Wed, Jun 26, 2024
Volume 14, Issue 2 (Spring 2024)
PTJ 2024, 14(2): 115-124 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Hadadnezhad M, Letafatkar A, Moradi M, Shah Saheb M S, Norouzi G, Salehi S. The Relationship Between Upper Extremity Functional Tests Scores With Strength, Proprioception, and Posture in Male Volleyball Players. PTJ 2024; 14 (2) :115-124
URL: http://ptj.uswr.ac.ir/article-1-606-en.html
URL: http://ptj.uswr.ac.ir/article-1-606-en.html
Malihe Hadadnezhad1 

 , Amir Letafatkar1 , Mohsen Moradi * 1, Maryam Sadat Shah Saheb2 , Gholamreza Norouzi3 , Shahin Salehi4
, Amir Letafatkar1 , Mohsen Moradi * 1, Maryam Sadat Shah Saheb2 , Gholamreza Norouzi3 , Shahin Salehi4
, Amir Letafatkar1 , Mohsen Moradi * 1, Maryam Sadat Shah Saheb2 , Gholamreza Norouzi3 , Shahin Salehi4
1- Department of Biomechanics and Sports Injury, Faculty of Physical Education and Sports Sciences, Kharazmi University, Tehran, Iran.
2- Department of Sports Medicine and Health, Faculty of Physical Education and Sports Sciences, University of Tehran, Tehran, Iran.
3- Department of Sports Injury and Physiology, Faculty of Physical Education and Sports Sciences, University of Arak, Arak, Iran.
4- Department of Sports Medicine, Faculty of Medicine, Imam Hussein Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
2- Department of Sports Medicine and Health, Faculty of Physical Education and Sports Sciences, University of Tehran, Tehran, Iran.
3- Department of Sports Injury and Physiology, Faculty of Physical Education and Sports Sciences, University of Arak, Arak, Iran.
4- Department of Sports Medicine, Faculty of Medicine, Imam Hussein Hospital, Shahid Beheshti University of Medical Sciences, Tehran, Iran.
Full-Text [PDF 728 kb]
(77 Downloads)
| Abstract (HTML) (532 Views)
Full-Text: (71 Views)
Introduction
Volleyball is considered one of the most popular sports disciplines today with approximately 200 million players worldwide, according to statistics provided by the World Volleyball Federation (FIVB) [1]. Although volleyball is considered a low-risk sport, athletes who participate in this sport are still at risk of various injuries [1].
Many of the skills performed in this sport, such as spiking, serving, and blocking, require continuous contact of the athlete’s upper limbs with the ball in an overhead position. Of these skills, spiking and serving are perhaps the most important skills in volleyball [2]. Repetitive strikes induce compounded pressure on the shoulder girdle of the athlete. The shoulder function of volleyball players depends on the accurate, coordinated, and correct functioning of the rotator cuff muscles and shoulder stabilizers. Regrettably, during repetitive movements in volleyball, musculoskeletal structures may be subjected to excessive loads, leading to acute shoulder injuries or injuries arising from overuse [2]. In the absence of proper treatment and rehabilitation for shoulder injuries resulting from overuse, it is plausible that these injuries may progress over time, leading to functional impairment in the shoulders of volleyball athletes. The incidence of shoulder injuries in volleyball athletes is higher compared to many other sports disciplines. Chandran et al. (2021) reported that the prevalence of shoulder injuries in volleyball players was higher compared to other sports, and stated that shoulder pain was the most common complaint of volleyball players [3].
Spiking or serving in volleyball, at the moment of hitting the ball with the hand, requires control, power, and flexibility, and in other words, maintaining stability during high mobility in the shoulder area [4]. In a manner such that, due to the external forces exerted by the ball onto the body, this mobility and stability must be facilitated within the kinetic chain [4].
Studies have also concluded that proprioception, flexibility, and range of motion are the most important risk factors for shoulder injuries. These factors are especially important in overhead athletes, as they have significantly looser joint capsules and excessive range of motion [5]. In this regard, Zarei et al. (2021) investigated the effect of injury prevention exercises on proprioception and dynamic stability of the shoulder joint of volleyball athletes and concluded that these exercises can improve the proprioception of the athletes’ shoulder [4].
Studies have shown that any change in the alignment of the spine, such as kyphosis, lordosis, scoliosis, and head forward posture, can lead to poor posture and imbalance. If these factors are identified through functional tests before participating in competitions, sports medicine specialists can intervene by designing and implementing targeted prevention strategies to reduce the risk of injury.
Functional tests are now used in pre-season athlete assessments to identify performance deficiencies with the goal of injury prevention. Among the few tests designed to assess upper extremity function, the upper quarter Y-balance test is one of the most appropriate tests that assess the individual’s upper extremity function in a closed kinetic chain [8].
The use of screening and pre-season athlete assessment methods reduces the likelihood of recurrent injuries. The use of an effective upper extremity functional assessment method can be useful in planning preventive or rehabilitation exercises for these injuries. However, there is currently limited evidence on upper extremity functional assessment methods [9].
Given the importance of strength, proprioception, posture, and flexibility in volleyball athletes, the review of most studies on the effects of various exercises on these variables and the upper extremity function of athletes, and the lack of studies that have examined the relationship between the scores of upper extremity functional tests with the variables of strength, range of motion, shoulder proprioception, and posture of male volleyball players, therefore, the present study investigates whether there is a relationship between the scores of upper extremity functional tests with isometric strength, range of motion, shoulder proprioception, and posture of male volleyball players.
Materials and Methods
The present study, methodologically, is characterized as a correlational investigation. The statistical population of the present study was male university volleyball players, of whom 50 participants were selected using the G*Power software, version 3.1.9.7 on a convenience basis according to the inclusion and exclusion criteria of the research. The inclusion criteria for the study comprised male volleyball players between the ages of 18 and 24 who had participated in volleyball for an average of three sessions per week for at least 1.5 h per session in the past year [10], and had a normal body mass index (18-25) [10]. The exclusion criteria for the study were having any history of fracture or surgery to the shoulder joint [4], having a history of neurological and musculoskeletal diseases that limit movement [11], having any pain in the upper extremity before or during the tests, and having a history of shoulder dislocation or subluxation [4].
The necessary explanations were given about the stages of the research, and the consent form for voluntary and informed participation in the research was signed by the research participants. To measure the necessary, the research participants were asked to attend the test site according to the specified schedule. After the attendance of the participants, the measurements related to the research variables were taken.
To assess power and proprioception, an isokinetic device was used. After 5 min of warm-up with the dynamometer, the concentric strength of internal and external rotators and muscles of abductors, flexors, adductors, and extensors was measured at speeds of 180 and 300 degrees. The power assessment was performed only on the dominant shoulder of the participants. When performing the test, the participant sat on the seat of the device and the attachment was installed according to the device instructions and adjusted to the length of each participant’s arm so that the glenohumeral joint was in neutral rotational position. The device settings included the following items: 5 degrees of rotation of the dynamometer, 45 degrees of tilt of the dynamometer, 35 degrees of rotation of the seat of the device, and 85 degrees of the backrest of the seat to be in this position. The participants were seated on the seat of the device. The hips and torso of the participants were fixed by a strap (belt) to prevent the substitution of large muscles. The shoulder was in abduction of 90 degrees, the elbow in flexion of 90 degrees, and the range of motion of the device was between 90 degrees of external rotation and 60 degrees of internal rotation [12]. During the test, the participants were verbally encouraged and the rest time between each test was 60 s [13].
To assess the proprioception of the shoulder, an isokinetic device was also used. For this purpose, the device was first introduced to the participants and the test method was taught. To perform the angle reconstruction test, the participants were seated on the isokinetic dynamometer with their eyes closed. The straps were tied to the participant’s chest to prevent excessive trunk movements. The speed of the dynamometer was set at 5 degrees/s and the dominant shoulder was placed in the scapular plane. The horizontal position of the dynamometer’s lever arm was defined as the angle and the range of motion relative to it was 90 degrees. The angles that the participant had to reconstruct included 45 and 90 degrees, which were reconstructed in the direction of the internal rotation range. The starting position for the 90-degree angle was 45 degrees, and for the reconstruction of the 45-degree angle, 90 degrees. The participant’s shoulder was actively brought to each of the 3 target angles and held for 10 s. The participant was asked to focus on this angle, then the arm was actively returned to the starting position and the participant rested for 5 s. This action was repeated twice and for the third time, the individual was asked to actively rotate the arm until the target angle was reached. When the participants felt that they had reached the target angle, they stopped the lever arm. This action was repeated three times and the absolute difference between the recorded angle and the target angle was recorded as the error (absolute angular error) and the mean of them was used for statistical analysis [14].
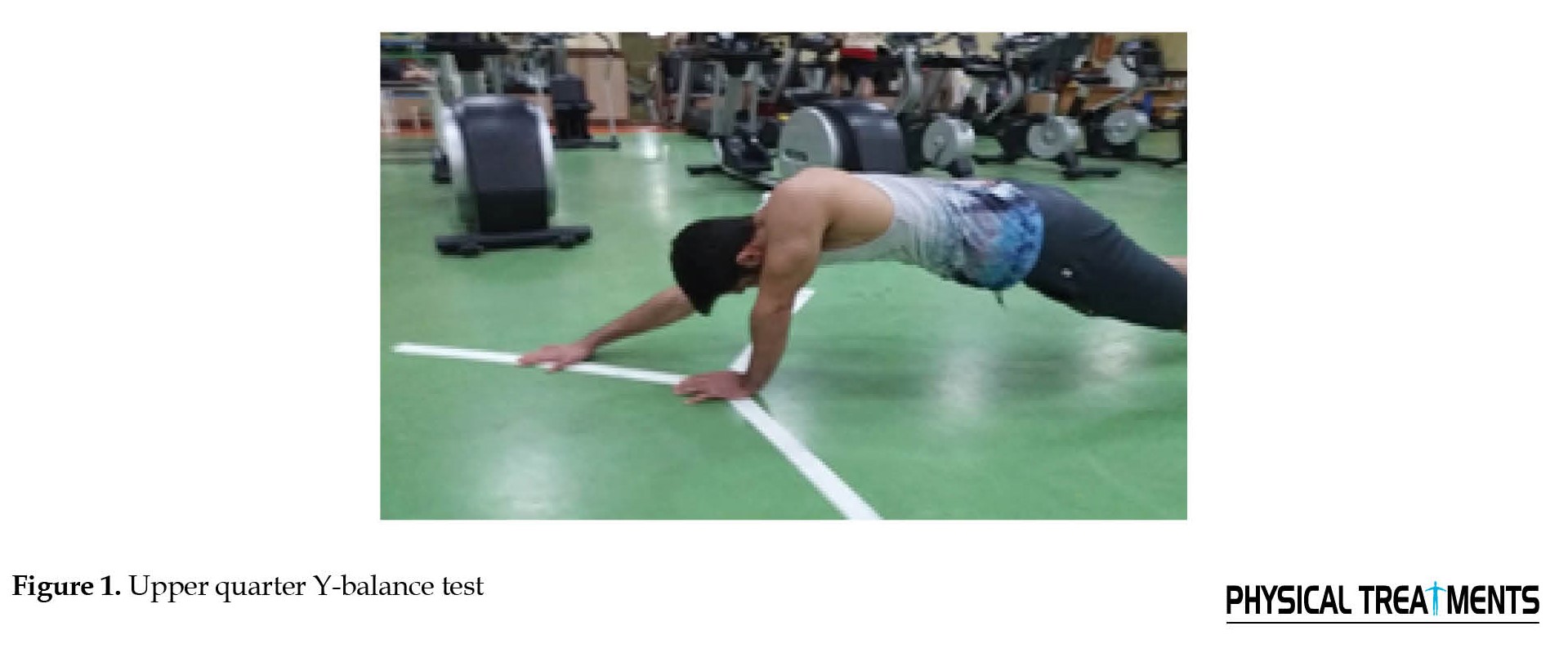
To assess the upper extremity function, the upper quarter Y-balance test was used and white paper labels similar to the Y-balance device were glued to the ground. Gorman et al. (2012) reported the validity of the upper quarter Y-balance test upper extremity function test in intra-rater correlation coefficient (ICC=0.99-0.80) and inter-rater correlation coefficient (ICC=0.90) [15].
These three labels were connected in such a way that they had an angle of 120 degrees relative to each other and were located in three directions, internal, lower external, and upper external. Each label was marked in cm so that when the test was performed, the examiner immediately recorded the amount of reach by the participant’s hand touching the label. As such, the participants should first place their non-dominant hand in the center of the connection of the three labels and assume a push-up position, then move their dominant hand to the maximum reach distance in the internal direction, immediately in the lower external direction, and then in the upper external direction, and finally returned to the initial test position [5]. The reach distance was divided by the length of the upper extremity in centimeters and multiplied by 100 to be calculated as a percentage of the length of the upper extremity (Figure 1).
 To measure the angles of the forward head and shoulder forward, the first three anatomical landmarks were identified, including the earlobe, the right acromion prominence, and the spinous process of the seventh vertebra (Figure 2).
To measure the angles of the forward head and shoulder forward, the first three anatomical landmarks were identified, including the earlobe, the right acromion prominence, and the spinous process of the seventh vertebra (Figure 2).
 Using a landmark, these landmarks were marked. Then, the participant was instructed to stand at the designated location next to the wall at a distance of 23 cm in such a way that the left arm was toward the wall. Then, a photographic tripod with a digital camera mounted on it was placed at a distance of 2.65 m from the wall, and its height was adjusted at the level of the participant’s right shoulder. The participants were asked to bend forward three times in the same position and also raise their hands above their heads three times, and then stand comfortably and naturally and look at an imaginary point on the opposite wall (eyes in line with the horizon). The examiner took a photo of the body in profile after 5 s of stopping. Finally, the desired photo was transferred to the computer, and using AutoCAD software, the angle of the line connecting the tragus and the seventh cervical vertebra with the vertical line (forward head angle) and the angle of the line connecting the same vertebra and the acromion process with the vertical line (forward shoulder angle) was measured [16].
Using a landmark, these landmarks were marked. Then, the participant was instructed to stand at the designated location next to the wall at a distance of 23 cm in such a way that the left arm was toward the wall. Then, a photographic tripod with a digital camera mounted on it was placed at a distance of 2.65 m from the wall, and its height was adjusted at the level of the participant’s right shoulder. The participants were asked to bend forward three times in the same position and also raise their hands above their heads three times, and then stand comfortably and naturally and look at an imaginary point on the opposite wall (eyes in line with the horizon). The examiner took a photo of the body in profile after 5 s of stopping. Finally, the desired photo was transferred to the computer, and using AutoCAD software, the angle of the line connecting the tragus and the seventh cervical vertebra with the vertical line (forward head angle) and the angle of the line connecting the same vertebra and the acromion process with the vertical line (forward shoulder angle) was measured [16].
The range of motion of flexion, extension, abduction, and internal and external rotation at 90 degrees of abduction was measured using a Robinson 3 goniometer from Australia. To do this, the subject lay on the bed in a supine position with their legs bent at the knee and their feet flat on the ground. To measure the range of motion using a goniometer, the universal axis of motion was marked on the prominence of the humerus head, and the axis of the goniometer was placed on it. The fixed arm was placed parallel to the participant’s body, and the movable arm was placed in the middle of the midline of the arm at the end of the movement, and the number read was recorded [17].
To measure the range of motion of shoulder extension, the participant lay prone on the bed with their palm facing the body and rotated their head to the opposite side. The center of the goniometer was placed on the humerus head, on the outside of the shoulder, and the fixed arm of the goniometer was parallel to the body surface. The movable arm was placed when the participant raised their arm and the midline of the arm was in line with the midline of the movable arm of the goniometer. The range of motion was recorded [17].
To measure the range of motion of shoulder abduction, the participant lay supine with the evaluator standing above the participant’s head. The participant’s palm faced up, and care was taken to ensure that the hand did not move up or down during the movement. The acromion was marked as the center of the goniometer, and the fixed arm was parallel to the sternum. The movable arm was placed between the participant’s arm, and the number was read [17].
To measure the range of motion of shoulder internal rotation, the participant lay supine with the arm abducted 90 degrees and the elbow flexed 90 degrees. A roll was also placed under the arm to separate it and allow for easy movement. The center of the goniometer was fixed on the olecranon, the fixed arm was perpendicular to the ground, and the movable arm was aligned with the midline of the forearm. The participant was asked to bring the hand down, and the number was recorded [17].
To measure the range of motion of shoulder external rotation, the participant lay supine with the arm abducted 90 degrees and the elbow flexed 90 degrees. A roll was also placed under the arm to facilitate movement. The center of the goniometer was placed on the olecranon, the fixed arm was perpendicular to the ground, and the movable arm was aligned with the midline of the forearm. The participant was asked to move the hand backward, and the number was recorded [17].
To assess the normality of the data, the Shapiro-Wilk statistical test was used. Given the normality of the data, the Pearson correlation coefficient test was used to assess the correlation between the variables. All statistical analyses were performed at the significance level of 0.05 and using SPSS software, version 20.
Results
The demographic characteristics of the participants are provided in Table 1.

There was no significant difference in the variables of age, height, weight, and body mass index between the groups.
Based on the normality of the data, the Pearson correlation coefficient was used to assess the correlation between functional tests with isokinetic strength, proprioception, shoulder range of motion, and posture of volleyball players. Descriptive statistical results are reported in Table 2.
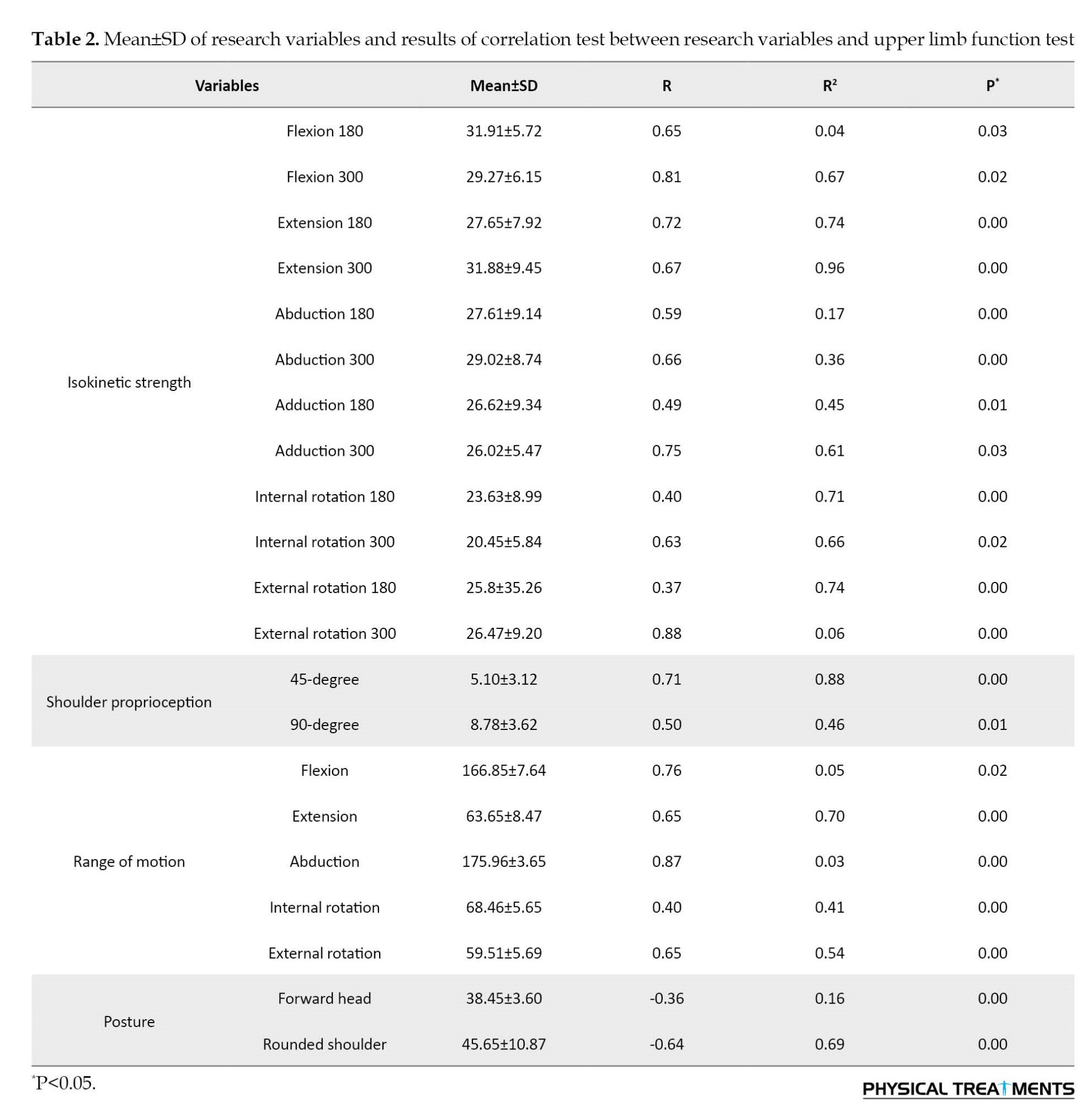
The Pearson correlation coefficient test results showed a significant correlation between the strength of the upper limb muscles in all directions and speeds with the upper limb functional test (P<0.05). Accordingly, with increasing muscle strength, performance also increased. The results also showed a significant correlation between shoulder proprioception at angles of 45 and 90 degrees and between the range of motion of the shoulder joint in all directions, with upper limb function (P<0.05).
A significant negative correlation was also observed between the results of the forward head and rounded shoulder tests and the results of the upper limb functional test (P<0.05). Accordingly, as the forward head and rounded shoulder angles increased, upper limb function decreased and vice versa.
Discussion
The current research investigated the relationship between scores of upper extremity functional tests with isokinetic strength, range of motion, proprioception, and posture in male volleyball players. The results revealed a significant and positive correlation between strength variables in all movements, proprioception at 45 and 90-degree angles, range of motion, and upper extremity performance. Additionally, a significant negative correlation was observed between the variables of forward head angle, forward shoulder angle, and upper extremity performance. These findings are in line with the studies conducted by Oliver et al. (2018) [18], Bauer et al. (2020) [9], and Walaszek et al. (2018) [19], while contradicting the results of Borms et al. (2016) [20]. However, limited research has been conducted on the subject following the findings of the present study.
The upper limb functional test is performed in a closed kinetic chain, while the isokinetic device measures the strength of the subjects in an open kinetic chain. This issue was one of the reasons that Borms et al. mentioned for the lack of a significant relationship between strength and performance in overhead athletes [20].
Past studies have reported that performing the upper quarter Y-balance test upper limb functional test requires strength, flexibility, neuromuscular control, core stability, balance, and proprioception, and is, therefore, a suitable test for preseason assessments and medical assessments [21].
The results showed a significant negative correlation between upper limb function and the degree of forward head and forward shoulder (P=0.001). There are different muscles with different functions in the shoulder girdle area, which are divided into two groups movers and stabilizers. The movers’ group in this area includes the pectoralis major, upper trapezius, levator scapulae, and anterior deltoid muscles. The stabilizers group of this area also includes the rhomboids, anterior serratus, posterior deltoid, supraspinatus, and infraspinatus muscles. In athletes who have hand movements above and in front of the body, such as volleyball players, the movers’ group of muscles is prone to shortening and the stabilizers group of muscles is prone to weakness and stretching [22]. The reason for this can be attributed to the repeated concentric contractions of the internal rotator muscles and eccentric contractions of the posterior shoulder muscles to prevent the increase in arm acceleration [23]during repetitive overhead hand movements in volleyball players in front of the body for a long time, which is a factor for shortening of the anterior muscles and stretching in the muscles of the posterior shoulder area and provides the basis for movement of the shoulders forward and bringing them closer together. This shortening in the muscles of the anterior shoulder area can also be a factor in reducing the range of motion of the external rotation of the shoulder. The results of various studies on the effects of different training programs that included strengthening the posterior shoulder muscles and stretching the anterior shoulder muscles can confirm this issue [24]. Performing natural joint movements requires a high degree of coordination between the two opposing muscle groups that control the joint movements. Coordination between the two opposing muscle groups in any pair of antagonist muscles depends on the functional balance between these muscle groups in terms of strength. If one muscle group is trained more than the other group (such as when performing a strength training program in which the external rotator muscles of the shoulder joint are forgotten and not trained compared to the internal rotator muscles, or when they are exposed to a much greater relative pressure than other muscles during exercise (such as repeated hand strikes in volleyball players), in this case, an imbalance of power between the two muscle groups may occur [25], which has been noted by various researchers in connection with sports [26].
A significant relationship was also found between the range of motion of the shoulder joint in all directions and upper limb function. Pour Rahim et al. (2021) in their study investigated the relationship between the range of motion of joints and the performance of 50-, 100-, and 200-m breaststroke swimmers. Their results showed that there is a significant relationship between the range of motion of joints and the time of 50-, 100-, and 200-m breaststroke swimming [27]. The results of the study showed a positive and significant relationship between the strength of the upper limb muscles in all movements and upper limb function (P<0.05). The results of the study also showed a positive and significant relationship between the shoulder joint proprioception at two angles of 45 degrees and 90 degrees and upper limb function (P<0.05). Since part of volleyball players’ training includes strength training exercises for the upper limb muscles, including power and plyometric movements, these exercises probably increase the strength of the muscles around the shoulder joint through neural adaptations, which increase the strength of the agonist muscle and reduce the activity of the antagonist muscle, which is the first mechanism for increasing strength at the beginning of training. This leads to subsequent improvement in performance. The strength of the muscles surrounding the joint and their simultaneous contraction to stabilize the joints of the upper limb, along with the activity of the deep receptors and neuromuscular control to maintain balance when reaching in three specific directions and achieving the greatest distance, is of particular importance.
Since many researchers have mentioned the upper limb functional test as a suitable test for assessing upper limb balance [5, 17, 20], factors that increase upper limb balance can improve the scores of this test and increase upper limb function as well. The theory that underlies the work of researchers in the study of movement and balance is the systems theory. According to the systems theory, the ability to maintain posture in space is due to the interactive, simultaneous, and complex effect of three neuromuscular and skeletal systems, which is called the posture control system [28]. Posture control requires the integration of four sensory inputs to determine the position of the body in space, as well as the ability of the musculoskeletal system to apply the appropriate force. According to this theory, the musculoskeletal factors that affect balance regulation include muscle properties and characteristics, joint range of motion, proprioception, and the biomechanical relationship of different parts of the body [28]. Previous studies have also shown a coordinated relationship between strength and proprioception with balance and performance. Therefore, with increasing strength and proprioception, the performance of the subjects can also increase. For this reason, one of the possible reasons for the significant positive correlation between strength and proprioception with upper limb function can be found in the same subject that volleyball players in the present study have strength and balance exercises in their weekly and monthly training program. As a result, their performance has probably increased.
Concerning the relationship between upper limb function and shoulder joint proprioception, studies have reported that increasing muscle strength facilitates and synchronizes fast-twitch and large motor units [29], stimulates muscle spindles, reduces the inhibitory effect of Golgi tendon organs, and also increases coordination of muscles involved in simultaneous activities.
With the stimulation of muscle spindles, muscle contraction causes an increase in the activity of gamma motor neurons present in the spindles, and this increase in sensitivity in the spindles improves joint position sense, which has a great effect on joint control [30].
Conclusion
Based on the findings of the present study, there is a significant positive correlation between upper limb function and isokinetic muscle strength, range of motion, and shoulder joint proprioception, and a significant negative correlation between forward head posture and forward shoulder posture in volleyball athletes. Therefore, it is suggested that coaches and specialists design the necessary exercises to improve shoulder joint strength, range of motion, and proprioception, and consequently correct forward head posture and forward shoulder posture in volleyball athletes.
Study limitations
One of the limitations of the present study is the issue of the effect of fatigue caused by the daily training of the subjects, as well as the lack of control of the psychological, nutritional, and sleep issues of the subjects in the measurement process of the variables.
Ethical Considerations
Compliance with ethical guidelines
This article is the result of a research project entitled “the relationship between upper limb functional tests scores with isokinetic strength, range of motion, shoulder proprioception, and posture of male volleyball players” that was approved by Sport Sciences Research Institute (Code: IR.SSRI.REC.1400.1043).
Funding
This study was approved by the Medical Sports Federation of the Islamic Republic of Iran in 2019 (Code 3430/248), which was implemented with the support of the relevant federation.
Authors' contributions
All authors contributed equally to preparing this article.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors extend their heartfelt thanks and appreciation to all coaches and athletes who assisted them in the execution of this research project. Your valuable support and collaboration have been indispensable to the success of this endeavor.
References
Volleyball is considered one of the most popular sports disciplines today with approximately 200 million players worldwide, according to statistics provided by the World Volleyball Federation (FIVB) [1]. Although volleyball is considered a low-risk sport, athletes who participate in this sport are still at risk of various injuries [1].
Many of the skills performed in this sport, such as spiking, serving, and blocking, require continuous contact of the athlete’s upper limbs with the ball in an overhead position. Of these skills, spiking and serving are perhaps the most important skills in volleyball [2]. Repetitive strikes induce compounded pressure on the shoulder girdle of the athlete. The shoulder function of volleyball players depends on the accurate, coordinated, and correct functioning of the rotator cuff muscles and shoulder stabilizers. Regrettably, during repetitive movements in volleyball, musculoskeletal structures may be subjected to excessive loads, leading to acute shoulder injuries or injuries arising from overuse [2]. In the absence of proper treatment and rehabilitation for shoulder injuries resulting from overuse, it is plausible that these injuries may progress over time, leading to functional impairment in the shoulders of volleyball athletes. The incidence of shoulder injuries in volleyball athletes is higher compared to many other sports disciplines. Chandran et al. (2021) reported that the prevalence of shoulder injuries in volleyball players was higher compared to other sports, and stated that shoulder pain was the most common complaint of volleyball players [3].
Spiking or serving in volleyball, at the moment of hitting the ball with the hand, requires control, power, and flexibility, and in other words, maintaining stability during high mobility in the shoulder area [4]. In a manner such that, due to the external forces exerted by the ball onto the body, this mobility and stability must be facilitated within the kinetic chain [4].
Studies have also concluded that proprioception, flexibility, and range of motion are the most important risk factors for shoulder injuries. These factors are especially important in overhead athletes, as they have significantly looser joint capsules and excessive range of motion [5]. In this regard, Zarei et al. (2021) investigated the effect of injury prevention exercises on proprioception and dynamic stability of the shoulder joint of volleyball athletes and concluded that these exercises can improve the proprioception of the athletes’ shoulder [4].
Studies have shown that any change in the alignment of the spine, such as kyphosis, lordosis, scoliosis, and head forward posture, can lead to poor posture and imbalance. If these factors are identified through functional tests before participating in competitions, sports medicine specialists can intervene by designing and implementing targeted prevention strategies to reduce the risk of injury.
Functional tests are now used in pre-season athlete assessments to identify performance deficiencies with the goal of injury prevention. Among the few tests designed to assess upper extremity function, the upper quarter Y-balance test is one of the most appropriate tests that assess the individual’s upper extremity function in a closed kinetic chain [8].
The use of screening and pre-season athlete assessment methods reduces the likelihood of recurrent injuries. The use of an effective upper extremity functional assessment method can be useful in planning preventive or rehabilitation exercises for these injuries. However, there is currently limited evidence on upper extremity functional assessment methods [9].
Given the importance of strength, proprioception, posture, and flexibility in volleyball athletes, the review of most studies on the effects of various exercises on these variables and the upper extremity function of athletes, and the lack of studies that have examined the relationship between the scores of upper extremity functional tests with the variables of strength, range of motion, shoulder proprioception, and posture of male volleyball players, therefore, the present study investigates whether there is a relationship between the scores of upper extremity functional tests with isometric strength, range of motion, shoulder proprioception, and posture of male volleyball players.
Materials and Methods
The present study, methodologically, is characterized as a correlational investigation. The statistical population of the present study was male university volleyball players, of whom 50 participants were selected using the G*Power software, version 3.1.9.7 on a convenience basis according to the inclusion and exclusion criteria of the research. The inclusion criteria for the study comprised male volleyball players between the ages of 18 and 24 who had participated in volleyball for an average of three sessions per week for at least 1.5 h per session in the past year [10], and had a normal body mass index (18-25) [10]. The exclusion criteria for the study were having any history of fracture or surgery to the shoulder joint [4], having a history of neurological and musculoskeletal diseases that limit movement [11], having any pain in the upper extremity before or during the tests, and having a history of shoulder dislocation or subluxation [4].
The necessary explanations were given about the stages of the research, and the consent form for voluntary and informed participation in the research was signed by the research participants. To measure the necessary, the research participants were asked to attend the test site according to the specified schedule. After the attendance of the participants, the measurements related to the research variables were taken.
To assess power and proprioception, an isokinetic device was used. After 5 min of warm-up with the dynamometer, the concentric strength of internal and external rotators and muscles of abductors, flexors, adductors, and extensors was measured at speeds of 180 and 300 degrees. The power assessment was performed only on the dominant shoulder of the participants. When performing the test, the participant sat on the seat of the device and the attachment was installed according to the device instructions and adjusted to the length of each participant’s arm so that the glenohumeral joint was in neutral rotational position. The device settings included the following items: 5 degrees of rotation of the dynamometer, 45 degrees of tilt of the dynamometer, 35 degrees of rotation of the seat of the device, and 85 degrees of the backrest of the seat to be in this position. The participants were seated on the seat of the device. The hips and torso of the participants were fixed by a strap (belt) to prevent the substitution of large muscles. The shoulder was in abduction of 90 degrees, the elbow in flexion of 90 degrees, and the range of motion of the device was between 90 degrees of external rotation and 60 degrees of internal rotation [12]. During the test, the participants were verbally encouraged and the rest time between each test was 60 s [13].
To assess the proprioception of the shoulder, an isokinetic device was also used. For this purpose, the device was first introduced to the participants and the test method was taught. To perform the angle reconstruction test, the participants were seated on the isokinetic dynamometer with their eyes closed. The straps were tied to the participant’s chest to prevent excessive trunk movements. The speed of the dynamometer was set at 5 degrees/s and the dominant shoulder was placed in the scapular plane. The horizontal position of the dynamometer’s lever arm was defined as the angle and the range of motion relative to it was 90 degrees. The angles that the participant had to reconstruct included 45 and 90 degrees, which were reconstructed in the direction of the internal rotation range. The starting position for the 90-degree angle was 45 degrees, and for the reconstruction of the 45-degree angle, 90 degrees. The participant’s shoulder was actively brought to each of the 3 target angles and held for 10 s. The participant was asked to focus on this angle, then the arm was actively returned to the starting position and the participant rested for 5 s. This action was repeated twice and for the third time, the individual was asked to actively rotate the arm until the target angle was reached. When the participants felt that they had reached the target angle, they stopped the lever arm. This action was repeated three times and the absolute difference between the recorded angle and the target angle was recorded as the error (absolute angular error) and the mean of them was used for statistical analysis [14].
To assess the upper extremity function, the upper quarter Y-balance test was used and white paper labels similar to the Y-balance device were glued to the ground. Gorman et al. (2012) reported the validity of the upper quarter Y-balance test upper extremity function test in intra-rater correlation coefficient (ICC=0.99-0.80) and inter-rater correlation coefficient (ICC=0.90) [15].
These three labels were connected in such a way that they had an angle of 120 degrees relative to each other and were located in three directions, internal, lower external, and upper external. Each label was marked in cm so that when the test was performed, the examiner immediately recorded the amount of reach by the participant’s hand touching the label. As such, the participants should first place their non-dominant hand in the center of the connection of the three labels and assume a push-up position, then move their dominant hand to the maximum reach distance in the internal direction, immediately in the lower external direction, and then in the upper external direction, and finally returned to the initial test position [5]. The reach distance was divided by the length of the upper extremity in centimeters and multiplied by 100 to be calculated as a percentage of the length of the upper extremity (Figure 1).
The range of motion of flexion, extension, abduction, and internal and external rotation at 90 degrees of abduction was measured using a Robinson 3 goniometer from Australia. To do this, the subject lay on the bed in a supine position with their legs bent at the knee and their feet flat on the ground. To measure the range of motion using a goniometer, the universal axis of motion was marked on the prominence of the humerus head, and the axis of the goniometer was placed on it. The fixed arm was placed parallel to the participant’s body, and the movable arm was placed in the middle of the midline of the arm at the end of the movement, and the number read was recorded [17].
To measure the range of motion of shoulder extension, the participant lay prone on the bed with their palm facing the body and rotated their head to the opposite side. The center of the goniometer was placed on the humerus head, on the outside of the shoulder, and the fixed arm of the goniometer was parallel to the body surface. The movable arm was placed when the participant raised their arm and the midline of the arm was in line with the midline of the movable arm of the goniometer. The range of motion was recorded [17].
To measure the range of motion of shoulder abduction, the participant lay supine with the evaluator standing above the participant’s head. The participant’s palm faced up, and care was taken to ensure that the hand did not move up or down during the movement. The acromion was marked as the center of the goniometer, and the fixed arm was parallel to the sternum. The movable arm was placed between the participant’s arm, and the number was read [17].
To measure the range of motion of shoulder internal rotation, the participant lay supine with the arm abducted 90 degrees and the elbow flexed 90 degrees. A roll was also placed under the arm to separate it and allow for easy movement. The center of the goniometer was fixed on the olecranon, the fixed arm was perpendicular to the ground, and the movable arm was aligned with the midline of the forearm. The participant was asked to bring the hand down, and the number was recorded [17].
To measure the range of motion of shoulder external rotation, the participant lay supine with the arm abducted 90 degrees and the elbow flexed 90 degrees. A roll was also placed under the arm to facilitate movement. The center of the goniometer was placed on the olecranon, the fixed arm was perpendicular to the ground, and the movable arm was aligned with the midline of the forearm. The participant was asked to move the hand backward, and the number was recorded [17].
To assess the normality of the data, the Shapiro-Wilk statistical test was used. Given the normality of the data, the Pearson correlation coefficient test was used to assess the correlation between the variables. All statistical analyses were performed at the significance level of 0.05 and using SPSS software, version 20.
Results
The demographic characteristics of the participants are provided in Table 1.
There was no significant difference in the variables of age, height, weight, and body mass index between the groups.
Based on the normality of the data, the Pearson correlation coefficient was used to assess the correlation between functional tests with isokinetic strength, proprioception, shoulder range of motion, and posture of volleyball players. Descriptive statistical results are reported in Table 2.
The Pearson correlation coefficient test results showed a significant correlation between the strength of the upper limb muscles in all directions and speeds with the upper limb functional test (P<0.05). Accordingly, with increasing muscle strength, performance also increased. The results also showed a significant correlation between shoulder proprioception at angles of 45 and 90 degrees and between the range of motion of the shoulder joint in all directions, with upper limb function (P<0.05).
A significant negative correlation was also observed between the results of the forward head and rounded shoulder tests and the results of the upper limb functional test (P<0.05). Accordingly, as the forward head and rounded shoulder angles increased, upper limb function decreased and vice versa.
Discussion
The current research investigated the relationship between scores of upper extremity functional tests with isokinetic strength, range of motion, proprioception, and posture in male volleyball players. The results revealed a significant and positive correlation between strength variables in all movements, proprioception at 45 and 90-degree angles, range of motion, and upper extremity performance. Additionally, a significant negative correlation was observed between the variables of forward head angle, forward shoulder angle, and upper extremity performance. These findings are in line with the studies conducted by Oliver et al. (2018) [18], Bauer et al. (2020) [9], and Walaszek et al. (2018) [19], while contradicting the results of Borms et al. (2016) [20]. However, limited research has been conducted on the subject following the findings of the present study.
The upper limb functional test is performed in a closed kinetic chain, while the isokinetic device measures the strength of the subjects in an open kinetic chain. This issue was one of the reasons that Borms et al. mentioned for the lack of a significant relationship between strength and performance in overhead athletes [20].
Past studies have reported that performing the upper quarter Y-balance test upper limb functional test requires strength, flexibility, neuromuscular control, core stability, balance, and proprioception, and is, therefore, a suitable test for preseason assessments and medical assessments [21].
The results showed a significant negative correlation between upper limb function and the degree of forward head and forward shoulder (P=0.001). There are different muscles with different functions in the shoulder girdle area, which are divided into two groups movers and stabilizers. The movers’ group in this area includes the pectoralis major, upper trapezius, levator scapulae, and anterior deltoid muscles. The stabilizers group of this area also includes the rhomboids, anterior serratus, posterior deltoid, supraspinatus, and infraspinatus muscles. In athletes who have hand movements above and in front of the body, such as volleyball players, the movers’ group of muscles is prone to shortening and the stabilizers group of muscles is prone to weakness and stretching [22]. The reason for this can be attributed to the repeated concentric contractions of the internal rotator muscles and eccentric contractions of the posterior shoulder muscles to prevent the increase in arm acceleration [23]during repetitive overhead hand movements in volleyball players in front of the body for a long time, which is a factor for shortening of the anterior muscles and stretching in the muscles of the posterior shoulder area and provides the basis for movement of the shoulders forward and bringing them closer together. This shortening in the muscles of the anterior shoulder area can also be a factor in reducing the range of motion of the external rotation of the shoulder. The results of various studies on the effects of different training programs that included strengthening the posterior shoulder muscles and stretching the anterior shoulder muscles can confirm this issue [24]. Performing natural joint movements requires a high degree of coordination between the two opposing muscle groups that control the joint movements. Coordination between the two opposing muscle groups in any pair of antagonist muscles depends on the functional balance between these muscle groups in terms of strength. If one muscle group is trained more than the other group (such as when performing a strength training program in which the external rotator muscles of the shoulder joint are forgotten and not trained compared to the internal rotator muscles, or when they are exposed to a much greater relative pressure than other muscles during exercise (such as repeated hand strikes in volleyball players), in this case, an imbalance of power between the two muscle groups may occur [25], which has been noted by various researchers in connection with sports [26].
A significant relationship was also found between the range of motion of the shoulder joint in all directions and upper limb function. Pour Rahim et al. (2021) in their study investigated the relationship between the range of motion of joints and the performance of 50-, 100-, and 200-m breaststroke swimmers. Their results showed that there is a significant relationship between the range of motion of joints and the time of 50-, 100-, and 200-m breaststroke swimming [27]. The results of the study showed a positive and significant relationship between the strength of the upper limb muscles in all movements and upper limb function (P<0.05). The results of the study also showed a positive and significant relationship between the shoulder joint proprioception at two angles of 45 degrees and 90 degrees and upper limb function (P<0.05). Since part of volleyball players’ training includes strength training exercises for the upper limb muscles, including power and plyometric movements, these exercises probably increase the strength of the muscles around the shoulder joint through neural adaptations, which increase the strength of the agonist muscle and reduce the activity of the antagonist muscle, which is the first mechanism for increasing strength at the beginning of training. This leads to subsequent improvement in performance. The strength of the muscles surrounding the joint and their simultaneous contraction to stabilize the joints of the upper limb, along with the activity of the deep receptors and neuromuscular control to maintain balance when reaching in three specific directions and achieving the greatest distance, is of particular importance.
Since many researchers have mentioned the upper limb functional test as a suitable test for assessing upper limb balance [5, 17, 20], factors that increase upper limb balance can improve the scores of this test and increase upper limb function as well. The theory that underlies the work of researchers in the study of movement and balance is the systems theory. According to the systems theory, the ability to maintain posture in space is due to the interactive, simultaneous, and complex effect of three neuromuscular and skeletal systems, which is called the posture control system [28]. Posture control requires the integration of four sensory inputs to determine the position of the body in space, as well as the ability of the musculoskeletal system to apply the appropriate force. According to this theory, the musculoskeletal factors that affect balance regulation include muscle properties and characteristics, joint range of motion, proprioception, and the biomechanical relationship of different parts of the body [28]. Previous studies have also shown a coordinated relationship between strength and proprioception with balance and performance. Therefore, with increasing strength and proprioception, the performance of the subjects can also increase. For this reason, one of the possible reasons for the significant positive correlation between strength and proprioception with upper limb function can be found in the same subject that volleyball players in the present study have strength and balance exercises in their weekly and monthly training program. As a result, their performance has probably increased.
Concerning the relationship between upper limb function and shoulder joint proprioception, studies have reported that increasing muscle strength facilitates and synchronizes fast-twitch and large motor units [29], stimulates muscle spindles, reduces the inhibitory effect of Golgi tendon organs, and also increases coordination of muscles involved in simultaneous activities.
With the stimulation of muscle spindles, muscle contraction causes an increase in the activity of gamma motor neurons present in the spindles, and this increase in sensitivity in the spindles improves joint position sense, which has a great effect on joint control [30].
Conclusion
Based on the findings of the present study, there is a significant positive correlation between upper limb function and isokinetic muscle strength, range of motion, and shoulder joint proprioception, and a significant negative correlation between forward head posture and forward shoulder posture in volleyball athletes. Therefore, it is suggested that coaches and specialists design the necessary exercises to improve shoulder joint strength, range of motion, and proprioception, and consequently correct forward head posture and forward shoulder posture in volleyball athletes.
Study limitations
One of the limitations of the present study is the issue of the effect of fatigue caused by the daily training of the subjects, as well as the lack of control of the psychological, nutritional, and sleep issues of the subjects in the measurement process of the variables.
Ethical Considerations
Compliance with ethical guidelines
This article is the result of a research project entitled “the relationship between upper limb functional tests scores with isokinetic strength, range of motion, shoulder proprioception, and posture of male volleyball players” that was approved by Sport Sciences Research Institute (Code: IR.SSRI.REC.1400.1043).
Funding
This study was approved by the Medical Sports Federation of the Islamic Republic of Iran in 2019 (Code 3430/248), which was implemented with the support of the relevant federation.
Authors' contributions
All authors contributed equally to preparing this article.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors extend their heartfelt thanks and appreciation to all coaches and athletes who assisted them in the execution of this research project. Your valuable support and collaboration have been indispensable to the success of this endeavor.
References
- Juhan T, Bolia IK, Kang HP, Homere A, Romano R, Tibone JE, et al. Injury epidemiology and time lost from participation in women’s NCAA Division I Indoor Versus Beach Volleyball Players. Orthopaedic Journal of Sports Medicine. 2021; 9(4):23259671211004546. [DOI:10.1177/23259671211004546] [PMID]
- Wasser JG, Tripp B, Bruner ML, Bailey DR, Leitz RS, Zaremski JL, et al. Volleyball-related injuries in adolescent female players: An initial report. The Physician and Sportsmedicine. 2021; 49(3):323-30. [DOI:10.1080/00913847.2020.1826284] [PMID]
- Chandran A, Morris SN, Lempke LB, Boltz AJ, Robison HJ, Collins CL. Epidemiology of injuries in National Collegiate Athletic Association Women’s Volleyball: 2014-2015 Through 2018-2019. Journal of Athletic Training. 2021; 56(7):659–65. [DOI:10.4085/1062-6050-370-20]
- Zarei M, Eshghi S, Hosseinzadeh M. The effect of a shoulder injury prevention programme on proprioception and dynamic stability of young volleyball players; a randomized controlled trial. BMC Sports Science, Medicine and Rehabilitation. 2021; 13(1):71. [DOI:10.1186/s13102-021-00300-5] [PMID]
- Kim Y, Lee JM, Wellsandt E, Rosen AB. Comparison of shoulder range of motion, strength, and upper quarter dynamic balance between NCAA division I overhead athletes with and without a history of shoulder injury. Physical Therapy in Sport. 2020; 42:53-60. [DOI:10.1016/j.ptsp.2019.12.007] [PMID]
- Abbasi H, Alizadeh MH, Rajabi R, Mohammadi F. Comparison of static and dynamic postural stability between individuals with and without forward head posture. Physical Treatments-Specific Physical Therapy Journal. 2020; 10(3):127-34. [DOI:10.32598/ptj.10.3.364.3]
- Eslami R, Bahrami D, Mohsenzadeh H, Shahali H. Dynamic and static postural control among fighter pilots with spinal sagittal plane deformities. Medical Journal Armed Forces India. 2021; 77(4):459-65. [DOI:10.1016/j.mjafi.2021.03.017] [PMID]
- Schwiertz G, Beurskens R, Muehlbauer T. Discriminative validity of the lower and upper quarter Y-Balance test performance: A comparison between healthy trained and untrained youth. BMC Sports Science, Medicine & Rehabilitation. 2020; 12(1):73. [DOI:10.1186/s13102-020-00220-w] [PMID]
- Bauer J, Schedler S, Fischer S, Muehlbauer T. Relationship between Upper Quarter Y Balance Test performance and throwing proficiency in adolescent Olympic handball players. BMC Sports Science, Medicine & Rehabilitation. 2020; 12:50. [DOI:10.1186/s13102-020-00199-4] [PMID]
- Moradi M, Hadadnezhad M, Letafatkar A, Khosrokiani Z, Baker JS. Efficacy of throwing exercise with TheraBand in male volleyball players with shoulder internal rotation deficit: A randomized controlled trial. BMC Musculoskeletal Disorders. 2020; 21(1):376. [DOI:10.1186/s12891-020-03414-y] [PMID]
- Mirhassanzadeh Kooh-Kamar M, Hadadenjad M, Khaleghi Tazji M. [The impact of eight weeks of focused shoulder exercises on shoulder pain, proprioception, and kinematics, and upper limb function in male volleyball players with shoulder impingement syndrome: A randomized controlled clinical trial (Persian)]. Medical Journal of Tabriz University of Medical Sciences. 2020; 42(4):466-75. [DOI:10.34172/mj.2020.069]
- Thomas SJ, Swanik CB, Higginson JS, Kaminski TW, Swanik KA, Bartolozzi AR, et al. A bilateral comparison of posterior capsule thickness and its correlation with glenohumeral range of motion and scapular upward rotation in collegiate baseball players. Journal of Shoulder and Elbow Surgery. 2011; 20(5):708-16. [DOI:10.1016/j.jse.2010.08.031] [PMID]
- Celik D, Sirmen B, Demirhan M. The relationship of muscle strength and pain in subacromial impingement syndrome. Acta Orthopaedica et Traumatologica Turcica. 2011; 45(2):79-84. [DOI:10.3944/AOTT.2011.2425] [PMID]
- Westrick RB, Miller JM, Carow SD, Gerber JP. Exploration of the Y-Balance test for assessment of upper quarter closed kinetic chain performance. International Journal of Sports Physical Therapy. 2012; 7(2):139:47. [PMID]
- Gorman PP, Butler RJ, Plisky PJ, Kiesel KB. Upper quarter Y Balance Test: Reliability and performance comparison between genders in active adults. The Journal of Strength & Conditioning Research. 2012; 26(11):3043-8. [DOI:10.1519/JSC.0b013e3182472fdb] [PMID]
- Maddaluno MLM, Ferreira APA, Tavares ACLC, Meziat-Filho N, Ferreira AS. Craniocervical posture assessed with photogrammetry and the accuracy of palpation methods for locating the seventh cervical spinous process: A cross-sectional study. Journal of Manipulative and Physiological Therapeutics. 2021; 44(3):196-204. [DOI:10.1016/j.jmpt.2020.07.012] [PMID]
- Gliga AC, Neagu N, Szabo DA. Optimising the validity of shoulder range of motion evaluation: A comparative study. BRAIN Broad Research in Artificial Intelligence and Neuroscience. 2021; 11(4Sup1):101-12. [DOI:10.18662/brain/11.4Sup1/158]
- Olivier N, Daussin FN. Relationships between isokinetic shoulder evaluation and fitness characteristics of elite French female Water-Polo players. Journal of Human Kinetics. 2018; 64:5-11. [DOI:10.1515/hukin-2017-0181] [PMID]
- Walaszek R, Chwała W, Walaszek K, Burdacki M. The assessment of the relationships between body posture indices and the Y-Balance Test results in the adolescents. Acta of Bioengineering and Biomechanics. 2018; 20(2):149-57. [PMID]
- Borms D, Cools A. Upper-extremity functional performance tests: Reference values for overhead athletes. International Journal of Sports Medicine. 2018; 39(06):433-41. [DOI:10.1055/a-0573-1388] [PMID]
- Gribble PA, Hertel J, Plisky P. Using the Star Excursion Balance Test to assess dynamic postural-control deficits and outcomes in lower extremity injury: A literature and systematic review. Journal of Athletic Training. 2012; 47(3):339-57. [DOI:10.4085/1062-6050-47.3.08] [PMID]
- Penha PJ, João SM, Casarotto RA, Amino CJ, Penteado DC. Postural assessment of girls between 7 and 10 years of age. Clinics. 2005; 60(1):9-16. [DOI:10.1590/S1807-59322005000100004] [PMID]
- Hurd WJ, Kaplan KM, ElAttrache NS, Jobe FW, Morrey BF, Kaufman KR. A profile of glenohumeral internal and external rotation motion in the uninjured high school baseball pitcher, part II: strength. Journal of Athletic Training. 2011; 46(3):289-95. [DOI:10.4085/1062-6050-46.3.289]
- Hajihosseini E, Norasteh A, Shamsi A, Daneshmandi H. The effects of strengthening, stretching and comprehensive exercises on forward shoulder posture correction. Physical Treatments-Specific Physical Therapy Journal. 2014; 4(3):123-32. [Link]
- Grace TG. Muscle imbalance and extremity injury. A perplexing relationship. Sports Medicine (Auckland, NZ). 1985; 2(2):77-82. [DOI:10.2165/00007256-198502020-00001] [PMID]
- Lees A. Science and the major racket sports: A review. Journal of Sports Sciences. 2003; 21(9):707-32. [DOI:10.1080/0264041031000140275] [PMID]
- PourRahim Ghouroghchi A, Pahlevani M. [The investigation of relationship between the joints range of motion and time of 50, 100 and 200m breaststroke swimming in 12-13 years elite swimmer boys participated in the National Championship of the Country Selection in 2016 in Tehran (Persian)]. Journal of Rafsanjan University of Medical Sciences. 2019; 18(2):161-76. [Link]
- Winter DA. Human balance and posture control during standing and walking. Gait & Posture. 1995; 3(4):193-214. [DOI:10.1016/0966-6362(96)82849-9]
- Trowbridge CA. The effects of strength and plyometric training on joint position, joint moments, and joint stiffness at the knee. Ann Arbor: University Microfilms; 2004. [Link]
- Docherty CL, Moore JH, Arnold BL. Effects of strength training on strength development and joint position sense in functionally unstable ankles. Journal of Athletic Training. 1998; 33(4):310-4. [PMID]
Type of Study: Research |
Subject:
Special
Received: 2023/10/22 | Accepted: 2024/03/9 | Published: 2024/04/1
Received: 2023/10/22 | Accepted: 2024/03/9 | Published: 2024/04/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Attribution-NonCommercial 4.0 International License.
Contact Information
Journal Office Tel: +9821 71732837, 71732220
Publisher Tel: +9821 4535 5555, 4535 5000 (EXT: 108)
Email: physicaltreatments@gmail.com
