Wed, May 27, 2026
Volume 16, Issue 1 (Winter 2026)
PTJ 2026, 16(1): 5-14 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Mohamadi S, Boozari S, Delshad V, Esmaeeli M. Effects of Taping on Pelvic Floor Dysfunctions: A Systematic Review of Randomized Controlled Trials. PTJ 2026; 16 (1) :5-14
URL: http://ptj.uswr.ac.ir/article-1-701-en.html
URL: http://ptj.uswr.ac.ir/article-1-701-en.html



1- Department of Physiotherapy, Faculty of Rehabilitation, Social Welfare and Rehabilitation Sciences University, Tehran, Iran.
2- Department of Physiotherapy, Faculty of Medical Sciences, Tarbiat Modares University, Tehran, Iran.
3- Health in Emergency and Disaster Research Center, Social Health Research Institute, Social Welfare and Rehabilitation Sciences University, Tehran, Iran.
4- Department of Physiotherapy, School of Rehabilitation, Tehran University of medical sciences, Tehran, Iran.
2- Department of Physiotherapy, Faculty of Medical Sciences, Tarbiat Modares University, Tehran, Iran.
3- Health in Emergency and Disaster Research Center, Social Health Research Institute, Social Welfare and Rehabilitation Sciences University, Tehran, Iran.
4- Department of Physiotherapy, School of Rehabilitation, Tehran University of medical sciences, Tehran, Iran.
Full-Text [PDF 587 kb]
(619 Downloads)
| Abstract (HTML) (1706 Views)
Full-Text: (195 Views)
Introduction
Pelvic floor dysfunctions are highly common clinical problems, encompassing a wide variety of disorders [1]. In addition to pelvic organ prolapse, these dysfunctions include defecatory and sexual system issues, lower urinary tract sensory and emptying abnormalities, intestinal and urinary incontinence, and several chronic pain syndromes [1, 2]. These conditions significantly influence the quality of life, especially in the female population [1, 2].
Pelvic floor physiotherapy is regarded as a primary, low-risk, minimally invasive therapy for both the management and prevention of pelvic floor dysfunctions [3, 4]. It includes pelvic floor muscle training (PFMT), electrical impulse therapy, magnetotherapy, manual therapy, laser therapy, acupuncture, behavioral therapy (bowel and bladder training), biofeedback, and kinesio taping (KT) [4-6]. However, studies using KT as a simple, safe, non-invasive and inexpensive modality for pelvic floor conditions are insufficient, and its effects in different conditions are not well understood [4].
The lower urinary tract’s sensory and emptying problems, along with issues in the defecatory and sexual systems, pelvic organ prolapse, and urinary and bowel incontinence, can have several possible causes for these conditions. One explanation for the effectiveness of KT is the reduction of compression caused by lifting the skin, fascia, and subcutaneous tissues, which increases blood and lymph circulation and, in turn, reduces inflammation and pain related to chronic pain syndromes [4, 7, 8]. Other possible mechanisms include fascial correction, which may lead to an increase in the range of motion, improvement in neuromuscular control, and enhanced joint positioning through mechanoreceptor stimulation and kinesthetic awareness [5, 7, 8]. Also, KT can facilitate or inhibit muscle activity and help in injury prevention [7]. Additionally, various studies suggest that KT application may activate the cutaneous-visceral reflex mechanism associated with Head’s zones [4-6].
Despite contradictory data regarding KT efficacy in treating various ailments and among healthy individuals, KT remains a common and widely utilized physiotherapy technique [5, 9]. This is due to the results of limited studies suggesting that KT can be clinically beneficial [7]. However, collecting and reviewing the results of valid studies in this area can still pave the way for clinical practice and future research. Therefore, despite the potential positive effects of kinesiotaping on pelvic floor dysfunctions, research on this topic is limited and unclear. This study sought to explore the effects of KT on the management of pelvic floor dysfunction, evaluating a range of outcomes in comparison to sham or certain conservative non-KT therapies. Summarizing and analyzing strong and credible studies in this field can create opportunities for future research to conduct more comprehensive and accurate studies.
Materials and Methods
Search strategy
The standards of the preferred reporting items for systematic reviews and meta-analysis (PRISMA) served as the foundation for our search approach [10]. Articles were included that examined the effects of KT alone or combination with other treatment modalities for different pelvic floor dysfunctions. Accessible databases comprising PubMed, Scopus, ScienceDirect, Medline and Web of Science were searched from the earliest records up to March 2024. the Following syntaxes were used to search relevant articles: (Kinesio-taping OR kinesio tape OR kinesiology taping) AND (pelvic floor physiotherapy OR pelvic floor physical therapy OR pelvic floor treatment OR nonpharmacological pelvic floor treatment OR pelvic floor conservative treatment) AND (pelvic floor dysfunction OR pelvic floor disorder OR vaginal dysfunction OR anal dysfunction OR urethral dysfunction OR urinary incontinence OR anal incontinence OR urge incontinence OR stress incontinence OR overactive bladder OR constipation OR sexual dysfunction OR vaginismus OR pelvic floor dyssynergia OR erectile dysfunction OR pelvic organ prolapse OR defecatory dysfunction OR voiding dysfunction OR chronic pelvic pain syndrome). We searched each of the words within each set of parentheses (a total of three sets of parentheses) that were separated by “OR” with each of the words in the next two sets of parentheses, which were separated by “AND,” using the “plus sign.” This way, with each search, we included three words or phrases, and thus we found all relevant articles (e.g. KT+pelvic floor physiotherapy+pelvic floor dysfunction).
Eligibility criteria for study selection
First, two independent authors (Somayeh Mohamadi and Sahar Boozari) considered the eligibility of the obtained studies by their titles and abstracts to identify which one can be included for peer review. The population, intervention, comparison, outcomes, and study design (PICOS) criteria were used to assess whether a study was eligible. In the present systematic review, the PICOS criteria were as follows: P: Patients with pelvic floor dysfunctions; I: KT; C: Comparison with other conservative treatment modalities; O: Improvements in quality of life, pelvic floor muscle (PFM) strength, bowel and bladder symptoms, discomfort, disability, and other aspects; S: Controlled clinical trials that are randomized.
The two researchers reviewed full-text papers if titles or abstracts did not contain sufficient information for eligibility. Duplicates were eliminated, and if the two investigators could not agree on the eligibility of any included studies, a third investigator (VD) made the final decision based on the precise inclusion and exclusion criteria, results, and research design (PICOS). In the current study, the inclusion criteria were as follows: 1) the papers should compare KT with sham KT or other conservative treatment modalities; 2) the studies should investigate pelvic floor dysfunctions; 3) the studies should report any parameters related to improvement in the pelvic symptoms (pain, PFM performance disability, bowel and bladder symptoms, quality of life, etc.); 4) only RCTs; and 5) full-text original articles were published in the English language. Articles published in other languages, articles published or presented at conferences, seminars, or theses, and research published in abstract form were excluded from the study.
Quality assessment
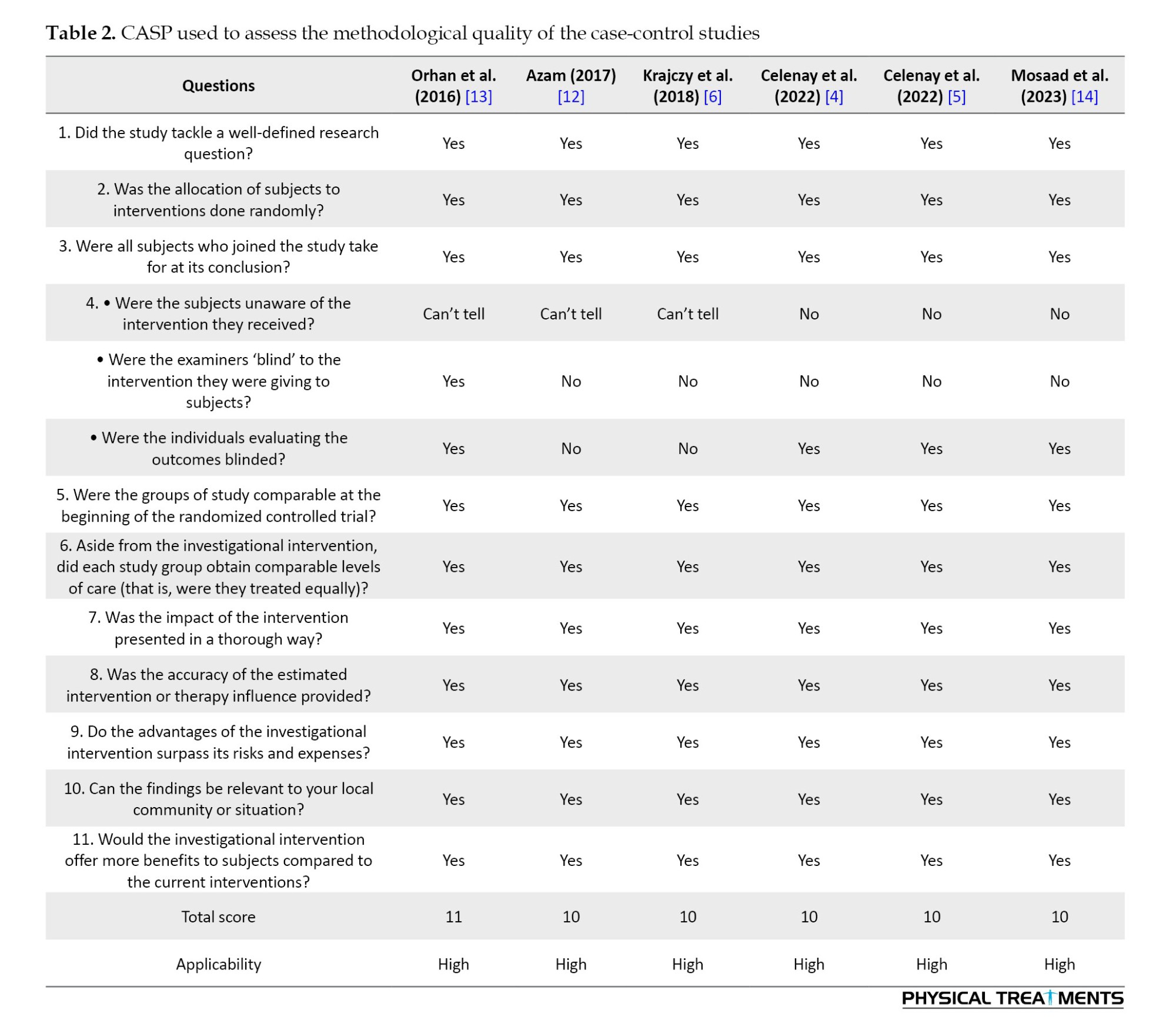
Studies included in the current systematic review were evaluated using the critical appraisal skills program (CASP) checklist for clinical trial studies in terms of methodological quality [11]. This checklist consisted of 11 questions for RTCs, organized into four sections. Section A comprises three questions addressing whether “the study design is appropriate for a randomized clinical trial.” Section B includes three questions assessing whether “the study is methodologically sound.” Section C comprises three questions focused on “what the results are.” Finally, Section D contains two questions that inquire whether “the results are locally applicable.” The questions can be answered with “yes”, “no”, or “can’t say”. All studies were scored by the same two independent investigators that assessed the eligibility of the studies. If any disagreement arose regarding the answers to questions in each article, the two investigators discussed the differences to reach a final decision. If the disagreement could not be resolved, a third researcher was involved in the discussion panel to achieve consensus. The final agreement was reached based on the majority opinion.
Data extraction
Information from all included studies was extracted and summarized in the form of a table, which includes the authors and year of publication, study design, diagnosis, participants’ characteristics (group type and sample size), outcome measures (pelvic pain, PFM strength, questionnaires, voiding diaries), and main results.
Results
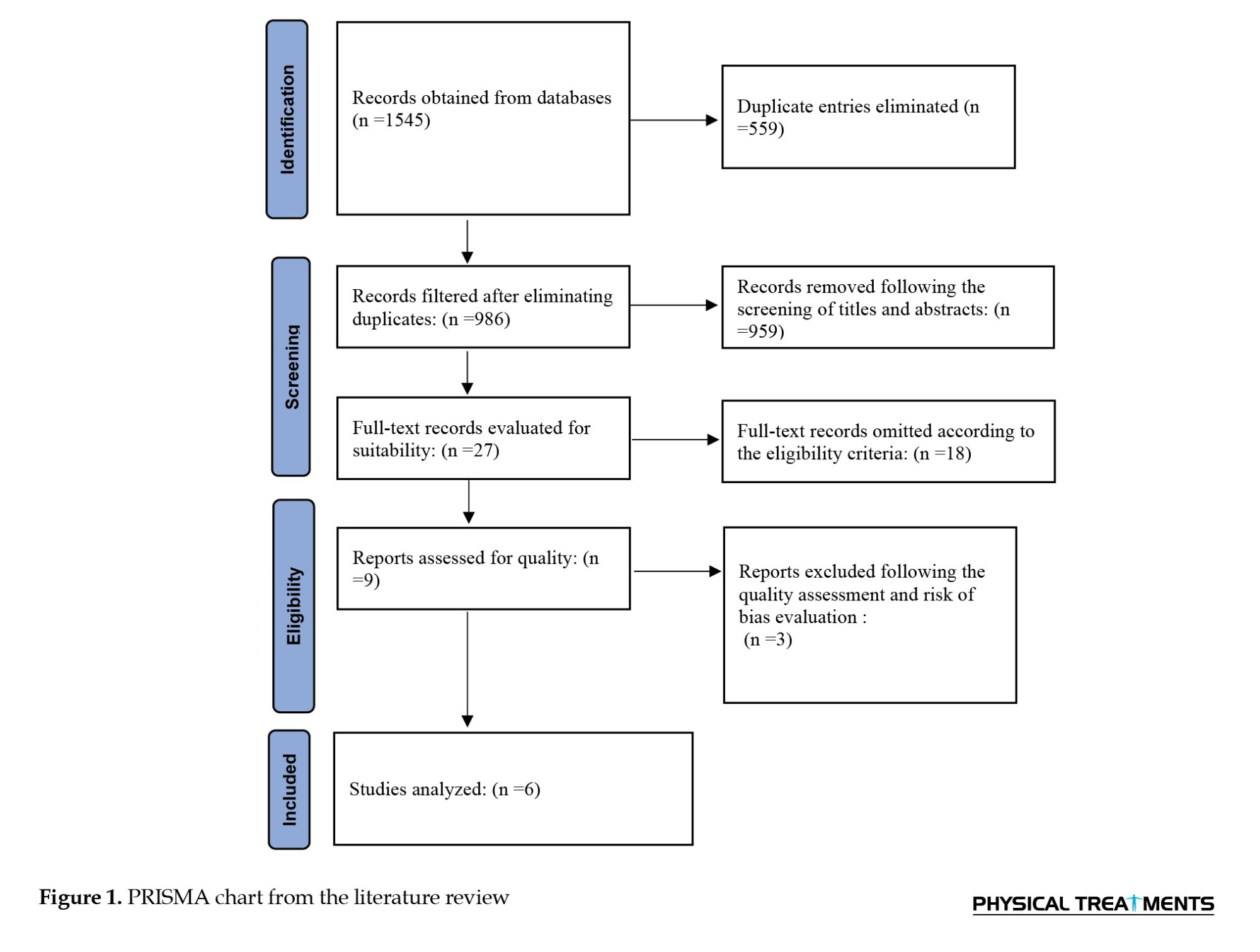
A total of 1545 possible articles were discovered in the initial search using the databases listed in the search strategy. Once duplicates were eliminated, 986 records were left. After screening the title, abstract, and full text, if required, in accordance with the inclusion and exclusion criteria, only 27 articles were deemed acceptable. Nine studies were found to be eligible after applying the CASP checklist. Ultimately, six studies were chosen for examination after receiving moderate to high-quality ratings. A flow chart of PRISMA 10 is displayed in Figure 1.
Results of the included studies
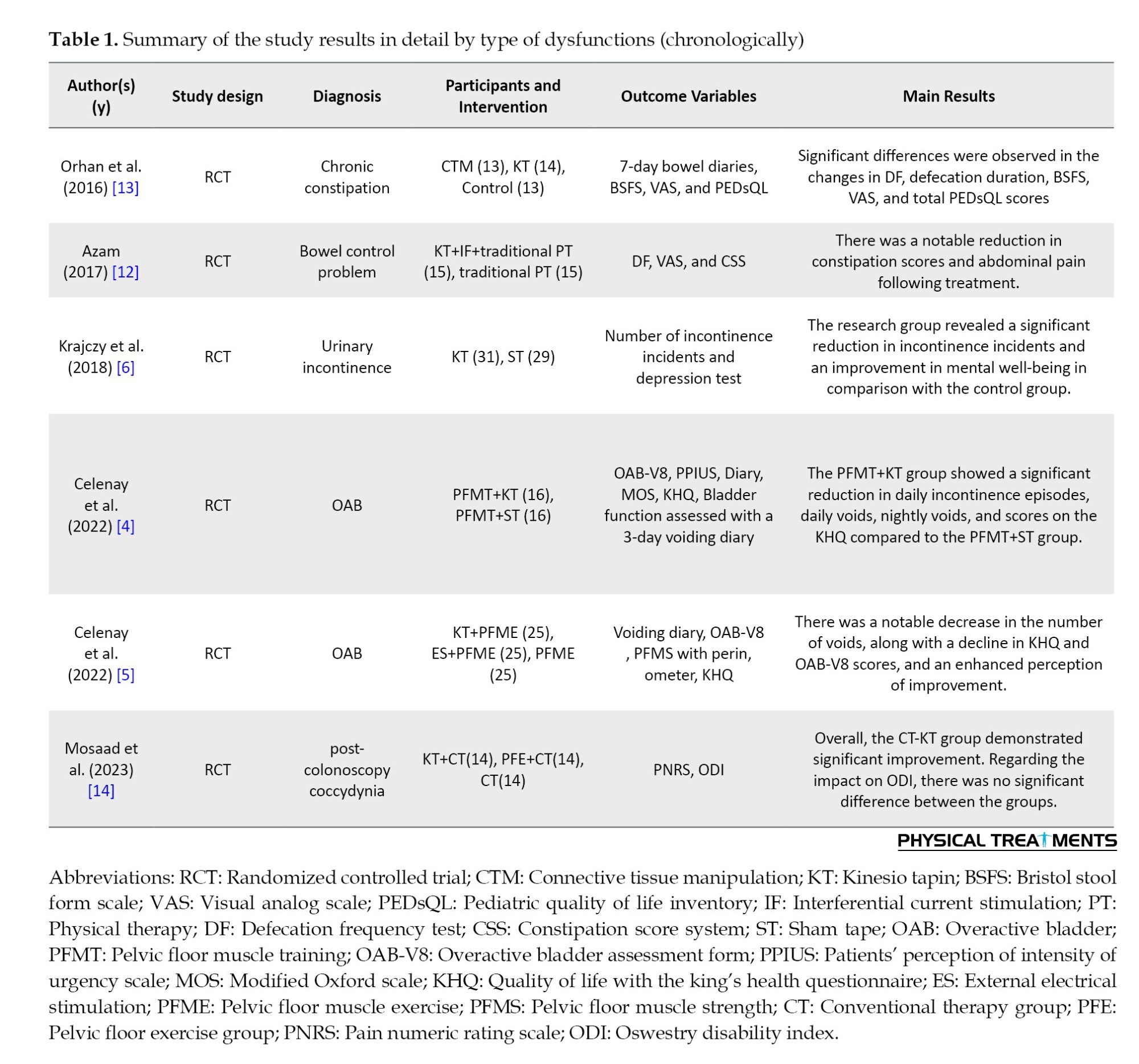
A summary of the relevant articles is presented in Table 1. Of the six studies, urinary system conditions were investigated in three studies 4-6, defecatory conditions were assessed in three studies [12, 13], and coccydynia was assessed in one study [14]. Due to the scattered and inconsistent outcome measures in the studies, it was not possible to calculate the effect size or conduct a meta-analysis.
Quality assessment
All of the featured articles had an average quality rated as moderate to high. Table 2 provides a summary of the CASP findings. High applicability was demonstrated by the included RTCs.
Discussion
This systematic review was conducted on previous studies that investigated the improvement of pelvic floor dysfunction with KT compared to other conservative treatment modalities using different outcome measures. KT, when combined with other conservative treatments, showed better therapeutic results for pelvic floor dysfunctions. Regarding the findings of the reviewed studies, most studies reported positive outcomes with KT; however, methodological limitations and inconsistent results warrant caution.
Outcome measures among the three groups of the studies based on the affected system
Effect of KT on urinary system conditions (lower urinary tract symptom)
Urinary system conditions encompass a range of symptoms and refer to certain types of functional disorders affecting the lower urinary tract, which are highly prevalent syndromes [5]. Physiotherapeutic methods, including KT, are recommended and recognized treatment approaches for urinary incontinence, but there have been very few studies in this area [6].
In a survey by Krajczy et al. which examined the effects of 4 days of KT in two groups (KT and placebo KT), of children with urinary incontinence, the study focused on the number of incontinence episodes and their mental state [6]. The frequency of incontinence episodes and the results of depression tests significantly reduced, demonstrating that KT had a positive impact on the patients’ mental health [6]. The mechanism behind this effect can be explained as follows: The reflex action from KT applications in the lower abdominal and sacral areas may enhance proprioception and help regulate the tone of the musculofascial bladder and urinary tract system 6. The limitations of this study was the lack of a quantitative assessment of incontinence, such as urine volume, as well as other factors, like somatic characteristics. Additionally, the lack of blinding in the Krajczy et al.’s study could introduce bias into the results in the intervention group [6].
In a study by Celenay et al. the effects of PFMT with KT (per Kenzo Kase’s KT method) 15 were assessed in women with overactive bladder (OAB) syndrome for 6 weeks [5]. In comparison to PFMT plus sham tape (ST), they found that PFMT plus KT was more effective in reducing OAB symptoms and the sense of urgency, as well as in improving PFM strength, bladder function, and quality of life. Additional improvements in the PFMT+KT group compared to the PFMT+ST group may be due to KT’s ability to regulate the tone of the musculofascial system in the area associated with the bladder reflex. Based on these findings, KT may be a viable additional treatment option for OAB symptoms [5]. However, the weaknesses of this study included the evaluation of only short-term effects of KT and the lack of blinding. Additionally, the current study did not include a urodynamic evaluation [5].
In a different study, Celenay et al. compared the effects of external electrical stimulation (ES) or Kenzo Kase’s KT method in addition to pelvic floor muscle exercise (PFME), with solitary PFME in three groups of women with OAB over a 6-week period using the same outcome measures as their earlier study [4]. They discovered that when combined with PFME, KT and ES were more successful than PFME alone at reducing OAB symptoms, improving quality of life, and creating a sense of improvement [4]. The control of myofascial tone may be the cause of these improved outcomes when KT is applied in the bladder reflex area. This trial, like the previous ones, did not assess the long-term effects of KT, blinding, or urodynamic assessment.
Incorporating KT, a simple, non-invasive, and safe technique, into the treatment regimens for patients with urinary system problems could enhance the effectiveness of the programs in alleviating related symptoms and improving quality of life by enhancing bladder tone and boosting proprioception through increased patients’ bladder awareness. However, we need more definitive evidence.
Effect of KT on defecatory system conditions
There is a lack of adequate research utilizing KT for bowel problems. Based on the studies conducted on the bowel dysfunctions in children, KT has been shown to have a positive effect on bowel symptoms, including constipation and bowel control [13].
In relation to constipation, the study by orhan focused on children with cerebral palsy (CP) and surveyed the impact of connective tissue manipulation (CTM) compared to two models of KT and a control group over 4 weeks [13]. This study showed that both CTM and KT are similarly effective approaches for managing pediatric constipation. The CTM and KT were found to have positive effects on defecation frequency (DF), duration, consistency, discomfort, strain and overall quality of life in CP children with chronic constipation [13]. The likely mechanisms of KT involve stimulating the reflex zone of the bowel, reducing abdominal bloating and discomfort and promoting bowel movements, through the application of KT to the abdominal area [13]. The robustness of this study include the utilization of reliable measurement tools to evaluate bowel symptoms and the application of the non-invasive intervention known as KT. However, the lack of a double-blind, placebo-controlled trial and the absence of long-term follow-up were limitations of this study [13].
In another study by Azam, the researcher examined the impact of combining lower abdominal KT, interferential (IF) ES, and routine traditional physiotherapy (PT), compared to a control group that received only routine traditional physiotherapy, over a period of 12 weeks. He found an enhancement in bowel control among children with meningomyelocele in the research group compared to the control group [12]. The assessment of DF per week, the use of the visual analog scale (VAS) to measure abdominal pain, and the constipation score system (CSS) to evaluate changes in bowel control all demonstrated significant improvement in the group that received KT plus IF plus PT [12]. Through the application of KT to the lower abdomen and sacral region, blood and lymph circulation in these areas improve, alongside the stimulation of cutaneous mechanoreceptors such as free nerve endings, Pacini corpuscles, and Ruffini endings within the fascia. This process provides the central nervous system (CNS) with data regarding pain and position. The activation of mechanoreceptors via KT results in a reduction in sympathetic nervous system activity and an elevation in parasympathetic activity, leading to better bowel control by increase intestinal tone and intestinal peristalsis movements [16]. However, there are insufficient studies about the effects of KT on defecatory system in the general population and high-quality methodology, making it difficult to draw definitive conclusions.
Effect of KT on pelvic girdle pain
In a related study organized by Mosaad et al. on the management of post-colonoscopy coccydynia, the researchers compared the effects of adding KT to conventional therapy (CT) with pelvic floor exercise (PFE) and CT in both groups. The study involved a 4-week training period. The results indicated that CT-KT demonstrated greater effectiveness than CT-PFE in decreasing pain linked to coccydynia following a colonoscopy. Nevertheless, there was no notable difference between their impacts on functional disability, as assessed by the oswestry disability index (ODI) [14].
Numerous studies have revealed that KT is effective in alleviating pain and enhancing functional ability [17-19]. KT is considered a highly effective technique to enhance blood and lymphatic circulation, restoring muscle tension, and realigning joints [20-22]. One proposed mechanism is that the application of KT provides cutaneous stretch stimulation, which leads to pain inhibition according to gait control theory [23]. Additionally, it is believed that the application of KT enhances afferent feedback, which may stimulate the neuromuscular pathways [24].
A possible explanation for the lack of improvement in functional disability following the use of KT and PFE may be insufficient treatment duration and inadequate loading of these modalities to promote the enhancement of patients’ functional abilities. Therefore, it is possible that a longer duration of treatment and higher loading will be necessary to improve the patients’ functional disabilities and ODI scores.
Outcomes of the three groups of the studies
Taking everything into account, KT has become one of the most commonly utilized physiotherapy methods. Nevertheless, to our current understanding, there are not many studies examining the effects of KT alone on pelvic floor conditions in the literature, and the existing studies are of moderate quality, producing inconsistent and ambiguous findings. Furthermore, it is challenging to compare, for instance, bowel and bladder dysfunctions, as well as differences between children and adults or men and women. Another factor that complicates these comparisons is that few studies evaluate the impact of KT application as a stand-alone technique in comparison to sham or placebo effects, and the majority of studies combine KT applications with other conservative treatment techniques. Limiting the reviewed sources to only English language articles, while excluding theses, presentations, and other types of publications, along with the inability to conduct a meta-analysis or calculate effect sizes due to the small number of studies and the diverse, scattered variables examined, were limitations of our review study.
To enhance the applicability of the findings, it is advised that future research with a sufficient sample size investigate additional parameters, such as the quantitative assessment of incontinence (urodynamic outcomes, such as urine volume) and other parameters, like the somatic characteristics (demographic and physical characteristics of subjects) [6]. It appears that identifying traits that are beneficial for treatment may be possible by examining these additional factors. Additionally, studies that explore the durability and long-term outcomes of KT on patients with various pelvic floor issues are needed.
Conclusion
According to the limited research currently available, KT, whether used alone or in conjunction with other conservative therapy approaches, may benefit individuals with pelvic floor dysfunctions both physically and psychologically. The incorporation of KT, a straightforward, non-invasive, safe, and effective adjunctive technique, may improve pelvic floor symptoms and enhance the quality of life for patients with pelvic floor dysfunction. Therefore, KT could be considered a complementary therapy for urinary incontinence and defecatory disorders; however, further high-quality RCTs with standardized protocols and larger, multi-center studies are needed.
Ethical Considerations
Compliance with ethical guidelines
There were no ethical considerations to be considered in this research.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Software and supervision: Vahid Delshad; Methodology, resources, data collection, project administration and visualization: Somayeh Mohamadi and Sahar Boozari and Vahid Delshad; Conceptualization, validation, investigation, review & Editing: All authors.
Conflict of interest
The authors declared no conflict of interest.
References
Pelvic floor dysfunctions are highly common clinical problems, encompassing a wide variety of disorders [1]. In addition to pelvic organ prolapse, these dysfunctions include defecatory and sexual system issues, lower urinary tract sensory and emptying abnormalities, intestinal and urinary incontinence, and several chronic pain syndromes [1, 2]. These conditions significantly influence the quality of life, especially in the female population [1, 2].
Pelvic floor physiotherapy is regarded as a primary, low-risk, minimally invasive therapy for both the management and prevention of pelvic floor dysfunctions [3, 4]. It includes pelvic floor muscle training (PFMT), electrical impulse therapy, magnetotherapy, manual therapy, laser therapy, acupuncture, behavioral therapy (bowel and bladder training), biofeedback, and kinesio taping (KT) [4-6]. However, studies using KT as a simple, safe, non-invasive and inexpensive modality for pelvic floor conditions are insufficient, and its effects in different conditions are not well understood [4].
The lower urinary tract’s sensory and emptying problems, along with issues in the defecatory and sexual systems, pelvic organ prolapse, and urinary and bowel incontinence, can have several possible causes for these conditions. One explanation for the effectiveness of KT is the reduction of compression caused by lifting the skin, fascia, and subcutaneous tissues, which increases blood and lymph circulation and, in turn, reduces inflammation and pain related to chronic pain syndromes [4, 7, 8]. Other possible mechanisms include fascial correction, which may lead to an increase in the range of motion, improvement in neuromuscular control, and enhanced joint positioning through mechanoreceptor stimulation and kinesthetic awareness [5, 7, 8]. Also, KT can facilitate or inhibit muscle activity and help in injury prevention [7]. Additionally, various studies suggest that KT application may activate the cutaneous-visceral reflex mechanism associated with Head’s zones [4-6].
Despite contradictory data regarding KT efficacy in treating various ailments and among healthy individuals, KT remains a common and widely utilized physiotherapy technique [5, 9]. This is due to the results of limited studies suggesting that KT can be clinically beneficial [7]. However, collecting and reviewing the results of valid studies in this area can still pave the way for clinical practice and future research. Therefore, despite the potential positive effects of kinesiotaping on pelvic floor dysfunctions, research on this topic is limited and unclear. This study sought to explore the effects of KT on the management of pelvic floor dysfunction, evaluating a range of outcomes in comparison to sham or certain conservative non-KT therapies. Summarizing and analyzing strong and credible studies in this field can create opportunities for future research to conduct more comprehensive and accurate studies.
Materials and Methods
Search strategy
The standards of the preferred reporting items for systematic reviews and meta-analysis (PRISMA) served as the foundation for our search approach [10]. Articles were included that examined the effects of KT alone or combination with other treatment modalities for different pelvic floor dysfunctions. Accessible databases comprising PubMed, Scopus, ScienceDirect, Medline and Web of Science were searched from the earliest records up to March 2024. the Following syntaxes were used to search relevant articles: (Kinesio-taping OR kinesio tape OR kinesiology taping) AND (pelvic floor physiotherapy OR pelvic floor physical therapy OR pelvic floor treatment OR nonpharmacological pelvic floor treatment OR pelvic floor conservative treatment) AND (pelvic floor dysfunction OR pelvic floor disorder OR vaginal dysfunction OR anal dysfunction OR urethral dysfunction OR urinary incontinence OR anal incontinence OR urge incontinence OR stress incontinence OR overactive bladder OR constipation OR sexual dysfunction OR vaginismus OR pelvic floor dyssynergia OR erectile dysfunction OR pelvic organ prolapse OR defecatory dysfunction OR voiding dysfunction OR chronic pelvic pain syndrome). We searched each of the words within each set of parentheses (a total of three sets of parentheses) that were separated by “OR” with each of the words in the next two sets of parentheses, which were separated by “AND,” using the “plus sign.” This way, with each search, we included three words or phrases, and thus we found all relevant articles (e.g. KT+pelvic floor physiotherapy+pelvic floor dysfunction).
Eligibility criteria for study selection
First, two independent authors (Somayeh Mohamadi and Sahar Boozari) considered the eligibility of the obtained studies by their titles and abstracts to identify which one can be included for peer review. The population, intervention, comparison, outcomes, and study design (PICOS) criteria were used to assess whether a study was eligible. In the present systematic review, the PICOS criteria were as follows: P: Patients with pelvic floor dysfunctions; I: KT; C: Comparison with other conservative treatment modalities; O: Improvements in quality of life, pelvic floor muscle (PFM) strength, bowel and bladder symptoms, discomfort, disability, and other aspects; S: Controlled clinical trials that are randomized.
The two researchers reviewed full-text papers if titles or abstracts did not contain sufficient information for eligibility. Duplicates were eliminated, and if the two investigators could not agree on the eligibility of any included studies, a third investigator (VD) made the final decision based on the precise inclusion and exclusion criteria, results, and research design (PICOS). In the current study, the inclusion criteria were as follows: 1) the papers should compare KT with sham KT or other conservative treatment modalities; 2) the studies should investigate pelvic floor dysfunctions; 3) the studies should report any parameters related to improvement in the pelvic symptoms (pain, PFM performance disability, bowel and bladder symptoms, quality of life, etc.); 4) only RCTs; and 5) full-text original articles were published in the English language. Articles published in other languages, articles published or presented at conferences, seminars, or theses, and research published in abstract form were excluded from the study.
Quality assessment
Studies included in the current systematic review were evaluated using the critical appraisal skills program (CASP) checklist for clinical trial studies in terms of methodological quality [11]. This checklist consisted of 11 questions for RTCs, organized into four sections. Section A comprises three questions addressing whether “the study design is appropriate for a randomized clinical trial.” Section B includes three questions assessing whether “the study is methodologically sound.” Section C comprises three questions focused on “what the results are.” Finally, Section D contains two questions that inquire whether “the results are locally applicable.” The questions can be answered with “yes”, “no”, or “can’t say”. All studies were scored by the same two independent investigators that assessed the eligibility of the studies. If any disagreement arose regarding the answers to questions in each article, the two investigators discussed the differences to reach a final decision. If the disagreement could not be resolved, a third researcher was involved in the discussion panel to achieve consensus. The final agreement was reached based on the majority opinion.
Data extraction
Information from all included studies was extracted and summarized in the form of a table, which includes the authors and year of publication, study design, diagnosis, participants’ characteristics (group type and sample size), outcome measures (pelvic pain, PFM strength, questionnaires, voiding diaries), and main results.
Results
A total of 1545 possible articles were discovered in the initial search using the databases listed in the search strategy. Once duplicates were eliminated, 986 records were left. After screening the title, abstract, and full text, if required, in accordance with the inclusion and exclusion criteria, only 27 articles were deemed acceptable. Nine studies were found to be eligible after applying the CASP checklist. Ultimately, six studies were chosen for examination after receiving moderate to high-quality ratings. A flow chart of PRISMA 10 is displayed in Figure 1.
Results of the included studies
A summary of the relevant articles is presented in Table 1. Of the six studies, urinary system conditions were investigated in three studies 4-6, defecatory conditions were assessed in three studies [12, 13], and coccydynia was assessed in one study [14]. Due to the scattered and inconsistent outcome measures in the studies, it was not possible to calculate the effect size or conduct a meta-analysis.
Quality assessment
All of the featured articles had an average quality rated as moderate to high. Table 2 provides a summary of the CASP findings. High applicability was demonstrated by the included RTCs.
Discussion
This systematic review was conducted on previous studies that investigated the improvement of pelvic floor dysfunction with KT compared to other conservative treatment modalities using different outcome measures. KT, when combined with other conservative treatments, showed better therapeutic results for pelvic floor dysfunctions. Regarding the findings of the reviewed studies, most studies reported positive outcomes with KT; however, methodological limitations and inconsistent results warrant caution.
Outcome measures among the three groups of the studies based on the affected system
Effect of KT on urinary system conditions (lower urinary tract symptom)
Urinary system conditions encompass a range of symptoms and refer to certain types of functional disorders affecting the lower urinary tract, which are highly prevalent syndromes [5]. Physiotherapeutic methods, including KT, are recommended and recognized treatment approaches for urinary incontinence, but there have been very few studies in this area [6].
In a survey by Krajczy et al. which examined the effects of 4 days of KT in two groups (KT and placebo KT), of children with urinary incontinence, the study focused on the number of incontinence episodes and their mental state [6]. The frequency of incontinence episodes and the results of depression tests significantly reduced, demonstrating that KT had a positive impact on the patients’ mental health [6]. The mechanism behind this effect can be explained as follows: The reflex action from KT applications in the lower abdominal and sacral areas may enhance proprioception and help regulate the tone of the musculofascial bladder and urinary tract system 6. The limitations of this study was the lack of a quantitative assessment of incontinence, such as urine volume, as well as other factors, like somatic characteristics. Additionally, the lack of blinding in the Krajczy et al.’s study could introduce bias into the results in the intervention group [6].
In a study by Celenay et al. the effects of PFMT with KT (per Kenzo Kase’s KT method) 15 were assessed in women with overactive bladder (OAB) syndrome for 6 weeks [5]. In comparison to PFMT plus sham tape (ST), they found that PFMT plus KT was more effective in reducing OAB symptoms and the sense of urgency, as well as in improving PFM strength, bladder function, and quality of life. Additional improvements in the PFMT+KT group compared to the PFMT+ST group may be due to KT’s ability to regulate the tone of the musculofascial system in the area associated with the bladder reflex. Based on these findings, KT may be a viable additional treatment option for OAB symptoms [5]. However, the weaknesses of this study included the evaluation of only short-term effects of KT and the lack of blinding. Additionally, the current study did not include a urodynamic evaluation [5].
In a different study, Celenay et al. compared the effects of external electrical stimulation (ES) or Kenzo Kase’s KT method in addition to pelvic floor muscle exercise (PFME), with solitary PFME in three groups of women with OAB over a 6-week period using the same outcome measures as their earlier study [4]. They discovered that when combined with PFME, KT and ES were more successful than PFME alone at reducing OAB symptoms, improving quality of life, and creating a sense of improvement [4]. The control of myofascial tone may be the cause of these improved outcomes when KT is applied in the bladder reflex area. This trial, like the previous ones, did not assess the long-term effects of KT, blinding, or urodynamic assessment.
Incorporating KT, a simple, non-invasive, and safe technique, into the treatment regimens for patients with urinary system problems could enhance the effectiveness of the programs in alleviating related symptoms and improving quality of life by enhancing bladder tone and boosting proprioception through increased patients’ bladder awareness. However, we need more definitive evidence.
Effect of KT on defecatory system conditions
There is a lack of adequate research utilizing KT for bowel problems. Based on the studies conducted on the bowel dysfunctions in children, KT has been shown to have a positive effect on bowel symptoms, including constipation and bowel control [13].
In relation to constipation, the study by orhan focused on children with cerebral palsy (CP) and surveyed the impact of connective tissue manipulation (CTM) compared to two models of KT and a control group over 4 weeks [13]. This study showed that both CTM and KT are similarly effective approaches for managing pediatric constipation. The CTM and KT were found to have positive effects on defecation frequency (DF), duration, consistency, discomfort, strain and overall quality of life in CP children with chronic constipation [13]. The likely mechanisms of KT involve stimulating the reflex zone of the bowel, reducing abdominal bloating and discomfort and promoting bowel movements, through the application of KT to the abdominal area [13]. The robustness of this study include the utilization of reliable measurement tools to evaluate bowel symptoms and the application of the non-invasive intervention known as KT. However, the lack of a double-blind, placebo-controlled trial and the absence of long-term follow-up were limitations of this study [13].
In another study by Azam, the researcher examined the impact of combining lower abdominal KT, interferential (IF) ES, and routine traditional physiotherapy (PT), compared to a control group that received only routine traditional physiotherapy, over a period of 12 weeks. He found an enhancement in bowel control among children with meningomyelocele in the research group compared to the control group [12]. The assessment of DF per week, the use of the visual analog scale (VAS) to measure abdominal pain, and the constipation score system (CSS) to evaluate changes in bowel control all demonstrated significant improvement in the group that received KT plus IF plus PT [12]. Through the application of KT to the lower abdomen and sacral region, blood and lymph circulation in these areas improve, alongside the stimulation of cutaneous mechanoreceptors such as free nerve endings, Pacini corpuscles, and Ruffini endings within the fascia. This process provides the central nervous system (CNS) with data regarding pain and position. The activation of mechanoreceptors via KT results in a reduction in sympathetic nervous system activity and an elevation in parasympathetic activity, leading to better bowel control by increase intestinal tone and intestinal peristalsis movements [16]. However, there are insufficient studies about the effects of KT on defecatory system in the general population and high-quality methodology, making it difficult to draw definitive conclusions.
Effect of KT on pelvic girdle pain
In a related study organized by Mosaad et al. on the management of post-colonoscopy coccydynia, the researchers compared the effects of adding KT to conventional therapy (CT) with pelvic floor exercise (PFE) and CT in both groups. The study involved a 4-week training period. The results indicated that CT-KT demonstrated greater effectiveness than CT-PFE in decreasing pain linked to coccydynia following a colonoscopy. Nevertheless, there was no notable difference between their impacts on functional disability, as assessed by the oswestry disability index (ODI) [14].
Numerous studies have revealed that KT is effective in alleviating pain and enhancing functional ability [17-19]. KT is considered a highly effective technique to enhance blood and lymphatic circulation, restoring muscle tension, and realigning joints [20-22]. One proposed mechanism is that the application of KT provides cutaneous stretch stimulation, which leads to pain inhibition according to gait control theory [23]. Additionally, it is believed that the application of KT enhances afferent feedback, which may stimulate the neuromuscular pathways [24].
A possible explanation for the lack of improvement in functional disability following the use of KT and PFE may be insufficient treatment duration and inadequate loading of these modalities to promote the enhancement of patients’ functional abilities. Therefore, it is possible that a longer duration of treatment and higher loading will be necessary to improve the patients’ functional disabilities and ODI scores.
Outcomes of the three groups of the studies
Taking everything into account, KT has become one of the most commonly utilized physiotherapy methods. Nevertheless, to our current understanding, there are not many studies examining the effects of KT alone on pelvic floor conditions in the literature, and the existing studies are of moderate quality, producing inconsistent and ambiguous findings. Furthermore, it is challenging to compare, for instance, bowel and bladder dysfunctions, as well as differences between children and adults or men and women. Another factor that complicates these comparisons is that few studies evaluate the impact of KT application as a stand-alone technique in comparison to sham or placebo effects, and the majority of studies combine KT applications with other conservative treatment techniques. Limiting the reviewed sources to only English language articles, while excluding theses, presentations, and other types of publications, along with the inability to conduct a meta-analysis or calculate effect sizes due to the small number of studies and the diverse, scattered variables examined, were limitations of our review study.
To enhance the applicability of the findings, it is advised that future research with a sufficient sample size investigate additional parameters, such as the quantitative assessment of incontinence (urodynamic outcomes, such as urine volume) and other parameters, like the somatic characteristics (demographic and physical characteristics of subjects) [6]. It appears that identifying traits that are beneficial for treatment may be possible by examining these additional factors. Additionally, studies that explore the durability and long-term outcomes of KT on patients with various pelvic floor issues are needed.
Conclusion
According to the limited research currently available, KT, whether used alone or in conjunction with other conservative therapy approaches, may benefit individuals with pelvic floor dysfunctions both physically and psychologically. The incorporation of KT, a straightforward, non-invasive, safe, and effective adjunctive technique, may improve pelvic floor symptoms and enhance the quality of life for patients with pelvic floor dysfunction. Therefore, KT could be considered a complementary therapy for urinary incontinence and defecatory disorders; however, further high-quality RCTs with standardized protocols and larger, multi-center studies are needed.
Ethical Considerations
Compliance with ethical guidelines
There were no ethical considerations to be considered in this research.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Software and supervision: Vahid Delshad; Methodology, resources, data collection, project administration and visualization: Somayeh Mohamadi and Sahar Boozari and Vahid Delshad; Conceptualization, validation, investigation, review & Editing: All authors.
Conflict of interest
The authors declared no conflict of interest.
References
- Bump RC, Norton PA. Epidemiology and natural history of pelvic floor dysfunction. Obstetrics and Gynecology Clinics of North America. 1998; 25(4):723-46. [DOI:10.1016/S0889-8545(05)70039-5] [PMID]
- Iacobellis F, Reginelli A, Berritto D, Gagliardi G, Laporta A, Brillantino A, et al. Pelvic foor dysfunctions: How to image patients? Japanese Journal of Radiology. 2020; 38(1):47-63.[DOI:10.1007/s11604-019-00903-6] [PMID]
- Wallacea LS, Millerb LD, Mishraa K. Pelvic floor physical therapy in the treatment of pelvic floor dysfunction in women. Current Opinion in Obstetrics & Gynecology. 2019; 31(6):485-93. [DOI:10.1097/GCO.0000000000000584] [PMID]
- Celenay ST, Karaaslan Y, Coban O, Oskay K. A comparison of Kinesio taping and external electrical stimulation in addition to pelvic floor muscle exercise and sole pelvic floor muscle exercise in women with overactive bladder: A randomized controlled study. Disability and Rehabilitation. 2022; 44(18):5124-32. [DOI:10.1080/09638288.2021.1925751] [PMID]
- Celenay ST, Korkut Z, Oskay K, Aydin A. The effects of pelvic floor muscle training combined with Kinesio taping on bladder symptoms, pelvic floor muscle strength, and quality of life in women with overactive bladder syndrome: A randomized sham-controlled trial. Physiotherapy Theory and Practice. 2022; 38(2):266-75. [DOI:10.1080/09593985.2020.1750079] [PMID]
- Krajczy M, Luniewski J, Bogacz K, Szczegielniak J. Evaluation of applying Kinesio taping in children with urinary incontinence. Journal of Pediatric Urology. 2018; 14(6):550.e1-550.e6. [DOI:10.1016/j.jpurol.2018.06.013] [PMID]
- Morris D, Jones D, Ryan H, Ryan CG. The clinical effects of Kinesio® Tex taping: A systematic review. Physiotherapy Theory and Practice. 2012; 29(4):259-70. [DOI:10.3109/09593985.2012.731675] [PMID]
- Krajczy M, Bogacz K, Luniewski J, Szczegielniak J. The influence of kinesio taping on the effects of physiotherapy in patients after laparoscopic cholecystectomy. The Scientific World Journal. 2012; 2012:948282. [DOI:10.1100/2012/948282] [PMID]
- Alexander CM, Stynes S, Thomas A, Lewis J, Harrison PJ. Does tape facilitate or inhibit the lower fibres of trapezius? Manual Therapy 2003; 8(1):37-41. [DOI:10.1054/math.2002.0485] [PMID]
- Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred reporting items for systematic review and meta-analysis protocols (prisma-p) 2015 statement. Systematic Reviews. 2015; 4(1):1-9. [DOI:10.1186/2046-4053-4-1]
- Naidoo N, Nguyen VT, Ravaud P, Young B, Amiel P, Schanté D, et al. The research burden of randomized controlled trial participation: A systematic thematic synthesis of qualitative evidence. BMC Medicine. 2020; 18(1):6 [DOI:10.1186/s12916-019-1476-5] [PMID]
- Azam AM. Effcacy of lower abdominal kinesio taping plus interferential electrical stimulation techniques in the improvement of bowel control in meningomyelocele children. Journal of Pediatrics and Neonatal Care. 2017; 7(4):00298. [Link]
- Orhan C, Kaya Kara O, Kaya S, Akbayrak T, Kerem Gunel M, Baltaci G. The effects of connective tissue manipulation and Kinesio Taping on chronic constipation in children with cerebral palsy: A randomized controlled trial. Disability and Rehabilitation. 2018; 40(1):10-20. [DOI:10.1080/09638288.2016.1236412] [PMID]
- Mosaad EH, Mohamed AY, Fawzy AA, Mohamed MH. The effect of adding kinesiotaping versus pelvic floor exercise to conventional therapy in the management of post-colonoscopy coccydynia: A single-blind randomized controlled trial. African Health Sciences. 2023; 23(1):575-83. [DOI:10.4314/ahs.v23i1.60] [PMID]
- Kase K, Wallis J, Kase T. Clinical therapeutic applications of the Kinesio taping method. Dallas: Kinesio Taping Association; 2003. [Link]
- Callaghan MJ, Selfe J, Bagley PJ, Oldham JA. The effects of patellar taping on knee joint proprioception. Journal of Athletic Training. 2002; 37(1):19-24. [PMID]
- Yoshida A, Kahanov L. Effect of Kinesio taping on lower trunk range of motions. Research in Sports Medicine (Print). 2007; 15(2):103-12. [DOI:10.1080/15438620701405206] [PMID]
- Dawood RS, Kattabei OM, Nasef SA, Battarjee KA, Abdelraouf OR. Effectiveness of Kinesio taping versus cervical traction on mechanical neck dysfunction. International Journal of Therapies and Rehabilitation Research. 2013; 2(2):1-2. [Link]
- Abdel-Aal NM, Elgohary HM, Soliman ES, Waked IS. Effects of kinesiotaping and exercise program on patients with obesity-induced coccydynia: A randomized, double-blinded, sham-controlled clinical trial Clinical Rehabilitation. 2020; 34(4):471-9. [DOI:10.1177/0269215519897414] [PMID]
- Lee JH, Yoo WG. Application of posterior pelvic tilt taping for the treatment of chronic low back pain with sacroiliac joint dysfunction and increased sacral horizontal angle. Physical Therapy in Sport. 2012; 13(4):279-85. [DOI:10.1016/j.ptsp.2011.10.003] [PMID]
- Hsu YH, Chen WY, Lin HC, Wang WT, Shih YF. The effects of taping on scapular kinematics and muscle performance in baseball players with shoulder impingement syndrome. Journal of Electromyography and Kinesiology. 2009; 19(6):1092-9. [DOI:10.1016/j.jelekin.2008.11.003] [PMID]
- Lee MH, Lee CR, Park JS, Lee SY, Jeong TG, Son GS, et al. Influence of kinesiotaping on the motor neuron conduction velocity. Journal of Physical Therapy Science. 2011; 23(2):313-5. [DOI:10.1589/jpts.23.313]
- Paoloni M, Bernetti A, Fratocchi G, Mangone M, Parrinello L, Del Pilar Cooper M, et al. Kinesio Taping applied to lumbar muscles influences clinical and electromyographic characteristics in chronic low back pain patients. European Journal of Physical And Rehabilitation Medicine. 2011; 47(2):237-43. [Link]
- Kase K. Clinical therapeutic applications of the Kinesio taping method. Tokyo, Japan: Ken Ikai; 2003. [Link]
Type of Study: Systematic Review |
Subject:
Sport injury and corrective exercises
Received: 2024/12/1 | Accepted: 2025/01/4 | Published: 2026/01/1
Received: 2024/12/1 | Accepted: 2025/01/4 | Published: 2026/01/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
