such as the transversus abdominis and multifidus), improves segmental spinal control, and restores proprioception. This leads to better movement accuracy and less abnormal loading. Furthermore, CSE may modulate pain perception in the central nervous system, facilitate cortical reorganization, and reduce fear avoidance through gradual exposure to movement. CTT provides temporary pain relief that makes it easier to exercise, but it does not address underlying motor control or mental health issues. Previous studies have shown that motor control exercises yield better short-term results, particularly when combined with passive modalities and educational components.
To ensure the reliability of analytical results, researchers must control for age variation in their studies. Furthermore, to enhance participant comprehension across diverse backgrounds, it is crucial to validate outcome measures, such as the ODI and FABQ, using culturally relevant Arabic versions. Employing authentic Arabic translations of these instruments minimize confusion and lead to more dependable study.
This research possesses several strengths, including its randomized controlled trial design, which enhances reliability, and the use of allocation concealment via sealed envelopes to minimize selection bias. The study utilized validated outcome measures—VAS, ODI, and FABQ—which are suitable for assessing the multifaceted, biopsychosocial nature of CNLBP. Additionally, the incorporation of effect sizes alongside P-values strengthens the statistical rigor of the findings. Moreover, the research is distinguished by its inclusion of the fear-avoidance belief scale, a significant psychological variable often overlooked in related studies. This study has several limitations. The small sample size and short intervention duration significantly limit the generalizability and long-term applicability of the findings. Furthermore, including participants from only two clinical centers may restrict external validity. The lack of long-term follow-up also prevents the measurement of sustained benefits. Despite these limitations, the study makes a strong case for core stability training in CNLBP within the routine management.
However, this study is compromised by a small sample size, a short intervention time with lack of prolonged follow-up, and variability of therapist experience, all of which can provoke bias. Subsequent research should control for these confounds by using larger sample sizes, longer follow-up periods, and more homogeneous therapist training to confirm these results and guide their application.
Conclusion
The study conducted on adults with CNLBP in Bethlehem demonstrated that while CSE+CTT and CTT alone effectively reduced pain, disability, and fear-avoidance beliefs after four weeks, the combined approach yielded significantly greater improvements. These findings suggest that integrating CSE into conventional physiotherapy protocols can offer enhanced benefits for patients with CNLBP. Clinicians are encouraged to incorporate targeted core stability training alongside standard therapies to optimize patient outcomes. Further research is essential to determine the most effective long-term therapy options and to assess enduring benefits beyond the initial treatment phase.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of the University of Ahliyay, Bethlehem, Palestine (Code: CAMS/PTBR/3/145/2024). The Universal Trial Number assigned by the World Health Organization (WHO) (Code: U1111-1316-4673). Before any data collection, patients provided their informed consent, adhering to the Helsinki Declaration of 2008.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Formal analysis, project administration, supervision, resources, visualization and software, Writing, review and editing: Azzam Alarab; Writing the original draft: Maram Abu Aker; Conceptualization, validation, investigation, methodology and data collection: All authors.
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgments
The authors thank all the patients who participated in the study.
References
- Deyo RA, Cherkin D, Conrad D, Volinn E. Cost, controversy, crisis: low back pain and the health of the public. Annual Review of Public Health. 1991; 12:141-56. [DOI:10.1146/annurev.pu.12.050191.001041] [PMID]
- Hoy D, Bain C, Williams G, March L, Brooks P, Blyth F, Woolf A, Vos T, Buchbinder R. A systematic review of the global prevalence of low back pain. Arthritis and Rheumatism. 2012; 64(6):2028-37. [DOI:10.1002/art.34347] [PMID]
- GBD 2021 Low Back Pain Collaborators. Global, regional, and national burden of low back pain, 1990-2020, its attributable risk factors, and projections to 2050: A systematic analysis of the global burden of disease study 2021. The Lancet. Rheumatology. 2023; 5(6):e316-29. [DOI:10.1016/S2665-9913(23)00098-X] [PMID]
- Chen S, Chen M, Wu X, Lin S, Tao C, Cao H, et al. Global, regional and national burden of low back pain 1990-2019: A systematic analysis of the global burden of disease study 2019. Journal of Orthopaedic Translation. 2021; 32:49-58. [DOI:10.1016/j.jot.2021.07.005] [PMID]
- Safiri S, Nejadghaderi SA, Noori M, Sullman MJM, Collins GS, Kaufman JS, et al. The burden of low back pain and its association with socio-demographic variables in the Middle East and North Africa region, 1990-2019. BMC Musculoskeletal Disorders. 2023; 24(1):59. [DOI:10.1186/s12891-023-06178-3] [PMID]
- Nicol V, Verdaguer C, Daste C, Bisseriex H, Lapeyre É, Lefèvre-Colau MM, et al. Chronic low back pain: A narrative review of recent international guidelines for diagnosis and conservative treatment. Journal of Clinical Medicine. 2023; 12(4):1685. [DOI:10.3390/jcm12041685] [PMID]
- Gong C, Dai S, Jin B, Xie Y. Comparison of Feng spinal mobilization with Maitland mobilization in management of chronic nonspecific low back pain: A cohort study. Medicine. 2023; 102(7):e32984. [DOI:10.1097/MD.0000000000032984] [PMID]
- Chiarotto A, Koes BW. Nonspecific low back pain. The New England Journal of Medicine. 2022; 386(18):1732-40. [DOI:10.1056/NEJMcp2032396] [PMID]
- Sirbu E, Onofrei RR, Szasz S, Susan M. Predictors of disability in patients with chronic low back pain. Archives of Medical Science. 2020; 19(1):94-100. [DOI:10.5114/aoms.2020.97057] [PMID]
- Robinault L, Niazi IK, Kumari N, Amjad I, Menard V, Haavik H. Non-specific low back pain: An inductive exploratory analysis through factor analysis and deep learning for better clustering. Brain Sciences. 2023; 13(6):946. [DOI:10.3390/brainsci13060946] [PMID]
- Custers P, Van de Kelft E, Eeckhaut B, Sabbe W, Hofman A, Debuysscher A, et al. Clinical examination, diagnosis, and conservative treatment of chronic low back pain: A narrative review. Life. 2024; 14(9):1090. [DOI:10.3390/life14091090] [PMID]
- Ahmed F, Rahman MU, Ullah K, Bhutta AH. Combination of core stability exercises and maitland manual therapy is better alternative in the management of chronic low back pain. Journal Riphah College of Rehabilitation Sciences. 2020; 8(01):S24-8. [DOI:10.5455/JRCRS.202008SI06]
- Dimitrijević V, Rašković B, Jevtić N, Nikolić S, Viduka D, Obradović B. Pain and disability therapy with stabilization exercises in patients with chronic low back pain: A meta-analysis. Healthcare. 2025; 13(9):960. [DOI:10.3390/healthcare13090960] [PMID]
- Boonstra AM, Schiphorst Preuper HR, Reneman MF, Posthumus JB, Stewart RE. Reliability and validity of the visual analogue scale for disability in patients with chronic musculoskeletal pain. International Journal of Rehabilitation Research. 2008; 31(2):165-9. [DOI:10.1097/MRR.0b013e3282fc0f93] [PMID]
- Bielewicz J, Daniluk B, Kamieniak P. VAS and NRS, same or different? Are visual analog scale values and numerical rating scale equally viable tools for assessing patients after microdiscectomy? Pain Research & Management. 2022; 2022:5337483. [DOI:10.1155/2022/5337483] [PMID]
- El Meidany YM, El Gaafary MM, Ahmed I. Cross-cultural adaptation and validation of an Arabic Health Assessment Questionnaire for use in rheumatoid arthritis patients. Joint Bone Spine. 2003; 70(3):195-202. [DOI:10.1016/S1297-319X(03)00004-6] [PMID]
- Sanjaroensuttikul N. The Oswestry low back pain disability questionnaire (version 1.0) Thai version. Journal of the Medical Association of Thailand. 2007; 90(7):1417-22. [PMID]
- Algarni AS, Ghorbel S, Jones JG, Guermazi M. Validation of an Arabic version of the Oswestry index in Saudi Arabia. Annals of Physical and Rehabilitation Medicine. 2014; 57(9-10):653-63. [DOI:10.1016/j.rehab.2014.06.006] [PMID]
- Wiangkham T, Phungwattanakul N, Tedsombun P, Kongmee I, Suwanmongkhon W, Chidnok W. Translation, cross-cultural adaptation and psychometric evaluation of the Thai version of the fear-avoidance beliefs questionnaire in patients with non-specific neck pain. Scandinavian Journal of Pain. 2020; 21(2):247-55. [DOI:10.1515/sjpain-2020-0116] [PMID]
- Nazir SNB, Pereira FA, Muhammad A, Shamsi II, Khan MU. The relationship between fear-avoidance beliefs, disability, and physical capacity in patients with chronic low back pain. Mediterranean Journal of Rheumatology. 2022; 33(3):305-10. [DOI:10.31138/mjr.33.3.305] [PMID]
- Aasdahl L, Marchand GH, Gismervik SØ, Myhre K, Fimland MS, Røe C. The fear avoidance beliefs questionnaire (FABQ) does it really measure fear beliefs? Spine. 2020; 45(2):134-40. [DOI:10.1097/BRS.0000000000003188] [PMID]
- Alanazi F, Gleeson P, Olson S, Roddey T. Translation and validation of the Arabic version of the fear-avoidance beliefs questionnaire in patients with low back pain. Spine. 2017; 42(7):E411-6. [DOI:10.1097/BRS.0000000000001802] [PMID]
- Goswami M, Tiwari M, Goswami Y, Gupta V, Tomar A. The efficacy of core stability exercises versus conventional physiotherapy in lower back pain. International Journal of Science and Research Archive Internet. 2024; 12(1):2562-7. [DOI:10.30574/ijsra.2024.12.1.1063]
- Nwodo OD, Ibikunle PO, Ogbonna NL, Ani KU, Okonkwo AC, Eze CJ, et al. Review of core stability exercise versus conventional exercise in the management of chronic low back pain. African Health Sciences. 2022; 22(4):148-67. [DOI:10.4314/ahs.v22i4.19] [PMID]
- Koyuncu E, Tunali N, Saka S, Ural E, Yavuzer M. Effects of core stabilization exercises in patients with non-specific low back pain: Huber motion lab versus conventional. Baltic Journal of Health and Physical Activity. 2024; 16(1):8. [DOI:10.29359/BJHPA.16.1.08]
- Akhtar MW, Karimi H, Gilani SA. Effectiveness of core stabilization exercises and routine exercise therapy in management of pain in chronic non-specific low back pain: A randomized controlled clinical trial. Pakistan Journal of Medical Sciences. 2017; 33(4):1002-6. [DOI:10.12669/pjms.334.12664] [PMID]
- Kumar A, Gupta V, Khan MA, Srivastava H. Efficacy of core stabilization program and conventional exercises in low back pain. International Journal of Community Medicine And Public Health. 2023; 10(11):4298-302. [DOI:10.18203/2394-6040.ijcmph20233466]
- Londhe SP, Pawadshetty VS, Karanth V. To find the effectiveness of conventional exercise and core stabilization exercises in conditions with specific low back pain. International Journal of Science and Healthcare Research. 2020; 5(2):274-9. [Link]
- Karnati VNP, Sreekar Kumar Reddy R. Core stabilization program and conventional exercises in the patients with low back pain-A comparative study. International Journal of Physiotherapy. 2015; 2(1):352. [DOI:10.15621/ijphy/2015/v2i1/60041]
- Bibi M, Shah A. Comparing the efficacy of core stability exercises and conventional physical therapy in the management of lower back pain: A randomized controlled trial. Northwest Journal of Medical. 2023; 2(1):13. [DOI:10.69723/njms.02.01.0299]
Type of Study: Research |
Subject:
General
Received: 2025/01/22 | Accepted: 2025/09/14 | Published: 2026/04/16
Received: 2025/01/22 | Accepted: 2025/09/14 | Published: 2026/04/16
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
