Thu, May 28, 2026
Volume 15, Issue 1 (Winter 2025)
PTJ 2025, 15(1): 69-80 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Estiri Z, Salehi kalateh M S, Shahabi Kaseb M R, khademosharie M, Tayebi S M. The Effect of Six-weeks of Pilates Training With Music on Balance and the Quality of Life in Multiple Sclerosis Patients. PTJ 2025; 15 (1) :69-80
URL: http://ptj.uswr.ac.ir/article-1-644-en.html
URL: http://ptj.uswr.ac.ir/article-1-644-en.html
Zahra Estiri *1 

 , Maryam sadat Salehi kalateh1 , Mohammad Reza Shahabi Kaseb1 , Mitra Khademosharie2 , Seyed Morteza Tayebi3
, Maryam sadat Salehi kalateh1 , Mohammad Reza Shahabi Kaseb1 , Mitra Khademosharie2 , Seyed Morteza Tayebi3
, Maryam sadat Salehi kalateh1 , Mohammad Reza Shahabi Kaseb1 , Mitra Khademosharie2 , Seyed Morteza Tayebi3
1- Department of Motor Behavior, Faculty of Sport Sciences, Hakim Sabzevari University, Sabzevar, Iran.
2- Department of Sport Sciences, Faculty of Humanities, Kosar University of Bojnord, Bojnord, Iran.
3- Department of Exercise Physiology, Faculty of Physical Education and Sports Sciences, Allameh Tabataba’i University, Tehran, Iran.
2- Department of Sport Sciences, Faculty of Humanities, Kosar University of Bojnord, Bojnord, Iran.
3- Department of Exercise Physiology, Faculty of Physical Education and Sports Sciences, Allameh Tabataba’i University, Tehran, Iran.
Full-Text [PDF 563 kb]
(685 Downloads)
| Abstract (HTML) (3155 Views)
Full-Text: (901 Views)
Introduction
Multiple sclerosis (MS) is an immune system-mediated demyelinating disease, resulting in physical, cognitive, and depressive symptoms in twice as many women as men aged 20-50 years [1]. Previous studies indicated that about 11 to 15 persons in 1000 have MS. Based on the World Health Organization (WHO) studies, this ratio is 4 to 5 persons among 10000 in Iran [2].
The disease’s occurrence in youth increases social and economic problems for the patient, their family, and the community [3]. These patients’ weakness of limbs, fatigue, and motor disorders affect their function. In addition, 85% of MS patients experience motor problems [4]. Balance is considered to maintain optimal body posture in static and dynamic positions and is a criterion for the whole body’s function. Additionally, the sensory information obtained from somatosensory (proprioception), vestibular, and visual systems affects balance maintenance [5]. The presence of dynamic balance in a person is one of the critical factors of triumphant gait, and most MS patients consider imbalance as the most challenging symptom of the disease, which is regarded as the initial cause of disorder in going and falling [6]. Around 20% of these falls may lead to newer problems such as fracture and infection, and motor restrictions in patients [7].
Furthermore, the quality of life in these patients is considered less and is influenced negatively by motor disorders and fatigue, according to previous studies [8, 9]. Mental and physical issues affect the quality of life of the person. They are considered as the factor limiting physical activity, which results in depending on person to others and an indirect increase in the severity of the disease in these people [10].
Despite the advancements in medical science in recent years, there is currently no definitive and eradicating therapy for MS disease, and most of the current therapeutic approaches result in decreasing symptoms or disease processes [11, 12]. In this regard, sports can be applied as complementary therapies, along with pharmaceutical approaches [12]. Considering the lack of definitive treatment using new medicines and their high costs and side effects, non-pharmacological approaches can be practical and accepted by patients easily [13]. Appropriate and particular exercise and physical activity for this group of patients can probably be effective in advancing their motor and cognitive capabilities. The usefulness of regular exercises for these patients was specified well [13-15]. Most of the exercise therapy studies focus on exercise in water, plyometric exercises, and aerobic and strength exercises or a combination of both while implementing various exercises, such as yoga, tai chi, and Pilates used as complementary therapy in exercise therapy, among utilizing mind and body [16].
Using the Pilates exercise method challenges the sensory, skeletal, nervous and muscular systems required for dynamic balance [17]. It helps develop trunk muscles and restore muscle balance by strengthening, stretching, and breathing. Additionally, Pilates exercises result in increasing physical function (flexibility, muscular strength, endurance, power and cardiorespiratory fitness) and motor control (control of trunk, static and dynamic stability and beauty of movement) [18]. Limited studies were conducted on the effect of these exercises on MS patients by representing the effectiveness of Pilates exercises on physical and cognitive factors. Guclu-Gunduz et al. (2014) found that eight weeks of Pilates exercises improved the muscular strength of lower and upper limbs, mobility, and balance in MS patients in the experimental group compared to the control group [19]. Based on the results of another study, 12 weeks of Pilates significantly increases dynamic balance in female MS patients, similar to exercises in water [20]. Abasıyanık et al. showed that eight weeks of Pilates exercises were superior to the home exercise program in walking endurance, postural stability, core stability, respiratory, and cognitive functions [21]. People suffering from this disease are facing many problems that limit the patients’ participation in health promotion activities and, as a result, increase secondary complications and limit their independent lives, which ultimately harms their quality of life. Physical, psychological, social, and economic dimensions of quality of life undergo many changes in chronic diseases [22].
In addition to Pilates exercises, music is one of the most effective tools for increasing concentration and attention. Listening to music can improve self-control, physical movements, movement balance, and bodily states [23]. In a study, researchers reported positive effects of music on the acquisition of balance in people with Parkinson’s disease [24]. In another study, researchers investigated the effect of the focus of attention and the combination of focus and music on static and dynamic balance learning in attention deficit hyperactivity disorder (ADHD) children. They concluded that using instructions and music affects the balance performance of these children and improves their balance scores [25].
Due to limited studies in this area [19-21, 26] and considering the studies conducted on Pilates exercises, assessment of using music, and effects of these exercises on body and mind, the present study compares the effect of Pilates exercises with and without music on balance function and the quality of life in MS patients. Based on the previous studies, this question is proposed whether using music, along with Pilates exercises, can affect the amount of balance (motor skill) and quality of life in participants as a positive factor or may influence negatively or fail to affect the balance of MS patients as considerable over-load.
Materials and Methods
Data collection method
Female volunteers were invited and registered to participate in the present study by referring to the MS association in Sabzevar City, Iran. After recalling and inviting participation by the confirmation of specialist physicians, 29 female patients aged 20-50 years were selected through convenient sampling. The inclusion criteria of the present study were the expanded disability status scale (EDSS) between 2-5, which specialist physicians determined through conducting examinations related to the diagnosis of MS disease, such as magnetic resonance imaging or computed tomography scan and the functional tests related to balance, strength, gait capability, and vision and tactile testing (to the extent that patients can do exercises), age range of 20-50 years, regular menstrual cycle, absence of other diseases (heart problems, diabetes, epilepsy and other particular problems that limited the implementation of exercises), non-participation in regular sports program and consumption of almost similar medicine.
After the early registration of participants, a dating meeting was held to introduce the study’s overall design, nutrition program, and pharmaceutical program, as well as to conduct cardiovascular-respiratory tests for entering the study and completing the consent form. Further, the initial anthropometric and demographic data, including age, height, weight and the percentage of subcutaneous fat, were recorded.
The patients were divided into experimental and control groups based on leg muscles’ strength homogenization. Leg muscles’ strength was measured using a dynamometer. Regarding the first day, tests and the exercise process were explained to the participants in each group. Further, all participants were pre-tested using a stabilimeter and dynamic balance test and they completed the quality-of-life questionnaire. Furthermore, they were homogenized based on the early strength test and randomly divided into three groups: Two experimental groups (n=10 in each group) and a control group (n=9). Then, the participants were post-tested using the mentioned tool after six weeks.
Measurement of demographic data and disability index
The height and weight of participants were determined by using a tape measure (Komelon [South Korea] Company with 1/16th of an inch or 1-mm sensitivity) on the wall and a digital scale (Etekcity [China] Company with 0.1 pounds (~0.05 kg) sensitivity), respectively.
Body composition
The body fat percentage and waist-to-hip ratio related to participants were measured using a body composition analyzer (In Body 3.0, South Korea). To this end, all participants were asked to refer to the laboratory of physical education in the university as overnight fasting. After turning the device on, the participants were requested to drain the bladder using wipes to humidify their feet and foothold on the device. Then, they should go on a foothold, take handles, and keep them until the charts of the device end after entering the required data by the tester. Finally, the obtained data were printed and used [27].
Expanded disability status scale
EDSS measures the severity of physical, neurological, and muscular disability in MS patients. The scores of the scale range from 0 to 10, in which 0 and 10 represent the lack of physical disorder in the field of systems function and very severe disability, respectively [28]. The patients with the maximum score of five were selected in the present study.
Static balance
Static balance was assessed using a stabilimeter (Iranian Danesh Salar Company). This device measures and analyzes body oscillations indirectly based on the reaction of static level to the forces caused by changing the center of gravity in person. The data related to body movement are used in different parameters two-dimensionally during standing with open and closed eyes as instantaneously and visually. This instrument’s minimum acceptable reliability and validity is 0.70, and its maximum acceptable reliability is 0.90 [29]. Regarding the method of measuring static and dynamic balance, the prerequisites for testing, including calibrating the device and providing required explanations about the overall testing process to each participant, were conducted after turning on the stabilimeter. Then, each patient went on the device for 30 s with his dominant leg as bare leg and looked at a specific point mounted on the wall by considering his height. Since each head movement displaces the center of gravity, a specific point is considered to prevent his eye movements from affecting his surroundings [30]. The mean of rate changes in the body movement of participants obtained by averaging diversion in four directions was used in the present study.
Balance test of timed up and go
Dynamic balance was evaluated using timed up and go (TUG). Considering the test’s method, the participant should get up from a seat and handle-less without using his hands, return, and sit on their seat after crossing an eight-foot path (2.44 m). Regarding the present study, the participants were asked to do this activity with more speed and skill without running, and finally, overall time was recorded as their score. Due to the unfamiliarity of participants with the method of performing the test, they trained the test three times before recording the tests. Then, each of them conducted the test thrice and the meantime (s) were recorded as their score [31].
The dynamometer (HBM test and measurement [Hottinger Brüel & Kjaer GmbH], Germany) was applied for assessing to assess the strength of leg muscles and early homogenization of groups [32].
Music
Classical instrumental music with moderate intensity, confirmed by the Pilates association, was used in the present exercise program. These types of music give extraordinary relaxation to the athlete during the exercise and cause the pressure on the heart to decrease during the exercise. Also, the one engaged in Pilates eliminates all the mental preoccupations and turns this exercise into a meditation.
Quality of life
The quality of life was assessed by using a standard questionnaire containing 36 questions in the eight scales of public health (n=5), physical function (n=10), emotional health (n=5), physical pain (n=2), energy and happiness (n=4), social function (n=2), and the role of physical and mental health in limiting activities (4 and 3 questions, respectively). Regarding the calculation of responding to the questionnaire questions, the responses were first scored from 1 to 5 based on the Likert scale, where scores 1 and 5 represent the terrible and great status of participants, respectively. Then, the scores were converted into eight components ranging between 0 to 100. Finally, the mean sum of cases was calculated as the score of the intended scale regarding the quality of life, and the higher scores indicate a better quality of life [33].
Exercise program
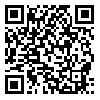
The exercise program was implemented for six weeks under the supervision of an exercise physiologist and 60-min sessions were held each week. The first experimental group performed Pilates exercises for six weeks. each week, three 60-min sessions were conducted under the supervision of a Pilates instructor in the morning. each exercise session was divided into three parts: Warming up (10-15 min), doing Pilates exercises (35-40 min) and cooling down (10 min) (Table 1).
The exercise were started by simple movements and then their intensity and complexity increased and then their intensity and complexity increased.
Further, the range of stretching, time and repetition of movements gradually increased with the participants’ progress and new exercises were added to each session compared to the previous session. The speed of progressing exercises related to all participants was at the same level. Further, they were recommended to do exercises as long as they did not feel pain and discomfort. The training intensity was determined using the Borg scale, in the first sessions between 4-5, in the next sessions 6-7 and in the last sessions 8-9. Furthermore, exercises were conducted in the sleeping position first, then sitting and standing [31]. Most exercises focused on the downer limb, and a 30-s rest period with inhaling and exhaling between movements was considered (Table 1). The second experimental group implemented these exercises with the music confirmed by the Pilates association. Finally, the patients in the control group only did their daily activities during the exercise course. Table 1 represents an example of a session of the Pilates exercise program.
Statistical analysis
Descriptive statistics were used to summarize collected information and recognize the community more so that the data could be analyzed. Further, statistical hypotheses were tested using inferential statistics, and data distribution was estimated to be normal based on Kolmogorov-Smirnov and the Levene tests. Analysis of covariance and Fisher least significant difference post hoc test were used to compare groups and specify their difference. The calculations were conducted using the SPSS software, version 22 and the significance level was P<0.05.
Results
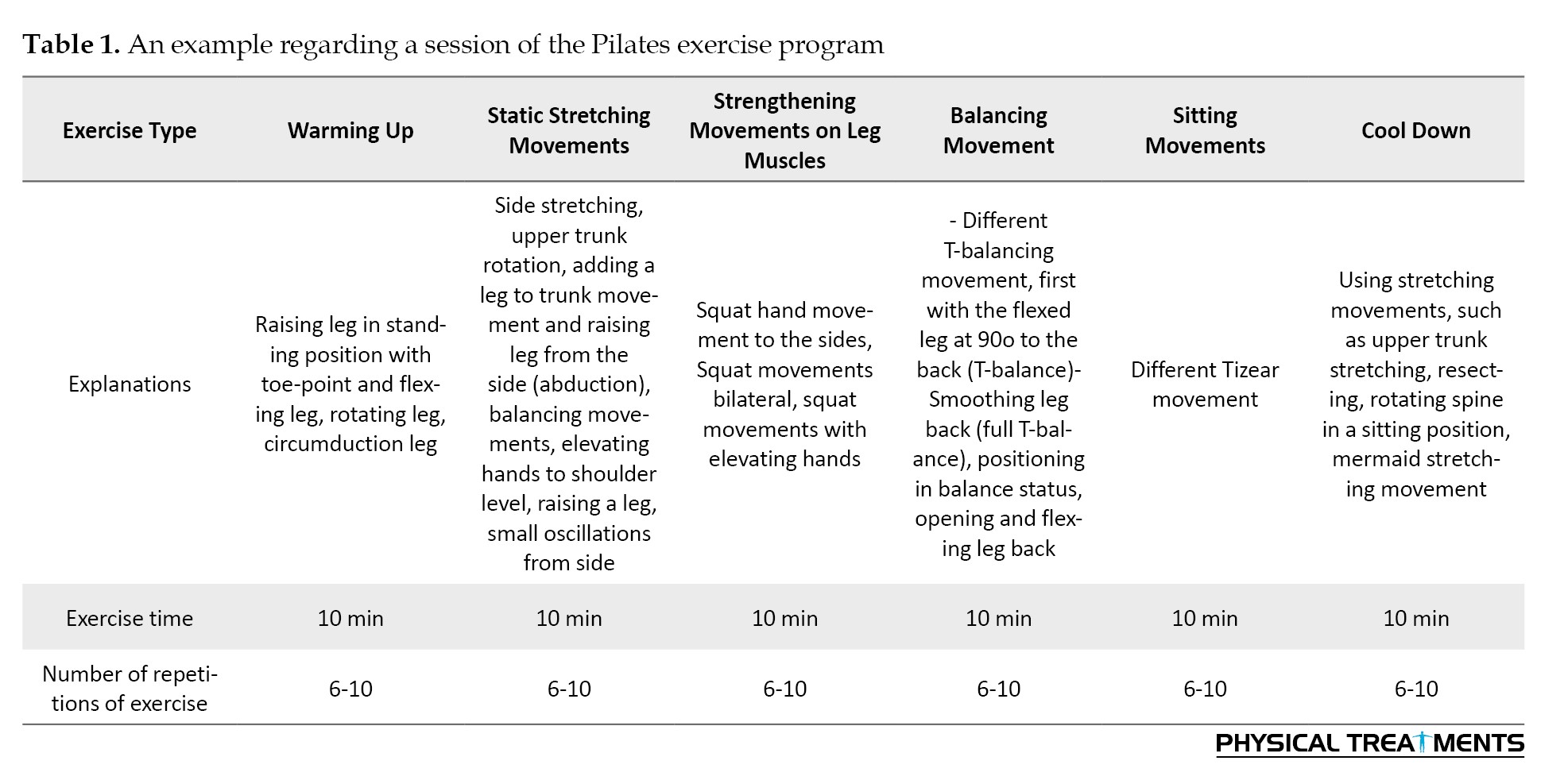
The Kolmogorov-Smirnov test showed normal data distribution (P>0.05). Demographic and clinical characteristics of the participants are shown in Table 2.
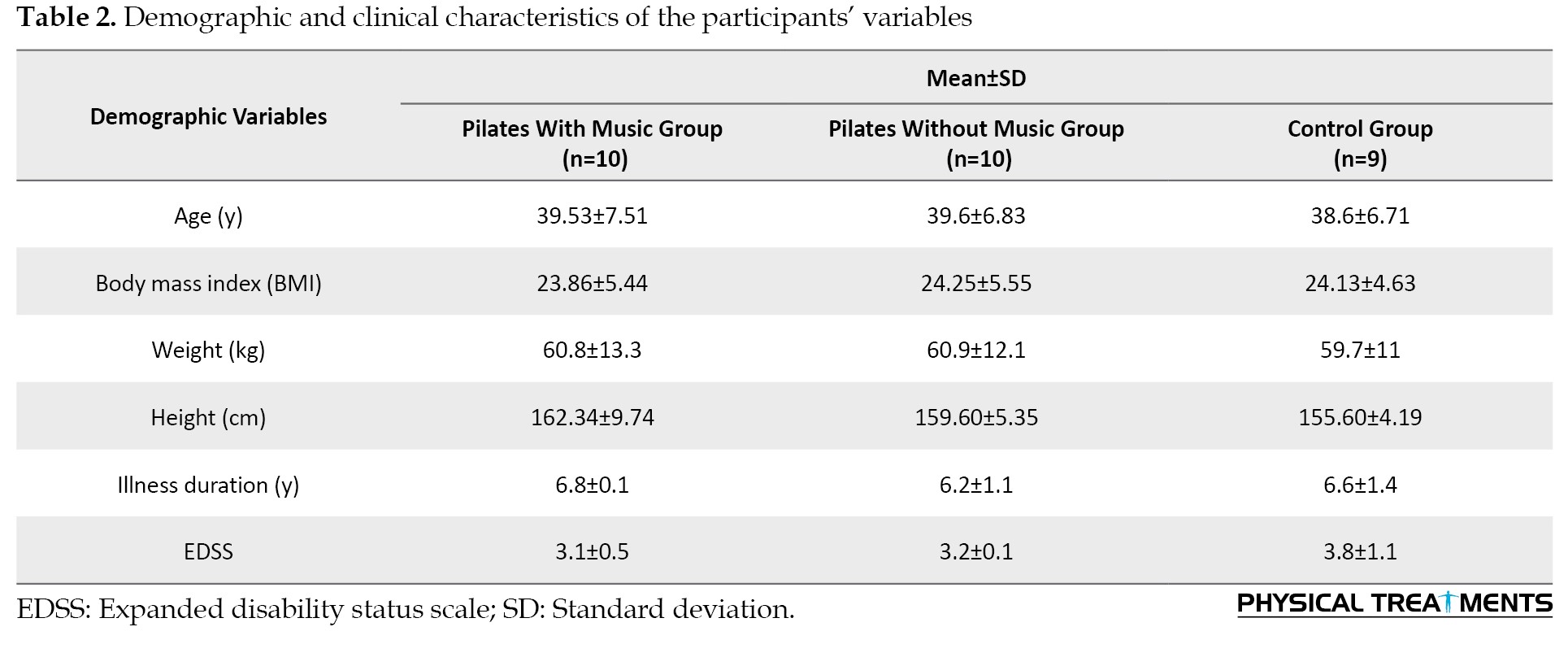
Meanwhile, Table 3 provides the Mean±SD of the pre-test and post-test findings in experimental and control groups.
The static and dynamic balance measurement was based on deviation and time, respectively.
As shown in Table 4, a significant difference is observed between the groups in the post-test based on the results of the analysis of covariance (P=0.02) in static balance.
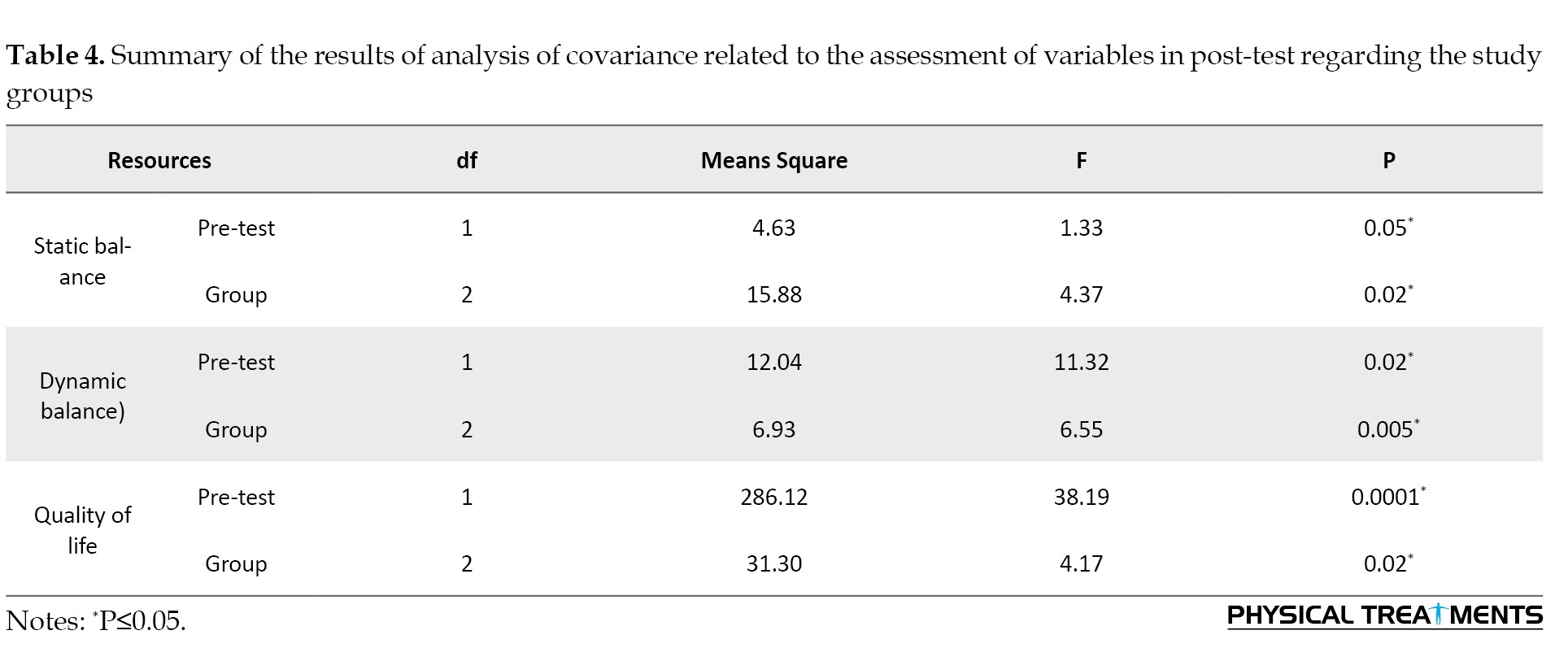
Considering this significant difference, the least significant difference post hoc test and the paired comparison of groups, the control group significantly differed from Pilates exercise with (P=0.004) and without music groups (P=0.008). In contrast, no significant difference was observed between Pilates with (P=0.421) and without music groups, although the pilates group’s mean scores were higher than the control group.
Based on the results in Table 4, the groups are significantly different in post-test (P=0.005) in dynamic balance. A statistically significant difference was observed between the control group and Pilates exercise with (P=0.023) and without music (P=0.001) by considering this significant difference, LSD post hoc test and the paired comparison of groups. At the same time, there was no significant difference between Pilates exercises without and with music groups (P=0.347), although the mean scores of the Pilates group were better than the control group.
Furthermore, according to Table 4, a significant difference in quality of life is observed between the groups in the post-test (P=0.02). Considering the significant difference between the least significant difference post hoc test and the paired comparison of groups, the control group significantly differs from Pilates exercise with (P=0.04) and without music groups (P=0.009). Additionally, no significant difference was observed between Pilates without and with music groups (P=0.42), although the mean scores of the Pilates group were better than the control group.
Discussion
Based on the results of the present study, a Pilates exercise course without music improves static and dynamic balance and the quality of life in MS patients significantly. The findings of the balance test in the present study align with those of some other studies [19-21, 26, 34, 35], while they are inconsistent with those of DeBolt et al. [36]. Considering the significant relationship between balance and the strength of upper and lower trunk muscles, [13] an increase in the general strength of these muscles resulted in enhancing physical mobility and balance. In addition, DeBolt et al.’s results were inconsistent due to their exercise program’s features, intensity and nature [36]. They focused on increasing the strength of downer trunk muscles [36], while the study of Filipi et al. (2010) and the present study highlighted improving the general muscular strength in exercise programs, leading to the enhancement of motor function [34]. Since Pilates exercises can increase strength, they are considered an influential factor in improving postural stability by enhancing the strength of lower limb muscles and core stability [37]. Since progressive strengthening exercises improve joint position sense in injured joints by increasing the sensitivity of muscle spindles and over-load, applied in the present study’s exercise sessions, the participants’ balance increased and progressed significantly compared to the control group. Considering the dependency of downer limbs on their upper limbs and the importance of balance in MS patients, Pilates exercises can effectively increase the strength of leg muscles and downer limbs, especially extensor and flexor muscles [37].
Based on the present study’s findings, Pilates exercises with music significantly affect the static and dynamic balance of MS patients, which aligns with those of some studies. de Dreu et al. (2012) found that exercise therapy with music improves motor balance and gait capability in Parkinson’s patients, which can be achieved following the coordination between patient movement with the rhythm of music and the enjoyable nature of therapy [38]. Atigh et al. (2013) mentioned that the presence of music significantly influences the cooperation and motivation for implementing motor movements and accelerates improving the implementation of balance skills [39]. Considering the effect of Pilates exercises and music on the balance of participants and the consistency between the present study and those conducted by de Dreu et al. (2012) [38] and Atigh et al. (2013) [39], the participants of the present study utilized these benefits compared to the control group and no descriptive effect was observed in their function, regardless of the type of participants.
In another study, researchers investigated the effect of the focus of attention and the combination of the focus of attention and music on learning the static and dynamic balance of ADHD children. They concluded that using instructions and music affects the balance of these children and improves grades [40]. The research mentioned in the field of the effect of music on balance is also in line with the findings of this research, regardless of the type of subject. Although the positive effects of music on balance on other subjects have been mentioned in past research [38, 41], considering that in this research, no control group only listens to music, it cannot be acknowledged that the effect is caused by playing music or in the case of He commented on the effect created by the music.
Since both experimental groups’ static and dynamic balances improved with no significant difference, both exercise approaches can increase these balances. However, the effect of exercise type on increasing the scores related to the static and dynamic balance test of participants is more remarkable when considering the superiority of their mean in the pilates without music group compared to those of Pilates with music group. Most of the improvement observed in both groups was caused by performing a Pilates exercise program, and their difference can represent that playing music simultaneously with these exercises may attract participant attention to music and reduce their scores. Accordingly, using music can lead to less change in the amount of balance among MS patients.
Based on the results of the present study, Pilates exercises with and without music led to a significant decrease in the degree of physical disability and its improvement in patients, which is inconsistent with the findings of White et al. [42] and consistent with those of Ciampi et al. and Grazioli et al. [12, 43]. The different types of MS disease, history of disease, and type of exercise are regarded as the reason for the ineffectiveness of exercises in the study conducted by White et al. Clinical pieces of evidence indicated that controlling and improving the symptoms of MS is challenging in its three types among four types instead of relapsing-remitting MS [12].
The results of the present study showed that Pilates exercises enhanced the quality of life, which aligns with many studies [44-48], although only aerobic exercises were conducted in most of these studies. Based on previous studies, the quality of life in MS patients increased due to the effect of exercises on their motor and neural-psychological systems [46, 49]. Considering the present study’s findings, physical pain and physical and mental restriction in acting decreased after six- weeks of Pilates exercises, which was associated with increasing patients’ mental and physical health. Thus, it is probably regarded as a reason for enhancing the quality of life in the present study. The results of the present study are not in line with those obtained by Newman et al. (2007) and Rampello et al. (2007) [4, 50] due to the difference in the type, intensity, and session number of exercise.
Regular participation in the present study’s exercise program can be considered one of the possible mechanisms for improving the quality of life in these patients. Despite the contradiction between MS disease and the physical and mental health status of MS patients, regular sports activities can result in increasing health levels in both physical and mental fields based on previous studies in this regard [44, 51]. Additionally, if a person is sedentary, they can apply less energy to the activities, and consequently, his muscular mass and function decrease; these factors can play an essential role in decreasing the quality of life in patients [52]. However, inactivity due to the fear of falling endangers muscle function, movement capability, and physical preparedness in most individuals [53], leading to their sedentary lifestyle. These factors enhance the increasing risk of diseases such as heart problems, osteoporosis, obesity and diabetes in these patients and consequently are regarded as factors for decreasing their quality of life [54]. Sports exercises can positively affect the quality of life in MS patients by setting the amount of neurotransmitters in neurons and consequently balancing and homogenizing the neural function of a person and reducing mental abnormalities [55].
Further, they lead to compatibilities in the brain and spinal cord and, thus, an increase in the recall capability of motor units. A person can do movements better by enhancing the recall of motor units by the brain [56]. Finally, improving the balance can be regarded as one possible reason for enhancing the present study’s quality of life. Thus, improving balance and balancing exercises enhances the quality of life in these patients based on previous studies [57, 58].
Conclusion
Considering the significant effectiveness of Pilates exercises with and without music on the balance and quality of life of MS patients and considering that no significant difference was observed in the comparison of the two exercise groups, it can be said that the use of both types of exercise is suggested. Also, considering the superiority of scores in the Pilates group without music, it seems that, if possible, in sports clubs, including Pilates clubs, along with exercise, the quality is desirable for people with MS who have no experience in participating in these exercises. Consider training sessions more than using music. It is suggested that in future studies, the effect of these exercises on other movement factors of patients with MS should be measured, and if possible, larger samples and a narrower age range should be used to make the results more generalizable.
Ethical Considerations
Compliance with ethical guidelines
The present study was approved and recorded by the Ethics Committee of Sabzevar branch, Islamic Azad University, Sabzevar, Iran (Code: IR.IAU.S.REC.1398.001). The informed consent form was completed in the present study. The study’s objective was explained to the participants completely and they were assured of the confidentiality of the data.
Funding
This paper was extracted from the master thesis of Zahra Estiri, approved by Hakim Sabzevari University, Sabzevar, Iran.
Authors' contributions
Conceptualization, supervision and writing the original Draft: Zahra Estiri and Mohammad Reza Shahabi Kaseb; Methodology, statistics analysis and funding: Zahra Estiri and Mitra Khademosharie; Investigation and data collection: Maryam Sadat Salehi Kalateh Sadat; review and editing: All authors
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors are especially grateful to the participants in this study.
References
Multiple sclerosis (MS) is an immune system-mediated demyelinating disease, resulting in physical, cognitive, and depressive symptoms in twice as many women as men aged 20-50 years [1]. Previous studies indicated that about 11 to 15 persons in 1000 have MS. Based on the World Health Organization (WHO) studies, this ratio is 4 to 5 persons among 10000 in Iran [2].
The disease’s occurrence in youth increases social and economic problems for the patient, their family, and the community [3]. These patients’ weakness of limbs, fatigue, and motor disorders affect their function. In addition, 85% of MS patients experience motor problems [4]. Balance is considered to maintain optimal body posture in static and dynamic positions and is a criterion for the whole body’s function. Additionally, the sensory information obtained from somatosensory (proprioception), vestibular, and visual systems affects balance maintenance [5]. The presence of dynamic balance in a person is one of the critical factors of triumphant gait, and most MS patients consider imbalance as the most challenging symptom of the disease, which is regarded as the initial cause of disorder in going and falling [6]. Around 20% of these falls may lead to newer problems such as fracture and infection, and motor restrictions in patients [7].
Furthermore, the quality of life in these patients is considered less and is influenced negatively by motor disorders and fatigue, according to previous studies [8, 9]. Mental and physical issues affect the quality of life of the person. They are considered as the factor limiting physical activity, which results in depending on person to others and an indirect increase in the severity of the disease in these people [10].
Despite the advancements in medical science in recent years, there is currently no definitive and eradicating therapy for MS disease, and most of the current therapeutic approaches result in decreasing symptoms or disease processes [11, 12]. In this regard, sports can be applied as complementary therapies, along with pharmaceutical approaches [12]. Considering the lack of definitive treatment using new medicines and their high costs and side effects, non-pharmacological approaches can be practical and accepted by patients easily [13]. Appropriate and particular exercise and physical activity for this group of patients can probably be effective in advancing their motor and cognitive capabilities. The usefulness of regular exercises for these patients was specified well [13-15]. Most of the exercise therapy studies focus on exercise in water, plyometric exercises, and aerobic and strength exercises or a combination of both while implementing various exercises, such as yoga, tai chi, and Pilates used as complementary therapy in exercise therapy, among utilizing mind and body [16].
Using the Pilates exercise method challenges the sensory, skeletal, nervous and muscular systems required for dynamic balance [17]. It helps develop trunk muscles and restore muscle balance by strengthening, stretching, and breathing. Additionally, Pilates exercises result in increasing physical function (flexibility, muscular strength, endurance, power and cardiorespiratory fitness) and motor control (control of trunk, static and dynamic stability and beauty of movement) [18]. Limited studies were conducted on the effect of these exercises on MS patients by representing the effectiveness of Pilates exercises on physical and cognitive factors. Guclu-Gunduz et al. (2014) found that eight weeks of Pilates exercises improved the muscular strength of lower and upper limbs, mobility, and balance in MS patients in the experimental group compared to the control group [19]. Based on the results of another study, 12 weeks of Pilates significantly increases dynamic balance in female MS patients, similar to exercises in water [20]. Abasıyanık et al. showed that eight weeks of Pilates exercises were superior to the home exercise program in walking endurance, postural stability, core stability, respiratory, and cognitive functions [21]. People suffering from this disease are facing many problems that limit the patients’ participation in health promotion activities and, as a result, increase secondary complications and limit their independent lives, which ultimately harms their quality of life. Physical, psychological, social, and economic dimensions of quality of life undergo many changes in chronic diseases [22].
In addition to Pilates exercises, music is one of the most effective tools for increasing concentration and attention. Listening to music can improve self-control, physical movements, movement balance, and bodily states [23]. In a study, researchers reported positive effects of music on the acquisition of balance in people with Parkinson’s disease [24]. In another study, researchers investigated the effect of the focus of attention and the combination of focus and music on static and dynamic balance learning in attention deficit hyperactivity disorder (ADHD) children. They concluded that using instructions and music affects the balance performance of these children and improves their balance scores [25].
Due to limited studies in this area [19-21, 26] and considering the studies conducted on Pilates exercises, assessment of using music, and effects of these exercises on body and mind, the present study compares the effect of Pilates exercises with and without music on balance function and the quality of life in MS patients. Based on the previous studies, this question is proposed whether using music, along with Pilates exercises, can affect the amount of balance (motor skill) and quality of life in participants as a positive factor or may influence negatively or fail to affect the balance of MS patients as considerable over-load.
Materials and Methods
Data collection method
Female volunteers were invited and registered to participate in the present study by referring to the MS association in Sabzevar City, Iran. After recalling and inviting participation by the confirmation of specialist physicians, 29 female patients aged 20-50 years were selected through convenient sampling. The inclusion criteria of the present study were the expanded disability status scale (EDSS) between 2-5, which specialist physicians determined through conducting examinations related to the diagnosis of MS disease, such as magnetic resonance imaging or computed tomography scan and the functional tests related to balance, strength, gait capability, and vision and tactile testing (to the extent that patients can do exercises), age range of 20-50 years, regular menstrual cycle, absence of other diseases (heart problems, diabetes, epilepsy and other particular problems that limited the implementation of exercises), non-participation in regular sports program and consumption of almost similar medicine.
After the early registration of participants, a dating meeting was held to introduce the study’s overall design, nutrition program, and pharmaceutical program, as well as to conduct cardiovascular-respiratory tests for entering the study and completing the consent form. Further, the initial anthropometric and demographic data, including age, height, weight and the percentage of subcutaneous fat, were recorded.
The patients were divided into experimental and control groups based on leg muscles’ strength homogenization. Leg muscles’ strength was measured using a dynamometer. Regarding the first day, tests and the exercise process were explained to the participants in each group. Further, all participants were pre-tested using a stabilimeter and dynamic balance test and they completed the quality-of-life questionnaire. Furthermore, they were homogenized based on the early strength test and randomly divided into three groups: Two experimental groups (n=10 in each group) and a control group (n=9). Then, the participants were post-tested using the mentioned tool after six weeks.
Measurement of demographic data and disability index
The height and weight of participants were determined by using a tape measure (Komelon [South Korea] Company with 1/16th of an inch or 1-mm sensitivity) on the wall and a digital scale (Etekcity [China] Company with 0.1 pounds (~0.05 kg) sensitivity), respectively.
Body composition
The body fat percentage and waist-to-hip ratio related to participants were measured using a body composition analyzer (In Body 3.0, South Korea). To this end, all participants were asked to refer to the laboratory of physical education in the university as overnight fasting. After turning the device on, the participants were requested to drain the bladder using wipes to humidify their feet and foothold on the device. Then, they should go on a foothold, take handles, and keep them until the charts of the device end after entering the required data by the tester. Finally, the obtained data were printed and used [27].
Expanded disability status scale
EDSS measures the severity of physical, neurological, and muscular disability in MS patients. The scores of the scale range from 0 to 10, in which 0 and 10 represent the lack of physical disorder in the field of systems function and very severe disability, respectively [28]. The patients with the maximum score of five were selected in the present study.
Static balance
Static balance was assessed using a stabilimeter (Iranian Danesh Salar Company). This device measures and analyzes body oscillations indirectly based on the reaction of static level to the forces caused by changing the center of gravity in person. The data related to body movement are used in different parameters two-dimensionally during standing with open and closed eyes as instantaneously and visually. This instrument’s minimum acceptable reliability and validity is 0.70, and its maximum acceptable reliability is 0.90 [29]. Regarding the method of measuring static and dynamic balance, the prerequisites for testing, including calibrating the device and providing required explanations about the overall testing process to each participant, were conducted after turning on the stabilimeter. Then, each patient went on the device for 30 s with his dominant leg as bare leg and looked at a specific point mounted on the wall by considering his height. Since each head movement displaces the center of gravity, a specific point is considered to prevent his eye movements from affecting his surroundings [30]. The mean of rate changes in the body movement of participants obtained by averaging diversion in four directions was used in the present study.
Balance test of timed up and go
Dynamic balance was evaluated using timed up and go (TUG). Considering the test’s method, the participant should get up from a seat and handle-less without using his hands, return, and sit on their seat after crossing an eight-foot path (2.44 m). Regarding the present study, the participants were asked to do this activity with more speed and skill without running, and finally, overall time was recorded as their score. Due to the unfamiliarity of participants with the method of performing the test, they trained the test three times before recording the tests. Then, each of them conducted the test thrice and the meantime (s) were recorded as their score [31].
The dynamometer (HBM test and measurement [Hottinger Brüel & Kjaer GmbH], Germany) was applied for assessing to assess the strength of leg muscles and early homogenization of groups [32].
Music
Classical instrumental music with moderate intensity, confirmed by the Pilates association, was used in the present exercise program. These types of music give extraordinary relaxation to the athlete during the exercise and cause the pressure on the heart to decrease during the exercise. Also, the one engaged in Pilates eliminates all the mental preoccupations and turns this exercise into a meditation.
Quality of life
The quality of life was assessed by using a standard questionnaire containing 36 questions in the eight scales of public health (n=5), physical function (n=10), emotional health (n=5), physical pain (n=2), energy and happiness (n=4), social function (n=2), and the role of physical and mental health in limiting activities (4 and 3 questions, respectively). Regarding the calculation of responding to the questionnaire questions, the responses were first scored from 1 to 5 based on the Likert scale, where scores 1 and 5 represent the terrible and great status of participants, respectively. Then, the scores were converted into eight components ranging between 0 to 100. Finally, the mean sum of cases was calculated as the score of the intended scale regarding the quality of life, and the higher scores indicate a better quality of life [33].
Exercise program
The exercise program was implemented for six weeks under the supervision of an exercise physiologist and 60-min sessions were held each week. The first experimental group performed Pilates exercises for six weeks. each week, three 60-min sessions were conducted under the supervision of a Pilates instructor in the morning. each exercise session was divided into three parts: Warming up (10-15 min), doing Pilates exercises (35-40 min) and cooling down (10 min) (Table 1).
The exercise were started by simple movements and then their intensity and complexity increased and then their intensity and complexity increased.
Further, the range of stretching, time and repetition of movements gradually increased with the participants’ progress and new exercises were added to each session compared to the previous session. The speed of progressing exercises related to all participants was at the same level. Further, they were recommended to do exercises as long as they did not feel pain and discomfort. The training intensity was determined using the Borg scale, in the first sessions between 4-5, in the next sessions 6-7 and in the last sessions 8-9. Furthermore, exercises were conducted in the sleeping position first, then sitting and standing [31]. Most exercises focused on the downer limb, and a 30-s rest period with inhaling and exhaling between movements was considered (Table 1). The second experimental group implemented these exercises with the music confirmed by the Pilates association. Finally, the patients in the control group only did their daily activities during the exercise course. Table 1 represents an example of a session of the Pilates exercise program.
Statistical analysis
Descriptive statistics were used to summarize collected information and recognize the community more so that the data could be analyzed. Further, statistical hypotheses were tested using inferential statistics, and data distribution was estimated to be normal based on Kolmogorov-Smirnov and the Levene tests. Analysis of covariance and Fisher least significant difference post hoc test were used to compare groups and specify their difference. The calculations were conducted using the SPSS software, version 22 and the significance level was P<0.05.
Results
The Kolmogorov-Smirnov test showed normal data distribution (P>0.05). Demographic and clinical characteristics of the participants are shown in Table 2.
Meanwhile, Table 3 provides the Mean±SD of the pre-test and post-test findings in experimental and control groups.
The static and dynamic balance measurement was based on deviation and time, respectively.
As shown in Table 4, a significant difference is observed between the groups in the post-test based on the results of the analysis of covariance (P=0.02) in static balance.
Considering this significant difference, the least significant difference post hoc test and the paired comparison of groups, the control group significantly differed from Pilates exercise with (P=0.004) and without music groups (P=0.008). In contrast, no significant difference was observed between Pilates with (P=0.421) and without music groups, although the pilates group’s mean scores were higher than the control group.
Based on the results in Table 4, the groups are significantly different in post-test (P=0.005) in dynamic balance. A statistically significant difference was observed between the control group and Pilates exercise with (P=0.023) and without music (P=0.001) by considering this significant difference, LSD post hoc test and the paired comparison of groups. At the same time, there was no significant difference between Pilates exercises without and with music groups (P=0.347), although the mean scores of the Pilates group were better than the control group.
Furthermore, according to Table 4, a significant difference in quality of life is observed between the groups in the post-test (P=0.02). Considering the significant difference between the least significant difference post hoc test and the paired comparison of groups, the control group significantly differs from Pilates exercise with (P=0.04) and without music groups (P=0.009). Additionally, no significant difference was observed between Pilates without and with music groups (P=0.42), although the mean scores of the Pilates group were better than the control group.
Discussion
Based on the results of the present study, a Pilates exercise course without music improves static and dynamic balance and the quality of life in MS patients significantly. The findings of the balance test in the present study align with those of some other studies [19-21, 26, 34, 35], while they are inconsistent with those of DeBolt et al. [36]. Considering the significant relationship between balance and the strength of upper and lower trunk muscles, [13] an increase in the general strength of these muscles resulted in enhancing physical mobility and balance. In addition, DeBolt et al.’s results were inconsistent due to their exercise program’s features, intensity and nature [36]. They focused on increasing the strength of downer trunk muscles [36], while the study of Filipi et al. (2010) and the present study highlighted improving the general muscular strength in exercise programs, leading to the enhancement of motor function [34]. Since Pilates exercises can increase strength, they are considered an influential factor in improving postural stability by enhancing the strength of lower limb muscles and core stability [37]. Since progressive strengthening exercises improve joint position sense in injured joints by increasing the sensitivity of muscle spindles and over-load, applied in the present study’s exercise sessions, the participants’ balance increased and progressed significantly compared to the control group. Considering the dependency of downer limbs on their upper limbs and the importance of balance in MS patients, Pilates exercises can effectively increase the strength of leg muscles and downer limbs, especially extensor and flexor muscles [37].
Based on the present study’s findings, Pilates exercises with music significantly affect the static and dynamic balance of MS patients, which aligns with those of some studies. de Dreu et al. (2012) found that exercise therapy with music improves motor balance and gait capability in Parkinson’s patients, which can be achieved following the coordination between patient movement with the rhythm of music and the enjoyable nature of therapy [38]. Atigh et al. (2013) mentioned that the presence of music significantly influences the cooperation and motivation for implementing motor movements and accelerates improving the implementation of balance skills [39]. Considering the effect of Pilates exercises and music on the balance of participants and the consistency between the present study and those conducted by de Dreu et al. (2012) [38] and Atigh et al. (2013) [39], the participants of the present study utilized these benefits compared to the control group and no descriptive effect was observed in their function, regardless of the type of participants.
In another study, researchers investigated the effect of the focus of attention and the combination of the focus of attention and music on learning the static and dynamic balance of ADHD children. They concluded that using instructions and music affects the balance of these children and improves grades [40]. The research mentioned in the field of the effect of music on balance is also in line with the findings of this research, regardless of the type of subject. Although the positive effects of music on balance on other subjects have been mentioned in past research [38, 41], considering that in this research, no control group only listens to music, it cannot be acknowledged that the effect is caused by playing music or in the case of He commented on the effect created by the music.
Since both experimental groups’ static and dynamic balances improved with no significant difference, both exercise approaches can increase these balances. However, the effect of exercise type on increasing the scores related to the static and dynamic balance test of participants is more remarkable when considering the superiority of their mean in the pilates without music group compared to those of Pilates with music group. Most of the improvement observed in both groups was caused by performing a Pilates exercise program, and their difference can represent that playing music simultaneously with these exercises may attract participant attention to music and reduce their scores. Accordingly, using music can lead to less change in the amount of balance among MS patients.
Based on the results of the present study, Pilates exercises with and without music led to a significant decrease in the degree of physical disability and its improvement in patients, which is inconsistent with the findings of White et al. [42] and consistent with those of Ciampi et al. and Grazioli et al. [12, 43]. The different types of MS disease, history of disease, and type of exercise are regarded as the reason for the ineffectiveness of exercises in the study conducted by White et al. Clinical pieces of evidence indicated that controlling and improving the symptoms of MS is challenging in its three types among four types instead of relapsing-remitting MS [12].
The results of the present study showed that Pilates exercises enhanced the quality of life, which aligns with many studies [44-48], although only aerobic exercises were conducted in most of these studies. Based on previous studies, the quality of life in MS patients increased due to the effect of exercises on their motor and neural-psychological systems [46, 49]. Considering the present study’s findings, physical pain and physical and mental restriction in acting decreased after six- weeks of Pilates exercises, which was associated with increasing patients’ mental and physical health. Thus, it is probably regarded as a reason for enhancing the quality of life in the present study. The results of the present study are not in line with those obtained by Newman et al. (2007) and Rampello et al. (2007) [4, 50] due to the difference in the type, intensity, and session number of exercise.
Regular participation in the present study’s exercise program can be considered one of the possible mechanisms for improving the quality of life in these patients. Despite the contradiction between MS disease and the physical and mental health status of MS patients, regular sports activities can result in increasing health levels in both physical and mental fields based on previous studies in this regard [44, 51]. Additionally, if a person is sedentary, they can apply less energy to the activities, and consequently, his muscular mass and function decrease; these factors can play an essential role in decreasing the quality of life in patients [52]. However, inactivity due to the fear of falling endangers muscle function, movement capability, and physical preparedness in most individuals [53], leading to their sedentary lifestyle. These factors enhance the increasing risk of diseases such as heart problems, osteoporosis, obesity and diabetes in these patients and consequently are regarded as factors for decreasing their quality of life [54]. Sports exercises can positively affect the quality of life in MS patients by setting the amount of neurotransmitters in neurons and consequently balancing and homogenizing the neural function of a person and reducing mental abnormalities [55].
Further, they lead to compatibilities in the brain and spinal cord and, thus, an increase in the recall capability of motor units. A person can do movements better by enhancing the recall of motor units by the brain [56]. Finally, improving the balance can be regarded as one possible reason for enhancing the present study’s quality of life. Thus, improving balance and balancing exercises enhances the quality of life in these patients based on previous studies [57, 58].
Conclusion
Considering the significant effectiveness of Pilates exercises with and without music on the balance and quality of life of MS patients and considering that no significant difference was observed in the comparison of the two exercise groups, it can be said that the use of both types of exercise is suggested. Also, considering the superiority of scores in the Pilates group without music, it seems that, if possible, in sports clubs, including Pilates clubs, along with exercise, the quality is desirable for people with MS who have no experience in participating in these exercises. Consider training sessions more than using music. It is suggested that in future studies, the effect of these exercises on other movement factors of patients with MS should be measured, and if possible, larger samples and a narrower age range should be used to make the results more generalizable.
Ethical Considerations
Compliance with ethical guidelines
The present study was approved and recorded by the Ethics Committee of Sabzevar branch, Islamic Azad University, Sabzevar, Iran (Code: IR.IAU.S.REC.1398.001). The informed consent form was completed in the present study. The study’s objective was explained to the participants completely and they were assured of the confidentiality of the data.
Funding
This paper was extracted from the master thesis of Zahra Estiri, approved by Hakim Sabzevari University, Sabzevar, Iran.
Authors' contributions
Conceptualization, supervision and writing the original Draft: Zahra Estiri and Mohammad Reza Shahabi Kaseb; Methodology, statistics analysis and funding: Zahra Estiri and Mitra Khademosharie; Investigation and data collection: Maryam Sadat Salehi Kalateh Sadat; review and editing: All authors
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors are especially grateful to the participants in this study.
References
- Muhtaroglu M, Lafcı Fahrioglu S, Selcuk F, İlgi S. Evaluation of thoracic kyphosis angle and respiratory functions in patients with multiple sclerosis. Annals of Applied Sport Science. 2021; 9(2): e990. [DOI:10.52547/aassjournal.990]
- Browne P, Chandraratna D, Angood C, Tremlett H, Baker C, Taylor BV, et al. Atlas of Multiple Sclerosis 2013: A growing global problem with widespread inequity. Neurology. 2014; 83(11):1022-4. [DOI:10.1212/WNL.0000000000000768] [PMID] [PMCID]
- Brunner LS. Brunner & Suddarth's textbook of medical-surgical nursing. Philadelphia: Lippincott Williams & Wilkins; 2010. [Link]
- Newman MA, Dawes H, van den Berg M, Wade DT, Burridge J, Izadi H. Can aerobic treadmill training reduce the effort of walking and fatigue in people with multiple sclerosis: A pilot study. Multiple Sclerosis. 2007; 13(1):113-9. [DOI:10.1177/1352458506071169] [PMID]
- Farivar M, Harris S, Agana A, King AC. Lower limb cross-over effects on postural control: Impact of proximal and distal muscle fatigue. Biomechanics. 2024; 4(1):50-62. [DOI:10.3390/biomechanics4010004]
- Gunn H, Markevics S, Haas B, Marsden J, Freeman J. Systematic review: The effectiveness of interventions to reduce falls and improve balance in adults with multiple sclerosis. Archives of Physical Medicine and Rehabilitation. 2015; 96(10):1898-912. [DOI:10.1016/j.apmr.2015.05.018] [PMID]
- Cameron MH, Poel AJ, Haselkorn JK, Linke A, Bourdette D. Falls requiring medical attention among veterans with multiple sclerosis: A cohort study. Journal of Rehabilitation Research and Development. 2011; 48(1):13-20. [DOI:10.1682/JRRD.2009.12.0192] [PMID]
- Pérez de Heredia-Torres M, Huertas-Hoyas E, Sánchez-Camarero C, Máximo-Bocanegra N, Alegre-Ayala J, Sánchez-Herrera-Baeza P, et al. Occupational performance in multiple sclerosis and its relationship with quality of life and fatigue. European Journal of Physical and Rehabilitation Medicine. 2020; 56(2):148-54. [DOI:10.23736/S1973-9087.20.05914-6] [PMID]
- Amtmann D, Bamer AM, Kim J, Chung H, Salem R. People with multiple sclerosis report significantly worse symptoms and health related quality of life than the US general population as measured by PROMIS and NeuroQoL outcome measures. Disability and Health Journal. 2018; 11(1):99-107. [DOI:10.1016/j.dhjo.2017.04.008] [PMID]
- Eftekhari E, Nikbakht HA, Rabiei K. Effect of endurance training on aerobic power and quality of life in female patients with multiple sclerosis. Paper presented at: The 5th Interntional MS Congress in Iran. 1 November 2008; Tehran, Iran. [Link]
- Gholamzad M, Ebtekar M, Ardestani MS, Azimi M, Mahmodi Z, Mousavi MJ, Aslani S. A comprehensive review on the treatment approaches of multiple sclerosis: Currently and in the future. Inflammation Research. 2019; 68(1):25-38. [DOI:10.1007/s00011-018-1185-0] [PMID]
- Grazioli E, Tranchita E, Borriello G, Cerulli C, Minganti C, Parisi A. The effects of concurrent resistance and aerobic exercise training on functional status in patients with multiple sclerosis. Current Sports Medicine Reports. 2019; 18(12):452-7. [DOI:10.1249/JSR.0000000000000661] [PMID]
- Dalgas U, Stenager E, Ingemann-Hansen T. Multiple sclerosis and physical exercise: Recommendations for the application of resistance-, endurance- and combined training. Multiple Sclerosis. 2008; 14(1):35-53. [DOI:10.1177/1352458507079445] [PMID]
- Latimer-Cheung AE, Martin Ginis KA, Hicks AL, Motl RW, Pilutti LA, Duggan M, et al. Development of evidence-informed physical activity guidelines for adults with multiple sclerosis. Archives of Physical Medicine and Rehabilitation. 2013; 94(9):1829-36.e7. [DOI:10.1016/j.apmr.2013.04.020] [PMID]
- Huang WJ, Chen WW, Zhang X. Multiple sclerosis: Pathology, diagnosis and treatments. Experimental and Therapeutic Medicine. 2017; 13(6):3163-6. [DOI:10.3892/etm.2017.4410] [PMID] [PMCID]
- Wyss J. Therapeutic programs for musculoskeletal disorders. New York: Demos Medical Publishing; 2012. [Link]
- Fox EE, Hough AD, Creanor S, Gear M, Freeman JA. Effects of pilates-based core stability training in ambulant people with multiple sclerosis: Multicenter, assessor-blinded, randomized controlled trial. Physical Therapy. 2016; 96(8):1170-8. [DOI:10.2522/ptj.20150166] [PMID]
- Kalron A, Rosenblum U, Frid L, Achiron A. Pilates exercise training vs. physical therapy for improving walking and balance in people with multiple sclerosis: A randomized controlled trial. Clinical Rehabilitation. 2017; 31(3):319-28. [DOI:10.1177/0269215516637202] [PMID]
- Guclu-Gunduz A, Citaker S, Irkec C, Nazliel B, Batur-Caglayan HZ. The effects of pilates on balance, mobility and strength in patients with multiple sclerosis. NeuroRehabilitation. 2014; 34(2):337-42. [DOI:10.3233/NRE-130957] [PMID]
- Shanazari Z, Marandi S M, Minasian V. Effect of 12-week pilates and aquatic training on fatigue in women with multiple sclerosis. Mazandaran University of Medical Sciences. 2013; 22(98):257-64. [Link]
- Abasıyanık Z, Ertekin Ö, Kahraman T, Yigit P, Özakbaş S. The effects of Clinical Pilates training on walking, balance, fall risk, respiratory, and cognitive functions in persons with multiple sclerosis: A randomized controlled trial. Explore. 2020; 16(1):12-20. [DOI:10.1016/j.explore.2019.07.010] [PMID]
- Tollár J, Nagy F, Tóth BE, Török K, Szita K, Csutorás B, et al. Exercise effects on multiple sclerosis quality of life and clinical-motor symptoms. Medicine and Science in Sports and Exercise. 2020; 52(5):1007-14. [DOI:10.1249/01.mss.0000686548.23451.69] [PMID]
- Impellizzeri F, Leonardi S, Latella D, Maggio MG, Foti Cuzzola M, Russo M, et al. An integrative cognitive rehabilitation using neurologic music therapy in multiple sclerosis: A pilot study. Medicine. 2020; 99(4):e18866. [DOI:10.1097/MD.0000000000018866] [PMID] [PMCID]
- Zhou Z, Zhou R, Wei W, Luan R, Li K. Effects of music-based movement therapy on motor function, balance, gait, mental health, and quality of life for patients with Parkinson's disease: A systematic review and meta-analysis. Clinical Rehabilitation. 2021; 35(7):937-51.[DOI:10.1177/0269215521990526] [PMID]
- Yujuan W. Effect of creative dance on attention deficit hyperactivity disorder childrens attention. Revista Argentina de Clínica Psicológica. 2021; 30(1):11-20. [DOI: 10.24205/03276716.2020.2099]
- Duff WRD, Andrushko JW, Renshaw DW, Chilibeck PD, Farthing JP, Danielson J, et al. Impact of pilates exercise in multiple sclerosis: A randomized controlled trial. International Journal of MS Care. 2018; 20(2):92-100. [DOI:10.7224/1537-2073.2017-066] [PMID] [PMCID]
- Ayvaz G, Çimen AR. Methods for body composition analysis in adults. The Open Obesity Journal. 2011; 3: 62-9. [DOI:10.2174/1876823701103010062]
- Ziemssen T. Multiple sclerosis beyond EDSS: Depression and fatigue. Journal of the Neurological Sciences. 2009; 277(Suppl 1):S37-41. [DOI:10.1016/S0022-510X(09)70011-5] [PMID]
- Hedbávný P, Bago G, Kalichová M. Influence of strength abilities on quality of the handstand. International Journal of Sport and Health Sciences. 2013; 7(10):602-8. [Link]
- Harrison PL, Littlewood C. Relationship between pes planus foot type and postural stability. Indian Journal of Physiotherapy and Occupational Therapy. 2010; 4(3):21-4. [Link]
- Sebastião E, Sandroff BM, Learmonth YC, Motl RW. Validity of the timed up and go test as a measure of functional mobility in persons with multiple sclerosis. Archives of Physical Medicine and Rehabilitation. 2016; 97(7):1072-7. [DOI:10.1016/j.apmr.2015.12.031] [PMID]
- Hadavi F. [Measurement, deliberation and evaluation in physical education (Persian)]. Tehran: Mehr Sobhan; 2013. [Link]
- Simeoni M, Auquier P, Fernandez O, Flachenecker P, Stecchi S, Constantinescu C, et al. Validation of the multiple sclerosis international quality of life questionnaire. Multiple Sclerosis. 2008; 14(2):219-30. [DOI:10.1177/1352458507080733] [PMID]
- Filipi ML, Leuschen MP, Huisinga J, Schmaderer L, Vogel J, Kucera D, et al. Impact of resistance training on balance and gait in multiple sclerosis. International Journal of MS Care. 2010; 12(1):6-12. [DOI:10.7224/1537-2073-12.1.6]
- Sánchez-Lastra MA, Martínez-Aldao D, Molina AJ, Ayán C. Pilates for people with multiple sclerosis: A systematic review and meta-analysis. Multiple Sclerosis and Related Disorders. 2019; 28:199-212. [DOI:10.1016/j.msard.2019.01.006] [PMID]
- DeBolt LS, McCubbin JA. The effects of home-based resistance exercise on balance, power, and mobility in adults with multiple sclerosis. Archives of Physical Medicine and Rehabilitation. 2004; 85(2):290-7. [DOI:10.1016/j.apmr.2003.06.003] [PMID]
- Yu JH, Lee GC. Effect of core stability training using pilates on lower extremity muscle strength and postural stability in healthy subjects. Isokinetics and Exercise Science. 2012; 20(2):141-6. [DOI:10.3233/IES-2012-0462]
- de Dreu MJ, van der Wilk AS, Poppe E, Kwakkel G, van Wegen EE. Rehabilitation, exercise therapy and music in patients with Parkinson's disease: A meta-analysis of the effects of music-based movement therapy on walking ability, balance and quality of life. Parkinsonism & Related Disorders. 2012; 18(Suppl 1):S114-9. [DOI:10.1016/S1353-8020(11)70036-0] [PMID]
- Atigh A, Akbarfahimi M, Alizadeh M, Rad MM. The effect of musical movement activities on the balance function of autistic children. Journal of Kermanshah University of Medical Sciences. 2013; 17(8):e74389. [Link]
- Majorek M, Tüchelmann T, Heusser P. Therapeutic Eurythmy-movement therapy for children with attention deficit hyperactivity disorder (ADHD): A pilot study. Complementary Therapies in Nursing & Midwifery. 2004; 10(1):46-53. [DOI:10.1016/S1353-6117(03)00087-8] [PMID]
- Sanglakh Goochan Atigh A, Akbarfahimi M, Alizadeh Zarei M. [The effect of movement activities in synchronization with music on motor proficiency of children with autism (Persian)]. Journal of Advanced Medical Sciences and Applied Technologies. 2017; 3(2):61-8. [DOI:10.18869/nrip.jamsat.3.2.61]
- White LJ, Dressendorfer RH. Exercise and multiple sclerosis. Sports Medicine. 2004; 34(15):1077-100. [DOI:10.2165/00007256-200434150-00005] [PMID]
- Ciampi E, Uribe-San-Martin R, Vásquez M, Ruiz-Tagle A, Labbe T, Cruz JP, et al. Relationship between Social Cognition and traditional cognitive impairment in Progressive Multiple Sclerosis and possible implicated neuroanatomical regions. Multiple Sclerosis and Related Disorders. 2018; 20:122-28. [DOI:10.1016/j.msard.2018.01.013] [PMID]
- Reynolds ER, Ashbaugh AD, Hockenberry BJ, McGrew CA. Multiple sclerosis and exercise: A literature review. Current Sports Medicine Reports. 2018; 17(1):31-5. [DOI:10.1249/JSR.0000000000000446] [PMID]
- Ahmadi A, Arastoo AA, Nikbakht M, Zahednejad S, Rajabpour M. Comparison of the effect of 8 weeks aerobic and yoga training on ambulatory function, fatigue and mood status in MS patients. Iranian Red Crescent Medical Journal. 2013; 15(6):449-54. [DOI:10.5812/ircmj.3597] [PMID]
- kargar M. [Changes in quality of life and fatigue in women with multiple sclerosis after 8 weeks of aquatic exercise training (Persian)]. Journal of Fundamentals of Mental Health. 2010; 12(47):562-73. [DOI:10.22038/jfmh.2010.1038]
- Schmidt S, Wonneberger M. Long-term endurance exercise improves aerobic capacity in patients with relapsing-remitting multiple sclerosis: Impact of baseline fatigue.Journal of the Neurological Sciences. 2014; 336(1-2):29-35. [DOI:10.1016/j.jns.2013.09.035] [PMID]
- Alvarenga-Filho H, Sacramento PM, Ferreira TB, Hygino J, Abreu JEC, Carvalho SR, et al. Combined exercise training reduces fatigue and modulates the cytokine profile of T-cells from multiple sclerosis patients in response to neuromediators.Journal of Neuroimmunology. 2016; 293:91-9. [DOI:10.1016/j.jneuroim.2016.02.014] [PMID]
- Motl RW, McAuley E, Snook EM, Gliottoni RC. Physical activity and quality of life in multiple sclerosis: intermediary roles of disability, fatigue, mood, pain, self-efficacy and social support. Psychology, Health & Medicine. 2009; 14(1):111-24. [DOI:10.1080/13548500802241902] [PMID] [PMCID]
- Rampello A, Franceschini M, Piepoli M, Antenucci R, Lenti G, Olivieri D, et al. Effect of aerobic training on walking capacity and maximal exercise tolerance in patients with multiple sclerosis: A randomized crossover controlled study. Physical Therapy. 2007; 87(5):545-55. [DOI:10.2522/ptj.20060085] [PMID]
- Rietberg MB, Brooks D, Uitdehaag BM, Kwakkel G. Exercise therapy for multiple sclerosis. The Cochrane Database of Systematic Reviews. 2005; 2005(1):CD003980. [DOI:10.1002/14651858.CD003980.pub2] [PMID] [PMCID]
- Edwards T, Pilutti LA. The effect of exercise training in adults with multiple sclerosis with severe mobility disability: A systematic review and future research directions. Multiple Sclerosis and Related Disorders. 2017; 16:31-9. [DOI:10.1016/j.msard.2017.06.003] [PMID]
- Vister E, Tijsma ME, Hoang PD, Lord SR. Fatigue, physical activity, quality of life, and fall risk in people with multiple sclerosis. International Journal of MS Care. 2017; 19(2):91-8. [DOI:10.7224/1537-2073.2015-077] [PMID] [PMCID]
- Mayo NE, Bayley M, Duquette P, Lapierre Y, Anderson R, Bartlett S. The role of exercise in modifying outcomes for people with multiple sclerosis: A randomized trial. BMC Neurology. 2013; 13:69. [DOI:10.1186/1471-2377-13-69] [PMID] [PMCID]
- Hassan EA, Amin MA. Pilates exercises influence on the serotonin hormone, some physical variables and the depression degree in battered women. World Journal of Sport Sciences. 2011; 5(2):89-100. [Link]
- Rosenbaum DA. Human motor control. Academic Press; 2009. [Link]
- Sangelaji B, Nabavi SM, Estebsari F, Banshi MR, Rashidian H, Jamshidi E, et al. Effect of combination exercise therapy on walking distance, postural balance, fatigue and quality of life in multiple sclerosis patients: A clinical trial study. Iranian Red Crescent Medical Journal. 2014; 16(6):e17173. [DOI:10.5812/ircmj.17173] [PMID] [PMCID]
- Kasser SL, Jacobs JV, Ford M, Tourville TW. Effects of balance-specific exercises on balance, physical activity and quality of life in adults with multiple sclerosis: A pilot investigation. Disability and Rehabilitation. 2015; 37(24):2238-49. [DOI:10.3109/09638288.2015.1019008] [PMID]
Type of Study: Research |
Subject:
Sport injury and corrective exercises
Received: 2024/06/7 | Accepted: 2024/09/1 | Published: 2024/01/13
Received: 2024/06/7 | Accepted: 2024/09/1 | Published: 2024/01/13
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
