Mon, Jul 27, 2026
Volume 16, Issue 1 (Winter 2026)
PTJ 2026, 16(1): 105-114 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Rahimi M, Dehghani M, Rahnama A. Investigation of Musculoskeletal Disorders and Their Relationship with Work Posture and Experience in Female Tailors. PTJ 2026; 16 (1) :105-114
URL: http://ptj.uswr.ac.ir/article-1-641-en.html
URL: http://ptj.uswr.ac.ir/article-1-641-en.html



1- Department of Corrective Exercises and Sport Injuries, Faculty of Sport Sciences, Shahid Rajaee Teacher Training University, Tehran, Iran.
Full-Text [PDF 526 kb]
(639 Downloads)
| Abstract (HTML) (2341 Views)
Full-Text: (212 Views)
Introduction
The tailoring profession is characterized by repetitive movements, constrained postures, and prolonged standing, all of which are recognized as major ergonomic risk factors for occupation-related musculoskeletal disorders (OMSDs) [1]. OMSDs are among the most prevalent occupational injuries and causes of disability in both developed and developing countries, with a higher prevalence among women than men [2]. OMSDs typically affect the lower back, neck, and upper extremities. These disorders represent the most common occupational injuries, leading to significant work loss and disability. The prevalence of these conditions results in decreased productivity and quality of work, increased healthcare costs, increased absenteeism, and premature disability [3].
Various risk factors contribute to the development of OMSDs, which can be categorized into physical risk factors, such as poor posture, lifting and carrying heavy loads, and repetitive tasks, and psychosocial and individual risk factors [4]. Among physical factors and risk factors, poor posture is considered one of the most significant, and various methods have been proposed for its assessment. Among the ergonomic assessment techniques presented, observational methods based on pen and paper have particular advantages, as they do not require specialized equipment or tools and allow for quick evaluation in a short period [3].
Tailoring is an occupation with a high prevalence of OMSDs. Tailors are required to sit for long periods with their heads bent over sewing machines, demanding high levels of precision and focus. Additionally, the repetitive nature of their work contributes to a high prevalence of OMSD symptoms in the neck and shoulders. A one-year study in Sweden reported a 75% prevalence of neck and shoulder pain among tailors. Similarly, in a study of garment production workers in Los Angeles, 24% of tailors reported neck and shoulder pain, and 16% reported pain in the distal upper extremities [5]. Ekechukwu et al. reported the highest prevalence of OMSDs among tailors in Inogou City in the scapula (43%), followed by the low back (36%) and knees (23%) [1]. Jalali et al. found a prevalence of OMSDs in the upper extremities of tailors, specifically in the wrist and palm (42%), fingers (27%), shoulder (20%), and elbow (10%) [6]. Studies have demonstrated a strong link between posture and workstation design, suggesting that posture problems can stem from improper workstation design. Etemadi Nejad et al. [5]investigated the standardization of tailors’ tables and chairs, and the results showed that using a sewing table with a 5-10 degree tilt significantly reduced shoulder and neck muscle activity. However, this reduction was only significant when comparing the conventional workstation to the new one, and no significant difference was observed among the different configurations of the new workstations. This could be attributed to the need for further optimization of the workstation design or the influence of individual factors. One reason for this issue is the lack of instruction on correct posture for individuals.
Research also shows that with increasing age, body dimensions, muscle strength, and upper extremity range of motion decrease, making individuals more susceptible to OMSDs [7]. Prolonged exposure to repetitive tasks over an extended period, often associated with increased work experience and advancing age, can lead to the wear and tear of body components, akin to the deterioration of a mechanical machine. This deterioration manifests as OMSDs, a prevalent health concern [8]. A study by Jalali et al. established a direct correlation between age and work experience and the prevalence of upper extremity disorders [6]. The nature of tailoring tasks appears to predispose individuals to OMSDs in the upper extremities and ankle regions. These disorders can lead to decreased work efficiency, impaired performance, increased fatigue, increased absenteeism, and work-related disability retirement among tailors. Therefore, considering the significance of addressing the health needs of tailors, who are predominantly women, this study aimed to investigate the prevalence of OMSDs and common working postures, as well as their association with work experience, to determine the health needs of this population.
Materials and Methods
This study employed a descriptive cross-sectional research design. The study population comprised female tailors in Isfahan City, Iran. Participants were selected using convenience sampling and were included based on pre-determined inclusion and exclusion criteria.
Inclusion criteria encompassed the absence of a history of surgery or fractures in the upper or lower extremities, the absence of congenital abnormalities or disorders affecting the upper or lower extremities, and a minimum of 5 years of experience in tailoring. Exclusion criteria included incomplete questionnaires and participant non-compliance during data collection [9]. In order to obtain informed consent, the study’s objectives were explained to the eligible participants, and they were informed that participation in the research was voluntary. They were also assured that their information would be kept confidential.
To assess the prevalence of OMSDs, the nordic musculoskeletal questionnaire was employed. The nordic musculoskeletal questionnaire was developed and validated in 1987 by Ekechukwu et al. at the Scandinavian occupational health institute [1, 10]. This widely used questionnaire comprises 11 items and consists of two sections: A general questionnaire and a specific questionnaire [11]. Participants can complete the Nordic Musculoskeletal questionnaire using self-report methods via paper, Internet, or telephone, or through an interview. The nordic musculoskeletal questionnaire presents a visual representation of the human body with nine anatomical regions to assist participants in marking the areas of their body where they experienced symptoms of pain, discomfort, or numbness within the past 7 days and 12 months. Responses are indicated using a yes/no format. The general questionnaire aims for a comprehensive evaluation, addressing OMSD symptoms throughout the body, while the specific questionnaire delves into a deeper analysis of these symptoms in specific body regions, including the neck, shoulders, low back, wrists, and hands [11]. The nordic musculoskeletal questionnaire has demonstrated test-re-test reliability and validity of 0.73 and 0.8, respectively. Its sensitivity and specificity range from 66-92% and 71-88%, respectively [1]. The Persian version of the Nordic musculoskeletal questionnaire was validated by Mokhtarinia et al. and exhibited good reliability (ICC=0.70) [11].
The rapid entire body assessment (REBA) method was employed to evaluate the postures of the participants at their workstations. Developed in 2000 by Hignet et al. the REBA method is a comprehensive body assessment tool that provides a simultaneous analysis of the upper extremities (arms, forearms, and wrists), trunk, neck, and legs [12]. This method also considers additional factors, such as force or load exerted, type of grip, and muscular activity during the evaluation [13]. The REBA method is particularly suitable for assessing occupations involving static or dynamic postures and frequent postural changes. In the REBA method, the posture or activity to be evaluated is first selected and then coded using the provided diagrams. The posture score for each body part is combined with the force exertion and activity type scores to determine the overall risk of musculoskeletal injury. The priority levels for corrective actions suggested by this method indicate the need for ergonomic intervention programs. The present study investigated the association between the overall REBA score, ranging from 1 to 15, and musculoskeletal disorders.
Statistical analysis
Descriptive statistics, including mean, standard deviation, frequency, cumulative frequency, minimum, and maximum, were employed to describe the data. The Kolmogorov-Smirnov test, skewness, and kurtosis were used to assess the normality of data distribution. Spearman’s correlation coefficient was utilized to examine the associations between the study variables. All statistical analyses were performed using SPSS software, version 25 with a significance level of P>0.05. Microsoft Excel was used to generate graphical representations.
Results
The Kolmogorov-Smirnov test revealed that the data did not follow a normal distribution (P<0.05). Therefore, Spearman’s correlation coefficient was employed to examine the associations between musculoskeletal disorders, work experience, and REBA scores. Table 1 presents the demographic characteristics of the study participants.
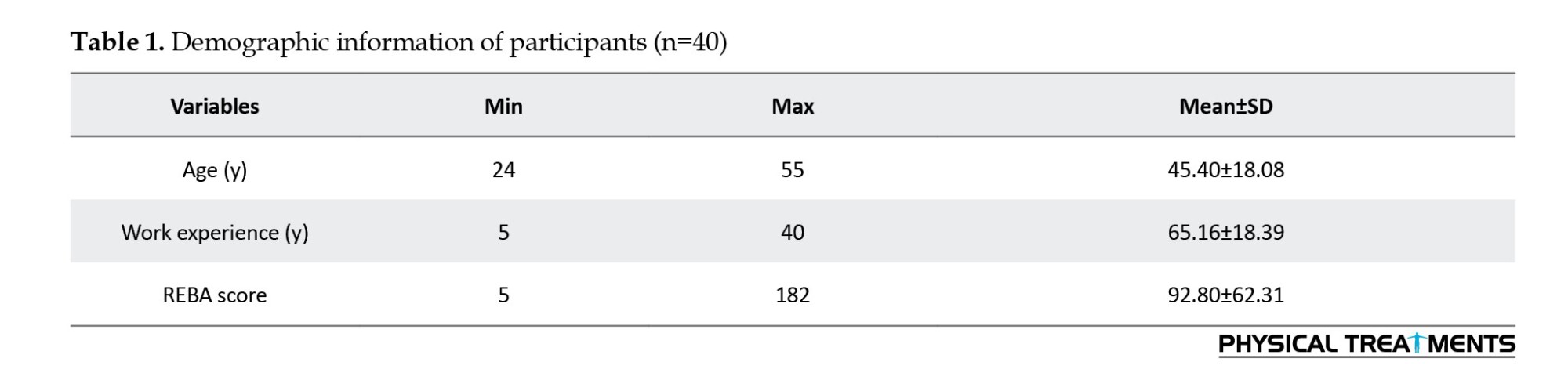
Table 2 reports the final scores, percentage frequencies, and risk levels in the REBA assessment. Based on this, 8 out of 40 subjects are facing a medium risk level and need urgent action. Twenty-seven individuals had a high risk level that requires urgent action as soon as possible, and 5 individuals had a very high risk level that requires immediate action.
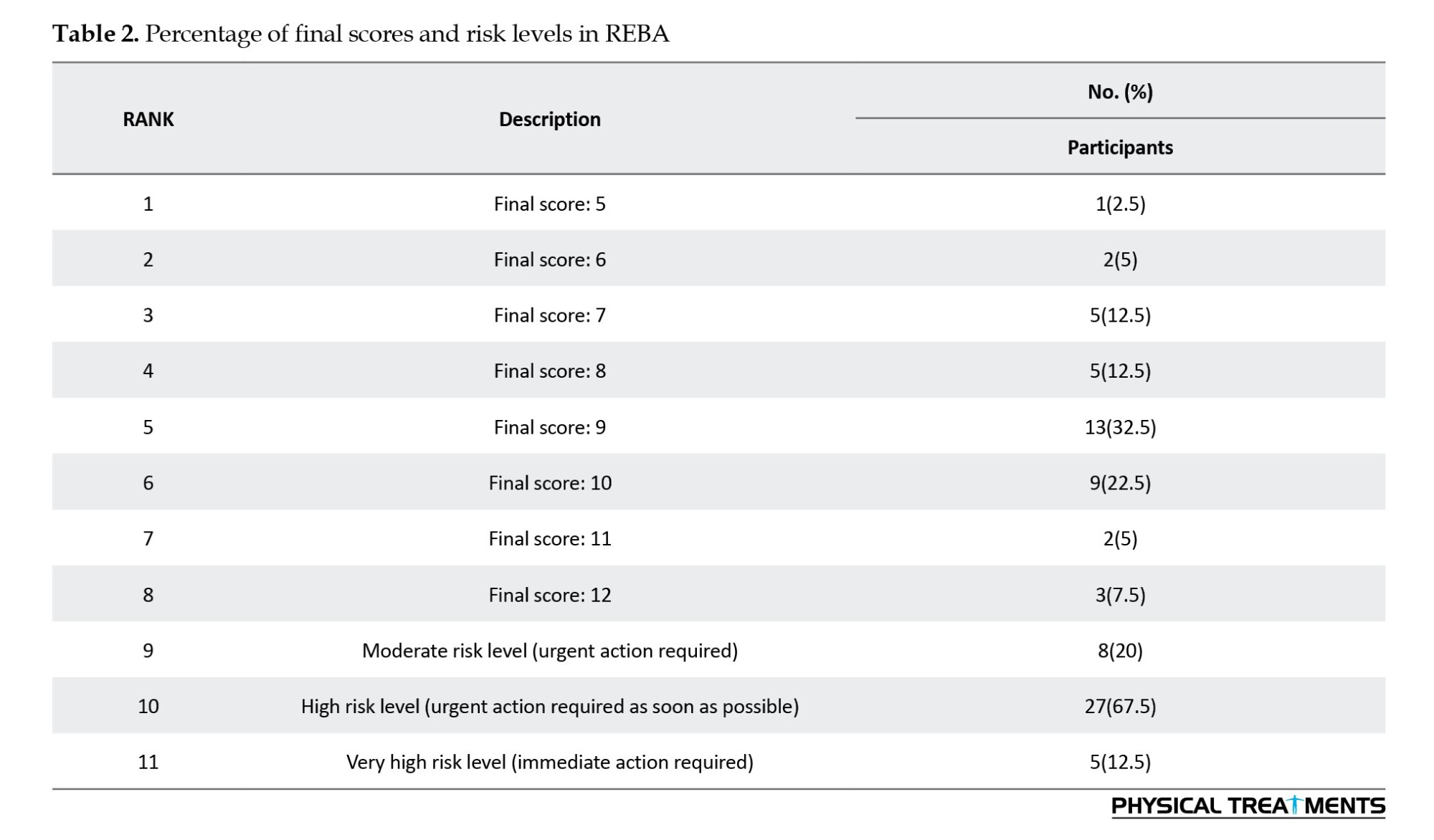
Figure 1 illustrates the prevalence of OMSDs experienced by the study participants in the past 12 months. According to the figure, 92.5% of the participants reported OMSDs in the lumbar region, 62.5% in the neck region, 57.5% in the shoulder region, 45% in the scapular and knee regions, 27.5% in the elbow and pelvic regions, 25% in the wrist region, and 15% in the ankle region.
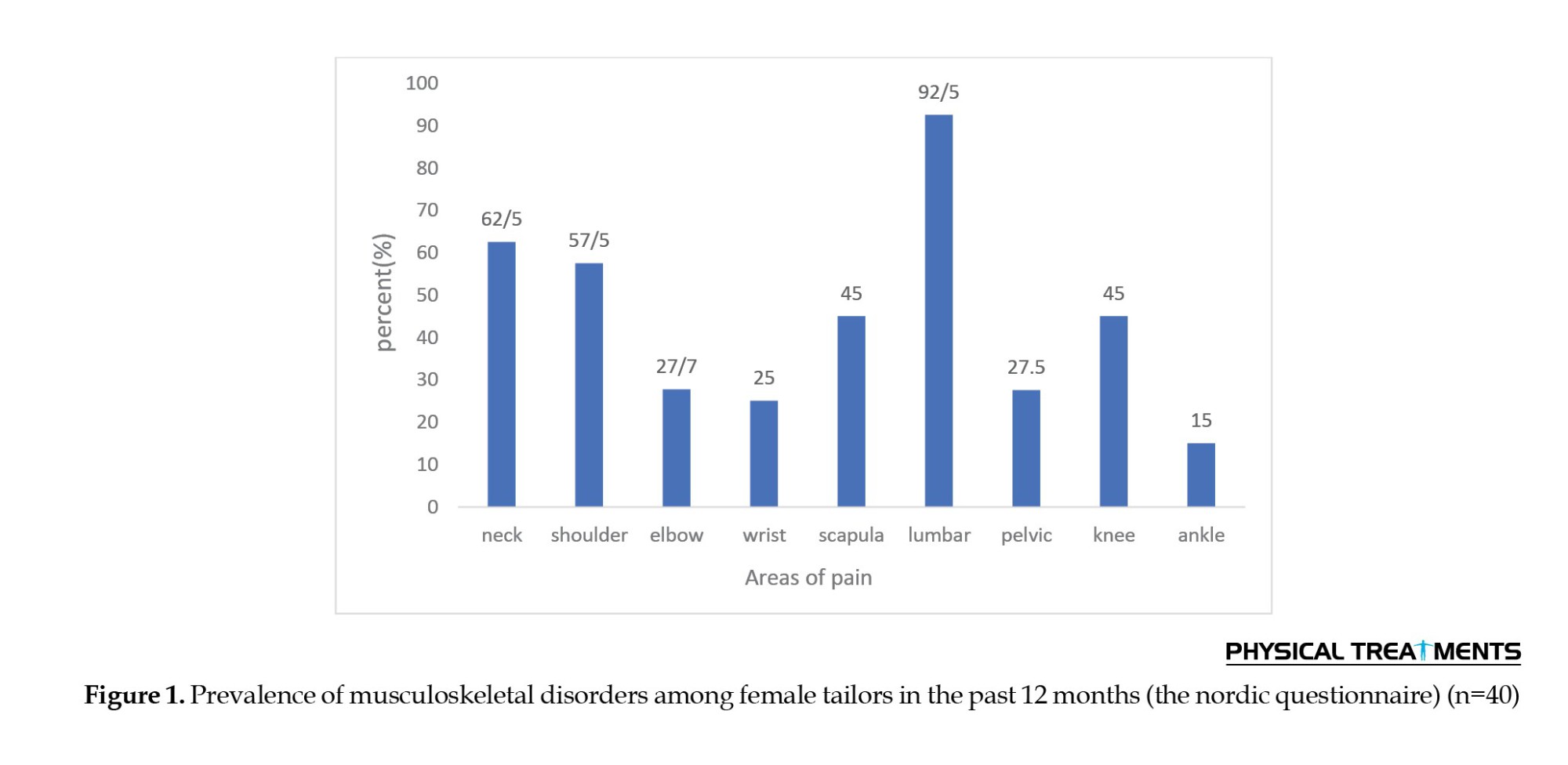
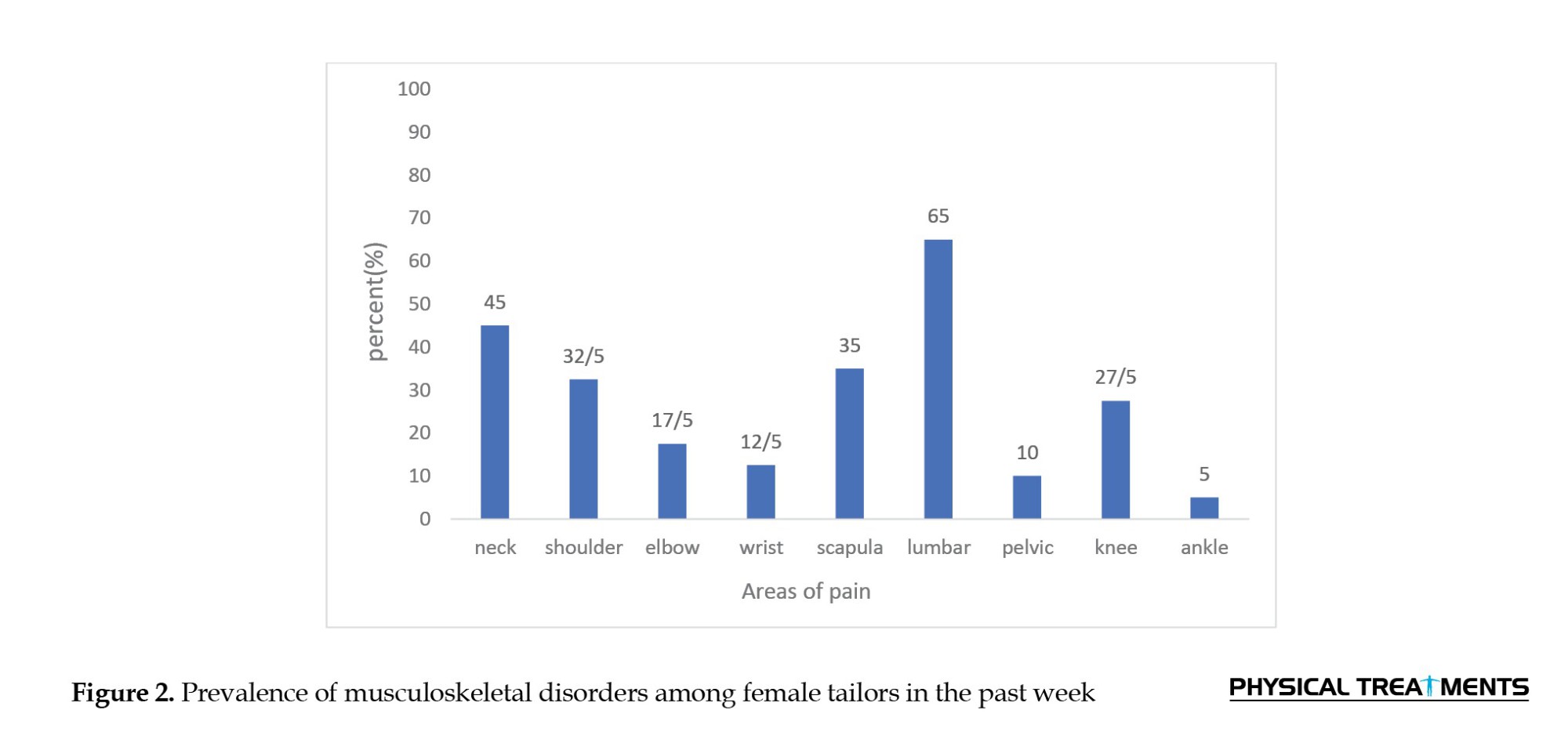
Figure 2 illustrates the prevalence of MSDs among study subjects in the past week. Specifically, 65% of the subjects reported MSDs in the lower back, 45% in the neck, 32.5% in the shoulder, 35% in the shoulder and knee regions, 27.5% in the elbow, 17.5% in the pelvic, 10% in the wrist, and 12.5% in the ankle.
Figures 2 and 3 also depicts the current prevalence of OMSDs among the study participants. As shown in the figure, 57.5% of the participants reported current OMSDs in the lumbar region, 25% in the neck region, 20% in the shoulder region, 12.5% in the scapular region, 7.5% in the knee and wrist regions, 5% in the ankle region, and 5% in the elbow region.
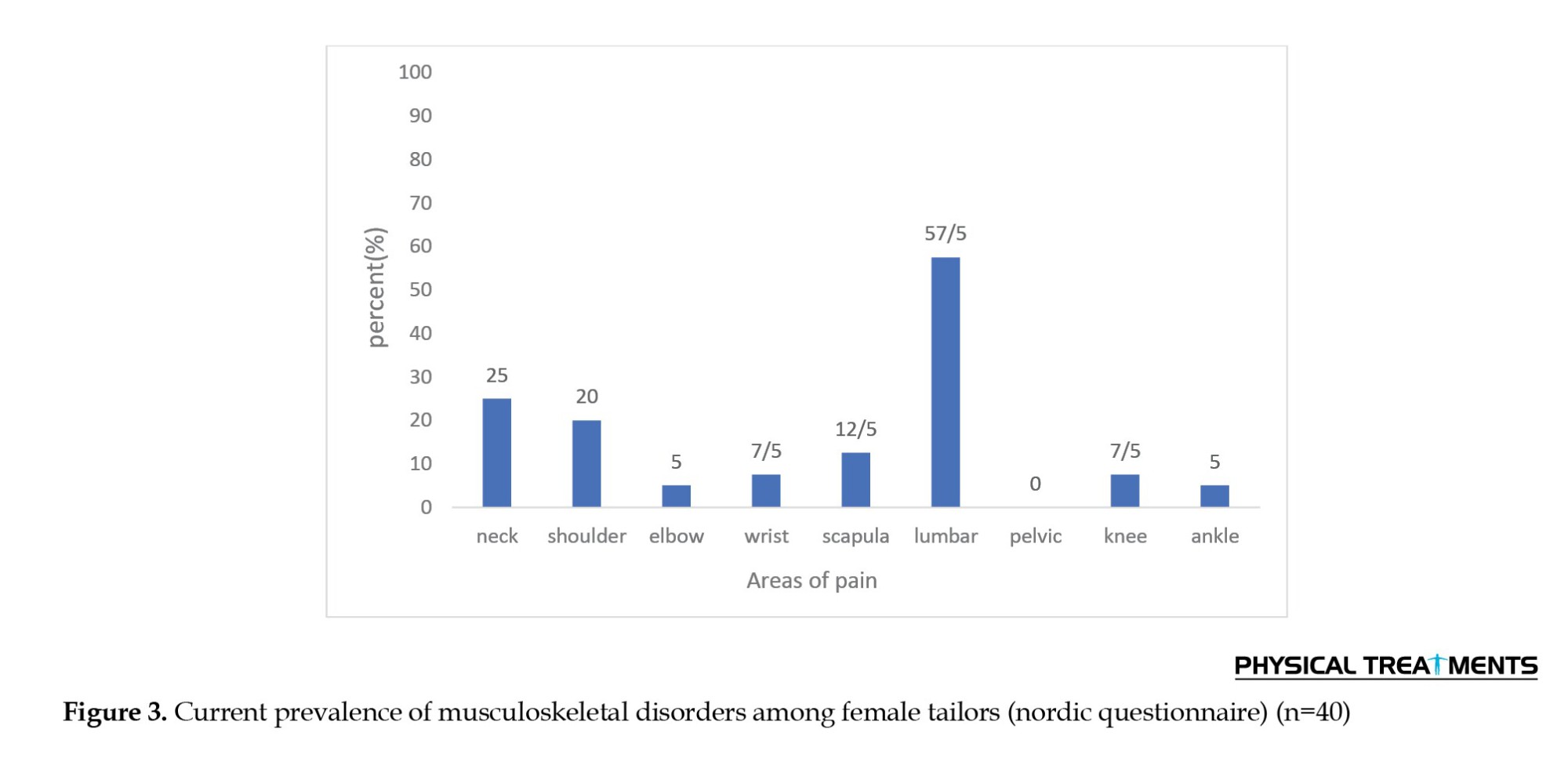
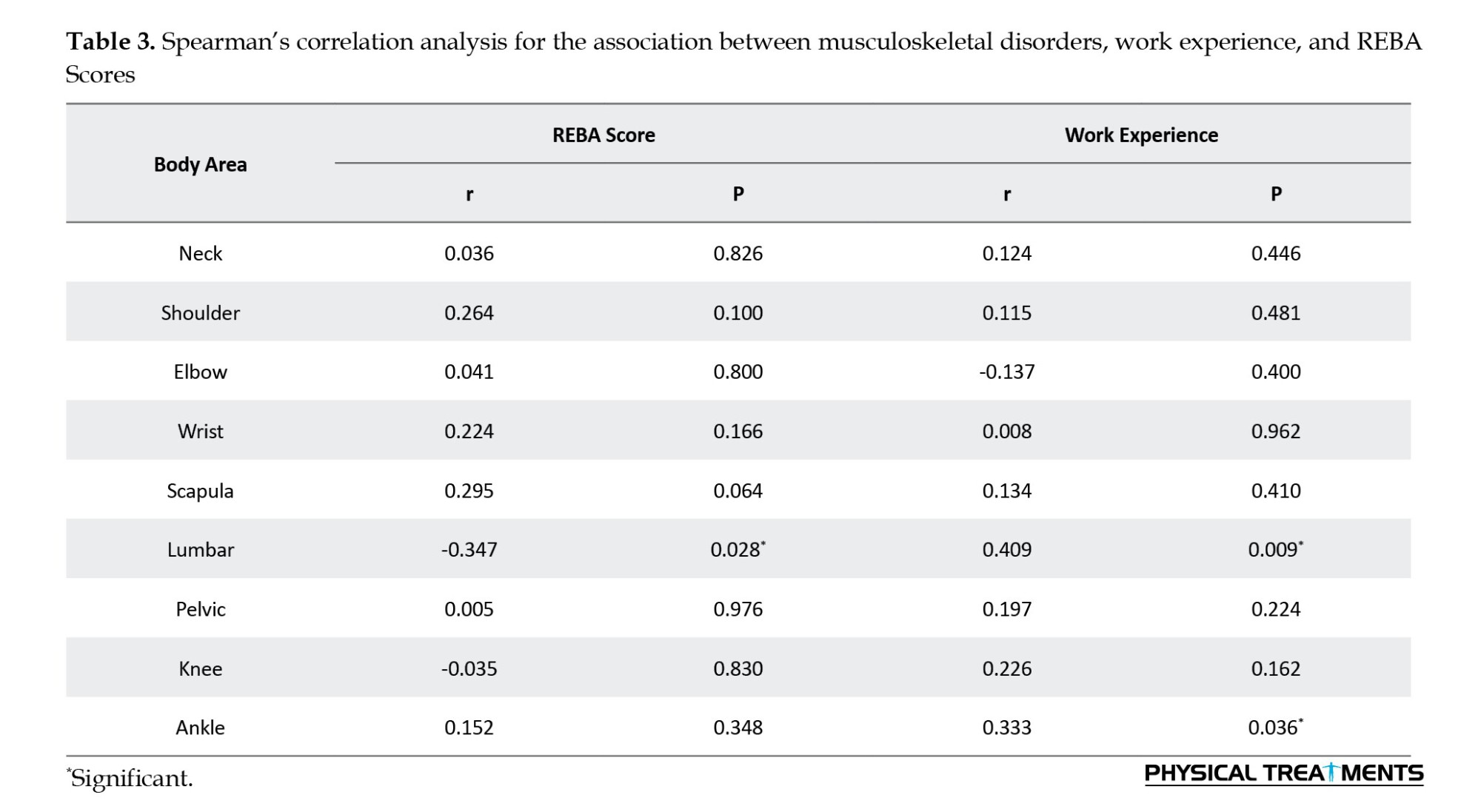
The findings further revealed a significant inverse association between MSDs in the lumbar region and work experience (P=0.028). Additionally, a significant positive association was observed between OMSDs in the lumbar region (P=0.009) and the ankle region (P=0.036) and REBA scores. No significant associations were found between the other study variables.
Discussion
The present study aimed to investigate the prevalence of OMSDs among female tailors in Isfahan City and their association with work posture and work experience. The findings revealed a significant inverse association between OMSDs in the lumbar region and work experience, as well as a significant positive association between OMSDs in the lumbar and ankle regions with REBA scores. No significant associations were found between the other study variables. Additionally, the lumbar, neck, shoulder, scapula, and knee regions were the most prevalent sites of OMSDs. The highest prevalence rates of injuries in the past 12 months were observed in the lumbar (92.5%), neck (62.5%), shoulder (57.5%), scapula, and knee regions (45%). Additionally, the highest prevalence rates in the past week were found in the lumbar (65%), neck (45%), and scapula (35%) regions. Currently, the highest prevalence rates were noted in the lumbar (57.5%), neck (25%), and shoulder (20%) regions. The findings of the present study are consistent with those of previous investigations by Ekechukwu et al. [1], Bashtani et al. [13], Schibye et al. [14], Kaergaard & Andersen [15], Dianat et al. [16], Öztürk et al. [17], Afifezadeh et al. [18], and Rahimi et al. [19].
Various domestic and international studies have been conducted to investigate MSDs among tailors. For instance, Schibye et al. conducted a study to assess the prevalence of OMSDs in 327 sewing machine operators using the Nordic Questionnaire. Their findings revealed the highest prevalence of pain symptoms and disorders in the shoulder and neck regions [14]. In a similar study, Kaergaard & Andersen assessed 243 female sewing machine operators. The findings revealed a prevalence of 15.2% for carpal tunnel syndrome and 5.8% for tenosynovitis of the intrinsic rotator muscles of the wrist. These rates were significantly higher compared to those in the control group (9% and 2.2%, respectively). The results suggested that in addition to work experience, pre-existing disorders, age, body mass index, smoking, and previous strain also contribute to the occurrence of these disorders [15].
Dianat et al. reported the highest prevalence of MSDs among sewing machine operators in the following regions: Lumbar (85%), neck (76%), hands and wrists (53%), and scapula (48%) [16]. In the study by Öztürk et al. [17] the highest prevalence of MSDs among tailors was observed in the trunk (62.5%), neck (50.5%), and shoulder (50.2%) regions. Additionally, 65% of female participants in the study had experienced musculoskeletal pain and discomfort in the past 6 months. The final REBA score in this study indicated an immediate need for workstation modifications. The findings also revealed that female tailors were not only exposed to a high level of ergonomic risk factors but also experienced a high prevalence of OMSDs [17].
Afifezadeh et al. investigated sewing machine operators and found that the highest prevalence of symptoms over 12 months was in the lumbar region, with a prevalence of 54.9% [18]. Using the OWAS method, Tüzün et al. studied female tailors and found that over 50% of female workers in this profession were exposed to ergonomic hazards [19]. Ekechukwu et al. reported an estimated prevalence of 67% for OMSDs in their study population. MSDs were most prevalent in the scapula (43%), lumbar (36.3%), and knee (23.3%) regions [1]. This study also demonstrated a significant association between OMSD prevalence and fatigue and age [1].
In the tailoring profession, shoulder and forearm muscles are often subjected to static postures and excessive use. This can lead to premature fatigue due to lactic acid accumulation in these muscles and impaired blood circulation. A study by Mohammad Hamed Hosseini in 2003 suggested that static shoulder activity among dentists could be a contributing factor to the prevalence of shoulder muscle disorders [6]. Therefore, it is recommended to implement rest breaks between activities to enhance recovery time and adjust worktable heights to reduce static postures associated with job tasks, thereby mitigating the occurrence of related complications. The muscles of the upper body are constantly engaged in maintaining posture during work, which is one of the reasons for OMSDs among tailors. In most occupational groups, the highest prevalence of symptoms is reported in the lumbar region. This can be attributed to the unique and delicate anatomy of the spine, as well as the influence of various individual, physical, and psychosocial factors, such as age, gender, education level, smoking habits, occupational predisposing factors, such as poor body postures, non-adherence to ergonomic principles in workstation design, improper lifting and carrying of heavy loads, excessive stress, and job dissatisfaction [20].
The findings of the present study were inconsistent with those of Jalali et al. who reported the highest prevalence of disorders in the wrist and palm regions. A potential explanation for this discrepancy and the decline in the prevalence of wrist and palm disorders to lower ranks in the present study may be attributed to technological advancements and the mechanization of tailoring tasks over the past two decades [6].
In the study by Jalali et al. [6] the body postures of tailors, saddlers, and carpet weavers during work were assessed using the OCRA method and the Nordic questionnaire. The results revealed that the prevalence of MSDs among tailors was 42.4% in the wrist and palm regions, 27.1% in the fingers, 20.3% in the shoulder, and 10.2% in the elbow [6].
Jafari et al.’s research was consistent with the present study regarding posture at work [2]. In the present study, the final REBA score was 8.92, with 67.5% of participants classified as high risk and 12.5% as very high risk. These individuals exhibited a higher percentage of symptoms in all body regions. Table 3 demonstrates a significant positive correlation between MSDs in the lumbar and ankle regions and the REBA score.
Jafari et al. investigated the impact of ergonomic training on the work posture of tailors. In this study, the final REBA score was reported as 9.6, with 51.4% of individuals falling into the posture score category of 7. After providing posture training to tailors, this percentage was reduced to 19.2% [2]. Therefore, posture training plays a crucial role in reducing occupation-related risk and safeguarding worker health. However, the extent to which posture correction can effectively mitigate MSDs remains a topic of debate.
Etemadi Nejad et al. examined the influence of workstations on the muscle activity of the shoulder and neck regions in tailors. Following adjustments to the table height and incline, the muscles under investigation exhibited reduced activity levels [5]. Nonetheless, the health history and physical activity levels of individuals should also be considered. Research suggests that individuals with low physical activity levels and weak muscles experience insufficient muscular support for their spines and bones.
Therefore, in addition to providing training on proper posture during work and modifying workstations, exercise protocols focusing on strengthening the core stabilizing muscles and shoulder girdle are strongly recommended for tailors. This approach aims to enhance the ability to maintain proper posture consistently and reduce strain on the spine and shoulder joints.
Conclusion
The high prevalence of OMSDs, particularly in the lumbar and neck regions, and their significant correlation with REBA scores underscore the need for ergonomic interventions and improved work posture in this profession. The inverse relationship between disorders and work experience suggests that newcomers may be unaware of the risk factors associated with work posture, while experienced individuals may have adopted strategies to mitigate pain and disorders. The relatively high REBA scores in this study highlight the poor design of tailoring workstations and indicate the necessity of posture correction during work and ergonomic workstation improvements. The practical significance of these findings lies in the prevention of disorders, the introduction of preventive techniques and corrective exercises, and the education and awareness of tailors to reduce risks and improve working conditions.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of the Sport Sciences Research Institute (Code: SSRI.REC-2205-1659[R2]), the research objectives were explained to the participants. Individuals voluntarily participated in the study with full knowledge and consent by completing a consent form. They were free to withdraw from the study at any stage of the research if they chose not to continue.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Data collection and review: Maryam Dehghani; Data analysis: Afsaane Rahnama and Maryam Dehghani; Manuscript preparation: Mohammad Rahimi, Afsaane Rahnama
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgments
The authors would like to thank all the participants who completed the questionnaires and the loved ones who assisted us in the implementation of this project. We hope that measures will be taken to reduce musculoskeletal disorders and common abnormalities among tailors.
Reference
The tailoring profession is characterized by repetitive movements, constrained postures, and prolonged standing, all of which are recognized as major ergonomic risk factors for occupation-related musculoskeletal disorders (OMSDs) [1]. OMSDs are among the most prevalent occupational injuries and causes of disability in both developed and developing countries, with a higher prevalence among women than men [2]. OMSDs typically affect the lower back, neck, and upper extremities. These disorders represent the most common occupational injuries, leading to significant work loss and disability. The prevalence of these conditions results in decreased productivity and quality of work, increased healthcare costs, increased absenteeism, and premature disability [3].
Various risk factors contribute to the development of OMSDs, which can be categorized into physical risk factors, such as poor posture, lifting and carrying heavy loads, and repetitive tasks, and psychosocial and individual risk factors [4]. Among physical factors and risk factors, poor posture is considered one of the most significant, and various methods have been proposed for its assessment. Among the ergonomic assessment techniques presented, observational methods based on pen and paper have particular advantages, as they do not require specialized equipment or tools and allow for quick evaluation in a short period [3].
Tailoring is an occupation with a high prevalence of OMSDs. Tailors are required to sit for long periods with their heads bent over sewing machines, demanding high levels of precision and focus. Additionally, the repetitive nature of their work contributes to a high prevalence of OMSD symptoms in the neck and shoulders. A one-year study in Sweden reported a 75% prevalence of neck and shoulder pain among tailors. Similarly, in a study of garment production workers in Los Angeles, 24% of tailors reported neck and shoulder pain, and 16% reported pain in the distal upper extremities [5]. Ekechukwu et al. reported the highest prevalence of OMSDs among tailors in Inogou City in the scapula (43%), followed by the low back (36%) and knees (23%) [1]. Jalali et al. found a prevalence of OMSDs in the upper extremities of tailors, specifically in the wrist and palm (42%), fingers (27%), shoulder (20%), and elbow (10%) [6]. Studies have demonstrated a strong link between posture and workstation design, suggesting that posture problems can stem from improper workstation design. Etemadi Nejad et al. [5]investigated the standardization of tailors’ tables and chairs, and the results showed that using a sewing table with a 5-10 degree tilt significantly reduced shoulder and neck muscle activity. However, this reduction was only significant when comparing the conventional workstation to the new one, and no significant difference was observed among the different configurations of the new workstations. This could be attributed to the need for further optimization of the workstation design or the influence of individual factors. One reason for this issue is the lack of instruction on correct posture for individuals.
Research also shows that with increasing age, body dimensions, muscle strength, and upper extremity range of motion decrease, making individuals more susceptible to OMSDs [7]. Prolonged exposure to repetitive tasks over an extended period, often associated with increased work experience and advancing age, can lead to the wear and tear of body components, akin to the deterioration of a mechanical machine. This deterioration manifests as OMSDs, a prevalent health concern [8]. A study by Jalali et al. established a direct correlation between age and work experience and the prevalence of upper extremity disorders [6]. The nature of tailoring tasks appears to predispose individuals to OMSDs in the upper extremities and ankle regions. These disorders can lead to decreased work efficiency, impaired performance, increased fatigue, increased absenteeism, and work-related disability retirement among tailors. Therefore, considering the significance of addressing the health needs of tailors, who are predominantly women, this study aimed to investigate the prevalence of OMSDs and common working postures, as well as their association with work experience, to determine the health needs of this population.
Materials and Methods
This study employed a descriptive cross-sectional research design. The study population comprised female tailors in Isfahan City, Iran. Participants were selected using convenience sampling and were included based on pre-determined inclusion and exclusion criteria.
Inclusion criteria encompassed the absence of a history of surgery or fractures in the upper or lower extremities, the absence of congenital abnormalities or disorders affecting the upper or lower extremities, and a minimum of 5 years of experience in tailoring. Exclusion criteria included incomplete questionnaires and participant non-compliance during data collection [9]. In order to obtain informed consent, the study’s objectives were explained to the eligible participants, and they were informed that participation in the research was voluntary. They were also assured that their information would be kept confidential.
To assess the prevalence of OMSDs, the nordic musculoskeletal questionnaire was employed. The nordic musculoskeletal questionnaire was developed and validated in 1987 by Ekechukwu et al. at the Scandinavian occupational health institute [1, 10]. This widely used questionnaire comprises 11 items and consists of two sections: A general questionnaire and a specific questionnaire [11]. Participants can complete the Nordic Musculoskeletal questionnaire using self-report methods via paper, Internet, or telephone, or through an interview. The nordic musculoskeletal questionnaire presents a visual representation of the human body with nine anatomical regions to assist participants in marking the areas of their body where they experienced symptoms of pain, discomfort, or numbness within the past 7 days and 12 months. Responses are indicated using a yes/no format. The general questionnaire aims for a comprehensive evaluation, addressing OMSD symptoms throughout the body, while the specific questionnaire delves into a deeper analysis of these symptoms in specific body regions, including the neck, shoulders, low back, wrists, and hands [11]. The nordic musculoskeletal questionnaire has demonstrated test-re-test reliability and validity of 0.73 and 0.8, respectively. Its sensitivity and specificity range from 66-92% and 71-88%, respectively [1]. The Persian version of the Nordic musculoskeletal questionnaire was validated by Mokhtarinia et al. and exhibited good reliability (ICC=0.70) [11].
The rapid entire body assessment (REBA) method was employed to evaluate the postures of the participants at their workstations. Developed in 2000 by Hignet et al. the REBA method is a comprehensive body assessment tool that provides a simultaneous analysis of the upper extremities (arms, forearms, and wrists), trunk, neck, and legs [12]. This method also considers additional factors, such as force or load exerted, type of grip, and muscular activity during the evaluation [13]. The REBA method is particularly suitable for assessing occupations involving static or dynamic postures and frequent postural changes. In the REBA method, the posture or activity to be evaluated is first selected and then coded using the provided diagrams. The posture score for each body part is combined with the force exertion and activity type scores to determine the overall risk of musculoskeletal injury. The priority levels for corrective actions suggested by this method indicate the need for ergonomic intervention programs. The present study investigated the association between the overall REBA score, ranging from 1 to 15, and musculoskeletal disorders.
Statistical analysis
Descriptive statistics, including mean, standard deviation, frequency, cumulative frequency, minimum, and maximum, were employed to describe the data. The Kolmogorov-Smirnov test, skewness, and kurtosis were used to assess the normality of data distribution. Spearman’s correlation coefficient was utilized to examine the associations between the study variables. All statistical analyses were performed using SPSS software, version 25 with a significance level of P>0.05. Microsoft Excel was used to generate graphical representations.
Results
The Kolmogorov-Smirnov test revealed that the data did not follow a normal distribution (P<0.05). Therefore, Spearman’s correlation coefficient was employed to examine the associations between musculoskeletal disorders, work experience, and REBA scores. Table 1 presents the demographic characteristics of the study participants.
Table 2 reports the final scores, percentage frequencies, and risk levels in the REBA assessment. Based on this, 8 out of 40 subjects are facing a medium risk level and need urgent action. Twenty-seven individuals had a high risk level that requires urgent action as soon as possible, and 5 individuals had a very high risk level that requires immediate action.
Figure 1 illustrates the prevalence of OMSDs experienced by the study participants in the past 12 months. According to the figure, 92.5% of the participants reported OMSDs in the lumbar region, 62.5% in the neck region, 57.5% in the shoulder region, 45% in the scapular and knee regions, 27.5% in the elbow and pelvic regions, 25% in the wrist region, and 15% in the ankle region.
Figure 2 illustrates the prevalence of MSDs among study subjects in the past week. Specifically, 65% of the subjects reported MSDs in the lower back, 45% in the neck, 32.5% in the shoulder, 35% in the shoulder and knee regions, 27.5% in the elbow, 17.5% in the pelvic, 10% in the wrist, and 12.5% in the ankle.
Figures 2 and 3 also depicts the current prevalence of OMSDs among the study participants. As shown in the figure, 57.5% of the participants reported current OMSDs in the lumbar region, 25% in the neck region, 20% in the shoulder region, 12.5% in the scapular region, 7.5% in the knee and wrist regions, 5% in the ankle region, and 5% in the elbow region.
The findings further revealed a significant inverse association between MSDs in the lumbar region and work experience (P=0.028). Additionally, a significant positive association was observed between OMSDs in the lumbar region (P=0.009) and the ankle region (P=0.036) and REBA scores. No significant associations were found between the other study variables.
Discussion
The present study aimed to investigate the prevalence of OMSDs among female tailors in Isfahan City and their association with work posture and work experience. The findings revealed a significant inverse association between OMSDs in the lumbar region and work experience, as well as a significant positive association between OMSDs in the lumbar and ankle regions with REBA scores. No significant associations were found between the other study variables. Additionally, the lumbar, neck, shoulder, scapula, and knee regions were the most prevalent sites of OMSDs. The highest prevalence rates of injuries in the past 12 months were observed in the lumbar (92.5%), neck (62.5%), shoulder (57.5%), scapula, and knee regions (45%). Additionally, the highest prevalence rates in the past week were found in the lumbar (65%), neck (45%), and scapula (35%) regions. Currently, the highest prevalence rates were noted in the lumbar (57.5%), neck (25%), and shoulder (20%) regions. The findings of the present study are consistent with those of previous investigations by Ekechukwu et al. [1], Bashtani et al. [13], Schibye et al. [14], Kaergaard & Andersen [15], Dianat et al. [16], Öztürk et al. [17], Afifezadeh et al. [18], and Rahimi et al. [19].
Various domestic and international studies have been conducted to investigate MSDs among tailors. For instance, Schibye et al. conducted a study to assess the prevalence of OMSDs in 327 sewing machine operators using the Nordic Questionnaire. Their findings revealed the highest prevalence of pain symptoms and disorders in the shoulder and neck regions [14]. In a similar study, Kaergaard & Andersen assessed 243 female sewing machine operators. The findings revealed a prevalence of 15.2% for carpal tunnel syndrome and 5.8% for tenosynovitis of the intrinsic rotator muscles of the wrist. These rates were significantly higher compared to those in the control group (9% and 2.2%, respectively). The results suggested that in addition to work experience, pre-existing disorders, age, body mass index, smoking, and previous strain also contribute to the occurrence of these disorders [15].
Dianat et al. reported the highest prevalence of MSDs among sewing machine operators in the following regions: Lumbar (85%), neck (76%), hands and wrists (53%), and scapula (48%) [16]. In the study by Öztürk et al. [17] the highest prevalence of MSDs among tailors was observed in the trunk (62.5%), neck (50.5%), and shoulder (50.2%) regions. Additionally, 65% of female participants in the study had experienced musculoskeletal pain and discomfort in the past 6 months. The final REBA score in this study indicated an immediate need for workstation modifications. The findings also revealed that female tailors were not only exposed to a high level of ergonomic risk factors but also experienced a high prevalence of OMSDs [17].
Afifezadeh et al. investigated sewing machine operators and found that the highest prevalence of symptoms over 12 months was in the lumbar region, with a prevalence of 54.9% [18]. Using the OWAS method, Tüzün et al. studied female tailors and found that over 50% of female workers in this profession were exposed to ergonomic hazards [19]. Ekechukwu et al. reported an estimated prevalence of 67% for OMSDs in their study population. MSDs were most prevalent in the scapula (43%), lumbar (36.3%), and knee (23.3%) regions [1]. This study also demonstrated a significant association between OMSD prevalence and fatigue and age [1].
In the tailoring profession, shoulder and forearm muscles are often subjected to static postures and excessive use. This can lead to premature fatigue due to lactic acid accumulation in these muscles and impaired blood circulation. A study by Mohammad Hamed Hosseini in 2003 suggested that static shoulder activity among dentists could be a contributing factor to the prevalence of shoulder muscle disorders [6]. Therefore, it is recommended to implement rest breaks between activities to enhance recovery time and adjust worktable heights to reduce static postures associated with job tasks, thereby mitigating the occurrence of related complications. The muscles of the upper body are constantly engaged in maintaining posture during work, which is one of the reasons for OMSDs among tailors. In most occupational groups, the highest prevalence of symptoms is reported in the lumbar region. This can be attributed to the unique and delicate anatomy of the spine, as well as the influence of various individual, physical, and psychosocial factors, such as age, gender, education level, smoking habits, occupational predisposing factors, such as poor body postures, non-adherence to ergonomic principles in workstation design, improper lifting and carrying of heavy loads, excessive stress, and job dissatisfaction [20].
The findings of the present study were inconsistent with those of Jalali et al. who reported the highest prevalence of disorders in the wrist and palm regions. A potential explanation for this discrepancy and the decline in the prevalence of wrist and palm disorders to lower ranks in the present study may be attributed to technological advancements and the mechanization of tailoring tasks over the past two decades [6].
In the study by Jalali et al. [6] the body postures of tailors, saddlers, and carpet weavers during work were assessed using the OCRA method and the Nordic questionnaire. The results revealed that the prevalence of MSDs among tailors was 42.4% in the wrist and palm regions, 27.1% in the fingers, 20.3% in the shoulder, and 10.2% in the elbow [6].
Jafari et al.’s research was consistent with the present study regarding posture at work [2]. In the present study, the final REBA score was 8.92, with 67.5% of participants classified as high risk and 12.5% as very high risk. These individuals exhibited a higher percentage of symptoms in all body regions. Table 3 demonstrates a significant positive correlation between MSDs in the lumbar and ankle regions and the REBA score.
Jafari et al. investigated the impact of ergonomic training on the work posture of tailors. In this study, the final REBA score was reported as 9.6, with 51.4% of individuals falling into the posture score category of 7. After providing posture training to tailors, this percentage was reduced to 19.2% [2]. Therefore, posture training plays a crucial role in reducing occupation-related risk and safeguarding worker health. However, the extent to which posture correction can effectively mitigate MSDs remains a topic of debate.
Etemadi Nejad et al. examined the influence of workstations on the muscle activity of the shoulder and neck regions in tailors. Following adjustments to the table height and incline, the muscles under investigation exhibited reduced activity levels [5]. Nonetheless, the health history and physical activity levels of individuals should also be considered. Research suggests that individuals with low physical activity levels and weak muscles experience insufficient muscular support for their spines and bones.
Therefore, in addition to providing training on proper posture during work and modifying workstations, exercise protocols focusing on strengthening the core stabilizing muscles and shoulder girdle are strongly recommended for tailors. This approach aims to enhance the ability to maintain proper posture consistently and reduce strain on the spine and shoulder joints.
Conclusion
The high prevalence of OMSDs, particularly in the lumbar and neck regions, and their significant correlation with REBA scores underscore the need for ergonomic interventions and improved work posture in this profession. The inverse relationship between disorders and work experience suggests that newcomers may be unaware of the risk factors associated with work posture, while experienced individuals may have adopted strategies to mitigate pain and disorders. The relatively high REBA scores in this study highlight the poor design of tailoring workstations and indicate the necessity of posture correction during work and ergonomic workstation improvements. The practical significance of these findings lies in the prevention of disorders, the introduction of preventive techniques and corrective exercises, and the education and awareness of tailors to reduce risks and improve working conditions.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of the Sport Sciences Research Institute (Code: SSRI.REC-2205-1659[R2]), the research objectives were explained to the participants. Individuals voluntarily participated in the study with full knowledge and consent by completing a consent form. They were free to withdraw from the study at any stage of the research if they chose not to continue.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Data collection and review: Maryam Dehghani; Data analysis: Afsaane Rahnama and Maryam Dehghani; Manuscript preparation: Mohammad Rahimi, Afsaane Rahnama
Conflict of interest
The authors declared no conflicts of interest.
Acknowledgments
The authors would like to thank all the participants who completed the questionnaires and the loved ones who assisted us in the implementation of this project. We hope that measures will be taken to reduce musculoskeletal disorders and common abnormalities among tailors.
Reference
- Ekechukwu END, Okolo NC, Atueyi BC. Ergonomic evaluation and the predictors of occupation related musculoskeletal disorders among tailors in Enugu Metropolis. Journal of the Nigeria Society of Physiotherapy. 2021; 20(1):33-41. [DOI:10.5897/JNSP2021.0010]
- Jafari SM, Fazli B, Nurani M, Sharifpoor Z. [Risk assessment of musculoskeletal disorder by RULA method, and effect evaluation of ergonomic training on tailor working conditions (Persian)]. Occupational Medicine Quarterly Journal. 2013; 5(2):43-50. [Link]
- Ebrahimian H, Hokmabadi R, Shoja E. [Evaluation of ergonomic postures of dental professions by rapid entire body assessment (REBA) in North Khorasan, Iran (Persian)]. Journal of North Khorasan University of Medical Sciences. 2014; 5(5):961-7. [DOI:10.29252/jnkums.5.5.S5.961]
- Karami M, Ezabadi SG, Karami Z, Sahranavard Y. [Determining the prevalence of musculoskeletal injuries and its relationship with workplace posture in copper industry repairmen (Persian)]. Occupational Hygiene and Health Promotion. 2021; 5(3):1-9. [DOI:10.18502/ohhp.v5i3.7786]
- Etemadi Nejad S, Hosseininejad E, Yazdani Charati J, Ghaempanah F, Yousefi Chemazkati M, Amani A. [Effect of workstation designed for sewing, on neck and shoulder muscles of users (Persian)]. Iranian Journal of Ergonomics. 2020; 7(4):12-20. [DOI:10.30699/jergon.7.4.12]
- Jalali A, Nasle Seraji J. [The ergonomical study of the postures of doing in tailors, shoe makers, saddlers and carpet makers by OCRA analysis method (Persian)]. Iranian Journal of Forensic Medicine. 2006; 12(1):8-13. [Link]
- Trinkoff AM, Lipscomb JA, Geiger-Brown J, Brady B. Musculoskeletal problems of the neck, shoulder, and back and functional consequences in nurses. American Journal of Industrial Medicine. 2002; 41(3):170-8. [DOI:10.1002/ajim.10048] [PMID]
- Zarei F, Mousavifard SA, Ardestani M. [Assessment of musculoskeletal disorder prevalence and associated risk factors of a metal structure manufacturing company in Tehran (Persian)]. Journal of Environmental Health Engineering. 2016; 4(1):10-9. [Link]
- Shahmohammadi F, Rahimi M, Ghasemi A. [Investigation of musculoskeletal disorders in yutab factory and its relationship with posture at work, work experience and body mass index (Persian)]. Karafan. 2024; 21(2):599-612. [DOI:10.48301/kssa.2022.340560.2089]
- Nadri H, Nadri A, Rohani B, Fasih Ramandi F, Amin Sobhani M, Naseh I. [Assessment of musculoskeletal disorders prevalence and body discomfort among dentists by visual analog discomfort scale (Persian)]. Journal of Mashhad Dental School. 2015; 39(4):363-72. [DOI:10.22038/jmds.2015.5809]
- Mokhtarinia H, Shafiee A, Pashmdarfard M. [Translation and localization of the extended nordic musculoskeletal questionnaire and the evaluation of the face validity and test-retest reliability of its Persian version (Persian)]. Iranian Journal of Ergonomics. 2015; 3(3):21-9. [Link]
- Hignett S, McAtamney L. Rapid entire body assessment (REBA). Applied Ergonomics. 2000; 31(2):201-5. [DOI:10.1016/S0003-6870(99)00039-3] [PMID]
- Bashtani A, Amouzadeh E, Yazdani Cherati J, Etemadinezhad S, Kalateh Arabi H, Haji Omid K. [Investigating the effect of ergonomic interventions on work postures by REBA method in small workshops of Sabzevar city (Persian)]. Journal of Sabzevar University of Medical Sciences. 2022; 28(6):874-84. [Link]
- Schibye B, Skov T, Ekner D, Christiansen JU, Sjøgaard G. Musculoskeletal symptoms among sewing machine operators. Scandinavian Journal of Work, Environment & Health. 1995; 21(6):427-34. [DOI:10.5271/sjweh.58] [PMID]
- Kaergaard A, Andersen JH. Musculoskeletal disorders of the neck and shoulders in female sewing machine operators: Prevalence, incidence, and prognosis. Occupational and Environmental Medicine. 2000; 57(8):528-34. [DOI:10.1136/oem.57.8.528] [PMID]
- Dianat I, Kord M, Yahyazade P, Karimi MA, Stedmon AW. Association of individual and work-related risk factors with musculoskeletal symptoms among Iranian sewing machine operators. Applied Ergonomics. 2015; 51:180-8. [DOI:10.1016/j.apergo.2015.04.017] [PMID]
- Öztürk N, Esin MN. Investigation of musculoskeletal symptoms and ergonomic risk factors among female sewing machine operators in Turkey. International Journal of Industrial Ergonomics. 2011; 41(6):585-91. [DOI:10.1016/j.ergon.2011.07.001]
- Afifezadeh Kashani H, Daneshvar S, Choobineh A, Tabatabaei S. Investigation of musculoskeletal disorders in sewing machine operators in clothing manufacturing industry. The First International Conference of Ergonomics. 19 May 2008; Tehran, Iran. [Link]
- Rahimi M, Khanvirdi F, Shirzad M, Sazegar F. Correlation of postural abnormalities and musculoskeletal disorders with work experience and body mass index of car repairmen. Physical Treatments-Specific Physical Therapy Journal. 2023; 13(1):45-54. [DOI:10.32598/ptj.13.1.542.2]
- Bawab W, Ismail K, Awada S, Rachidi S, AL Hajje AM, Salameh P. Prevalence and risk factors of low back pain among office workers in lebanon. International Journal of Occupational Hygiene. 2015; 7(1):45-52. [Link]
Type of Study: Research |
Subject:
General
Received: 2024/05/5 | Accepted: 2025/05/31 | Published: 2026/01/15
Received: 2024/05/5 | Accepted: 2025/05/31 | Published: 2026/01/15
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
