Tue, Jul 21, 2026
Volume 15, Issue 1 (Winter 2025)
PTJ 2025, 15(1): 27-40 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Jafarnezhadgero A, Hamlabadi M P, Eskandari S, Anushirvani S. Effects of Thoracolumbosacral Braces on Gait Knetics and Muscle Activities Before and After Puberty in Kyphosis Child. PTJ 2025; 15 (1) :27-40
URL: http://ptj.uswr.ac.ir/article-1-613-en.html
URL: http://ptj.uswr.ac.ir/article-1-613-en.html



1- Department of Sport Management and Biomechanics, Faculty of Education Sciences and Psychology, University of Mohaghegh Ardabili, Ardabil, Iran.
2- Department of Physical Education and Sport Sciences, Faculty of Education Sciences and Psychology, University of Mohaghegh Ardabili, Ardabil, Iran.
3- Department of Sport Physiology, Faculty of Education Sciences and Psychology, University of Mohaghegh Ardabili, Ardabil, Iran.
2- Department of Physical Education and Sport Sciences, Faculty of Education Sciences and Psychology, University of Mohaghegh Ardabili, Ardabil, Iran.
3- Department of Sport Physiology, Faculty of Education Sciences and Psychology, University of Mohaghegh Ardabili, Ardabil, Iran.
Full-Text [PDF 532 kb]
(581 Downloads)
| Abstract (HTML) (4861 Views)
Full-Text: (636 Views)
Introduction
The spine is a complex structure of the body, consisting of vertebrae, discs, muscles and many ligaments [1]. The weakness of spinal muscles could lead to static, dynamic and stature unbalance in different individuals called misalignment [2]. Spinal alignment in the sagittal plane is altered as a child grows. The sacrum position, the angle of thoracic kyphosis and lumbar lordosis change with growth [3]. Postural alterations lead to deformity in children’s and adolescents’ posture [4].
Increasing the angle of thoracic kyphosis has unfavorable results for the respiratory system [5]. Moreover, increased thoracic kyphosis is related to a decline in physical performance, postural control, lower walking speed, and reduced household activity performance [6, 7]. Bracing has been used as the most effective nonoperative treatment for individuals with mild idiopathic scoliosis and kyphosis [8, 9]. Previous studies have shown improvements in kyphosis angle after using braces [10, 11].
On the other hand, lower hamstring muscle strength [12] and delayed onset of vastus medialis activation [13]have been observed in girls at later compared to earlier stages of puberty. While these findings indicate that female pubertal development may be associated with potentially suboptimal changes in neuromuscular function, there is a lack of substantive evidence to support these claims [14]. There is currently limited knowledge about the walking characteristics of people with kyphosis before and after puberty and the effect of a thoracolumbar brace on walking characteristics. Accordingly, this study investigates the effects of two types of thoracolumbosacral braces on gait kinetics and muscle activities during walking before and after puberty in kyphosis children.
Materials and Methods
Study participants
A total of 40 participants (20 boys and 20 girls) with kyphosis volunteered and provided their written informed consent to participate in this study. The patients were recruited in December 2019 from physical therapy clinics in Ardabil City, Iran. An orthopedic surgeon in a local clinic assessed all subjects before selection. To estimate the maturity status of our participants, a maturity index (i.e. timing of maturation) was calculated [15]. This assessment is non-invasive and therefore of high practical relevance to predict years from peak height- velocity (PHV) as a measure of maturity offset. Previously, this method has proven to be a valid tool for the estimation of maturity status [16]. According to the analyses, all of the participants were classified as pre-PHV (Table 1).
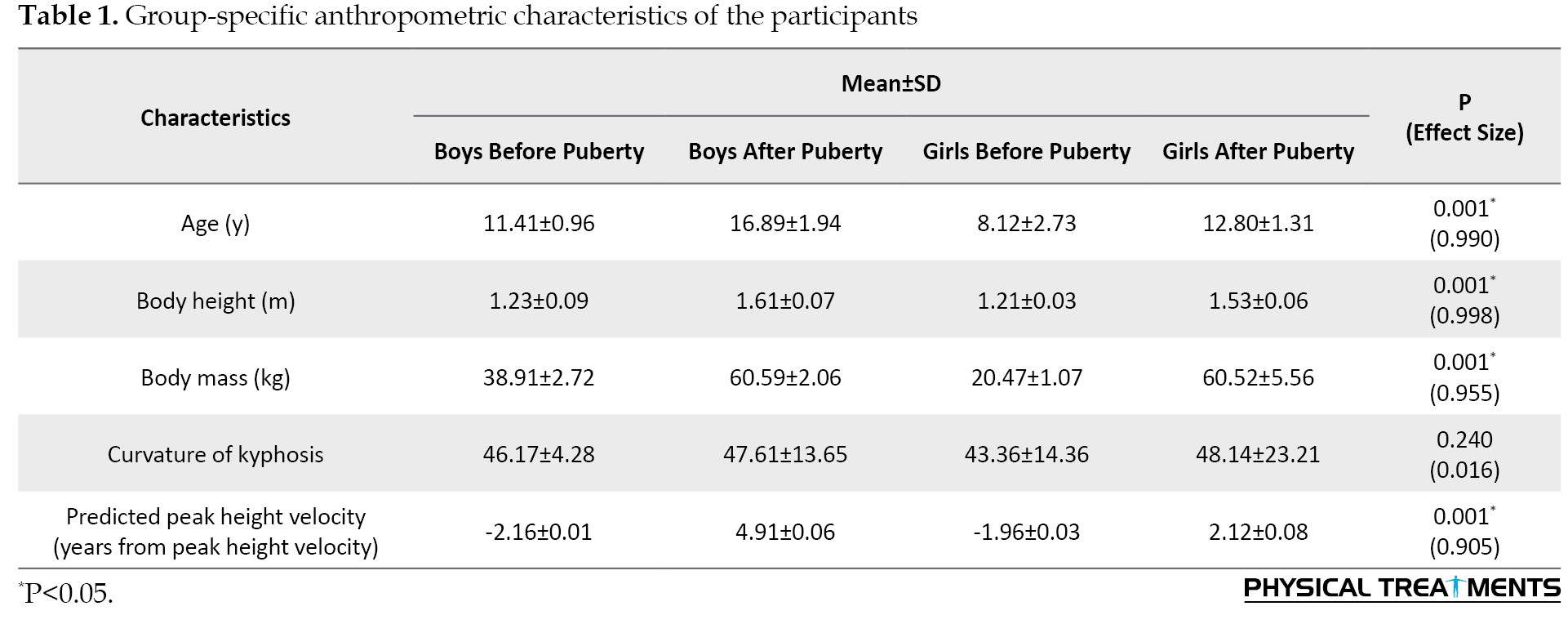
Thus, 40 boys and girls with kyphosis were divided into four groups.
Braces
To design a new corrective and wireless thoracolumbar brace, we made a thoraco-lumbo-sacral support. Its triangular design provides a good distribution of pressure on the shoulder, suitable for all ages, and adjustable hook and loop closure facilitates proper fastening [17]. The support structure of the present brace consists of six straps to adjust, an electronic enclosure, and two local stabilizers in which there is a bending sensor. The mobile application software (mobile app) of the designed brace could find out the bending angle and signal to the patient if the angle is more than the predefined angle by the vibration switch. To do this, the researcher must turn on the electronic circuit, then software and mobile phones connect with Bluetooth. Subsequently, the bending sensor data is transformed into the mobile app and it shows the amount of bending on your mobile phone.
Assessment of walking kinetics
A force plate (Bertec Corporation, Columbus, OH, United States) was used to record ground reaction force (GRF) data during walking at a sampling rate of 1000 Hz. The participants were asked to walk at a constant speed of ~1.00 m/s over an 18-m walkway. Three practice trials were performed to familiarize the participants with the test before performing five test trials with a 5-min rest between each trial to minimize the effects of fatigue. Kinetic data were processed as described by Jafarnezhadgero et al. (2022) [18]. GRFs were low pass filtered at 20 Hz (4th order Butterworth filter, zero lag). Specific gait characteristics (heel strike and toe-off) were identified using the Bertec force plate. For this purpose, a 10-N threshold was used to detect the stance phase of the gait cycle. The following dependent variables were extracted from GRF data Jafarnezhadgero et al. (2022) [18]. First (FZHC) and second vertical peak force (FZPO). Braking (FYHC) and propulsion forces (FYPO) were recorded from the anterior-posterior force curve. From the medial-lateral curve, we calculated the positive (lateral) peak (FXHC) which occurs right after heel contact. Moreover, we additionally assessed the negative peak which corresponds to the transfer of body mass to the contralateral limb (FXPO). GRF amplitudes were normalized to body weight (BW) and reported in %BW. The loading rate was defined as the slope between heel contact and FZHC on the vertical force curve. The free moment (FM) of the foot was also computed. Moreover, FM amplitudes were normalized concerning BW×height. All gait variables were averaged across five trials [19]. For stance phase analysis, GRF data were normalized to 101 data points.
Assessment of muscle activities
A wireless electromyography (EMG) system (EMG Pre-Amplifier, Biometrics Ltd., Nine Mile Point Ind. Est., Newport, United Kingdom) with eight pairs of bipolar Ag/AgCl surface electrodes (25 mm center-to-center distance, the input impedance of 100 MO, and common-mode rejection ratio of >110 dB) was used to record the activity of the tibialis anterior (TA), gastrocnemius medialis (Gas-M), biceps femoris (BF), semitendinosus (ST), vastus lateralis (VL), vastus medialis (VM), erector spinal (ES), and gluteus medius (Glut-M) muscles of the right leg [20]. A die-cut medical-grade double-sided adhesive tape (T350, Biometrics Ltd., Nine Mile Point Ind. Est., Newport, United Kingdom) was used to attach the electrodes to the muscle bellies. The raw EMG signals were digitized at 1000 Hz and streamed via Bluetooth to a computer for further analysis. According to the European recommendations for surface EMG (SENIAM), the skin surface was shaved and cleaned with alcohol (70% Ethanol–C2H5OH) over the selected muscles [20]. Thereafter, the skin was gently abraded before electrode placement [20]. GRF and EMG data were synchronized using the Nexus software, version 2.13 (Oxford Metrics, Oxford, United Kingdom). For EMG analyses, the gait cycle was divided into the following phases: Loading phase (0-20% of the gait cycle), mid-stance (20-47% of the gait cycle), and push-off (47-70% of the gait cycle) [21]. Using a handheld dynamometer, maximum voluntary isometric contraction (MVIC) was assessed for each recorded muscle to normalize EMG during walking to MVIC. All normalization procedures were realized following recommendations from a study [22]. For example, the participants were encouraged to perform the tests at maximal effort [23]. Three test trials were conducted with 1-2 min rest periods in between tests [23]. For measuring MVIC, an isometric belt (where the joint is locked) was used (set for zero velocity) [23]. This instrument is important to control testing factors that can influence the output and facilitate the production of maximal contraction. The maximum value of the MVIC test was considered for normalization purposes [22, 23].
Statistical analysis
The prior calculation of the sample size indicated that at least 40 subjects were required. For calculation, G*Power software, version 3.1.2.9, was used with a statistical power of 0.80 at an effect size of 0.80 with an α level of 0.05 and the respective statistical test based on a related study that examined walking in kyphosis patients [24, 25]. The Shapiro-Wilk test was used to confirm the normal distribution of data. The statistical analysis was done by two-way analysis of variance with repeated measures. Additionally, the effect sizes were determined by partial Eta-squared (η2p). The significance level was set at P<0.05. All analyses were performed using the SPSS software, version 26.
Results
Walking kinetics
The results demonstrated significant main effects of brace for FZHC (P=0.021, d=0.348), FZPO (P=0.024, d=0.317), FYPO (P=0.001, d=0.768), FXPO (P=0.001, d=0.513), impulse (imp)fx (P=0.011, d=0.519), ImpFZ (P=0.004, d=0.547), FMMAX (P=0.001, d=0.716), and FMMin (P=0.009, d=0.809). The paired-wise comparison revealed significantly greater FYPO, FXPO, ImpFZ, FMMAX, and FMMin (Table 1). The findings showed significant main effect of group for FZHC (P=0.021, d=0.348), FZPO (P=0.024, d=0.317), FYHC (P=0.001, d=0.768), FYPO (P=0.001, d=0.768), FXHC (P=0.001, d=0.513), time to reach the peak FYHC (P=0.001, d=0.513), time to reach the peak FYPO (P=0.001, d=0.513), ImpFY (P=0.011, d=0.519), ImpFZ (P=0.004, d=0.547) and FMMAX (P=0.001, d=0.716). The paired-wise comparison revealed significantly lower FZHC, FZPO, and ImpFX activities in the sensory support group than in the non-support group. Furthermore, significant group-by-time interactions were found for all variables (Table 2).


Muscle activities
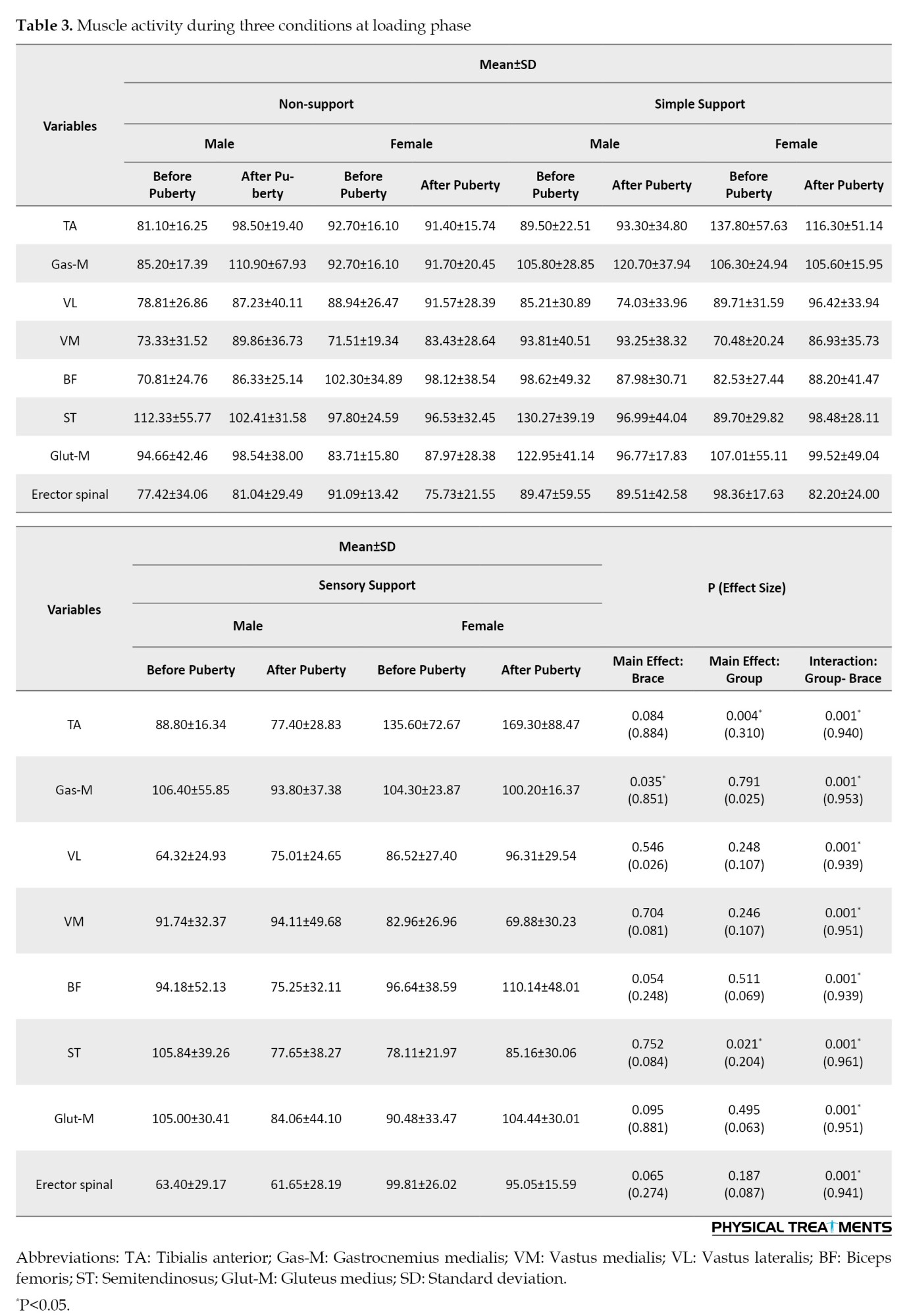
The results demonstrated significant main effects of brace for gas-med activity during the loading phase (P=0.035, d=0.581). The paired-wise comparison revealed significantly greater gas-med activity with brace increases. The findings showed a significant main effect of the group for glut-mid (P=0.004, d=0.310) and semitendinosus (P=0.021, d=0.204) during the loading phase. Meanwhile, the paired-wise comparison revealed significantly greater TA activity in the sensory support group than in the non-support group. Furthermore, significant group-by-time interactions were found for all muscle activity during the loading phase (P<0.05) (Table 3).
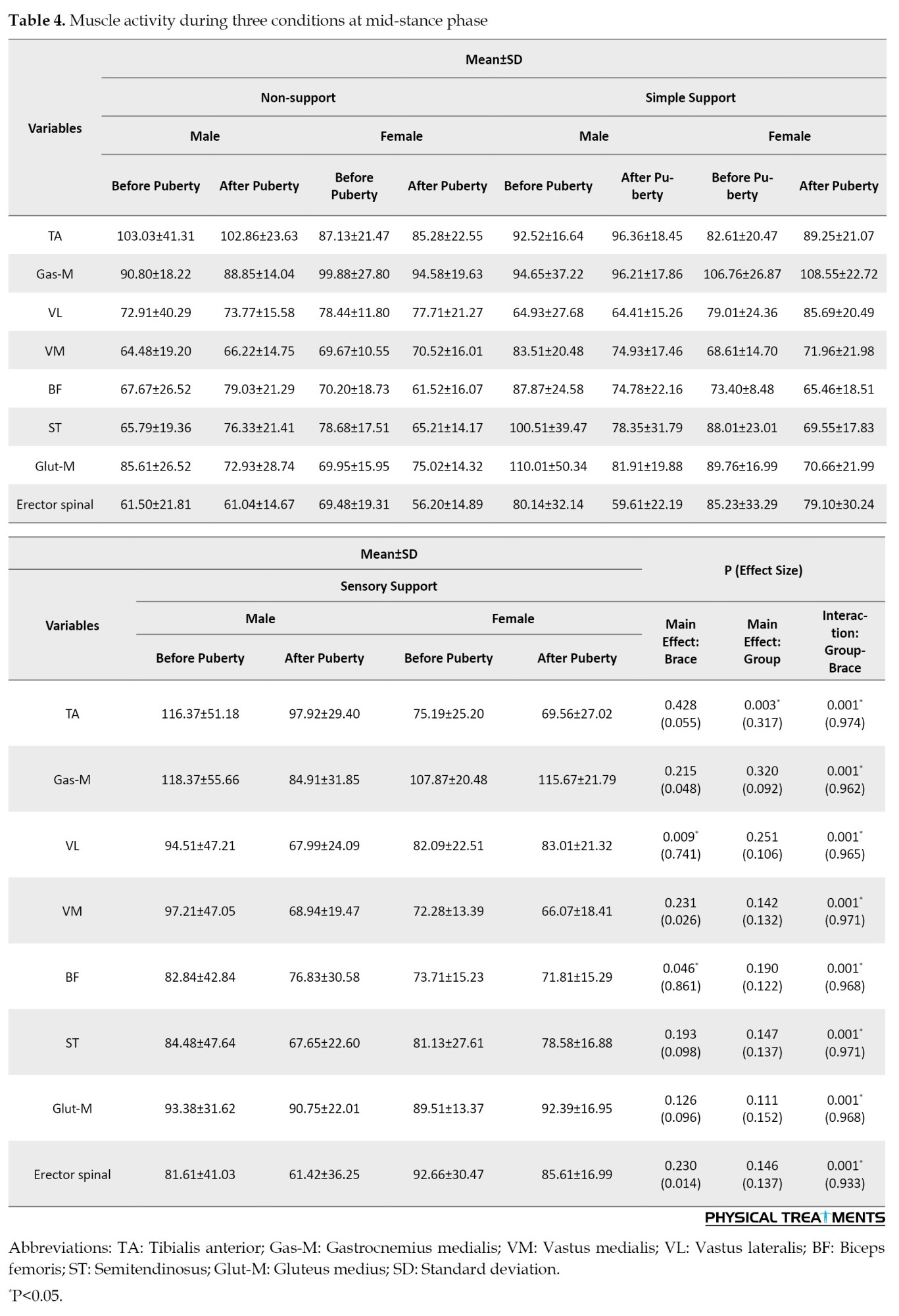
The results demonstrated significant main effects of brace for VL (P=0.009, d=0.741) and BF (P=0.046, d=0.861) activity during the mid-stance phase. The paired-wise comparison revealed significantly greater VL and BF activities with brace increases. The findings showed a significant main effect of the group for TA (P=0.003, d=0.317) during the mid-stance phase. Meanwhile, the paired-wise comparison revealed significantly greater TA activity in the Sensory support group than in the non-support group. Furthermore, significant group-by-time interactions were found for all muscle activity during the mid-stance phase (P<0.05) (Table 4).
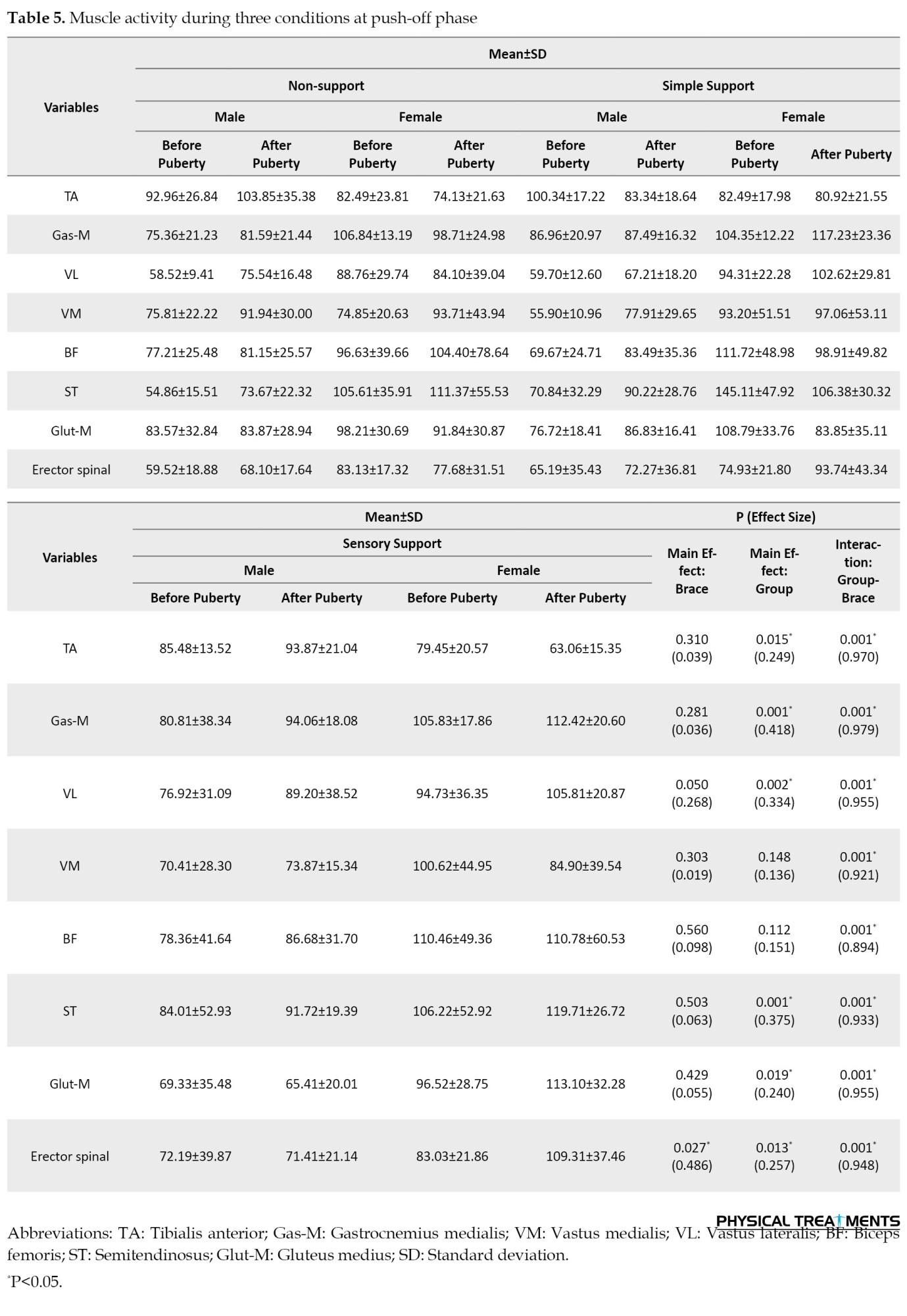
The findings showed a significant main effect of group for TA (P=0.015, d=0.249), gas-mid (P=0.001, d=0.418), VL (P=0.002, d=0.334), semitendinosus (P=0.001, d=0.375), Gult-Mid (P=0.019, d=0.240) and erector spinal (P=0.013, d=0.257) during push-off phase. The paired-wise comparison revealed significantly greater Gas-Med, Gult-Mid, and erector spinal activities in the sensory support group than in the non-support group. Furthermore, significant group-by-time interactions were found for all muscle activity during the mid-stance phase (P<0.05) (Table 5).
The results demonstrated significant main effects of the brace for TA activity during the swing phase (P=0.001, d=0.578). The paired-wise comparison revealed significantly lower TA activity with brace increases. Findings showed a significant main effect of group for VM (P=0.008, d=0.279), BF (P=0.001, d=0.463), glut-M (P=0.001, d=0.402), and erector spinal (P=0.004, d=0.309) during swing phase. The paired-wise comparison revealed significantly greater VM, BF, Glut-M, and erector spinal activities in the sensory support group than in the non-support group. Furthermore, significant group-by-time interactions were found for all muscle activity during the swing phase (P<0.05) (Table 6).

Discussion
This study investigates the effects of two types of throcolumbosacral braces on gait kinetics and muscle activity before and after puberty in kyphosis patients.
Walking kinetics
The results suggest that the bracing decreased GRF during walking. There is sufficient evidence of the association between increased GRF and lower extremity injury [26]. This result is consistent with previous studies suggesting that bracing could decrease GRF during walking [27]. Farahpour et al. argued that increased GRF during walking might lead to lumbar dysfunction [24]. From this point of view, our therapy may result in clinical improvement in patients with kyphosis. The findings demonstrated bracing increases the first lateral ground reaction forces during heel contact and push-off phase by 17.8% and 20.79%, respectively.
Muscle activities
The results of this study showed significant increases in medium- to large-sized bracing effects for gas-med and BF activities during the loading phase of walking and VL, BF, and TA activities at mid-stance, gas-mid, VL, ST, glut-mid, and erector spinal activities at push-off phase, and VM, BF, and erector spinal activities at swing phase. The activity of the TA muscle in this phase was not associated with the strong coupling activation of the tibialis posterior muscle [28]. In a study where electromyography and cinematography were synchronized [29], the authors reported that there was a high level of VL and VM activity at the initial stance phase, followed by a co-contraction of the ankle muscle to ensure stability, allowing for the downward force of the walker to be absorbed and total body stabilization achieved in preparation for the drive phase. On the other these authors also reported increasing EMG activity of the BF in this early support phase, with EMG activity rising to a higher level about middle stance and related to an increase in flexion of knee joint [29] are in consistent with the results of our study.
Also, the results of our study showed significant decreases and large-sized training effects for TA and Glut-M activities during the push-off phase and TA activities during walking at the swing phase.
Conclusion
Higher walking speed, lower vertical ground reaction force, effective muscle activity with braces, and difference loading rate in the bracing group compared with the without bracing group demonstrate the improvement of gait efficiency in the periods before and after puberty.
Ethical Considerations
Compliance with ethical guidelines
Ethical approval for research involving human participants was obtained from the Ardabil University of Medical Sciences, Ardabil, Iran (Code: IR.ARUMS.REC.1399.255).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors contributed equally to the conception and design of the study, data collection and analysis, interpretation of the results and drafting of the manuscript. Each author approved the final version of the manuscript for submission.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors thanks all subjects who volunteered to participate in the present study.
References
The spine is a complex structure of the body, consisting of vertebrae, discs, muscles and many ligaments [1]. The weakness of spinal muscles could lead to static, dynamic and stature unbalance in different individuals called misalignment [2]. Spinal alignment in the sagittal plane is altered as a child grows. The sacrum position, the angle of thoracic kyphosis and lumbar lordosis change with growth [3]. Postural alterations lead to deformity in children’s and adolescents’ posture [4].
Increasing the angle of thoracic kyphosis has unfavorable results for the respiratory system [5]. Moreover, increased thoracic kyphosis is related to a decline in physical performance, postural control, lower walking speed, and reduced household activity performance [6, 7]. Bracing has been used as the most effective nonoperative treatment for individuals with mild idiopathic scoliosis and kyphosis [8, 9]. Previous studies have shown improvements in kyphosis angle after using braces [10, 11].
On the other hand, lower hamstring muscle strength [12] and delayed onset of vastus medialis activation [13]have been observed in girls at later compared to earlier stages of puberty. While these findings indicate that female pubertal development may be associated with potentially suboptimal changes in neuromuscular function, there is a lack of substantive evidence to support these claims [14]. There is currently limited knowledge about the walking characteristics of people with kyphosis before and after puberty and the effect of a thoracolumbar brace on walking characteristics. Accordingly, this study investigates the effects of two types of thoracolumbosacral braces on gait kinetics and muscle activities during walking before and after puberty in kyphosis children.
Materials and Methods
Study participants
A total of 40 participants (20 boys and 20 girls) with kyphosis volunteered and provided their written informed consent to participate in this study. The patients were recruited in December 2019 from physical therapy clinics in Ardabil City, Iran. An orthopedic surgeon in a local clinic assessed all subjects before selection. To estimate the maturity status of our participants, a maturity index (i.e. timing of maturation) was calculated [15]. This assessment is non-invasive and therefore of high practical relevance to predict years from peak height- velocity (PHV) as a measure of maturity offset. Previously, this method has proven to be a valid tool for the estimation of maturity status [16]. According to the analyses, all of the participants were classified as pre-PHV (Table 1).
Thus, 40 boys and girls with kyphosis were divided into four groups.
Braces
To design a new corrective and wireless thoracolumbar brace, we made a thoraco-lumbo-sacral support. Its triangular design provides a good distribution of pressure on the shoulder, suitable for all ages, and adjustable hook and loop closure facilitates proper fastening [17]. The support structure of the present brace consists of six straps to adjust, an electronic enclosure, and two local stabilizers in which there is a bending sensor. The mobile application software (mobile app) of the designed brace could find out the bending angle and signal to the patient if the angle is more than the predefined angle by the vibration switch. To do this, the researcher must turn on the electronic circuit, then software and mobile phones connect with Bluetooth. Subsequently, the bending sensor data is transformed into the mobile app and it shows the amount of bending on your mobile phone.
Assessment of walking kinetics
A force plate (Bertec Corporation, Columbus, OH, United States) was used to record ground reaction force (GRF) data during walking at a sampling rate of 1000 Hz. The participants were asked to walk at a constant speed of ~1.00 m/s over an 18-m walkway. Three practice trials were performed to familiarize the participants with the test before performing five test trials with a 5-min rest between each trial to minimize the effects of fatigue. Kinetic data were processed as described by Jafarnezhadgero et al. (2022) [18]. GRFs were low pass filtered at 20 Hz (4th order Butterworth filter, zero lag). Specific gait characteristics (heel strike and toe-off) were identified using the Bertec force plate. For this purpose, a 10-N threshold was used to detect the stance phase of the gait cycle. The following dependent variables were extracted from GRF data Jafarnezhadgero et al. (2022) [18]. First (FZHC) and second vertical peak force (FZPO). Braking (FYHC) and propulsion forces (FYPO) were recorded from the anterior-posterior force curve. From the medial-lateral curve, we calculated the positive (lateral) peak (FXHC) which occurs right after heel contact. Moreover, we additionally assessed the negative peak which corresponds to the transfer of body mass to the contralateral limb (FXPO). GRF amplitudes were normalized to body weight (BW) and reported in %BW. The loading rate was defined as the slope between heel contact and FZHC on the vertical force curve. The free moment (FM) of the foot was also computed. Moreover, FM amplitudes were normalized concerning BW×height. All gait variables were averaged across five trials [19]. For stance phase analysis, GRF data were normalized to 101 data points.
Assessment of muscle activities
A wireless electromyography (EMG) system (EMG Pre-Amplifier, Biometrics Ltd., Nine Mile Point Ind. Est., Newport, United Kingdom) with eight pairs of bipolar Ag/AgCl surface electrodes (25 mm center-to-center distance, the input impedance of 100 MO, and common-mode rejection ratio of >110 dB) was used to record the activity of the tibialis anterior (TA), gastrocnemius medialis (Gas-M), biceps femoris (BF), semitendinosus (ST), vastus lateralis (VL), vastus medialis (VM), erector spinal (ES), and gluteus medius (Glut-M) muscles of the right leg [20]. A die-cut medical-grade double-sided adhesive tape (T350, Biometrics Ltd., Nine Mile Point Ind. Est., Newport, United Kingdom) was used to attach the electrodes to the muscle bellies. The raw EMG signals were digitized at 1000 Hz and streamed via Bluetooth to a computer for further analysis. According to the European recommendations for surface EMG (SENIAM), the skin surface was shaved and cleaned with alcohol (70% Ethanol–C2H5OH) over the selected muscles [20]. Thereafter, the skin was gently abraded before electrode placement [20]. GRF and EMG data were synchronized using the Nexus software, version 2.13 (Oxford Metrics, Oxford, United Kingdom). For EMG analyses, the gait cycle was divided into the following phases: Loading phase (0-20% of the gait cycle), mid-stance (20-47% of the gait cycle), and push-off (47-70% of the gait cycle) [21]. Using a handheld dynamometer, maximum voluntary isometric contraction (MVIC) was assessed for each recorded muscle to normalize EMG during walking to MVIC. All normalization procedures were realized following recommendations from a study [22]. For example, the participants were encouraged to perform the tests at maximal effort [23]. Three test trials were conducted with 1-2 min rest periods in between tests [23]. For measuring MVIC, an isometric belt (where the joint is locked) was used (set for zero velocity) [23]. This instrument is important to control testing factors that can influence the output and facilitate the production of maximal contraction. The maximum value of the MVIC test was considered for normalization purposes [22, 23].
Statistical analysis
The prior calculation of the sample size indicated that at least 40 subjects were required. For calculation, G*Power software, version 3.1.2.9, was used with a statistical power of 0.80 at an effect size of 0.80 with an α level of 0.05 and the respective statistical test based on a related study that examined walking in kyphosis patients [24, 25]. The Shapiro-Wilk test was used to confirm the normal distribution of data. The statistical analysis was done by two-way analysis of variance with repeated measures. Additionally, the effect sizes were determined by partial Eta-squared (η2p). The significance level was set at P<0.05. All analyses were performed using the SPSS software, version 26.
Results
Walking kinetics
The results demonstrated significant main effects of brace for FZHC (P=0.021, d=0.348), FZPO (P=0.024, d=0.317), FYPO (P=0.001, d=0.768), FXPO (P=0.001, d=0.513), impulse (imp)fx (P=0.011, d=0.519), ImpFZ (P=0.004, d=0.547), FMMAX (P=0.001, d=0.716), and FMMin (P=0.009, d=0.809). The paired-wise comparison revealed significantly greater FYPO, FXPO, ImpFZ, FMMAX, and FMMin (Table 1). The findings showed significant main effect of group for FZHC (P=0.021, d=0.348), FZPO (P=0.024, d=0.317), FYHC (P=0.001, d=0.768), FYPO (P=0.001, d=0.768), FXHC (P=0.001, d=0.513), time to reach the peak FYHC (P=0.001, d=0.513), time to reach the peak FYPO (P=0.001, d=0.513), ImpFY (P=0.011, d=0.519), ImpFZ (P=0.004, d=0.547) and FMMAX (P=0.001, d=0.716). The paired-wise comparison revealed significantly lower FZHC, FZPO, and ImpFX activities in the sensory support group than in the non-support group. Furthermore, significant group-by-time interactions were found for all variables (Table 2).
Muscle activities
The results demonstrated significant main effects of brace for gas-med activity during the loading phase (P=0.035, d=0.581). The paired-wise comparison revealed significantly greater gas-med activity with brace increases. The findings showed a significant main effect of the group for glut-mid (P=0.004, d=0.310) and semitendinosus (P=0.021, d=0.204) during the loading phase. Meanwhile, the paired-wise comparison revealed significantly greater TA activity in the sensory support group than in the non-support group. Furthermore, significant group-by-time interactions were found for all muscle activity during the loading phase (P<0.05) (Table 3).
The results demonstrated significant main effects of brace for VL (P=0.009, d=0.741) and BF (P=0.046, d=0.861) activity during the mid-stance phase. The paired-wise comparison revealed significantly greater VL and BF activities with brace increases. The findings showed a significant main effect of the group for TA (P=0.003, d=0.317) during the mid-stance phase. Meanwhile, the paired-wise comparison revealed significantly greater TA activity in the Sensory support group than in the non-support group. Furthermore, significant group-by-time interactions were found for all muscle activity during the mid-stance phase (P<0.05) (Table 4).
The findings showed a significant main effect of group for TA (P=0.015, d=0.249), gas-mid (P=0.001, d=0.418), VL (P=0.002, d=0.334), semitendinosus (P=0.001, d=0.375), Gult-Mid (P=0.019, d=0.240) and erector spinal (P=0.013, d=0.257) during push-off phase. The paired-wise comparison revealed significantly greater Gas-Med, Gult-Mid, and erector spinal activities in the sensory support group than in the non-support group. Furthermore, significant group-by-time interactions were found for all muscle activity during the mid-stance phase (P<0.05) (Table 5).
The results demonstrated significant main effects of the brace for TA activity during the swing phase (P=0.001, d=0.578). The paired-wise comparison revealed significantly lower TA activity with brace increases. Findings showed a significant main effect of group for VM (P=0.008, d=0.279), BF (P=0.001, d=0.463), glut-M (P=0.001, d=0.402), and erector spinal (P=0.004, d=0.309) during swing phase. The paired-wise comparison revealed significantly greater VM, BF, Glut-M, and erector spinal activities in the sensory support group than in the non-support group. Furthermore, significant group-by-time interactions were found for all muscle activity during the swing phase (P<0.05) (Table 6).
Discussion
This study investigates the effects of two types of throcolumbosacral braces on gait kinetics and muscle activity before and after puberty in kyphosis patients.
Walking kinetics
The results suggest that the bracing decreased GRF during walking. There is sufficient evidence of the association between increased GRF and lower extremity injury [26]. This result is consistent with previous studies suggesting that bracing could decrease GRF during walking [27]. Farahpour et al. argued that increased GRF during walking might lead to lumbar dysfunction [24]. From this point of view, our therapy may result in clinical improvement in patients with kyphosis. The findings demonstrated bracing increases the first lateral ground reaction forces during heel contact and push-off phase by 17.8% and 20.79%, respectively.
Muscle activities
The results of this study showed significant increases in medium- to large-sized bracing effects for gas-med and BF activities during the loading phase of walking and VL, BF, and TA activities at mid-stance, gas-mid, VL, ST, glut-mid, and erector spinal activities at push-off phase, and VM, BF, and erector spinal activities at swing phase. The activity of the TA muscle in this phase was not associated with the strong coupling activation of the tibialis posterior muscle [28]. In a study where electromyography and cinematography were synchronized [29], the authors reported that there was a high level of VL and VM activity at the initial stance phase, followed by a co-contraction of the ankle muscle to ensure stability, allowing for the downward force of the walker to be absorbed and total body stabilization achieved in preparation for the drive phase. On the other these authors also reported increasing EMG activity of the BF in this early support phase, with EMG activity rising to a higher level about middle stance and related to an increase in flexion of knee joint [29] are in consistent with the results of our study.
Also, the results of our study showed significant decreases and large-sized training effects for TA and Glut-M activities during the push-off phase and TA activities during walking at the swing phase.
Conclusion
Higher walking speed, lower vertical ground reaction force, effective muscle activity with braces, and difference loading rate in the bracing group compared with the without bracing group demonstrate the improvement of gait efficiency in the periods before and after puberty.
Ethical Considerations
Compliance with ethical guidelines
Ethical approval for research involving human participants was obtained from the Ardabil University of Medical Sciences, Ardabil, Iran (Code: IR.ARUMS.REC.1399.255).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
All authors contributed equally to the conception and design of the study, data collection and analysis, interpretation of the results and drafting of the manuscript. Each author approved the final version of the manuscript for submission.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors thanks all subjects who volunteered to participate in the present study.
References
- Rezvankhah N, Alizadeh M H, Kordi M R. The effect of four months of detraining following eight months of corrective exercises on lumbar lordosis of schoolgirls. Annals of Applied Sport Science. 2013; 1(2):19-24. [Link]
- Yazici AG, Mohammadi M. Exercise. The effect of corrective exercises on the thoracic kyphosis and lumbar lordosis of boy students. Turkish Journal of Sport and Exercise. 2017; 19(2):177-81. [DOI:10.15314/tsed.293311]
- Cil A, Yazici M, Uzumcugil A, Kandemir U, Alanay A, Alanay Y, et al. The evolution of sagittal segmental alignment of the spine during childhood. Spine. 2005; 30(1):93-100. [DOI:10.1097/01.brs.0000149074.21550.32] [PMID]
- Kratenová J, Zejglicová K, Malý M, Filipová V. Prevalence and risk factors of poor posture in school children in the Czech Republic. The Journal of School Health. 2007; 77(3):131-7. [DOI:10.1111/j.1746-1561.2007.00182.x] [PMID]
- Rajabi R, Seidi F, Mohamadi F. Which method is accurate when using the flexible ruler to measure the lumbar curvature angle”? deep point or mid-point of arch? World Applied Sciences Journal. 2008; 4(6):849-52. [Link]
- Balzini L, Vannucchi L, Benvenuti F, Benucci M, Monni M, Cappozzo A, et al. Clinical characteristics of flexed posture in elderly women. Journal of the American Geriatrics Society. 2003; 51(10):1419-26. [DOI:10.1046/j.1532-5415.2003.51460.x] [PMID]
- Ryan SD, Fried LP. The impact of kyphosis on daily functioning. Journal of the American Geriatrics Society. 1997; 45(12):1479-86. [DOI:10.1111/j.1532-5415.1997.tb03199.x] [PMID]
- Katz DE, Richards BS, Browne RH, Herring JA. A comparison between the Boston brace and the Charleston bending brace in adolescent idiopathic scoliosis. Spine. 1997; 22(12):1302-12. [DOI:10.1097/00007632-199706150-00005] [PMID]
- Lonstein JE, Winter RB. The Milwaukee brace for the treatment of adolescent idiopathic scoliosis. A review of one thousand and twenty patients. The Journal of Bone and Joint Surgery. 1994; 76(8):1207-21. [DOI:10.2106/00004623-199408000-00011] [PMID]
- Pfeifer M, Begerow B, Minne HW. Effects of a new spinal orthosis on posture, trunk strength, and quality of life in women with postmenopausal osteoporosis: A randomized trial. American Journal of Physical Medicine & Rehabilitation. 2004; 83(3):177-86. [DOI:10.1097/01.PHM.0000113403.16617.93] [PMID]
- Hamlabadi MP, Jafarnezhadgero A. The effect of 8 sessions of Thera-band exercises on the joint position sense of the knee and ankle in diabetic patients with osteoarthritis of the knee. Journal of Arak University of Medical Sciences. 2021; 12(1):31-43. [Link]
- Wild CY, Steele JR, Munro BJ. Insufficient hamstring strength compromises landing technique in adolescent girls. Medicine and Science in Sports and Exercise. 2013; 45(3):497-505. [DOI:10.1249/MSS.0b013e31827772f6] [PMID]
- Wild CY, Munro BJ, Steele JR. How young girls change their landing technique throughout the adolescent growth spurt. The American Journal of Sports Medicine. 2016; 44(5):1116-23. [DOI:10.1177/0363546516629419] [PMID]
- Sayer TA, Hinman RS, Paterson KL, Bennell KL, Hall M, Allison K, Bryant AL. Running-related muscle activation patterns and tibial acceleration across puberty. Journal of Electromyography and Kinesiology. 2020; 50:102381. [DOI:10.1016/j.jelekin.2019.102381] [PMID]
- Moore SA, McKay HA, Macdonald H, Nettlefold L, Baxter-Jones AD, Cameron N, et al. Enhancing a somatic maturity prediction model. Medicine and Science in Sports and Exercise. 2015; 47(8):1755-64. [DOI:10.1249/MSS.0000000000000588] [PMID]
- Malina RM, Bouchard C, Bar-Or O. Growth, maturation, and physical activity. Champaign: Human kinetics; 2004. [DOI:10.5040/9781492596837]
- Piran haml abadi M, Jafarnezhadgero A, Anoushirvani S. A preliminary design of new corrective and wireless thoracolumbar bracing for individuals with functional thoracolumbar kyphosis. Journal of Advanced Sport Technology. 2019; 3(1):33-6. [Link]
- Jafarnezhadgero AA, Hamlabadi MP, Sajedi H, Granacher U. Recreational runners who recovered from COVID-19 show different running kinetics and muscle activities compared with healthy controls. Gait & Posture. 2022; 91:260-5. [DOI:10.1016/j.gaitpost.2021.11.002] [PMID] [PMCID]
- Jafarnezhadgero A, Fatollahi A, Amirzadeh N, Siahkouhian M, Granacher U. Ground reaction forces and muscle activity while walking on sand versus stable ground in individuals with pronated feet compared with healthy controls. Plos One. 2019; 14(9):e0223219. [DOI:10.1371/journal.pone.0223219] [PMID] [PMCID]
- Hermens HJ, Freriks B, Merletti R, Stegeman D, Blok J, Rau G, et al. European recommendations for surface electromyography. Roessingh Research and Development. 1999; 8(2):13-54. [Link]
- Jafarnezhadgero A, Ghorbanloo F, Fatollahi A, Dionisio VC, Granacher U. Effects of an elastic resistance band exercise program on kinetics and muscle activities during walking in young adults with genu valgus: A double-blinded randomized controlled trial. Clinical Biomechanics. 2021; 81:105215. [DOI:10.1016/j.clinbiomech.2020.105215] [PMID]
- Emami S, Jafarnezhadgero A, Piran Hamlabadi M. The effect of knee orthosis on co-contraction values of knee and ankle muscles during running in people with knee deformity in the frontal plane. Journal of Rehabilitation Research in Nursing. 2022; 8(4):76-87. [Link]
- Besomi M, Hodges PW, Clancy EA, Van Dieën J, Hug F, Lowery M, et al. Consensus for experimental design in electromyography (CEDE) project: Amplitude normalization matrix. Journal of Electromyography and Kinesiology. 2020; 53:102438. [DOI:10.1016/j.jelekin.2020.102438] [PMID]
- Farahpour N, Jafarnezhad A, Damavandi M, Bakhtiari A, Allard P. Gait ground reaction force characteristics of low back pain patients with pronated foot and able-bodied individuals with and without foot pronation. Journal of Biomechanics. 2016; 49(9):1705-10. [DOI:10.1016/j.jbiomech.2016.03.056] [PMID]
- Farahpour N, Jafarnezhadgero A, Allard P, Majlesi M. Muscle activity and kinetics of lower limbs during walking in pronated feet individuals with and without low back pain. Journal of Electromyography and Kinesiology. 2018; 39:35-41. [DOI:10.1016/j.jelekin.2018.01.006] [PMID]
- Sharma J, Heagerty R, Dalal S, Banerjee B, Booker T. Risk factors associated with musculoskeletal injury: A prospective study of british infantry recruits. Current Rheumatology Reviews. 2019; 15(1):50-8. [DOI:10.2174/1573397114666180430103855] [PMID]
- Hamlabadi MP, Jafarnezhadgero A, Anoushirvani S. [The effect of two types of thoracolumbosacral braces on electromyography activity and pain index in patients with low back pain during walking (Persian)]. Anesthesiology and Pain. 12(1):1-10. [Link]
- Hunt AE, Smith RM, Torode M. Extrinsic muscle activity, foot motion and ankle joint moments during the stance phase of walking. Foot & Ankle International. 2001; 22(1):31-41. [DOI:10.1177/107110070102200105] [PMID]
- Elliott BC, Blanksby BA. The synchronization of muscle activity and body segment movements during a running cycle. Medicine and Science in Sports. 1979; 11(4):322-7. [DOI:10.1249/00005768-197901140-00002] [PMID]
Type of Study: Research |
Subject:
General
Received: 2023/11/18 | Accepted: 2024/06/5 | Published: 2024/01/13
Received: 2023/11/18 | Accepted: 2024/06/5 | Published: 2024/01/13
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
