Thu, Jul 30, 2026
Volume 15, Issue 2 (Spring 2025)
PTJ 2025, 15(2): 141-150 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Mozafari S, Ebrahimi E, Piri H. Prevalence of Sports Injuries in Female Elite Kumite Karate Players. PTJ 2025; 15 (2) :141-150
URL: http://ptj.uswr.ac.ir/article-1-640-en.html
URL: http://ptj.uswr.ac.ir/article-1-640-en.html



1- Department of Sports Injury and Corrective Exercises, Faculty of Sport Sciences, Allameh Tabataba’i University, Tehran, Iran.
Full-Text [PDF 2169 kb]
(990 Downloads)
| Abstract (HTML) (3103 Views)
Full-Text: (1428 Views)
Introduction
Karate is a martial art that originated in Okinawa, Japan [1]. The literal meaning of the word karate is “empty hand”, and based on the terminology, it is a combat without using equipment against the opponent [2]. Control karate consists of kata (training exercises with predetermined moves) and kumite (sparring). The World Karate Federation is the largest international governing body for Karate, with 198 members [3]. It was formed in 1990 and is the only karate organization recognized by the International Olympic Committee, and it has over 10 million members. The number of people participating in martial arts has increased drastically in recent years [4]. Karate, Taekwondo, and Judo are among the martial arts known as the most popular martial sports in the world [5, 6]. Participating in sports such as Karate or any other sport is not without risk of injury—an undesirable consequence [7]. Researchers endeavor to determine the reasons for this by examining the prevalence and severity of injuries in different sports and providing various approaches to prevent injuries [8]. According to the study by Thomas Tischer et al., the ankle is the most common injury in the kumite part, with 21.8% [9]. According to prior studies, injuries in karate have different causes; for example, Pal et al. and Lystad introduced direct contact with the opponent as the leading cause of injury in karate [7, 10]. Destombe et al. and Zetaruk et al. also believed long-term training causes injury [11, 12]. A study showed that the prevalence of karate training injuries is higher than in competitions [13].
In contrast, Naserpour and Mirjani, as well as Rahimi et al., have considered competition the most common time of injury [14, 15]. Regarding the prevalence of karate injuries, they found that 57.15% of injuries occur suddenly, 35.71% occur gradually, and 65.48% occur due to direct punch and kick contact [10] . Martial arts are considered high-risk activities, but severe injuries in Karate are rare [13]. In a study by Destombe et al. on French Karate players regarding injury severity, they reported that 68.7% of injuries were minor, 8.4% were moderate, 20.5% were severe, and 2.4% were severe [11]. Concerning the type of injuries inflicted on different parts of the body, Arriaza et al. reported that the most common karate injuries are contusions (47%) and lacerations (10%), respectively [16]. Due to the increasing number of people participating in sporting activities, especially championship sports, the health of athletes has received more attention [8]. Moreover, considering the high costs of treatment for many sports injuries and the irreparable damages that may result from injury to athletes, coaches and even other members of society are focused on providing solutions to reduce and prevent the occurrence of injuries [17]. Accordingly, using a questionnaire, this study attempts to consider the mechanisms involved in the prevalence of injuries. The results of this study can help design particular approaches to prevent injuries.
Materials and Methods
This retrospective study investigates the rate of acute and chronic injuries during the last 6 months in black belt female karate players with a training history of at least 6 years. The sample population includes 100 selected elite female karate players of the Kumite league. The inclusion criteria were having a black belt, a history of participating in league teams and doing Control karate. Athletes with less than 6 years of experience were excluded. All of the athletes proved the fulfillment of the study by signing the informed consent provided by the researchers.
The Oslo standard questionnaire was used in this study [18]. The Oslo questionnaire is a tool to analyze and assess health conditions longitudinally in athletic populations [19]. This questionnaire was translated into Persian and found valid and reliable (intraclass correlation coefficient= 0.89; content validity index= 0.79) [20]. This questionnaire includes essential information, such as age, height, weight, dominant hand, level of education, and training history of the athletes. This questionnaire also covers musculoskeletal system care and sports injuries, including the injury’s severity, location, type of injury, mechanism of injury (contact and non-contact), and time of injury (training, competition, warm-up, and cool-down). This questionnaire also examined the absence duration from competitions and training due to the injury and the treatments performed to heal the injury in two types of acute and chronic injuries. In this study, an acute sports injury is defined as a condition that occurs suddenly or accidentally and causes an athlete to stop training or a competition or causes a detectable injury. Acute injuries were considered conditions requiring medical care or keeping the athlete away from training or competition for at least 24 hours. An injury that causes pain during exercise without any visible external cause is considered a chronic injury. The characteristic of a chronic injury is that it gradually intensifies the pain during or after exercise. With the intensification, the pain may become intense enough to stop the exercise altogether. The anatomical regions of the player’s body were classified as follows: Lower limbs (toes, metatarsal bones, soles of the feet, heels, achilles tendon, ankles, calf muscles, lower leg, knee, thigh, hamstring, hip joint, glutes, pelvis, groin), trunk and head (abdomen, waist, chest, upper back, neck, face, teeth, eyebrow, other head injuries), upper limb (clavicle, between the neck and shoulder, shoulder, arm, elbow, forearm, wrist, palm, thumb, other fingers). The type of acute injury was classified as follows: Muscle cramp, strain, contusion (injury without skin tear), wound, sprain, ligament tear, joint dislocation, fracture, and unspecified pain. Also, the type of chronic injury was classified as follows: Stress fracture, tendonitis, bursitis, and nerve entrapment. The tissues involved in chronic injuries were classified as follows: Muscle, tendon, bone, joint, ligament, and nerve tissue. The data obtained were analyzed with a chi-squared test using SPSS Software version 26. The significance level was set at P<0.05.
Results
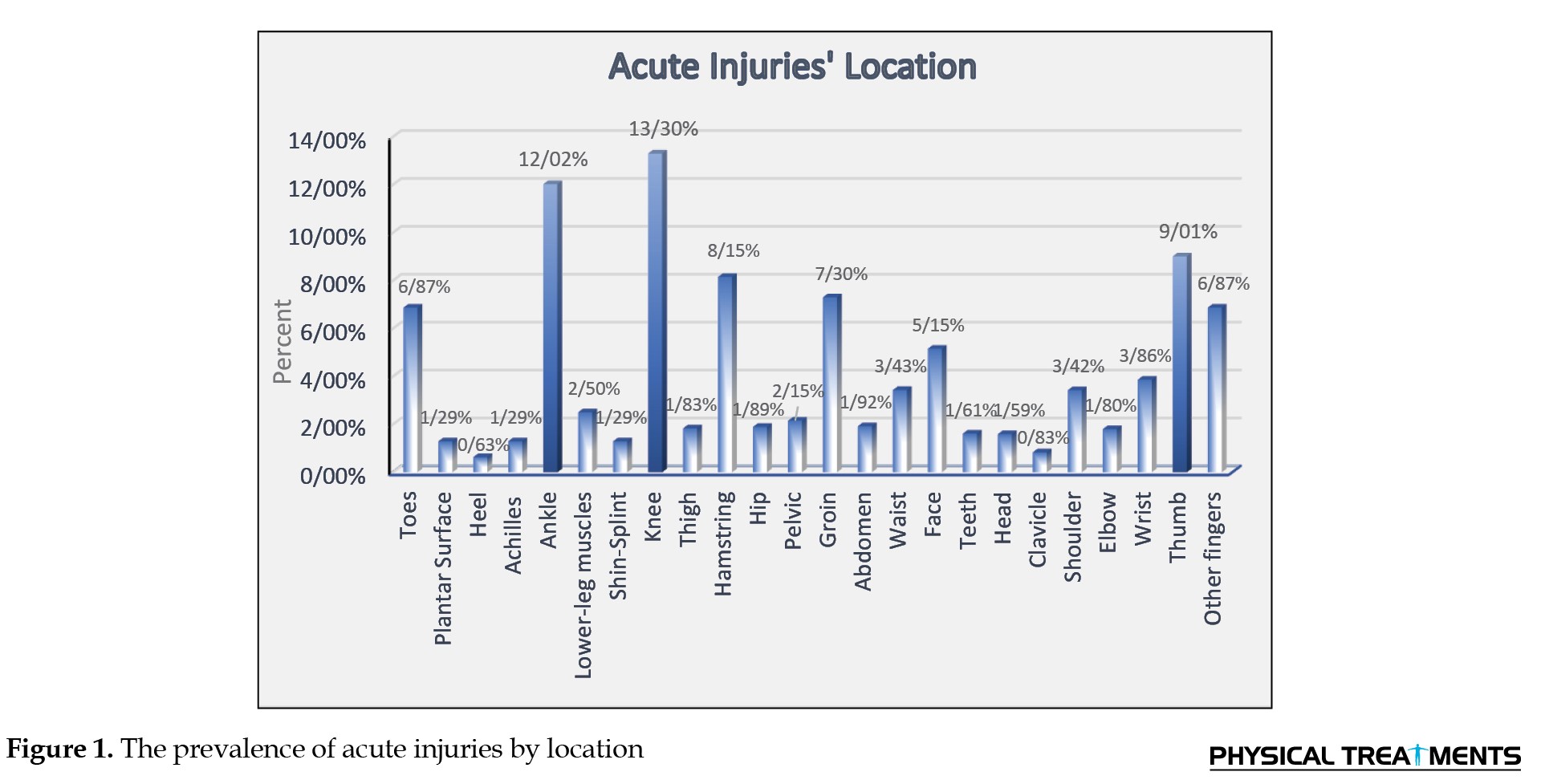
The results showed that the knee with 13.30%, ankle with 12.02%, and thumb with 9.01% were the most common locations of acute injury (χ2=248.052, P=0.001) (Figure 1).
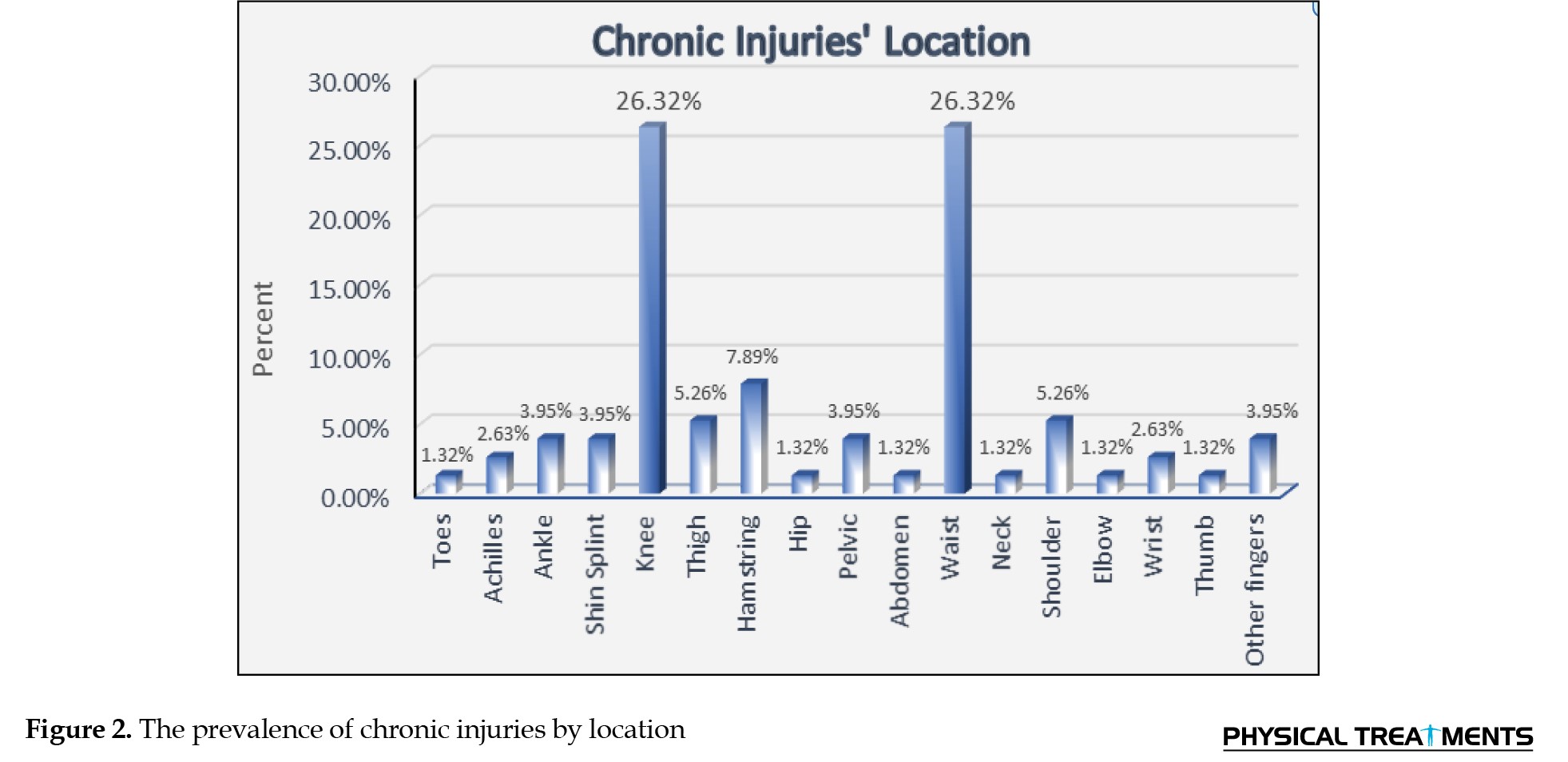
 Also, the lower back and knee by 26.32% and the hamstring by 7.89% were the most common locations of chronic injury (χ2=129.342, P=0.001) (Figure 2).
Also, the lower back and knee by 26.32% and the hamstring by 7.89% were the most common locations of chronic injury (χ2=129.342, P=0.001) (Figure 2).
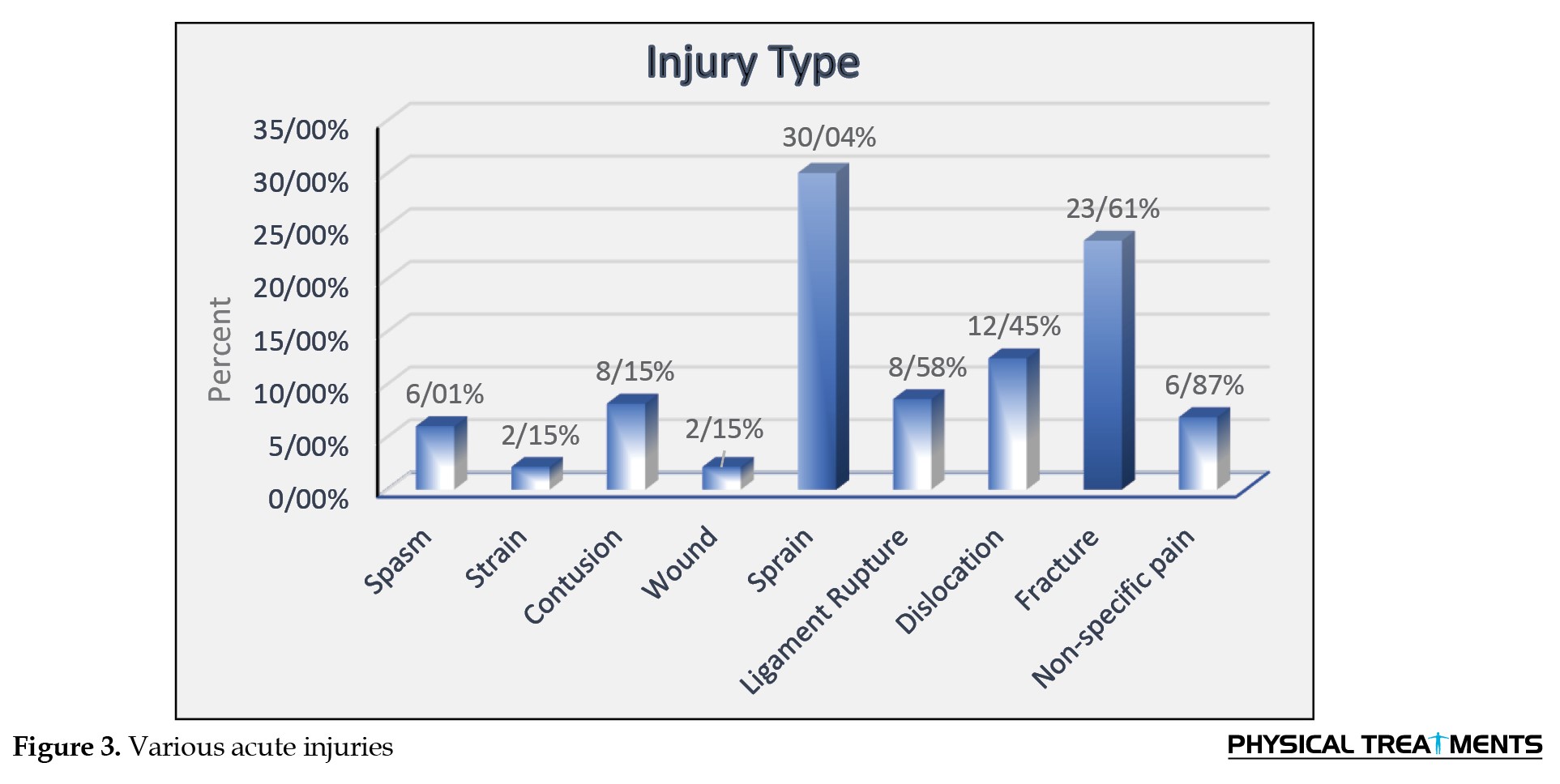
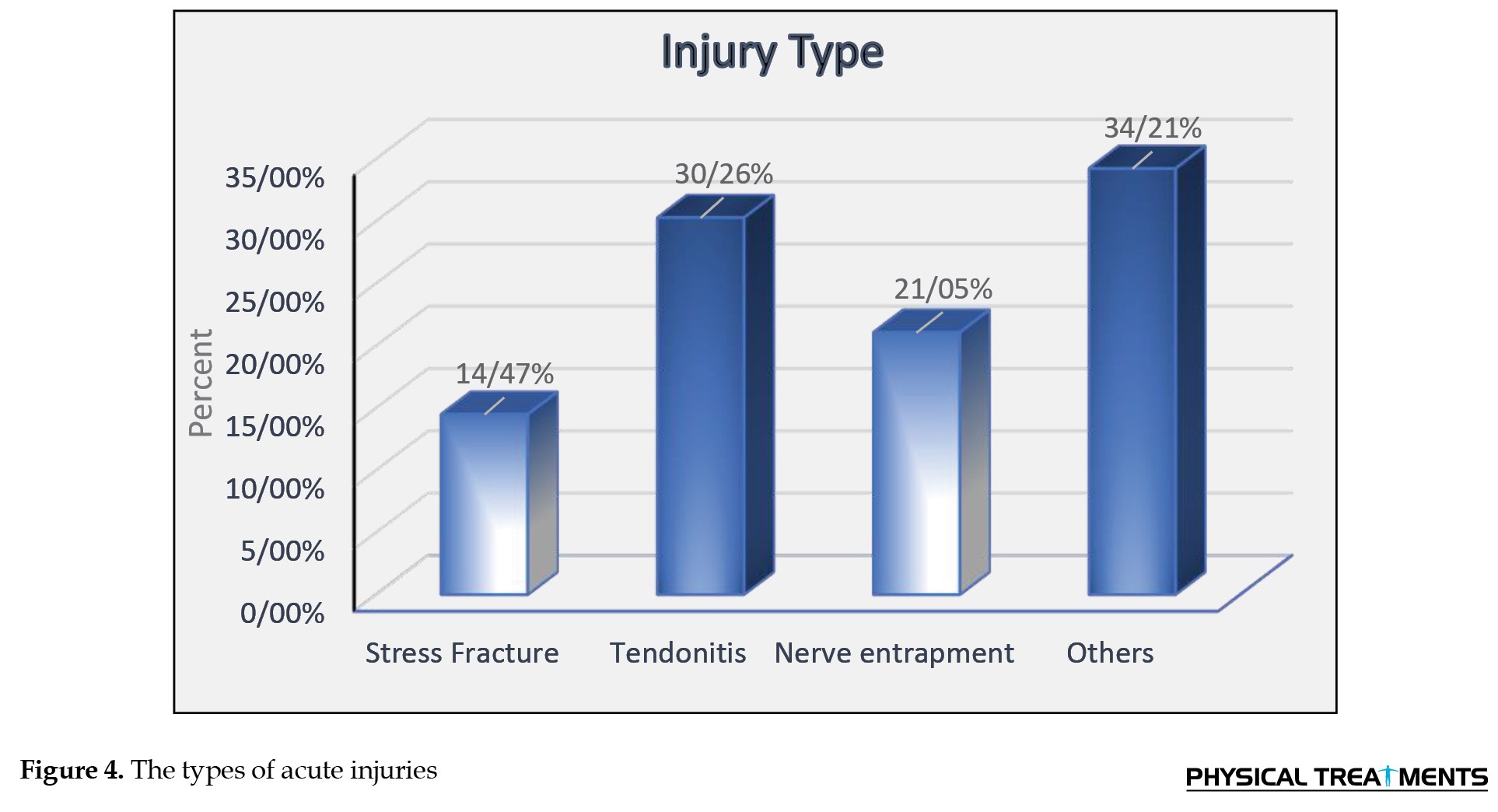
 Additionally, the results showed that sprain (30.04%), fracture (23.61%) and dislocation (12.45%) have the highest percentage in acute injuries (χ2=154.356, P=0.001) (Figure 3) and other injuries (34.21%), tendonitis (30.26%) and nerve entrapment (21.5%) have the highest percentage in chronic injuries (χ2=7.263, P=0.064) (Figure 4).
Additionally, the results showed that sprain (30.04%), fracture (23.61%) and dislocation (12.45%) have the highest percentage in acute injuries (χ2=154.356, P=0.001) (Figure 3) and other injuries (34.21%), tendonitis (30.26%) and nerve entrapment (21.5%) have the highest percentage in chronic injuries (χ2=7.263, P=0.064) (Figure 4).
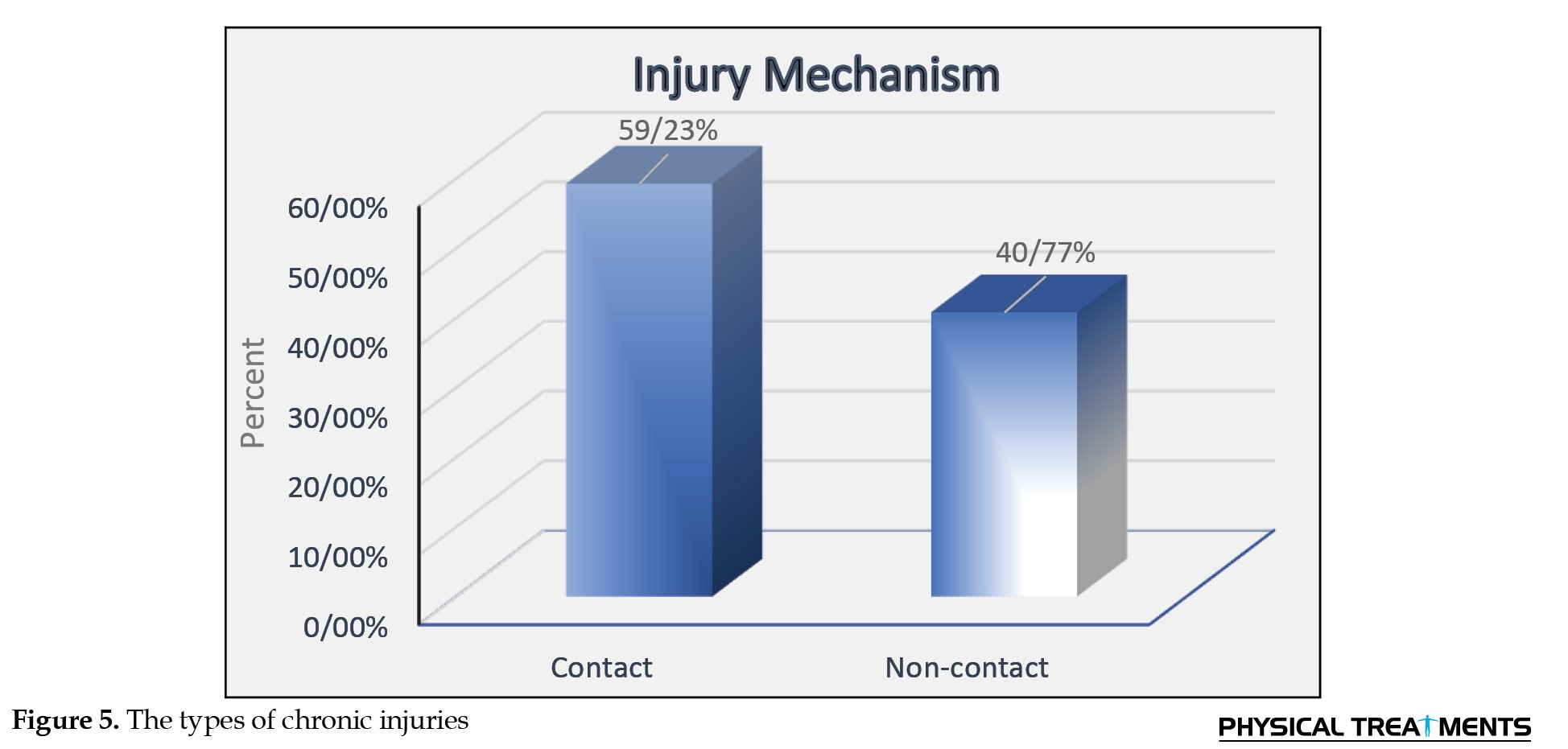
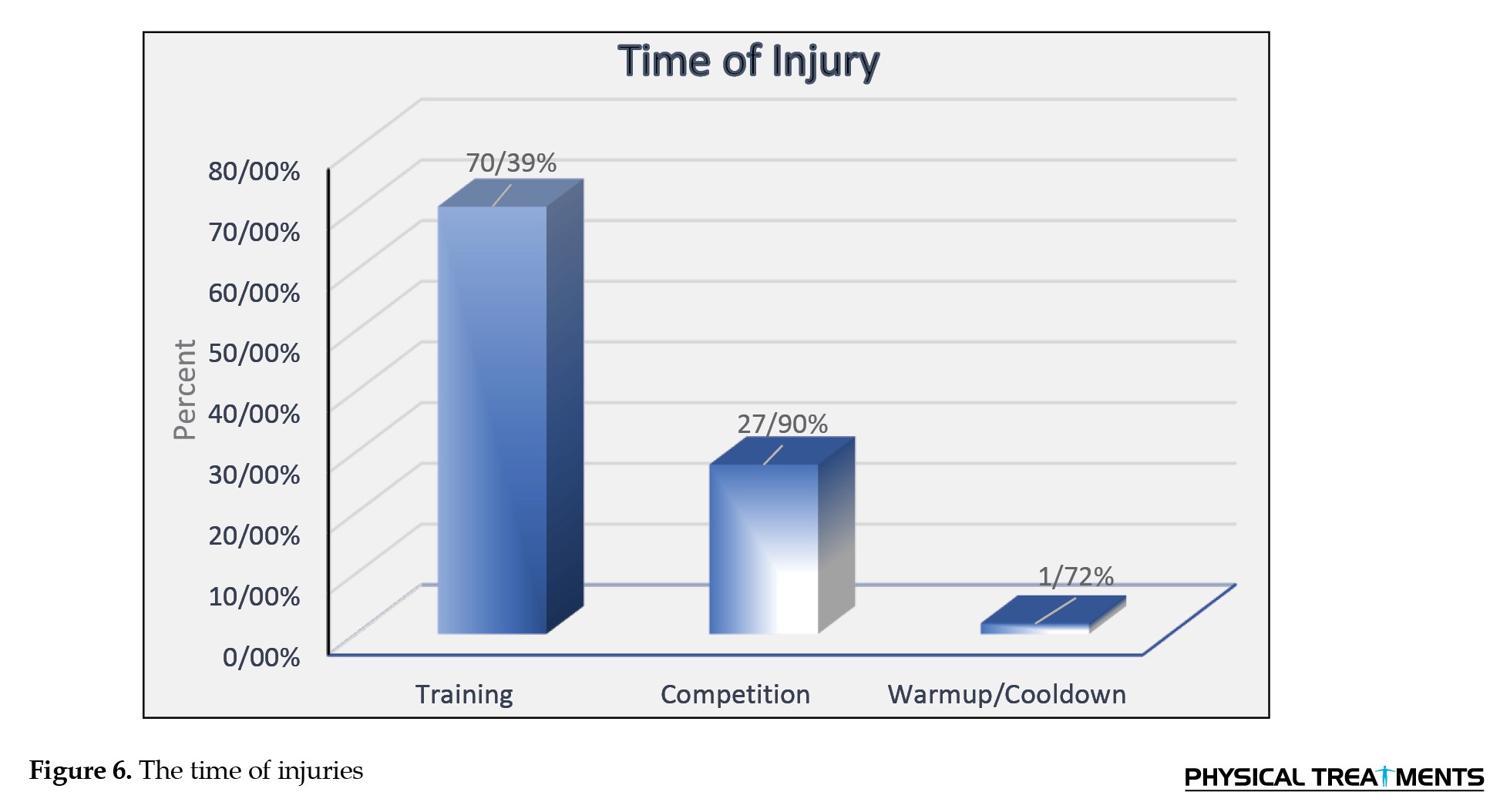
 Furthermore, the findings showed that acute contact injuries (59.23%) have a higher prevalence than non-contact injuries (40.77%) (χ2=7.936, P=0.05) (Figure 5), and these injuries have occurred more during training (70.39%) compared to during competitions and warm-up (χ2=7.263, P=0.064) (Figure 6).
Furthermore, the findings showed that acute contact injuries (59.23%) have a higher prevalence than non-contact injuries (40.77%) (χ2=7.936, P=0.05) (Figure 5), and these injuries have occurred more during training (70.39%) compared to during competitions and warm-up (χ2=7.263, P=0.064) (Figure 6).
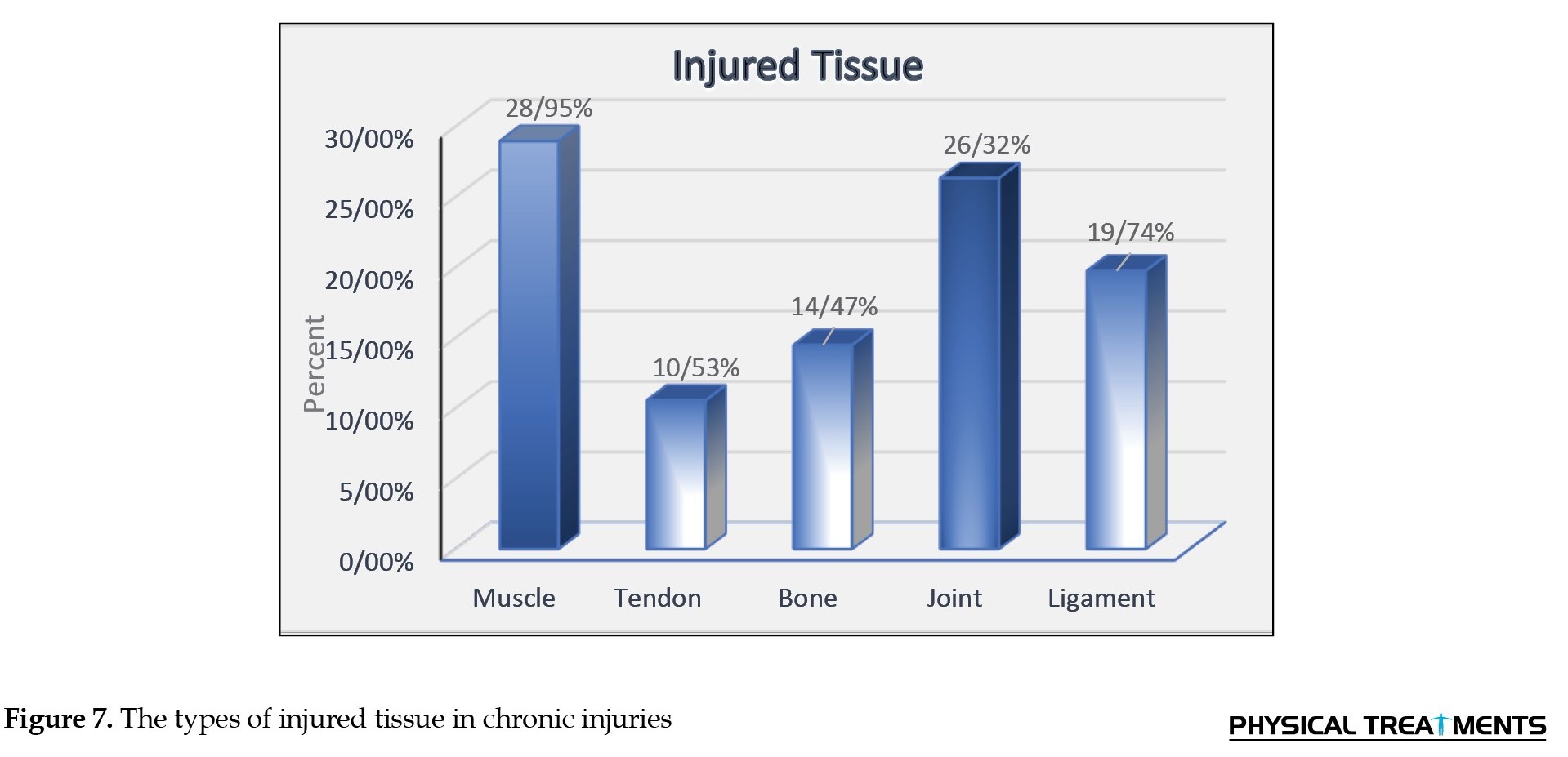
 Concerning chronic injuries, muscle (28.95%), joint (26.32%), and ligament tissues (19.74%) had the highest percentage (χ2=9.132, P=0.58) (Figure 7).
Concerning chronic injuries, muscle (28.95%), joint (26.32%), and ligament tissues (19.74%) had the highest percentage (χ2=9.132, P=0.58) (Figure 7).
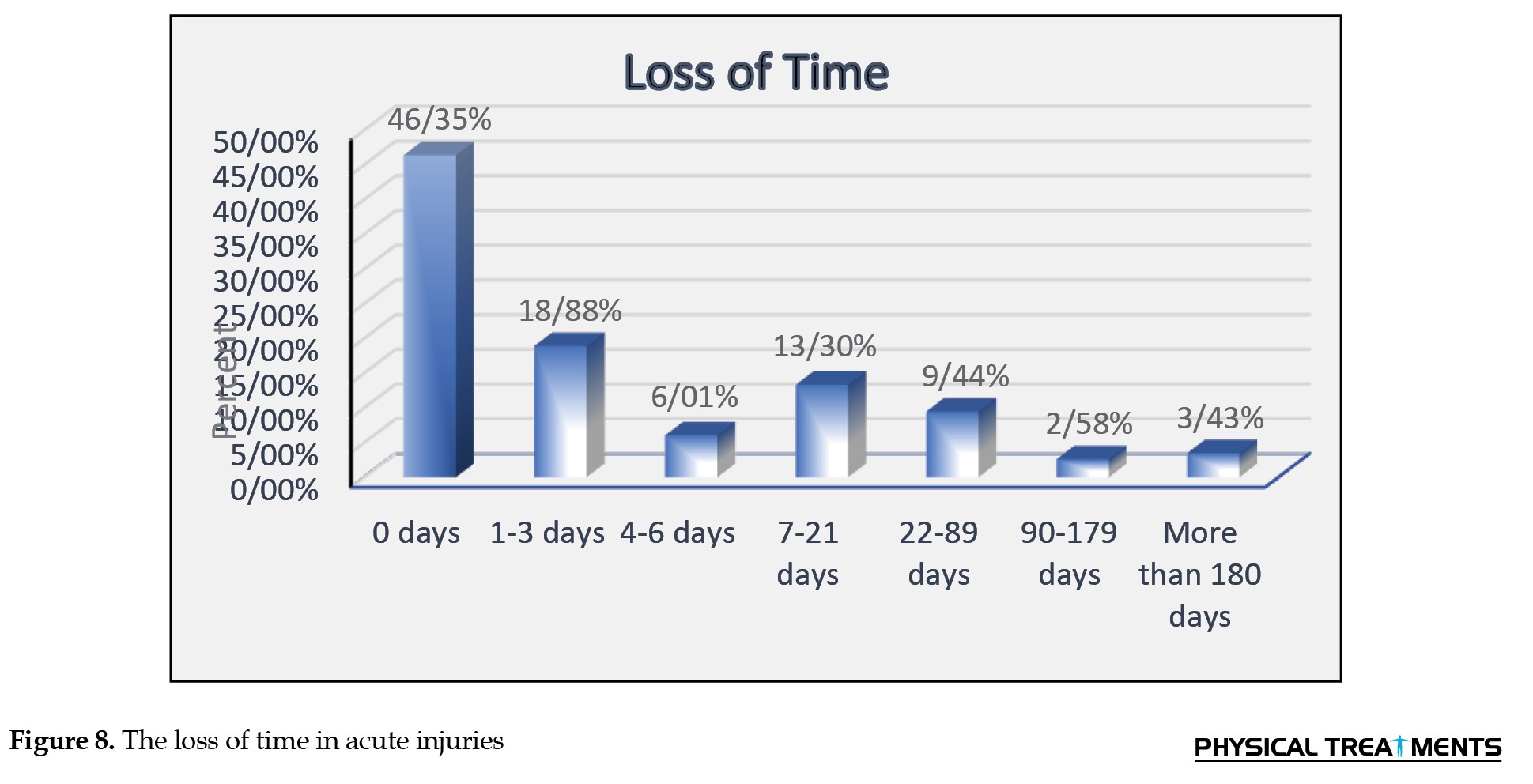
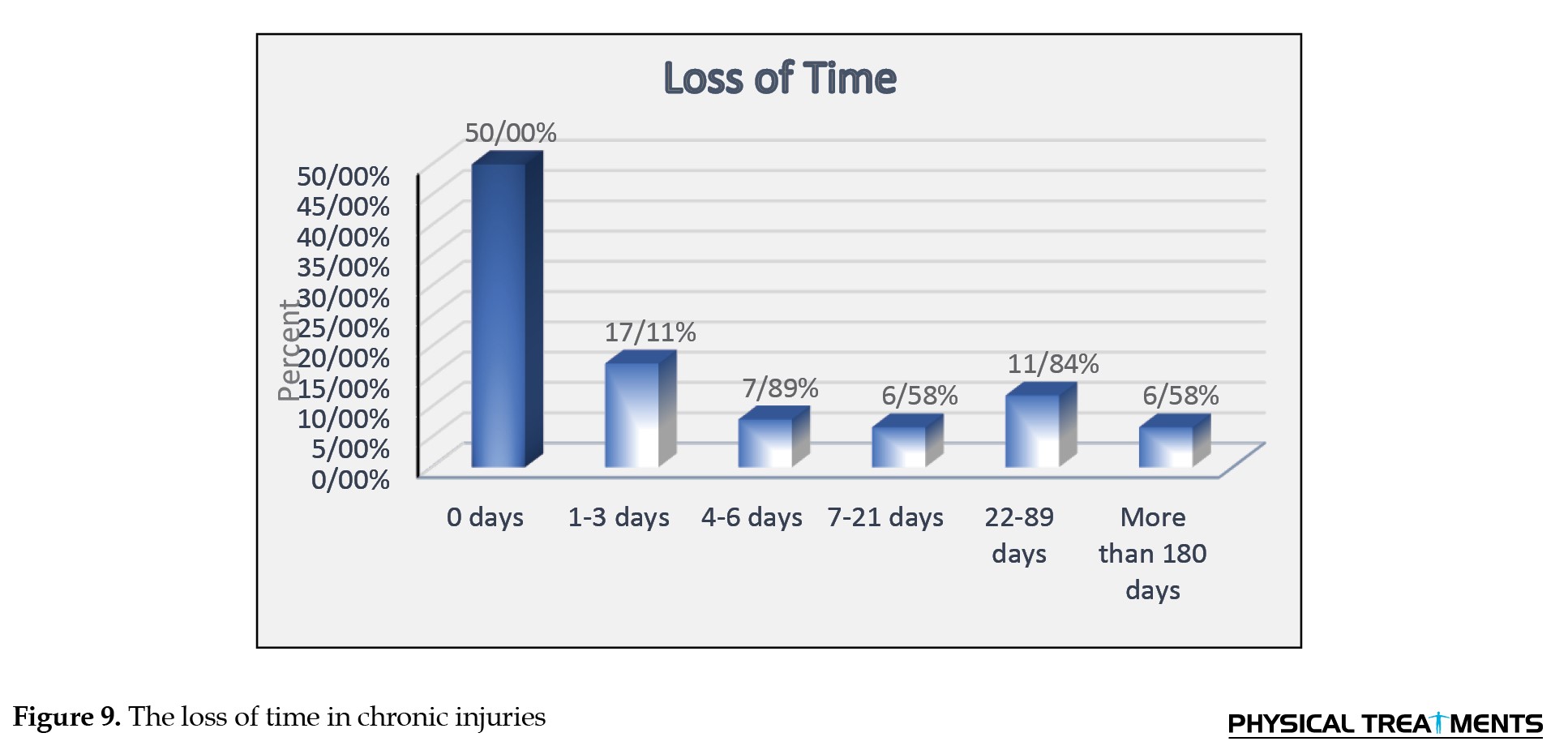
 In addition, the results showed that 46.35% of karate players with acute injury experience (χ2=227.888, P=0.001) (Figure 8) and 50% with chronic injury experience attended training and competitions without absence (χ2=64.526, P=0.001) (Figure 9).
In addition, the results showed that 46.35% of karate players with acute injury experience (χ2=227.888, P=0.001) (Figure 8) and 50% with chronic injury experience attended training and competitions without absence (χ2=64.526, P=0.001) (Figure 9).
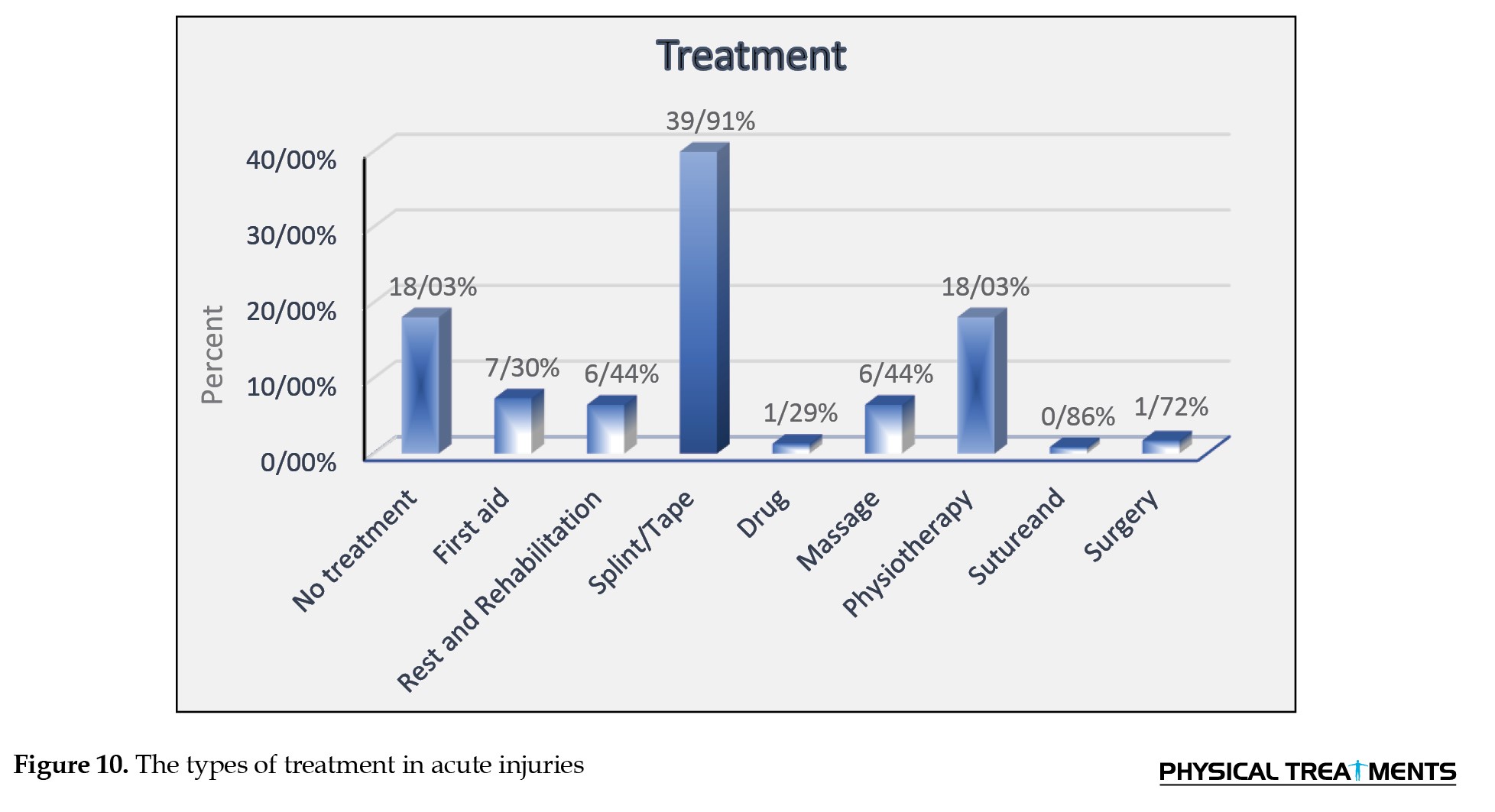
 Also, the results showed that splint/tape (39.91%) and physiotherapy (18.03%) are common treatments in acute injuries, respectively, among karate players (χ2=267.021, P=0.001) (Figure 10).
Also, the results showed that splint/tape (39.91%) and physiotherapy (18.03%) are common treatments in acute injuries, respectively, among karate players (χ2=267.021, P=0.001) (Figure 10).
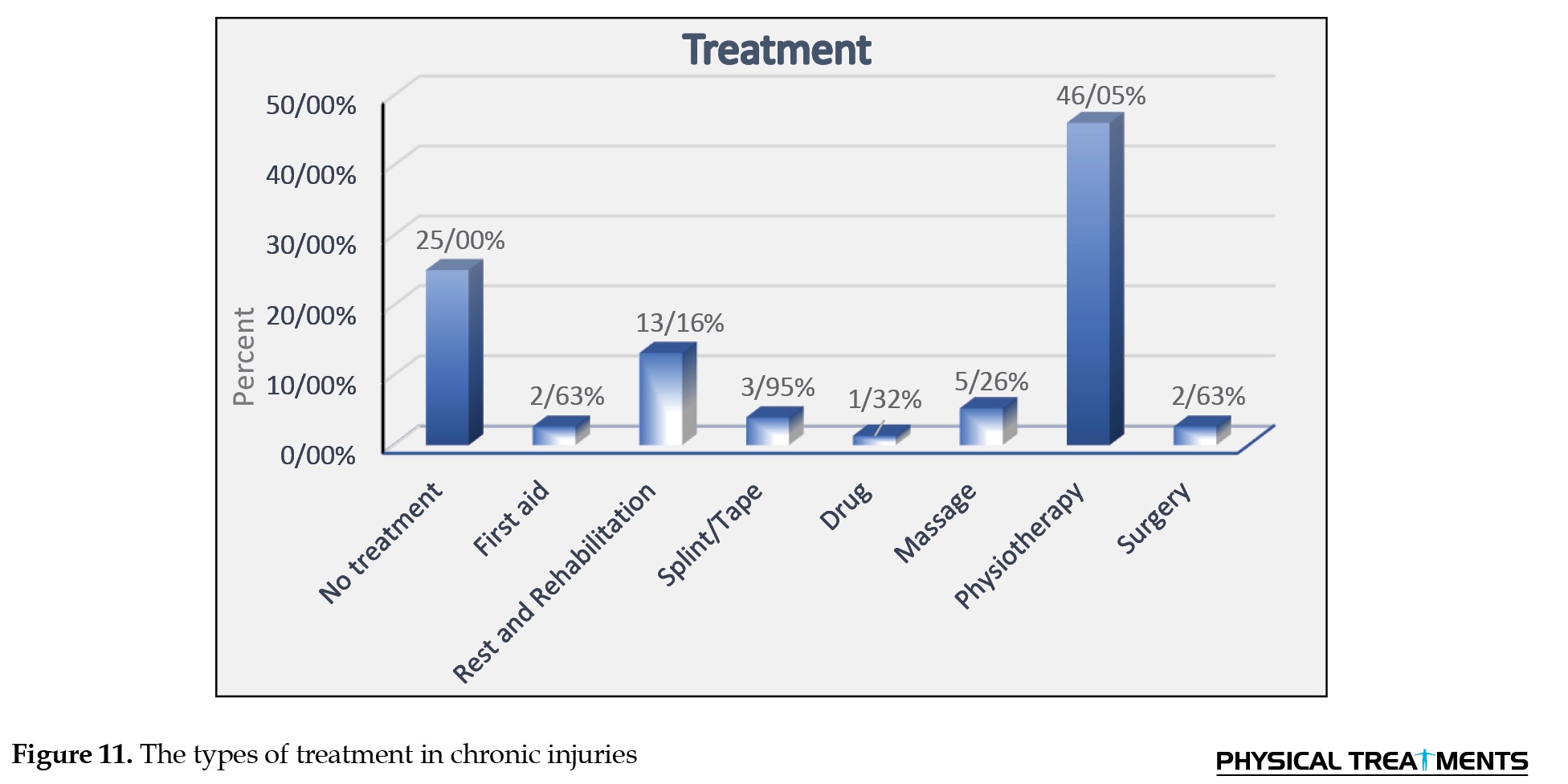
 In addition, physiotherapy (46.05%) was the primary treatment for chronic injuries (χ2=25.474, P=0.001) (Figure 11).
In addition, physiotherapy (46.05%) was the primary treatment for chronic injuries (χ2=25.474, P=0.001) (Figure 11).
Discussion
This study investigated the location, type, mechanism, time, severity of the injury, and treatments performed to manage the injuries in acute and chronic conditions. Concerning the location of the injury, the knee (13.30%) and ankle (12.02%) had the highest percentage of acute injuries. In contrast, the lower back and knee (26.32%) had the highest rate of chronic injuries. The results of the present study are consistent with Tischer et al., who reported that medical treatment was most needed for the knee, and the ankle joint was the most injured part in the kumite players [9]. Also, Rahimi et al. and Antekolović et al. reported that the lower limb is the most vulnerable part of the body in karate players [14, 21]. In addition, Naserpour and Mirjani have stated that 86% of karate players experience ankle sprains, which is the most common injury in girls [15].
Foot-related injuries are mainly caused by foot or lower leg contact with the opponent’s elbow or forearm. Also, taking a 3-point kick for players can lead to more use of kicks during training and competitions, and this factor can be considered a possible reason for higher injuries in the lower extremities [15].
Furthermore, the results of the present study in this part are inconsistent with the findings of Pal et al. and Cierna. They reported that the head and face sustain the most injuries, followed by the upper limb [10, 22-24]. The observed differences can be attributed to gender, age, style, level, and scoring rules changes [6, 7, 25, 26]. According to the present study, karate players will experience injuries to the lower back and lower limbs in the long term. In this regard, Tisal found that karate players can suffer back pain due to the mechanical stress imposed on them during repeated stretching exercises and being in the wrong position [27].
The results of this study show that sprains and fractures are the most common acute injuries, while other injuries and tendonitis account for the highest percentage of chronic injuries. Naserpour and Mirjani reported that 86% of professional karate practitioners had experienced ankle sprains [15], and Antekolović et al. and Tischer et al. believed that ankle sprain is the most common injury location with 11.4% [9, 21]. Moreover, Sterkowicz, as well as Przybycień and Pieter, reported fractures as the most common type of injury, and the results of the present study are aligned with theirs [28, 29]. The results of the present study are inconsistent with the results of Müller-Rath et al. and Zetaruk et al., who reported that bruises are the most common type of injury [12, 30]. Considering the unique role of the ligaments in the ankle joint in controlling its stability and performance during movement, sudden turns cause severe torsional and shear forces, which can result in tears in the ankle ligaments [31]. Kumite involves high contact during combat. In this regard, the results of this article about the mechanisms of acute injury showed that contact-type injuries have a higher prevalence than non-contact injuries, which is consistent with previous studies [10, 32, 33]. Despite the studies that stated the higher prevalence of contact injuries, Huang et al. showed that some lower limb injuries are of the non-contact type, which is inconsistent with the results of the present study [34].
The present study showed that most injuries occurred during training, consistent with the findings of Ziaee et al., Fatahi and Nikjoo, and Destombe et al. [2, 35]. However, some studies have reported that the percentage of injuries in competitions is higher than in training [8, 11, 15]. It is believed that spending more time on training by the athletes, lack of sufficient supervision by the coaches, and the athletes' refusal to use the complete equipment may be the main factors in increasing the risk of injury during training. The present study showed that about half of the karate players participate in training without being absent after experiencing acute and chronic injuries, which can be interpreted as minor severity of the injuries. Also, all the research that examined the severity of injuries showed that the injuries in karate are mild and minor, and serious injuries are infrequent. It seems that the controlled Karate and the non-contact styles of controlled Karate are among the main influencing factors in the mildness of most of the injuries in this sport. The present study’s findings regarding treatment methods showed that the use of splint/tape and physiotherapy in acute injuries and physiotherapy alone in chronic injuries is the most prevalent treatment option. Some studies have discussed that various equipment can be used to protect and treat injuries [36-38]. Also, other studies have also stated that rehabilitation with physiotherapy after chronic injuries is widely being done, consistent with the present study [39, 40].
Conclusion
Based on this study, knees, ankles, and lower back are more prone to injury than other body areas. These injuries mainly include sprains and tendonitis, which occur in ligaments, muscles and tendons.
One of the limitations of the present study is that it examined the injuries of elite kumite karate players. It did not include data and injuries from all karate players with different levels and styles. Also, the small sample size may be another limitation.
Ethical Considerations
Compliance with ethical guidelines
All ethical principles are considered in this article. The participants were informed of the purpose of the research and its implementation stages. They were also assured about the confidentiality of their information and were free to leave the study whenever they wished, and if desired, the research results would be available to them. A written consent has been obtained from the subjects. principles of the Helsinki Convention was also observed.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors contributed equally to the conception and design of the study, data collection and analysis, interception of the results, and manuscript drafting. Each author approved the submission of the final version of the manuscript.
Conflict of interest
The authors declared no conflict of interest.
References
Karate is a martial art that originated in Okinawa, Japan [1]. The literal meaning of the word karate is “empty hand”, and based on the terminology, it is a combat without using equipment against the opponent [2]. Control karate consists of kata (training exercises with predetermined moves) and kumite (sparring). The World Karate Federation is the largest international governing body for Karate, with 198 members [3]. It was formed in 1990 and is the only karate organization recognized by the International Olympic Committee, and it has over 10 million members. The number of people participating in martial arts has increased drastically in recent years [4]. Karate, Taekwondo, and Judo are among the martial arts known as the most popular martial sports in the world [5, 6]. Participating in sports such as Karate or any other sport is not without risk of injury—an undesirable consequence [7]. Researchers endeavor to determine the reasons for this by examining the prevalence and severity of injuries in different sports and providing various approaches to prevent injuries [8]. According to the study by Thomas Tischer et al., the ankle is the most common injury in the kumite part, with 21.8% [9]. According to prior studies, injuries in karate have different causes; for example, Pal et al. and Lystad introduced direct contact with the opponent as the leading cause of injury in karate [7, 10]. Destombe et al. and Zetaruk et al. also believed long-term training causes injury [11, 12]. A study showed that the prevalence of karate training injuries is higher than in competitions [13].
In contrast, Naserpour and Mirjani, as well as Rahimi et al., have considered competition the most common time of injury [14, 15]. Regarding the prevalence of karate injuries, they found that 57.15% of injuries occur suddenly, 35.71% occur gradually, and 65.48% occur due to direct punch and kick contact [10] . Martial arts are considered high-risk activities, but severe injuries in Karate are rare [13]. In a study by Destombe et al. on French Karate players regarding injury severity, they reported that 68.7% of injuries were minor, 8.4% were moderate, 20.5% were severe, and 2.4% were severe [11]. Concerning the type of injuries inflicted on different parts of the body, Arriaza et al. reported that the most common karate injuries are contusions (47%) and lacerations (10%), respectively [16]. Due to the increasing number of people participating in sporting activities, especially championship sports, the health of athletes has received more attention [8]. Moreover, considering the high costs of treatment for many sports injuries and the irreparable damages that may result from injury to athletes, coaches and even other members of society are focused on providing solutions to reduce and prevent the occurrence of injuries [17]. Accordingly, using a questionnaire, this study attempts to consider the mechanisms involved in the prevalence of injuries. The results of this study can help design particular approaches to prevent injuries.
Materials and Methods
This retrospective study investigates the rate of acute and chronic injuries during the last 6 months in black belt female karate players with a training history of at least 6 years. The sample population includes 100 selected elite female karate players of the Kumite league. The inclusion criteria were having a black belt, a history of participating in league teams and doing Control karate. Athletes with less than 6 years of experience were excluded. All of the athletes proved the fulfillment of the study by signing the informed consent provided by the researchers.
The Oslo standard questionnaire was used in this study [18]. The Oslo questionnaire is a tool to analyze and assess health conditions longitudinally in athletic populations [19]. This questionnaire was translated into Persian and found valid and reliable (intraclass correlation coefficient= 0.89; content validity index= 0.79) [20]. This questionnaire includes essential information, such as age, height, weight, dominant hand, level of education, and training history of the athletes. This questionnaire also covers musculoskeletal system care and sports injuries, including the injury’s severity, location, type of injury, mechanism of injury (contact and non-contact), and time of injury (training, competition, warm-up, and cool-down). This questionnaire also examined the absence duration from competitions and training due to the injury and the treatments performed to heal the injury in two types of acute and chronic injuries. In this study, an acute sports injury is defined as a condition that occurs suddenly or accidentally and causes an athlete to stop training or a competition or causes a detectable injury. Acute injuries were considered conditions requiring medical care or keeping the athlete away from training or competition for at least 24 hours. An injury that causes pain during exercise without any visible external cause is considered a chronic injury. The characteristic of a chronic injury is that it gradually intensifies the pain during or after exercise. With the intensification, the pain may become intense enough to stop the exercise altogether. The anatomical regions of the player’s body were classified as follows: Lower limbs (toes, metatarsal bones, soles of the feet, heels, achilles tendon, ankles, calf muscles, lower leg, knee, thigh, hamstring, hip joint, glutes, pelvis, groin), trunk and head (abdomen, waist, chest, upper back, neck, face, teeth, eyebrow, other head injuries), upper limb (clavicle, between the neck and shoulder, shoulder, arm, elbow, forearm, wrist, palm, thumb, other fingers). The type of acute injury was classified as follows: Muscle cramp, strain, contusion (injury without skin tear), wound, sprain, ligament tear, joint dislocation, fracture, and unspecified pain. Also, the type of chronic injury was classified as follows: Stress fracture, tendonitis, bursitis, and nerve entrapment. The tissues involved in chronic injuries were classified as follows: Muscle, tendon, bone, joint, ligament, and nerve tissue. The data obtained were analyzed with a chi-squared test using SPSS Software version 26. The significance level was set at P<0.05.
Results
The results showed that the knee with 13.30%, ankle with 12.02%, and thumb with 9.01% were the most common locations of acute injury (χ2=248.052, P=0.001) (Figure 1).
Discussion
This study investigated the location, type, mechanism, time, severity of the injury, and treatments performed to manage the injuries in acute and chronic conditions. Concerning the location of the injury, the knee (13.30%) and ankle (12.02%) had the highest percentage of acute injuries. In contrast, the lower back and knee (26.32%) had the highest rate of chronic injuries. The results of the present study are consistent with Tischer et al., who reported that medical treatment was most needed for the knee, and the ankle joint was the most injured part in the kumite players [9]. Also, Rahimi et al. and Antekolović et al. reported that the lower limb is the most vulnerable part of the body in karate players [14, 21]. In addition, Naserpour and Mirjani have stated that 86% of karate players experience ankle sprains, which is the most common injury in girls [15].
Foot-related injuries are mainly caused by foot or lower leg contact with the opponent’s elbow or forearm. Also, taking a 3-point kick for players can lead to more use of kicks during training and competitions, and this factor can be considered a possible reason for higher injuries in the lower extremities [15].
Furthermore, the results of the present study in this part are inconsistent with the findings of Pal et al. and Cierna. They reported that the head and face sustain the most injuries, followed by the upper limb [10, 22-24]. The observed differences can be attributed to gender, age, style, level, and scoring rules changes [6, 7, 25, 26]. According to the present study, karate players will experience injuries to the lower back and lower limbs in the long term. In this regard, Tisal found that karate players can suffer back pain due to the mechanical stress imposed on them during repeated stretching exercises and being in the wrong position [27].
The results of this study show that sprains and fractures are the most common acute injuries, while other injuries and tendonitis account for the highest percentage of chronic injuries. Naserpour and Mirjani reported that 86% of professional karate practitioners had experienced ankle sprains [15], and Antekolović et al. and Tischer et al. believed that ankle sprain is the most common injury location with 11.4% [9, 21]. Moreover, Sterkowicz, as well as Przybycień and Pieter, reported fractures as the most common type of injury, and the results of the present study are aligned with theirs [28, 29]. The results of the present study are inconsistent with the results of Müller-Rath et al. and Zetaruk et al., who reported that bruises are the most common type of injury [12, 30]. Considering the unique role of the ligaments in the ankle joint in controlling its stability and performance during movement, sudden turns cause severe torsional and shear forces, which can result in tears in the ankle ligaments [31]. Kumite involves high contact during combat. In this regard, the results of this article about the mechanisms of acute injury showed that contact-type injuries have a higher prevalence than non-contact injuries, which is consistent with previous studies [10, 32, 33]. Despite the studies that stated the higher prevalence of contact injuries, Huang et al. showed that some lower limb injuries are of the non-contact type, which is inconsistent with the results of the present study [34].
The present study showed that most injuries occurred during training, consistent with the findings of Ziaee et al., Fatahi and Nikjoo, and Destombe et al. [2, 35]. However, some studies have reported that the percentage of injuries in competitions is higher than in training [8, 11, 15]. It is believed that spending more time on training by the athletes, lack of sufficient supervision by the coaches, and the athletes' refusal to use the complete equipment may be the main factors in increasing the risk of injury during training. The present study showed that about half of the karate players participate in training without being absent after experiencing acute and chronic injuries, which can be interpreted as minor severity of the injuries. Also, all the research that examined the severity of injuries showed that the injuries in karate are mild and minor, and serious injuries are infrequent. It seems that the controlled Karate and the non-contact styles of controlled Karate are among the main influencing factors in the mildness of most of the injuries in this sport. The present study’s findings regarding treatment methods showed that the use of splint/tape and physiotherapy in acute injuries and physiotherapy alone in chronic injuries is the most prevalent treatment option. Some studies have discussed that various equipment can be used to protect and treat injuries [36-38]. Also, other studies have also stated that rehabilitation with physiotherapy after chronic injuries is widely being done, consistent with the present study [39, 40].
Conclusion
Based on this study, knees, ankles, and lower back are more prone to injury than other body areas. These injuries mainly include sprains and tendonitis, which occur in ligaments, muscles and tendons.
One of the limitations of the present study is that it examined the injuries of elite kumite karate players. It did not include data and injuries from all karate players with different levels and styles. Also, the small sample size may be another limitation.
Ethical Considerations
Compliance with ethical guidelines
All ethical principles are considered in this article. The participants were informed of the purpose of the research and its implementation stages. They were also assured about the confidentiality of their information and were free to leave the study whenever they wished, and if desired, the research results would be available to them. A written consent has been obtained from the subjects. principles of the Helsinki Convention was also observed.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors contributed equally to the conception and design of the study, data collection and analysis, interception of the results, and manuscript drafting. Each author approved the submission of the final version of the manuscript.
Conflict of interest
The authors declared no conflict of interest.
References
- Stricevic MV, Patel MR, Okazaki T, Swain BK. Karate: Historical perspective and injuries sustained in national and international tournament competitions. The American Journal of Sports Medicine. 1983; 11(5):320-4. [DOI:10.1177/036354658301100507] [PMID]
- Ziaee V, Shobbar M, Lotfian S, Ahmadinejad M. Sport injuries of karate during training: An epidemiologic study in Iran. Asian Journal of Sports Medicine. 2015; 6(2):e26832. [DOI:10.5812/asjsm.26832] [PMID]
- Lystad RP, Augustovičová D, Harris G, Beskin K, Arriaza R. Epidemiology of injuries in Olympic-style karate competitions: Systematic review and meta-analysis. British Journal of Sports Medicine. 2020; 54(16):976-83. [DOI:10.1136/bjsports-2020-101990] [PMID]
- Birrer RB. Trauma epidemiology in the martial arts: the results of an eighteen-year international survey. The American Journal of Sports Medicine. 1996; 24(6_suppl): S72-9. [DOI:10.1177/036354659602406S21]
- Fu FH, Stone DA. Sports injuries: Mechanism, prevention, treatment. Williams & Wilkins; 1994. [Link]
- Zetaruk MN, Violán MA, Zurakowski D, Micheli LJ. Injuries in martial arts: A comparison of five styles. British Journal of Sports Medicine. 2005; 39(1):29-33. [DOI:10.1136/bjsm.2003.010322] [PMID] [PMCID]
- Lystad RP. Epidemiology of injuries in full-contact combat sports. Australasian Epidemiologist. 2015; 22(1):14-8. [Link]
- Rahimi M, Halabchi F, Alibakhshi E, Kalali N, Nazari S. Sport injuries of Karatekas at international competitions. Journal of Military Medicine. 2012; 13(4):235-40. [Link]
- Tischer T, Lembcke B, Ellenrieder M, Glass Ä, Weigert W, Mittelmeier W. [Injuries in Karate Sports: A Survey Performed During the World Championship 2014 (German)]. Sportverletzung Sportschaden 2016; 30(4):204-10. [DOI:10.1055/s-0042-112689] [PMID]
- Pal S, Yadav J, Kalra S, Sindhu B. Prevalence of injury pattern among karate players in Delhi-National Capital Region- A cross-sectional survey. Journal of Clinical and Diagnostic Research. 2020; 14(8):YC10-2. [DOI:10.7860/JCDR/2020/45061.13993]
- Destombe C, Lejeune L, Guillodo Y, Roudaut A, Jousse S, Devauchelle V, et al. Incidence and nature of karate injuries. Joint Bone Spine. 2006; 73(2):182-8. [DOI:10.1016/j.jbspin.2005.02.003] [PMID]
- Zetaruk MN, Violan MA, Zurakowski D, Micheli LJ. Karate injuries in children and adolescents. Accident; Analysis and Prevention. 2000; 32(3):421-5. [DOI:10.1016/S0001-4575(99)00120-7] [PMID]
- Buschbacher RM, Shay T. Martial arts. Physical Medicine and Rehabilitation Clinics of North America. 1999; 10(1):35-47. [DOI:10.1016/S1047-9651(18)30214-6] [PMID]
- Rahimi M, Halabchi F, Ghasemi Gh, Zoketaf V. [Prevalence of Karate Injuries in Professional Karate Kai in Isfahan (Persian)]. Annals of Military and Health Sciences Research. 2009; 7(3):201-7. [Link]
- Naserpour H, Mirjani M. [The prevalence and etiology of ankle injury in professional karate players in Iran (Persian)]. Journal of Sport Biomechanics. 2019; 4(4):2-15. [DOI:10.32598/biomechanics.4.4.2]
- Arriaza R, Leyes M, Zaeimkohan H, Arriaza A. The injury profile of Karate World Championships: New rules, less injuries. Knee Surgery, Sports Traumatology, Arthroscopy. 2009; 17(12):1437-42. [DOI:10.1007/s00167-009-0856-3] [PMID]
- Thomas RE, Ornstein J. Injuries in karate: Systematic review. The Physician and Sportsmedicine. 2018; 46(3):279-303. [DOI:10.1080/00913847.2018.1472510] [PMID]
- Clarsen B, Rønsen O, Myklebust G, Flørenes TW, Bahr R. The Oslo Sports Trauma Research Center questionnaire on health problems: A new approach to prospective monitoring of illness and injury in elite athletes. British Journal of Sports Medicine. 2014; 48(9):754-60. [DOI:10.1136/bjsports-2012-092087] [PMID]
- Clarsen B, Bahr R, Myklebust G, Andersson SH, Docking SI, Drew M, et al. Improved reporting of overuse injuries and health problems in sport: An update of the Oslo Sport Trauma Research Center questionnaires. British Journal of Sports Medicine. 2020; 54(7):390-6. [DOI:10.1136/bjsports-2019-101337] [PMID]
- Mirkarimpour SH, Alizadeh MH, Rajabi R, Kazemnejad A. Validity and reliability of the Persian Version of Oslo Sport Trauma Research Center Questionnaire on Health Problems (OSTRC). Sport Sciences and Health Research. 2018; 10(1):1-17. [DOI:10.22059/jsmed.2019.217948.773]
- Antekolović L, Lenard M, Wertheimer V. [Učestalost i vrste ozljeda u karateu (Croatian)]. Hrvatski športskomedicinski vjesnik. 2016; 31(2):58-63. [Link]
- Čierna D, Barrientos M, Agrasar C, Arriaza R. Epidemiology of injuries in juniors participating in top-level karate competition: A prospective cohort study. British Journal of Sports Medicine. 2018; 52(11):730-4. [PMID]
- Pal S, Yadav J, Kalra S, Sindhu B. Injury profile in karate athletes-a literature review. Journal of Critical Reviews. 2020; 7(9):1150-5. [Link]
- Čierna D, Lystad RP. Epidemiology of competition injuries in youth karate athletes: A prospective cohort study. British Journal of Sports Medicine. 2017; 51(17):1285-8.[DOI:10.1136/bjsports-2017-097603] [PMID]
- Linares DV, Lacomba MT. Dolor en el entrenamiento en el karate de competición.: Estudio de prevalencia. Revista Internacional de Medicina y Ciencias de la Actividad Física y del Deporte. 2020; 20(78):335-52. [Link]
- Ambroży T, Mucha D, Czarnecki W, Ambroży D, Janusz M, Piwowarski J, et al. Most common injuries to professional contestant karate. Security Dimensions. 2015; 16:142-64. [Link]
- Tisal H. Surveillance medicale des competitions de sports de combat. Médecine du Sport. 2000; 74(3):6-13. [Link]
- Pieter W. Time-loss injuries in karate. Acta Kinesiologiae Universitatis Tartuensis. 2007; 12:104-5. [Link]
- Sterkowicz S, Sterkowicz-Przybycień K. Injuries in karate: A review. OA Sports Medicine. 2013; 1(2):14. [Link]
- Müller-Rath R, Miltner O, Mamarvar M, Mumme T. [Risk of injury in and adolescent and junior competitive karate (German)]. Sportverletz Sportschaden. 2005; 19(4):191-4. [DOI:10.1055/s-2005-858818] [PMID]
- Hrysomallis C, Goodman C. A review of resistance exercise and posture realignment. The Journal of Strength & Conditioning Research. 2001; 15(3):385-90. [DOI:10.1519/00124278-200108000-00022]
- Galic T, Kuncic D, Poklepovic Pericic T, Galic I, Mihanovic F, Bozic J, et al. Knowledge and attitudes about sports-related dental injuries and mouthguard use in young athletes in four different contact sports-water polo, karate, taekwondo and handball. Dental Traumatology. 2018; 34(3):175-81. [DOI:10.1111/edt.12394] [PMID]
- Greier K, Riechelmann H, Ziemska J. Sportverletzungen im Vollkontakt-und Semikontaktkarate (Ein Vergleich von Kyokushinkai-und traditionellem Karate). OP-Journal. 2016; 32(01):15-19. [DOI:10.1055/s-0042-110667]
- Huang KC, Hsu WH, Wang TC. Acute injury of anterior cruciate ligament during karate training. The Knee. 2007; 14(3):245-8. [DOI:10.1016/j.knee.2006.12.002] [PMID]
- Fatahi A, Nikjoo N. Karate pathology: A systematic Review. Journal of Sport Biomechanics. 2022; 8(2):90-112 . [Link]
- Piejko L, Mosler D, Grzebisz N. Sport injuries in karate kyokushin athletes. Biomedical Journal of Scientific & Technical Research. 2019; 15(1):11134-41. [DOI:10.26717/BJSTR.2019.15.002653]
- Johannsen HV, Noerregaard FO. Prevention of injury in karate. British Journal of Sports Medicine. 1988; 22(3):113-5. [DOI:10.1136/bjsm.22.3.113] [PMID]
- Macan J, Bundalo-Vrbanac D, Romić G. Effects of the new karate rules on the incidence and distribution of injuries. British Journal of Sports Medicine. 2006; 40(4):326-30; discussion 330. [DOI:10.1136/bjsm.2005.022459] [PMID]
- Thomas AJ. Physiotherapy led early rehabilitation of the patient with critical illness. Physical Therapy Reviews. 2011; 16(1):46-57. [DOI:10.1179/1743288X10Y.0000000022]
- Malmros B, Mortensen L, Jensen MB, Charles P. Positive effects of physiotherapy on chronic pain and performance in osteoporosis. Osteoporosis International . 1998; 8(3):215-21 [DOI:10.1007/s001980050057] [PMID]
Type of Study: Research |
Subject:
Sport injury and corrective exercises
Received: 2024/05/2 | Accepted: 2024/10/26 | Published: 2025/04/1
Received: 2024/05/2 | Accepted: 2024/10/26 | Published: 2025/04/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
