Thu, May 28, 2026
Volume 14, Issue 3 (Summer 2024)
PTJ 2024, 14(3): 191-200 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Azizi F, Raeisi Z, Ghasemi S. Effects of Sensorimotor Training With Visual Feedback on Knee Joint Alignment in Women With Dynamic Knee Valgus. PTJ 2024; 14 (3) :191-200
URL: http://ptj.uswr.ac.ir/article-1-623-en.html
URL: http://ptj.uswr.ac.ir/article-1-623-en.html



1- Department of Sports Injuries and Corrective Exercises, Faculty of Sports Sciences, Arak University, Arak, Iran.
2- Department of Sports Biomechanics, Faculty of Sports Sciences, Arak University, Arak, Iran.
2- Department of Sports Biomechanics, Faculty of Sports Sciences, Arak University, Arak, Iran.
Full-Text [PDF 1782 kb]
(1178 Downloads)
| Abstract (HTML) (3795 Views)
Full-Text: (1270 Views)
Introduction
The knee joint is commonly considered a hinge-type joint with two degrees of freedom, flexion extension, and internal-external rotation [1]. Dynamic knee valgus (DKV) is the term used to describe the misalignment of the knee joint that occurs in the frontal plane. This misalignment can be caused by excessive femoral adduction, internal rotation, tibial abduction, and external rotation [2, 3]. This condition represents the kinematic changes in the thigh, knee, and ankle [4], induced by multiple factors, including increased femoral anteversion and tibial torsion, reduced hip abductor muscle strength, uncontrolled muscles of the lower pelvic area, more tibial mobility, a wider pelvis, and an excessive Q angle [5]. DKV has also been introduced as the leading cause of anterior cruciate ligament (ACL) injury [6]. Thus far, few studies have explored the prevalence rate of this movement impairment and its relationship with lower extremity mobility, knee pain, and gender; however, some reports have revealed a higher prevalence rate in women and adolescents than men and adults [1, 2, 7].
Impaired proprioception has been observed to be a significant manifestation after DKV [8]. Proprioception is the key component of the sensorimotor (SM) system, sourced mainly from muscle spindles. It plays a significant role in understanding the spatial and biomechanical position of different body parts [9]. It can also expand the strength and stability of the lower extremities [10]. DKV complications include improper dynamic control of body parts and the inability to control the trunk, pelvis, knees, and ankles in the frontal and horizontal planes [11].
This condition is one of the most common risk factors to predict acute injuries and those caused by lower extremity overuse, such as patellofemoral pain syndrome (PFPS), ACL injury, meniscus tear (or the knee cartilage damage), iliotibial band syndrome (ITBS), knee osteoarthritis (KOA), and a medial collateral ligament (MCL) injury [4]. Among these, ACL injury is a significant concern, causing short- and long-term recovery episodes and substantial financial burdens. A higher possibility of re-injuries, negative psychological effects, increased risk of KOA, and decreased sports performance have also been presented among the consequences of knee-related injuries in female athletes [6]. On the other hand, DKV causes patellar instability, which means that overloading due to increased activity adds to the pressure on the knee joint and causes PFPS [12].
Various exercise programs have been used to rehabilitate DKV, including sportometric [6], plyometric [4, 13, 14], neuromuscular [15], corrective [8, 16], and strengthening [11] exercises, each with their advantages. SM training (SMT) combines balance and proprioceptive exercises commonly used for rehabilitation [9]. The exercises aim to fix muscle imbalance, improve balance, and enhance the functions of the neuromuscular and proprioceptive systems. Some studies have even utilized such exercises to manage pain, improve typical functions in patients with chronic musculoskeletal pain, correct muscle imbalance, and increase postural control. This training program has been accordingly designed based on a series of exercises to challenge the SM system [9, 17], which helps boost functional adaptation in the neuromuscular system and leads to better intramuscular coordination, balance control, augmented proprioception, and lower postural fluctuations, and subsequently reduced injuries [9, 18]. The basic concept raised in this training program is attaching greater importance to the central nervous system (CNS) in regulating movements rather than accentuating muscle strength to maintain joint stability [12]. In other words, SMT aims to improve muscular endurance response but not strength [10].
It has been shown that feedback is one of the best tools for learning motor skills quickly and easily. Some studies have shown that verbal and visual feedback (VF) through videos and mirrors can positively affect DKV [19]. For instance, Alvandi et al. discovered that VF-based training during the single-leg squat test (SLST) can enhance movement accuracy and provoke changes in muscle activation strategies [19]. Therefore, exercises become more effective when accompanied by feedback. Moreover, SMT can help build pelvic stability [20], and proprioception [18], minimize pain and pelvic organ prolapse [20], and boost postural stability [22], as the main risk factors of DKV. Against this background, the present study investigated the effects of an eight-week SMT program with VF on knee joint proprioception and alignment in women with DKV. The research hypothesis was that practicing SMT simultaneously with receiving VF can effectively improve knee joint proprioception and alignment in women with DKV.
Materials and Methods
Study design
This is a randomized clinical trial. Participants were 30 female students with DKV who voluntarily participated after signing a consent form. The Randlist software was utilized to randomly allocate subjects to different study groups. The randomization method used was parallel. Initially, the software was provided with the number of participants and groups. Then, a code was assigned to each participant. Finally, the software randomly assigned a group to each code. The intervention group attended an eight-week SMT program with VF, while the control group continued their daily routines.
Based on the G*Power software output for the analysis of covariance (ANCOVA), the sample size was estimated to be 34 individuals, with an effect size of 0.5, a significance level of 0.05, and a test power of 0.8 [23]. Considering dropout (5%), 36 participants were recruited (18 in each group). However, six individuals were excluded from the analysis due to their absence at the post-test stage, three from the control group and three from the intervention group.
The study included only females aged between 18 and 30 diagnosed with DKV based on positive leg squat test (LST) results. The participants were required to have no history of knee surgeries within the past year, no lower extremity injuries in the past year, and no neuro-orthopedic or special conditions. Those who missed two consecutive or three non-consecutive training sessions or were absent during the post-test stage were excluded from the study.
Assessment
As a type of abnormal movement impairment, dynamic knee valgus (DKV) can be evaluated through various tests, such as jumping and landing tests and the double-leg squat test (DLST). The squat test, which requires no unique equipment and can be conducted at any location, can effectively screen for this condition [24]. The participants with DKV were included in this study when the medial border of their patella crossed the medial part of the big toe during the DLST. To achieve this, each participant performed the LST five times in a controlled manner under standard conditions. The overhead squat test was performed with legs shoulder-width apart, toes forward, and hands above the head, mimicking sitting on a chair. If DKV was observed during the overhead squat, i.e. in three out of five movements, the test results were considered positive [6].
Likewise, the knee joint angle repositioning error during the SLST was employed to evaluate knee joint proprioception. The participants completed this test by the 60-degree bend of the knee joint with a metronome of 60 beats per minute (including two flexion beats and two back-to-the-initial-position ones). Upon placing the goniometer on the lateral compartment (that is, one arm of the goniometer set along the outer side of the thigh and one arm along the leg), the participants were asked to remake a 60-degree knee flexion angle with eyes closed. The test was repeated three times, and the mean difference between the angle made by the participants and the standard one was then recorded as the proprioceptive error for each case [8]. The test re-test reliability of this test was reported as 0.90 in the previous study [8].
The single-leg landing test (SLLT) was administered to measure knee alignment. Participants were asked to stand on a box 40 cm above the ground with their non-dominant leg and keep the heel of their dominant leg on the front edge of the box. Then, they had to land on their dominant leg when the examiner asked them to, without bending or jumping vertically, and maintain their balance for 5 seconds after landing [13, 14]. The test had to be repeated three times with 30-s intervals between each repetition. A digital camera recorded the landing. It is essential to note that the participants were not given any instructions about the correct landing technique or provided with feedback on their performance [4, 6].
The camera was positioned parallel to the frontal plane, 366 cm away from the landing box on the base, at a height of 102 cm to ensure that the lower extremity was visible within the camera frame [4]. Landmarks were placed at the ankle joint center, patella, and anterior superior iliac spine (ASIS) for greater accuracy [20, 25]. The participants performed three repetitions of landing from the box at a normal speed during daily activities. Using the Kinovea software, the DKV angle was calculated at the moment of maximum knee flexion after landing by connecting two lines drawn from the ASIS to the patella and one passing from the patella to the center of the ankle joint. The knee alignment angle was then calculated by deducting the value obtained from 180. The average angle during three repetitions was recorded for each participant in the field [4, 20]. The reliability of the test for detecting DKV has been reported by Munro et al. to be 0.88-0.91 [26]. All variables were measured and evaluated one session before and after the exercises.
VF-based SMT
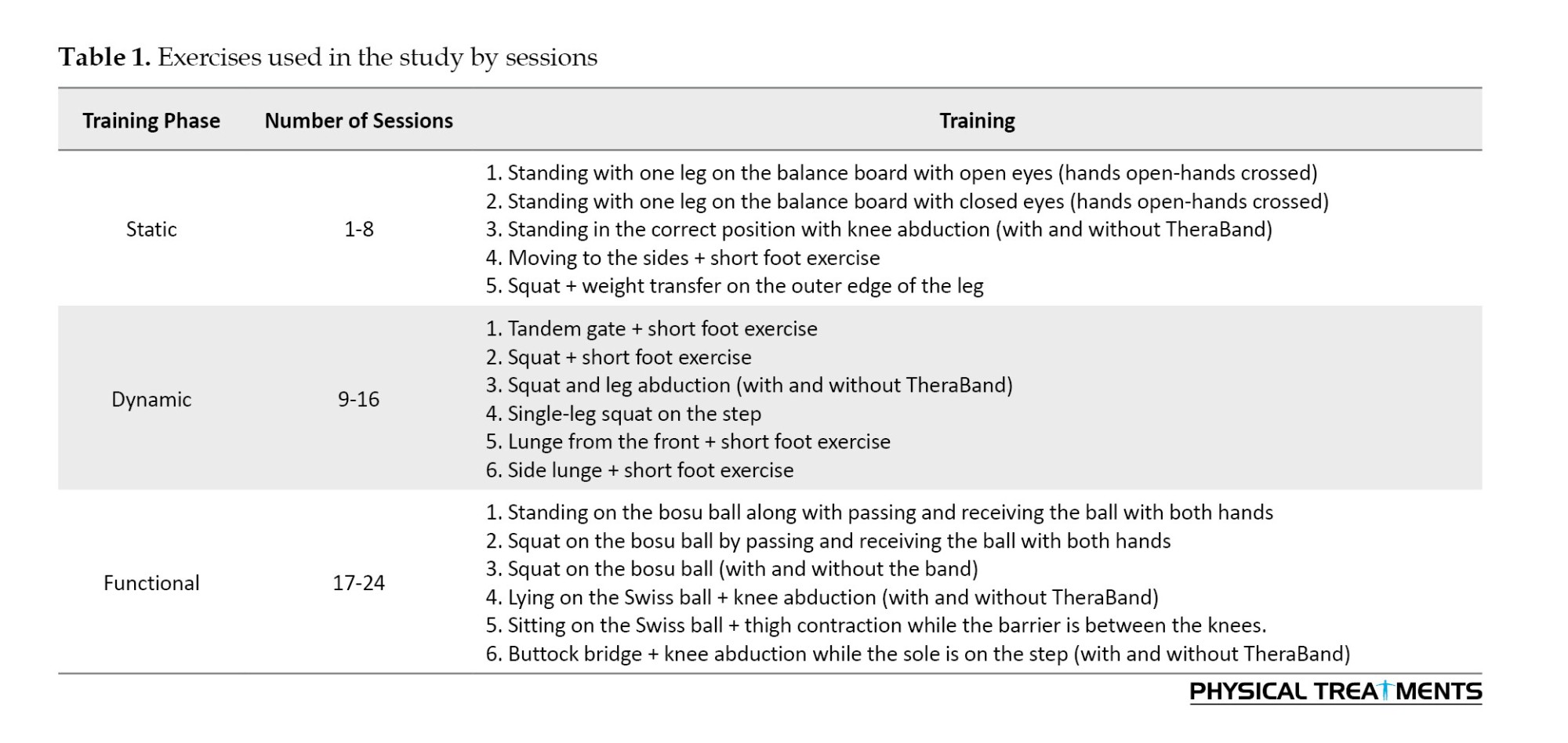
The intervention group completed the SMT program with VF within eight weeks, attending three sessions per week, each lasting 60 minutes. The training sessions included a 15-minute warm-up and stretching, 40 minutes of detailed exercises, and a 5-minute cool-down to return the body to rest. During this study, participants did not receive any other treatments, medications, or placebos. The exercises were performed using body weight, but resistance bands (TheraBand) were used to increase the intensity (Table 1). The principles and methods of the exercises were explained to the participants, and they were asked to maintain their regular practice throughout the training period. Additionally, all exercises were performed in front of mirrors with VF, allowing participants to control each movement by receiving feedback through the mirrors.
All exercises listed in Table 1 were completed during each session. The exercise routine began at the lowest level and gradually increased in intensity and volume over eight weeks. Figure 1 shows a sample of the exercises given.

The data were analyzed using IBM SPSS statistics software, version 26. The normality of the data was determined using the Shapiro-Wilk test. Since the data was normally distributed (P>0.05), the ANCOVA test was applied to remove intervening variables, adjust the pre-test stage scores, and make intergroup comparisons. A significance level of 0.05 was used for all tests. The data analyzer was not aware of the group classification. The information about the groups was provided to the data analyzer in the form of numbers 1 and 2 and for each participant with a code.
Results
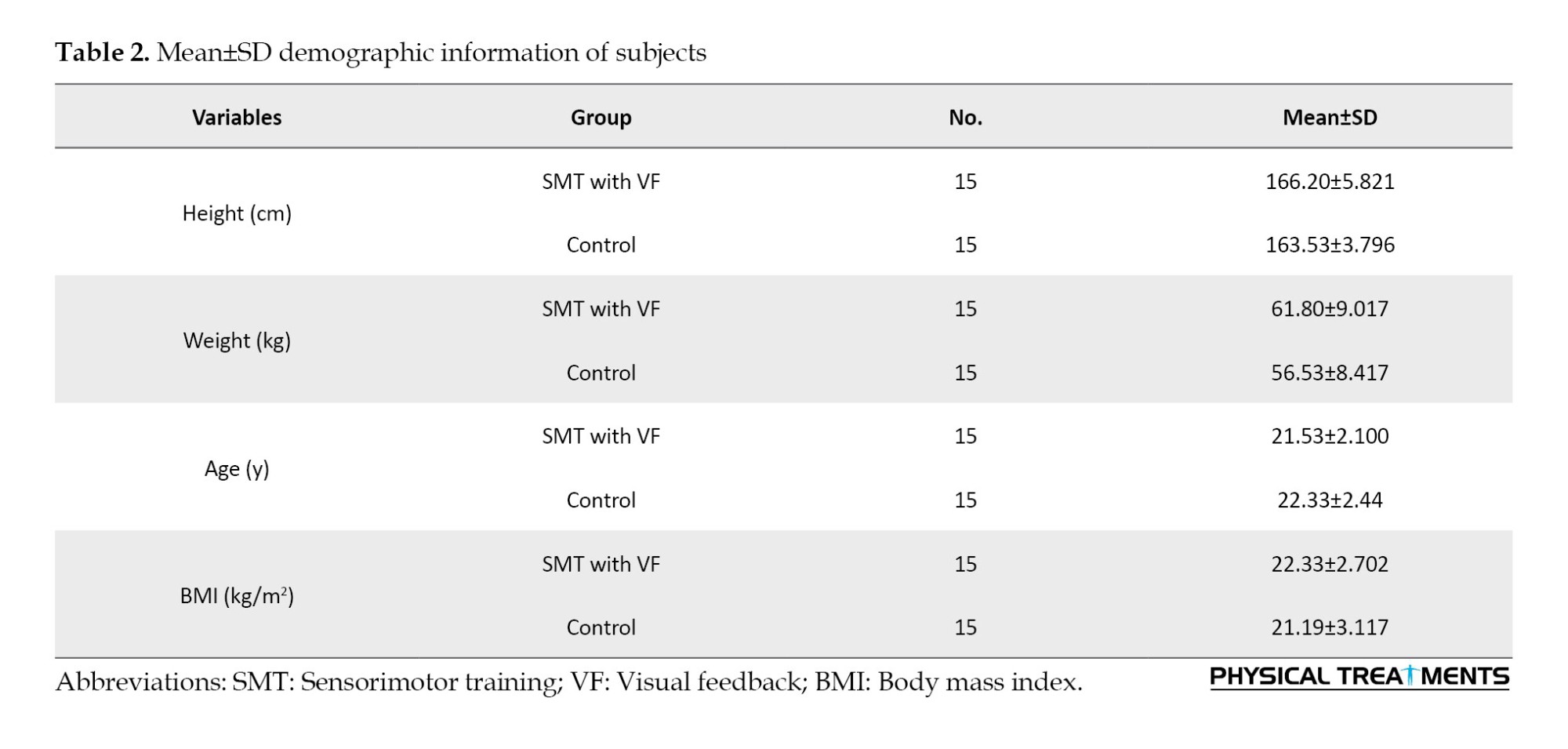
Table 2 presents the demographic characteristics of participants in each group.
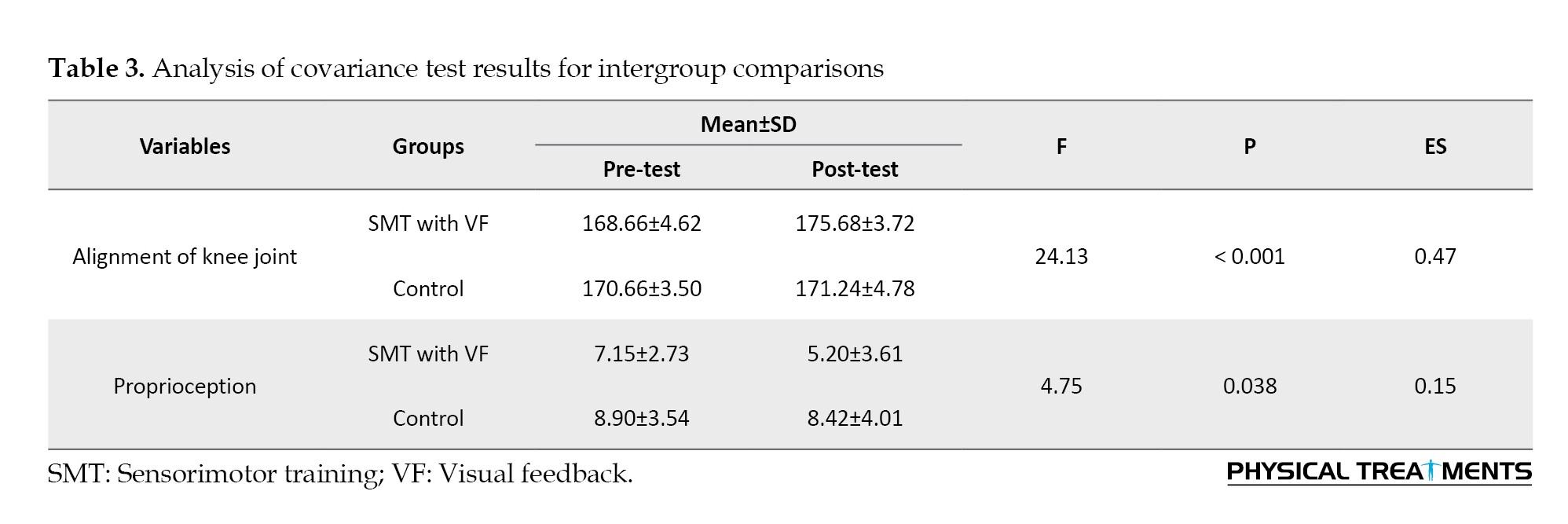
After analyzing the results of the intergroup comparisons using ANCOVA, with the pre-test stage scores as a covariate, it was found that the VF-based SMT program attended by participants in the intervention group significantly reduced knee joint proprioception (P=0.038, F=4.75, Eta=0.150) and improved knee alignment (P<0.001, F=24.13, Eta=0.472), as compared to those in the control group (Table 3).
Discussion
This study was conducted to examine the impact of an eight-week SMT program combined with VF on knee joint proprioception and alignment in women with DKV. The results indicated that SMT exercises with VF enhanced knee joint proprioception and alignment.
It is essential to note that any changes in the alignment of the lower extremities can lead to transformations in different body parts, resulting in deviations in various patterns [14, 27]. Disorders like DKV can affect the desired posture of the lower extremity, which can induce changes in the weight distribution in the knee. This issue can create pressure and variations in the knee joint position, reducing mechanical efficiency. Such an unfavorable situation can be the leading cause of multiple neuromuscular injuries. DKV is also a risk factor for various injuries, including ACL injury, PFPS, MCL injury, meniscus tear, ITBS, and KOA [24]. According to Ramezani et al., DKV refers to a range of kinematic changes in the lower extremity, including increased hip adduction and knee abduction, as well as internal rotation of the proximal components and external rotation of the distal ones. This can cause a maximized torque of the knee, which can increase the functional angle of the quadriceps muscles and the pressure of the external part of the patellofemoral joint [28]. Knee joint alignment can be assessed in both the sagittal and frontal planes. The knee joint should be examined from an anterior-posterior view in the frontal plane. The femoral angle in the inner part is also caused by the inclination angle in the proximal part of this bone. The longitudinal axis of the femur is thus about 10 degrees away from the longitudinal axis of the tibia, resulting in a physiological angle of approximately 170-175 degrees in adults with DKV in the frontal plane [29].
Performing exercises, such as SLST and DLST, forward and lateral lunges, single- and double-leg standing and landing on an unstable surface, and walking on soft and hard surfaces [20] have been effective ways to treat this condition. The training program implemented in this study included SMT, designed by Janda, aimed at escalating muscular endurance response rather than strength [10]. These exercises were a particular form of balance and proprioceptive to fix muscle imbalance, improve balance, and boost the functions of the neuromuscular and sensory systems [9, 17]. During the study, the interventions were split into three phases of exercise [20, 21]. In the first phase, the static phase, the participants were asked to maintain their center of gravity by using passive weight displacement or dealing with specific challenges requiring postural reflexive reactions to help with hip stability. In the second phase, the dynamic phase, the center of gravity challenges were executed dynamically, and some swing exercises were added to facilitate muscle stability. Finally, the participants performed functional progress and movements in the functional phase while maintaining hip stability. This phase was considered the final phase of the study [10].
Depending on the situation, SMT can be performed with or without tools and equipment. One of the main exercises in this program is short foot training, in which the internal longitudinal arch increases with the contraction of the plantar muscles while the toes are not contracted. According to Janda, this training can improve proprioception and postural stability [10]. Among other examples of the advanced form of SMT, balance exercises on bosu ball, Janda's balance sandals, and balance board should be mentioned. In this study, there was much attempt to improve the changes resulting from DKV and bring the body closer to the normal posture by a set of exercises, such as SLST and DLST, as well as forward and lateral lunges. Such exercises can strengthen the quadriceps and hip abductor muscles, reduce the femoral internal rotation angle, improve knee joint alignment, and minimize DKV [9, 20].
Claiborne et al. discovered a robust negative correlation between the isokinetic peak torque of the femoral abductor muscle and the external rotators and the DKV angle during the SLST. This means that increasing the strength of the quadriceps muscles of the thigh has reduced DKV [30]. As observed in previous studies, a significant positive relationship was observed between DKV and the Q angle. The Q angle expanded when the patella moved inside, and the knee valgus increased. Increasing the quadriceps angle can lead to more exposure of the quadriceps muscles to compressive and shearing forces. Weakness in these muscles can build up DKV, resulting in less stability and misalignment in the knee joint [27].
Furthermore, a study conducted by Alvandi et al. in 2018 suggests that incorporating VF during a squat test can effectively aid in improving joint position and range of motion (ROM), thus relieving symptoms of knee dysfunction [19]. Using VF to control joint position and focus on range of motion (ROM) during exercises can significantly help this process. According to the results of the present study, the combination of SMT and VF enhances knee joint alignment, confirming the research hypothesis on this variable. These results are consistent with the reports by Alvandi and Letafatkar [19], Mozafaripour et al. [31], and Claiborne et al. [30].
One of the main complications of DKV is weakness in controlling the trunk, pelvis, knee, and ankle in both the frontal and horizontal planes [31]. Proprioception, which helps perceive body parts' location, movement, and action, was first defined by Sherrington in 1960 [10]. Any disturbance in the feedforward and feedback control, changes in muscle stiffness, and inefficiency in the SMT system can lead to problems in proprioception [20]. Misalignment can cause biomechanical changes that may affect the loads applied to the joint, hip, and knee feedback, muscle mechanical efficiency, and joint proprioception, ultimately resulting in changes in neuromuscular system function [32].
Thus declined proprioception, as one of the SM components, has been documented among the main side effects of DKV. According to Sherrington, proprioception can enhance neuromuscular control. Similarly, Janda has referred to proprioception as the most crucial component of SMT. Therefore, SMT aims to increase the proprioception of the information that enters the CNS from the cutaneous receptors of the feet, the sacroiliac joint, and the cervical spine. This helps stimulate subcortical pathways and facilitates automatically coordinated patterns. Additionally, in conjunction with VF, SMT helps improve proprioception by enhancing balance and postural stability [10].
Improving the feedback and motor control of the body can be achieved by enhancing proprioception through increasing afferent nerve messages and adding to nerve receptors. This can also regulate muscle stiffness, positively affecting joint movement and posture control [33]. The CNS can influence musculoskeletal pain syndromes, as developed by Janda’s approach. In the present study, knee joint proprioception improved after an eight-week SMT program, likely due to the strengthening of the neuromuscular system and the regeneration of neuromuscular structures [33]. SMT is a comprehensive treatment protocol for improving and rehabilitating the musculoskeletal system. Previous research has established its effects on proprioception compared to balance and strengthening exercises [9]. The results of SMT’s effects on proprioception in participants with DKV supported the second hypothesis.
The results of this study are consistent with the results of Yalfani et al. [9] and inconsistent with those reported by Tsauo et al. [34] and Pohl et al. [35]. These discrepancies can be attributed to differences in the training programs prescribed. Pohl et al. [35] indicated the dissimilarity of the prescribed training programs and they [35] found that SMT did not further affect proprioception due to the type of complication, short training time, and selected exercises.
Conclusion
According to the study, an eight-week program with SMT and VF improved knee joint proprioception and alignment in women with DKV. This indicates that such exercises positively affect DKV and are recommended due to their low cost, ease of access, and simplicity.
It should be noted that this study was conducted on women; therefore its results may not apply to men with DKV. Therefore, future studies should also explore the effects of VF-based SMT programs on men. It is also suggested that knee alignment be evaluated in other functional tasks.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Research Ethics Committee of Arak University (Code: IR.ARAKU.REC.1402.008) and registered by the Iranian Registry of Clinical Trials (IRCT) (No.: IRCT2020204046368N12).
Funding
This article is based on master's thesis of Fatemeh Azizi, approved by Department of Sports Injuries and Corrective Exercises, Faculty of Sports Sciences, Arak University and was financially supported by the Research and Funding of Arak University.
Authors' contributions
Conceptualization and methodology: Zahra Raeisi and Fatemeh Azizi; Data curation: Fatemeh Azizi; Original draft preparation: All authors; Supervision and project administration: Zahra Raeisi.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors are grateful and would like to thank all the participants for taking part in this study.
References
The knee joint is commonly considered a hinge-type joint with two degrees of freedom, flexion extension, and internal-external rotation [1]. Dynamic knee valgus (DKV) is the term used to describe the misalignment of the knee joint that occurs in the frontal plane. This misalignment can be caused by excessive femoral adduction, internal rotation, tibial abduction, and external rotation [2, 3]. This condition represents the kinematic changes in the thigh, knee, and ankle [4], induced by multiple factors, including increased femoral anteversion and tibial torsion, reduced hip abductor muscle strength, uncontrolled muscles of the lower pelvic area, more tibial mobility, a wider pelvis, and an excessive Q angle [5]. DKV has also been introduced as the leading cause of anterior cruciate ligament (ACL) injury [6]. Thus far, few studies have explored the prevalence rate of this movement impairment and its relationship with lower extremity mobility, knee pain, and gender; however, some reports have revealed a higher prevalence rate in women and adolescents than men and adults [1, 2, 7].
Impaired proprioception has been observed to be a significant manifestation after DKV [8]. Proprioception is the key component of the sensorimotor (SM) system, sourced mainly from muscle spindles. It plays a significant role in understanding the spatial and biomechanical position of different body parts [9]. It can also expand the strength and stability of the lower extremities [10]. DKV complications include improper dynamic control of body parts and the inability to control the trunk, pelvis, knees, and ankles in the frontal and horizontal planes [11].
This condition is one of the most common risk factors to predict acute injuries and those caused by lower extremity overuse, such as patellofemoral pain syndrome (PFPS), ACL injury, meniscus tear (or the knee cartilage damage), iliotibial band syndrome (ITBS), knee osteoarthritis (KOA), and a medial collateral ligament (MCL) injury [4]. Among these, ACL injury is a significant concern, causing short- and long-term recovery episodes and substantial financial burdens. A higher possibility of re-injuries, negative psychological effects, increased risk of KOA, and decreased sports performance have also been presented among the consequences of knee-related injuries in female athletes [6]. On the other hand, DKV causes patellar instability, which means that overloading due to increased activity adds to the pressure on the knee joint and causes PFPS [12].
Various exercise programs have been used to rehabilitate DKV, including sportometric [6], plyometric [4, 13, 14], neuromuscular [15], corrective [8, 16], and strengthening [11] exercises, each with their advantages. SM training (SMT) combines balance and proprioceptive exercises commonly used for rehabilitation [9]. The exercises aim to fix muscle imbalance, improve balance, and enhance the functions of the neuromuscular and proprioceptive systems. Some studies have even utilized such exercises to manage pain, improve typical functions in patients with chronic musculoskeletal pain, correct muscle imbalance, and increase postural control. This training program has been accordingly designed based on a series of exercises to challenge the SM system [9, 17], which helps boost functional adaptation in the neuromuscular system and leads to better intramuscular coordination, balance control, augmented proprioception, and lower postural fluctuations, and subsequently reduced injuries [9, 18]. The basic concept raised in this training program is attaching greater importance to the central nervous system (CNS) in regulating movements rather than accentuating muscle strength to maintain joint stability [12]. In other words, SMT aims to improve muscular endurance response but not strength [10].
It has been shown that feedback is one of the best tools for learning motor skills quickly and easily. Some studies have shown that verbal and visual feedback (VF) through videos and mirrors can positively affect DKV [19]. For instance, Alvandi et al. discovered that VF-based training during the single-leg squat test (SLST) can enhance movement accuracy and provoke changes in muscle activation strategies [19]. Therefore, exercises become more effective when accompanied by feedback. Moreover, SMT can help build pelvic stability [20], and proprioception [18], minimize pain and pelvic organ prolapse [20], and boost postural stability [22], as the main risk factors of DKV. Against this background, the present study investigated the effects of an eight-week SMT program with VF on knee joint proprioception and alignment in women with DKV. The research hypothesis was that practicing SMT simultaneously with receiving VF can effectively improve knee joint proprioception and alignment in women with DKV.
Materials and Methods
Study design
This is a randomized clinical trial. Participants were 30 female students with DKV who voluntarily participated after signing a consent form. The Randlist software was utilized to randomly allocate subjects to different study groups. The randomization method used was parallel. Initially, the software was provided with the number of participants and groups. Then, a code was assigned to each participant. Finally, the software randomly assigned a group to each code. The intervention group attended an eight-week SMT program with VF, while the control group continued their daily routines.
Based on the G*Power software output for the analysis of covariance (ANCOVA), the sample size was estimated to be 34 individuals, with an effect size of 0.5, a significance level of 0.05, and a test power of 0.8 [23]. Considering dropout (5%), 36 participants were recruited (18 in each group). However, six individuals were excluded from the analysis due to their absence at the post-test stage, three from the control group and three from the intervention group.
The study included only females aged between 18 and 30 diagnosed with DKV based on positive leg squat test (LST) results. The participants were required to have no history of knee surgeries within the past year, no lower extremity injuries in the past year, and no neuro-orthopedic or special conditions. Those who missed two consecutive or three non-consecutive training sessions or were absent during the post-test stage were excluded from the study.
Assessment
As a type of abnormal movement impairment, dynamic knee valgus (DKV) can be evaluated through various tests, such as jumping and landing tests and the double-leg squat test (DLST). The squat test, which requires no unique equipment and can be conducted at any location, can effectively screen for this condition [24]. The participants with DKV were included in this study when the medial border of their patella crossed the medial part of the big toe during the DLST. To achieve this, each participant performed the LST five times in a controlled manner under standard conditions. The overhead squat test was performed with legs shoulder-width apart, toes forward, and hands above the head, mimicking sitting on a chair. If DKV was observed during the overhead squat, i.e. in three out of five movements, the test results were considered positive [6].
Likewise, the knee joint angle repositioning error during the SLST was employed to evaluate knee joint proprioception. The participants completed this test by the 60-degree bend of the knee joint with a metronome of 60 beats per minute (including two flexion beats and two back-to-the-initial-position ones). Upon placing the goniometer on the lateral compartment (that is, one arm of the goniometer set along the outer side of the thigh and one arm along the leg), the participants were asked to remake a 60-degree knee flexion angle with eyes closed. The test was repeated three times, and the mean difference between the angle made by the participants and the standard one was then recorded as the proprioceptive error for each case [8]. The test re-test reliability of this test was reported as 0.90 in the previous study [8].
The single-leg landing test (SLLT) was administered to measure knee alignment. Participants were asked to stand on a box 40 cm above the ground with their non-dominant leg and keep the heel of their dominant leg on the front edge of the box. Then, they had to land on their dominant leg when the examiner asked them to, without bending or jumping vertically, and maintain their balance for 5 seconds after landing [13, 14]. The test had to be repeated three times with 30-s intervals between each repetition. A digital camera recorded the landing. It is essential to note that the participants were not given any instructions about the correct landing technique or provided with feedback on their performance [4, 6].
The camera was positioned parallel to the frontal plane, 366 cm away from the landing box on the base, at a height of 102 cm to ensure that the lower extremity was visible within the camera frame [4]. Landmarks were placed at the ankle joint center, patella, and anterior superior iliac spine (ASIS) for greater accuracy [20, 25]. The participants performed three repetitions of landing from the box at a normal speed during daily activities. Using the Kinovea software, the DKV angle was calculated at the moment of maximum knee flexion after landing by connecting two lines drawn from the ASIS to the patella and one passing from the patella to the center of the ankle joint. The knee alignment angle was then calculated by deducting the value obtained from 180. The average angle during three repetitions was recorded for each participant in the field [4, 20]. The reliability of the test for detecting DKV has been reported by Munro et al. to be 0.88-0.91 [26]. All variables were measured and evaluated one session before and after the exercises.
VF-based SMT
The intervention group completed the SMT program with VF within eight weeks, attending three sessions per week, each lasting 60 minutes. The training sessions included a 15-minute warm-up and stretching, 40 minutes of detailed exercises, and a 5-minute cool-down to return the body to rest. During this study, participants did not receive any other treatments, medications, or placebos. The exercises were performed using body weight, but resistance bands (TheraBand) were used to increase the intensity (Table 1). The principles and methods of the exercises were explained to the participants, and they were asked to maintain their regular practice throughout the training period. Additionally, all exercises were performed in front of mirrors with VF, allowing participants to control each movement by receiving feedback through the mirrors.
All exercises listed in Table 1 were completed during each session. The exercise routine began at the lowest level and gradually increased in intensity and volume over eight weeks. Figure 1 shows a sample of the exercises given.
The data were analyzed using IBM SPSS statistics software, version 26. The normality of the data was determined using the Shapiro-Wilk test. Since the data was normally distributed (P>0.05), the ANCOVA test was applied to remove intervening variables, adjust the pre-test stage scores, and make intergroup comparisons. A significance level of 0.05 was used for all tests. The data analyzer was not aware of the group classification. The information about the groups was provided to the data analyzer in the form of numbers 1 and 2 and for each participant with a code.
Results
Table 2 presents the demographic characteristics of participants in each group.
After analyzing the results of the intergroup comparisons using ANCOVA, with the pre-test stage scores as a covariate, it was found that the VF-based SMT program attended by participants in the intervention group significantly reduced knee joint proprioception (P=0.038, F=4.75, Eta=0.150) and improved knee alignment (P<0.001, F=24.13, Eta=0.472), as compared to those in the control group (Table 3).
Discussion
This study was conducted to examine the impact of an eight-week SMT program combined with VF on knee joint proprioception and alignment in women with DKV. The results indicated that SMT exercises with VF enhanced knee joint proprioception and alignment.
It is essential to note that any changes in the alignment of the lower extremities can lead to transformations in different body parts, resulting in deviations in various patterns [14, 27]. Disorders like DKV can affect the desired posture of the lower extremity, which can induce changes in the weight distribution in the knee. This issue can create pressure and variations in the knee joint position, reducing mechanical efficiency. Such an unfavorable situation can be the leading cause of multiple neuromuscular injuries. DKV is also a risk factor for various injuries, including ACL injury, PFPS, MCL injury, meniscus tear, ITBS, and KOA [24]. According to Ramezani et al., DKV refers to a range of kinematic changes in the lower extremity, including increased hip adduction and knee abduction, as well as internal rotation of the proximal components and external rotation of the distal ones. This can cause a maximized torque of the knee, which can increase the functional angle of the quadriceps muscles and the pressure of the external part of the patellofemoral joint [28]. Knee joint alignment can be assessed in both the sagittal and frontal planes. The knee joint should be examined from an anterior-posterior view in the frontal plane. The femoral angle in the inner part is also caused by the inclination angle in the proximal part of this bone. The longitudinal axis of the femur is thus about 10 degrees away from the longitudinal axis of the tibia, resulting in a physiological angle of approximately 170-175 degrees in adults with DKV in the frontal plane [29].
Performing exercises, such as SLST and DLST, forward and lateral lunges, single- and double-leg standing and landing on an unstable surface, and walking on soft and hard surfaces [20] have been effective ways to treat this condition. The training program implemented in this study included SMT, designed by Janda, aimed at escalating muscular endurance response rather than strength [10]. These exercises were a particular form of balance and proprioceptive to fix muscle imbalance, improve balance, and boost the functions of the neuromuscular and sensory systems [9, 17]. During the study, the interventions were split into three phases of exercise [20, 21]. In the first phase, the static phase, the participants were asked to maintain their center of gravity by using passive weight displacement or dealing with specific challenges requiring postural reflexive reactions to help with hip stability. In the second phase, the dynamic phase, the center of gravity challenges were executed dynamically, and some swing exercises were added to facilitate muscle stability. Finally, the participants performed functional progress and movements in the functional phase while maintaining hip stability. This phase was considered the final phase of the study [10].
Depending on the situation, SMT can be performed with or without tools and equipment. One of the main exercises in this program is short foot training, in which the internal longitudinal arch increases with the contraction of the plantar muscles while the toes are not contracted. According to Janda, this training can improve proprioception and postural stability [10]. Among other examples of the advanced form of SMT, balance exercises on bosu ball, Janda's balance sandals, and balance board should be mentioned. In this study, there was much attempt to improve the changes resulting from DKV and bring the body closer to the normal posture by a set of exercises, such as SLST and DLST, as well as forward and lateral lunges. Such exercises can strengthen the quadriceps and hip abductor muscles, reduce the femoral internal rotation angle, improve knee joint alignment, and minimize DKV [9, 20].
Claiborne et al. discovered a robust negative correlation between the isokinetic peak torque of the femoral abductor muscle and the external rotators and the DKV angle during the SLST. This means that increasing the strength of the quadriceps muscles of the thigh has reduced DKV [30]. As observed in previous studies, a significant positive relationship was observed between DKV and the Q angle. The Q angle expanded when the patella moved inside, and the knee valgus increased. Increasing the quadriceps angle can lead to more exposure of the quadriceps muscles to compressive and shearing forces. Weakness in these muscles can build up DKV, resulting in less stability and misalignment in the knee joint [27].
Furthermore, a study conducted by Alvandi et al. in 2018 suggests that incorporating VF during a squat test can effectively aid in improving joint position and range of motion (ROM), thus relieving symptoms of knee dysfunction [19]. Using VF to control joint position and focus on range of motion (ROM) during exercises can significantly help this process. According to the results of the present study, the combination of SMT and VF enhances knee joint alignment, confirming the research hypothesis on this variable. These results are consistent with the reports by Alvandi and Letafatkar [19], Mozafaripour et al. [31], and Claiborne et al. [30].
One of the main complications of DKV is weakness in controlling the trunk, pelvis, knee, and ankle in both the frontal and horizontal planes [31]. Proprioception, which helps perceive body parts' location, movement, and action, was first defined by Sherrington in 1960 [10]. Any disturbance in the feedforward and feedback control, changes in muscle stiffness, and inefficiency in the SMT system can lead to problems in proprioception [20]. Misalignment can cause biomechanical changes that may affect the loads applied to the joint, hip, and knee feedback, muscle mechanical efficiency, and joint proprioception, ultimately resulting in changes in neuromuscular system function [32].
Thus declined proprioception, as one of the SM components, has been documented among the main side effects of DKV. According to Sherrington, proprioception can enhance neuromuscular control. Similarly, Janda has referred to proprioception as the most crucial component of SMT. Therefore, SMT aims to increase the proprioception of the information that enters the CNS from the cutaneous receptors of the feet, the sacroiliac joint, and the cervical spine. This helps stimulate subcortical pathways and facilitates automatically coordinated patterns. Additionally, in conjunction with VF, SMT helps improve proprioception by enhancing balance and postural stability [10].
Improving the feedback and motor control of the body can be achieved by enhancing proprioception through increasing afferent nerve messages and adding to nerve receptors. This can also regulate muscle stiffness, positively affecting joint movement and posture control [33]. The CNS can influence musculoskeletal pain syndromes, as developed by Janda’s approach. In the present study, knee joint proprioception improved after an eight-week SMT program, likely due to the strengthening of the neuromuscular system and the regeneration of neuromuscular structures [33]. SMT is a comprehensive treatment protocol for improving and rehabilitating the musculoskeletal system. Previous research has established its effects on proprioception compared to balance and strengthening exercises [9]. The results of SMT’s effects on proprioception in participants with DKV supported the second hypothesis.
The results of this study are consistent with the results of Yalfani et al. [9] and inconsistent with those reported by Tsauo et al. [34] and Pohl et al. [35]. These discrepancies can be attributed to differences in the training programs prescribed. Pohl et al. [35] indicated the dissimilarity of the prescribed training programs and they [35] found that SMT did not further affect proprioception due to the type of complication, short training time, and selected exercises.
Conclusion
According to the study, an eight-week program with SMT and VF improved knee joint proprioception and alignment in women with DKV. This indicates that such exercises positively affect DKV and are recommended due to their low cost, ease of access, and simplicity.
It should be noted that this study was conducted on women; therefore its results may not apply to men with DKV. Therefore, future studies should also explore the effects of VF-based SMT programs on men. It is also suggested that knee alignment be evaluated in other functional tasks.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Research Ethics Committee of Arak University (Code: IR.ARAKU.REC.1402.008) and registered by the Iranian Registry of Clinical Trials (IRCT) (No.: IRCT2020204046368N12).
Funding
This article is based on master's thesis of Fatemeh Azizi, approved by Department of Sports Injuries and Corrective Exercises, Faculty of Sports Sciences, Arak University and was financially supported by the Research and Funding of Arak University.
Authors' contributions
Conceptualization and methodology: Zahra Raeisi and Fatemeh Azizi; Data curation: Fatemeh Azizi; Original draft preparation: All authors; Supervision and project administration: Zahra Raeisi.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors are grateful and would like to thank all the participants for taking part in this study.
References
- Philp F, Leboeuf F, Pandyan A, Stewart C. "Dynamic knee valgus" - Are we measuring what we think we're measuring? An evaluation of static and functional knee calibration methods for application in gait and clinical screening tests of the overhead squat and hurdle step. Gait & Posture. 2019; 70:298-304. [DOI:10.1016/j.gaitpost.2019.03.006] [PMID]
- Ramezani F, Saki F. [Electromyographic activity of the knee muscles during single-leg landing in female athletes with and without dynamic knee valgus (Persian)]. The Scientific Journal of Rehabilitation Medicine. 2020; 9(4):268-77. [DOI:10.22037/jrm.2020.113171.2330]
- Saki F, Romiani H, Ziya M, Gheidi N. The effects of gluteus medius and tibialis anterior kinesio taping on postural control, knee kinematics, and knee proprioception in female athletes with dynamic knee valgus. Physical Therapy in Sport. 2022; 53:84-90. [DOI:10.1016/j.ptsp.2021.11.010] [PMID]
- Saki F, Madhosh M. [Effect of eight weeks plyometric training on pelvic and knee alignment in female with dynamic knee valgus (Persian)]. Journal for Research in Sport Rehabilitation, 2019; 6(12):21-9. [DOI:10.22084/RSR.2019.17644.1415]
- Larwa J, Stoy C, Chafetz RS, Boniello M, Franklin C. Stiff landings, core stability, and dynamic knee valgus: A systematic review on documented anterior cruciate ligament ruptures in male and female athletes. International Journal of Environmental Research and Public Health. 2021; 18(7):3826. [DOI:10.3390/ijerph18073826] [PMID] [PMCID]
- Mohammadi H, Fakhraei Rad N. The effect of sportsmetrics on the performance and knee valgus during landing of female soccer players. Physical Treatments Journal 2022; 12(3):175-88. [DOI:10.32598/ptj.12.3.534.1]
- Sanchis GJB, Lopes JM, Assis SJC, Catão RLA, Santos TRT, Roncalli AGDCO. Dynamic knee valgus prevalence in children and its association with pain intensity, foot mobility, and sex- A cross-sectional study. Heliyon. 2022; 8(10):e10984. [DOI:10.1016/j.heliyon.2022.e10984] [PMID] [PMCID]
- Mozafaripour E, Seidi F, Minoonejad H, Bayattork M, Khoshroo F. The effectiveness of the comprehensive corrective exercise program on kinematics and strength of lower extremities in males with dynamic knee valgus: A parallel-group randomized wait-list controlled trial. BMC Musculoskeletal Disorders. 2022; 23(1):700. [DOI:10.1186/s12891-022-05652-8] [PMID] [PMCID]
- Yalfani A, Ahmadi M, Gandomi F. [The effect of twelve weeks of sensorimotor exercises on distribution plantar pressure variables and symmetry index in patients with patellofemoral pain syndrome: A randomized double-blind clinical trial (Persian)]. Studies in Medical Sciences. 2020; 31(6):445-58. [Link]
- Page P. Sensorimotor training: A “global” approach for balance training. Journal of Bodywork and Movement Therapies. 2006; 10(1):77-84. [DOI:10.1016/j.jbmt.2005.04.006]
- Alzahrani AM, Alzhrani M, Alshahrani SN, Alghamdi W, Alqahtani M, Alzahrani H. Is hip muscle strength associated with dynamic knee valgus in a healthy adult population? A systematic review. International Journal of Environmental Research and Public Health. 2021; 18(14):7669. [DOI:10.3390/ijerph18147669] [PMID] [PMCID]
- Wilczyński B, Zorena K, Ślęzak D. Dynamic knee valgus in single-leg movement tasks. potentially modifiable factors and exercise training options. A literature review. International Journal of Environmental Research and Public Health. 2020; 17(21):8208. [DOI:10.3390/ijerph17218208] [PMID][PMCID]
- Saki F, Madhosh M, Sedaghati P. The effect of selective plyometric training on the lower extremity functional performance indexes of female athletes with dynamic knee valgus. Physical Treatments. 2019; 9(1):31-8. [DOI:10.32598/PTJ.9.1.31]
- Saki F, Madhoosh M. [Effect of eight weeks plyometric training on hip strength in female athletes with dynamic knee valgus (Persian)]. Journal of Applied Exercise Physiology. 2019; 15(29):155-67. [Link]
- Babagoltabar Samakoush H, Norasteh A. [Effect of a neuromuscular training on knee valgus, range of motion and muscle strength of soccer players with dynamic knee valgus (Persian)]. The Scientific Journal of Rehabilitation Medicine. 2023; 12(3):486-503. [DOI:10.32598/SJRM.12.3.8]
- Mohammadi H, Daneshmandi H, Alizadeh M. Effect of corrective exercises program on strength-ROM, and performance in basketball players with dynamic knee valgus. The Scientific Journal of Rehabilitation Medicine. 2019; 8(3):29-41. [DOI:10.22037/JRM.2019.111286.1887]
- Blasco JM, Hernández-Guillen D, Domínguez-Navarro F, Acosta-Ballester Y, Alakhdar-Mohmara Y, Roig-Casasús S. Sensorimotor training prior total knee arthroplasty and effects on functional outcome: A systematic review and meta-analysis. Gait & Posture. 2021; 86:83-93. [DOI:10.1016/j.gaitpost.2021.03.001] [PMID]
- Ahmad I, Noohu MM, Verma S, Singla D, Hussain ME. Effect of sensorimotor training on balance measures and proprioception among middle and older age adults with diabetic peripheral neuropathy. Gait & Posture. 2019; 74:114-20. [DOI:10.1016/j.gaitpost.2019.08.018] [PMID]
- Alvandi F, Letafatkar A. [Comparison of the immediate effects of mirror, raw video, and real-time visual feedback on dynamic lower limb alignment and pain in individuals with patellofemoral pain syndrome (Persian)]. The Scientific Journal of Rehabilitation Medicine. 2018; 7(4):153-9. [DOI:10.22037/JRM.2018.111120.1775]
- Yalfani A, Ahmadi M, Gandomi F. The effects of 12-weeks of sensorimotor exercise on pain, strength, pelvic drop, and dynamic knee valgus in males with patellofemoral pain syndrome. Physical Treatments. 2020; 10(3):159-68. [DOI:10.32598/ptj.10.3.442.1]
- Ahmed AF. Effect of sensorimotor training on balance in elderly patients with knee osteoarthritis. Journal of Advanced Research. 2011; 2(4):305-11. [DOI:10.1016/j.jare.2011.02.001]
- Pereira LC, Ulrich B, Runhaar J, Bierma-Zeinstra S, Jolles BM, Favre J. Effects of step width modifications on the ambulatory kinetics in patients with medial knee osteoarthritis. Osteoarthritis and Cartilage. 2021; 29(Supplement 2):S11. [DOI:10.1016/j.joca.2021.05.020]
- Zarali A, Raeisi Z. Effects of combined exercises and short foot exercise with and without isometric hip abduction in women with flatfoot. Physical Treatments 2023; 13(1):35-44. [DOI:10.32598/ptj.13.1.474.2]
- Saki F, Ramezani F. [Comparison of range of motion and strength of hip muscles in female athletes with and without dynamic knee valgus (Persian)]. Avicenna Journal of Clinical Medicine. 2020; 27(2):100-9. [DOI:10.29252/ajcm.27.2.100]
- Ahmadi M, Yalfani A, Gandomi F, Rashid K. The effect of twelve-week neurofeedback training on pain, proprioception, strength and postural balance in men with patellofemoral pain syndrome: A double-blind randomized control trial. Journal of Rehabilitation Sciences & Research. 2020; 7(2):66-74. [DOI:10.30476/jrsr.2020.84868.1067]
- Munro A, Herrington L, Carolan M. Reliability of 2-dimensional video assessment of frontal-plane dynamic knee valgus during common athletic screening tasks. Journal of Sport Rehabilitation. 2012; 21(1):7-11. [DOI:10.1123/jsr.21.1.7] [PMID]
- Bakhtiari Khou S, Saki F. [Relationship between lower extremity anatomical alignment and core muscle endurance with peak knee valgus angle during landing-jump in female athletes (Persian)]. Studies in Sport Medicine. 2023; 14(34):49-70. [DOI:10.22089/smj.2023.12910.1609]
- Ramezani F, Saki F, Sohrabi T. [The effects of exercise interventions on dynamic knee valgus: A systematic review (Persian)]. Irtiqa Imini Pishgiri Masdumiyat. 2022; 10(1):59-48. [DOI:10.22037/iipm.v10i1.35973]
- Sahrmann S. Movement system impairment syndromes of the extremities, cervical and thoracic spines. Edinburgh: Elsevier Health Sciences; 2010. [Link]
- Claiborne TL, Armstrong CW, Gandhi V, Pincivero DM. Relationship between hip and knee strength and knee valgus during a single leg squat. Journal of Applied Biomechanics. 2006; 22(1):41-50. [DOI:10.1123/jab.22.1.41] [PMID]
- Mozafaripour E, Seidi F, Minoonejad H, Shirzad E. Effect of 8 weeks comprehensive corrective exercise program on knee proprioception and quality of one leg squat performance subjects with dynamic knee valgus. Studies in Sport Medicine. 2019; 11(25):17-34. [DOI:10.22089/smj.2019.6608.1343]
- Norasteh AA, Dehcheshmeh MF, Shamlou Kazemi A. [The role of dynamic knee valgus in occurrence of knee injuries: A review study (Persian)]. The Scientific Journal of Rehabilitation Medicine. 2023; 12(2):186-201. [DOI:10.32598/SJRM.12.2.10]
- Ahmadi M, Yalfani A, Gandomi F. Effect of twelve weeks of sensorimotor training on pain, improvement proprioception, muscle strength, and postural control in men with patellofemoral pain syndrome: A randomized single-blind clinical trial. The Scientific Journal of Rehabilitation Medicine. 2021; 10(1):1-13. [DOI:10.22037/jrm.2020.112859.2271]
- Tsauo JY, Cheng PF, Yang RS. The effects of sensorimotor training on knee proprioception and function for patients with knee osteoarthritis: A preliminary report. Clinical Rehabilitation. 2008; 22(5):448-57. [DOI:10.1177/0269215507084597] [PMID]
- Pohl T, Brauner T, Wearing S, Stamer K, Horstmann T. Effects of sensorimotor training volume on recovery of sensorimotor function in patients following lower limb arthroplasty. BMC Musculoskeletal Disorders. 2015; 16:195. [DOI:10.1186/s12891-015-0644-9] [PMID] [PMCID]
Type of Study: Research |
Subject:
General
Received: 2024/01/15 | Accepted: 2024/05/5 | Published: 2024/07/1
Received: 2024/01/15 | Accepted: 2024/05/5 | Published: 2024/07/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
