Sat, Jul 25, 2026
Volume 14, Issue 1 (Winter 2024)
PTJ 2024, 14(1): 11-22 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Mahmoudi F, Daneshjoo A, Bahiraei S, Sahebozamani M. Effects of Injury Prevention Programs on Muscle Flexibility in Children and Adolescents: A Systematic Review. PTJ 2024; 14 (1) :11-22
URL: http://ptj.uswr.ac.ir/article-1-599-en.html
URL: http://ptj.uswr.ac.ir/article-1-599-en.html



1- Department of Sports Injuries and Corrective Exercises, Faculty of Sports Sciences, Shahid Bahonar University of Kerman, Kerman, Iran.
Full-Text [PDF 542 kb]
(3120 Downloads)
| Abstract (HTML) (3712 Views)
Full-Text: (3031 Views)
Introduction
Participation of children and adolescents in sports is known as a major cause of pain and injury [1, 2]. The medical, financial, and human resources associated with the economic burden of injury have different levels that are related to the individual and the society [3, 4, 5]. Injury prevention programs (IPPs) in children and adolescents are necessary to prevent sports injuries and reduce individual and social costs related to treatment and rehabilitation.
Injury prevention strategies mainly focus on risk factors. Athletes’ risk factors can be classified as either extrinsic or intrinsic, as well as modifiable or non-modifiable [6]. Shoe type, competition or skill level, level of play, or use of tape or brace equipment are examples of extrinsic risk factors [6]. In contrast, intrinsic factors influencing athletes’ risk encompass variables, such as age, sex, body dimensions, anatomical alignment challenges, muscle performance deficiencies, limited flexibility, impaired balance, coordination, endurance, previous injuries, foot morphology, and psychological or social considerations [7]. Any intrinsic or extrinsic factors can affect movement and performance. Some intrinsic risk factors, such as muscle flexibility are modifiable and thus can be targeted in IPPs [8]. IPPs are essential for the safety of youth sports. Multifaceted interventions with systematic frameworks are often used in standardized IPPs for youth [9]. In contrast to individualized programs, standardized IPPs are implemented either fully or partially on the field before training or competition begins, and regularly throughout the season [10].
The lack of flexibility is one of the most common possible intrinsic risk factors for developing muscle and ligament injuries [11]. The available data are insufficient to substantiate a connection between increased flexibility and a reduced risk of injury [12]. In reality, both excessive and insufficient flexibility can lead to injury, and, in certain situations, enhancing flexibility may increase injury susceptibility [13]. Injuries to muscles occurring within the normal range of motion are not attributed to a lack of flexibility [14]. However, athletes with imbalances in flexibility may be at a higher risk of injury [15]. In several prospective cohort studies, restricted range of motion due to muscle tightness [16, 17, 18, 19] and muscle asymmetry or interlimb range of motion asymmetry [20-22] have been associated with sports injuries.
Several randomized control trials (RCTs) have been published on the effect of injury prevention programs on flexibility in children and adolescents [23-27], and no systematic review study has been conducted in this field. As mentioned above, IPPs focus on risk factors, and muscle flexibility is a modifiable risk factor; therefore, the present systematic review was conducted to investigate the effects of IPPs on muscle flexibility in children and adolescents.
Materials and Methods
Search strategy and selection of studies
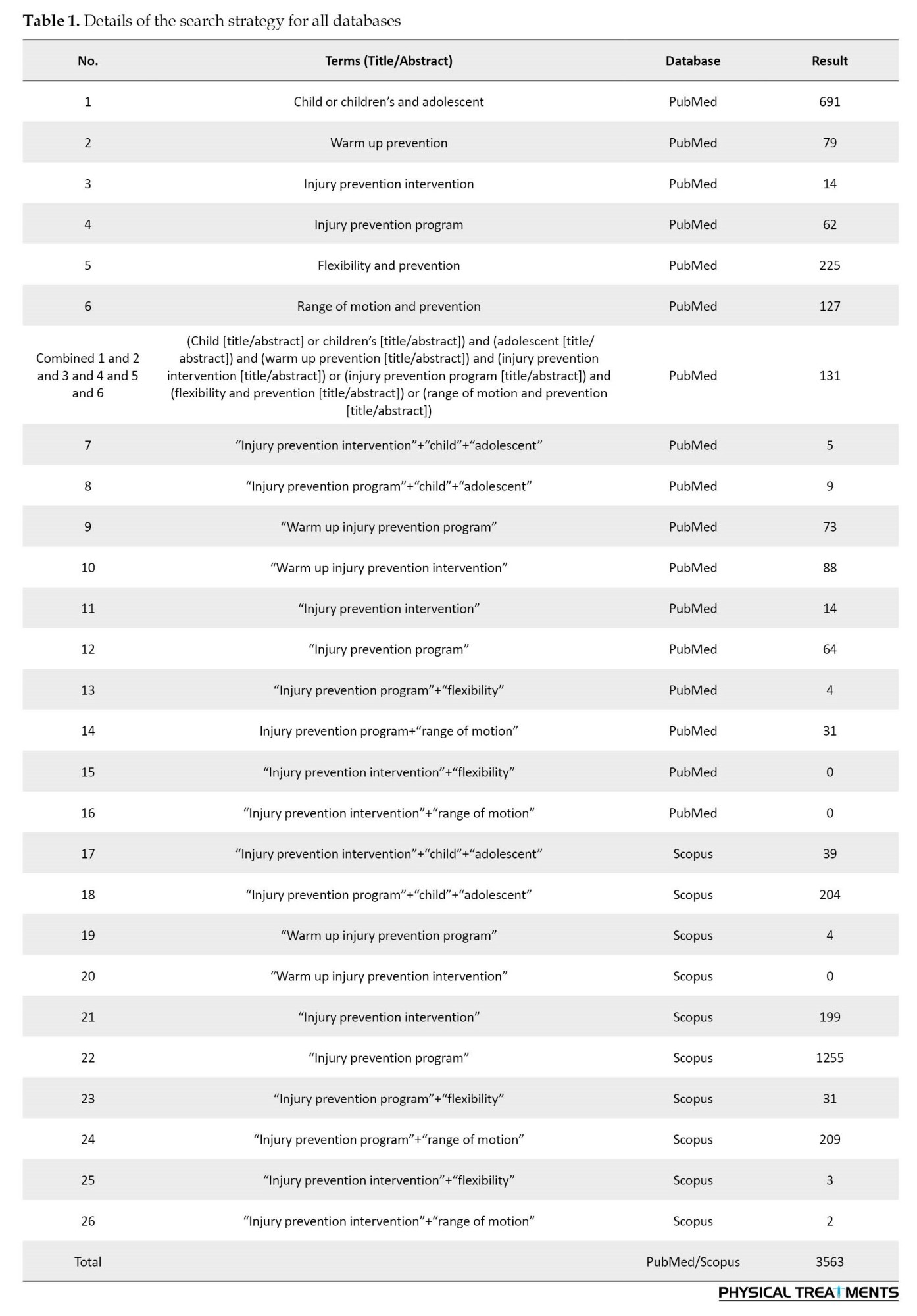
The International prospective register of systematic reviews has the protocol for this systematic review available online. This study is a systematic review based on the PRISMA checklist, and all relevant articles were extracted using a search strategy [28]. One of the reviewers (FM) searched the following electronic databases for relevant studies published up to December 2022 in PubMed and Scopus. Search terms were linked using Boolean logic (and [between categories], or [within categories]). Table 1 presents how to search all databases.
Following established inclusion and exclusion criteria, two reviewers (FM and SB) independently further reviewed studies for title and abstract content, and read the full text of studies meeting the criteria to determine final inclusion. In cases where the content was still ambiguous, the complete text was obtained for additional scrutiny, and suitable studies were pinpointed. After screening, the two reviewers (FM and SB) results were compared by another author (AD). Studies were reviewed by one of the reviewers (MS) collectively according to the eligibility criteria to resolve any disagreements.
Eligibility criteria
Relevant studies were identified using predetermined selection criteria and the population intervention comparison outcome study design (PICOS) technique [28]. The inclusion criteria included population: Subjects were children and adolescents with an average age under 17 years old, intervention: The intervention program was an injury prevention program (IPP), comparison: The study assessed an intervention group enrolled in a supervised warm-up prevention program and control the group, outcome: One of the primary outcomes was the muscle flexibility, study design: The types of studies were RCTs. The exclusion criteria included studies of other interventions, non-English language research, summaries of case reports, systematic reviews, interviews, and conferences, and a quasi-random assignment study with no available data.
Risk of bias assessment
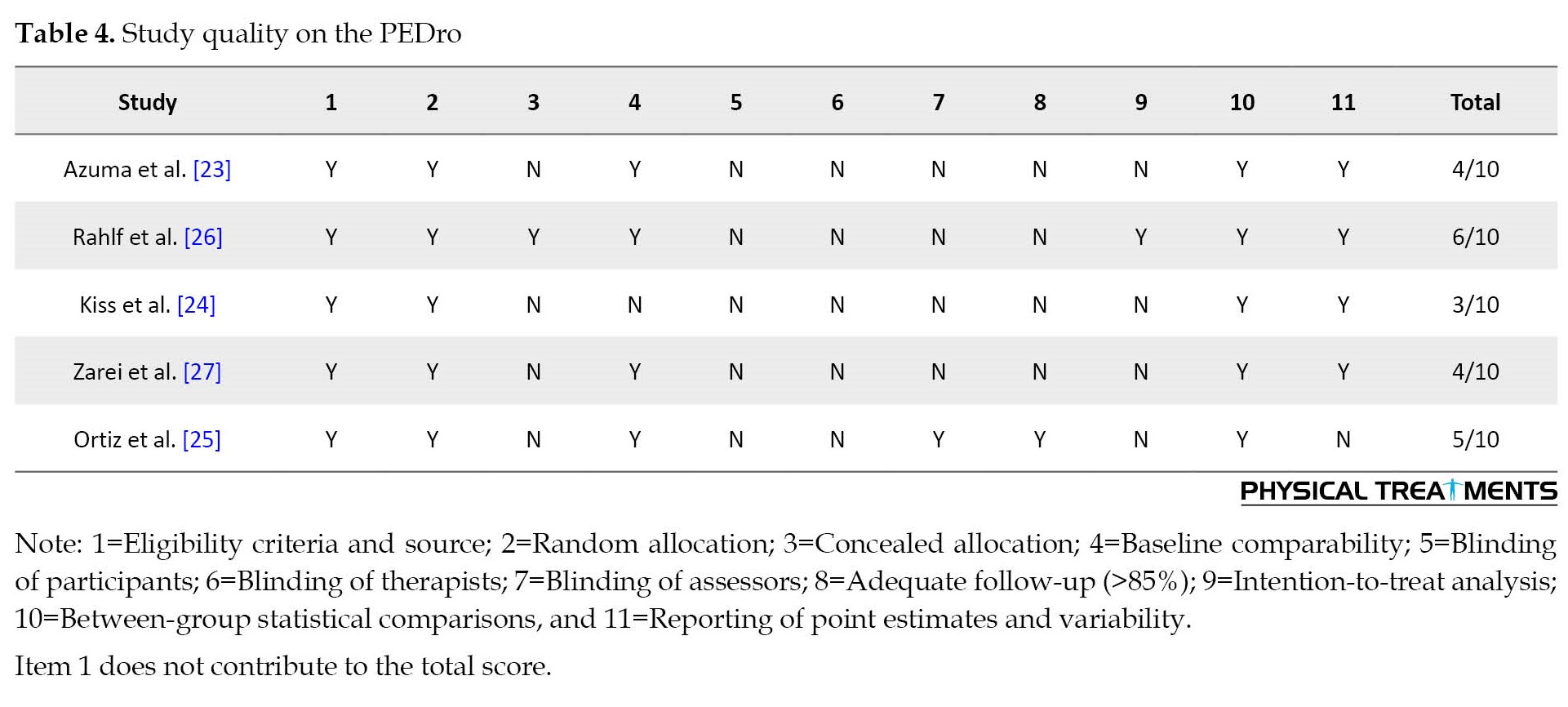
Two reviewers (AD and MS) used the physiotherapy evidence database scale (PEDro) to assess the quality of studies [29]. The scoring of this scale was done according to 11 factors from the Delphi list to evaluate the quality of RCTs, from 0 (high risk of bias) to 10 (low risk of bias) [30]. This scale assesses factors associated with the risk of bias in studies. The PEDro total score for items 2 to 11 was obtained as a total score from 0 to 10 [29]. Thus, PEDro scores <4 (0-3) are considered “poor”, 4-5 “fair”, 6-8 “good” and 9-10 “excellent” [31].
Data extraction
The reviewer (FM) used an Excel software, version 2019 (Microsoft, Redmond, WA, USA) to extract the necessary data from the included research. The retrieved data comprised two main types of information, basic study information, such as the author and research publication time, and study experimental parameters, including sample size, age, intervention type, frequency, duration, and outcome measures. An IPP is defined as “activities aimed at preventing, ameliorating, treating, and or reducing injury-related disability and mortality” [32]. Flexibility was defined as the result, representing an intrinsic property of body tissues that determines the achievable range of motion at a joint or group of joints without risk of injury [33].
Synthesis and analysis of data
According to the studies in this review, the data of the studies were derived from several different types of IPPs. On the other hand, the tests used to assess flexibility and the areas and muscles measured in the studies were different, which may affect the sample heterogeneity for each type of analysis. For these reasons, the final number of studies was considered insufficient for any type of meta-analysis.
Results
Search results
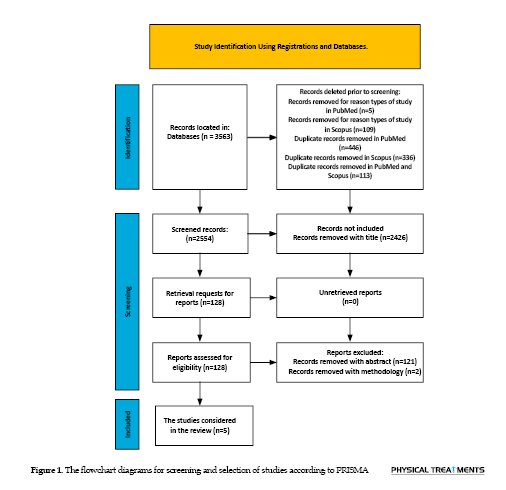
Up until December 1,2022,3563 studies were first obtained from several databases (PubMed and Scopus). After excluding 1009 duplicate and non-RCT studies, 2554 studies were obtained, and the following five studies were selected. The PRISMA standards were adhered to during the screening of specific studies. Figure 1 shows the selection process.
Characteristics of the included studies
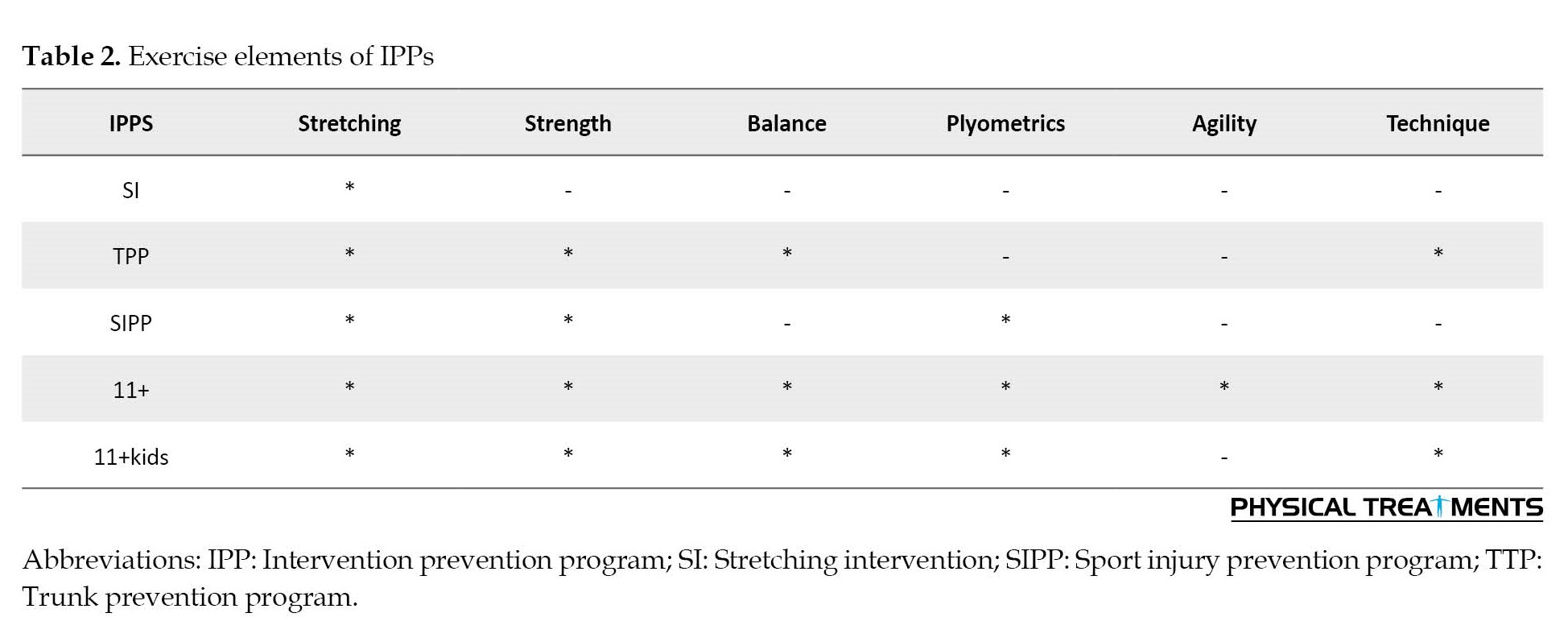
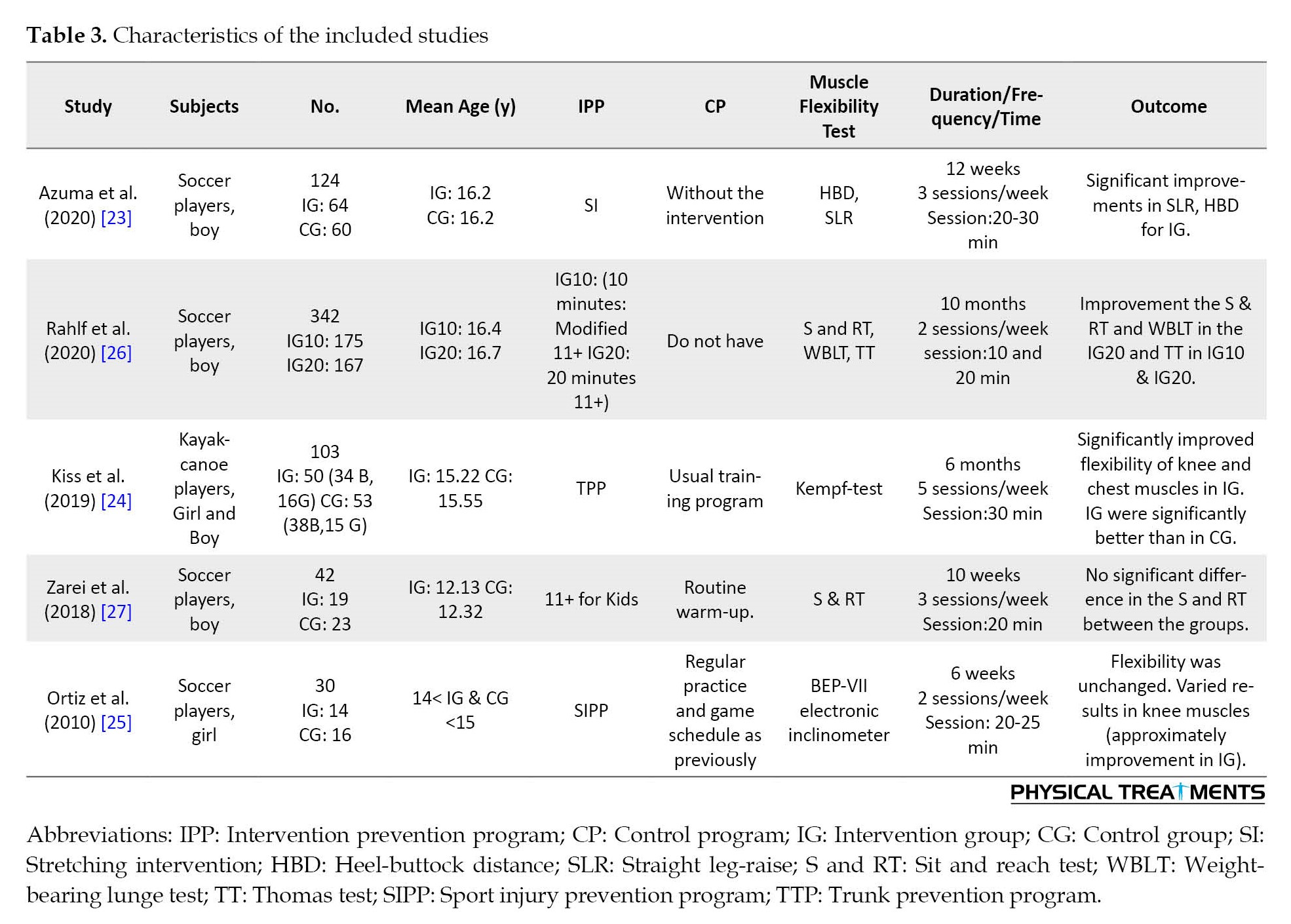
One of the five studies was a cluster-randomized trial [23], and the other 4 studies were RCTs [24-27]. A total of 641 participants (580 boys, and 61 girls) were included in this analysis. All players were below 17 years old. Three studies only included boys [23, 26, 27], one study included girls [25], and one study included 538 boys and girls [24] who were soccer players [23, 25-27], and 103 boys and girls who were kayak-canoe players [24]. The number of 489 participants (459 boys and 30 girls) (76%) received IPPs. The IPPs of these studies were stretching intervention (without the use of any equipment) [23], trunk prevention program (TPP) [24], sports injury prevention program (SIPP) [25], FIFA 11+ and modification FIFA 11+ [26], and FIFA 11+ for kids [27]. Table 2 presents a summary of the exercise elements of IPPs.
Normal and usual warm-up training was used in 4 studies [23-25, 27] and another study did not have a control group [26]. The IPP duration was 6 weeks to 10 months, the IPP frequency was 2 to 5 sessions per week, and the time per session was 10-30 minutes. Outcome indicators included the flexibility that was measured with heel-buttock distance (HBD), straight leg-raise (SLR) (quadriceps femoris, hamstring and hip rotator muscles) [23], Kempf-test (pectoralis major and quadriceps femoris) [24], BEP-VLL electronic inclinometer (iliopsoas, rectus femoris, hamstring and gastrocnemius) [25], Thomas test (TT) (hip flexibility), sit and reach test (S and RT) (hamstring and lower back flexibility) [26, 27], weight-bearing lunge test (WBLT) (dorsiflexion range of ankle) [26]. Table 3 summarizes the characteristics of the five included studies.
Risk of bias assessment
The range of PEDro scores was from three to six out of ten. The methodological quality of one study was “good” [26], three studies were “fair” [23, 25, 27], and one study was “poor” [24]. According to these PEDro ratings, the five included studies have a low risk of bias (Table 4).
Main results
Most injury prevention programs (three out of five articles) showed improvement in the muscle flexibility of children and adolescents (significant improvement between before and after the intervention). However, Azuma et al. showed no significant difference between IG and CG. The IG showed a significant improvement in HBD (decreased) and SLR (increased) after the stretching intervention [23]. As a result, TPP, the flexibility of the pectoralis major muscle on the right and left side improved (decreased) significantly in IG, but no significant change was observed in CG. Also, quadriceps flexibility in IG showed a significant improvement (decreased), although the change in the left leg of CG was not significant, but it was significant in the right leg. The effect of the program was significantly better in IG than in CG [24]. The SIPP showed that the flexibility of the rectus femoris, hamstring, and gastrocnemius muscles did not change significantly on the left side, but it showed improvement in flexibility on the right side, which had the greatest effect on the gastrocnemius. The IG group exhibited a significant increase in gastrocnemius muscle flexibility [25]. A significant difference was observed in S and RT and WBLT between the two 11+ programs, with 10 minutes (IG10) and 20 minutes (IG20). In IG20, a significant increase was observed in the pre- and Post-tests after 30 training sessions [26]. No significant difference was observed between IG and CG in S and RT [27].
Discussion
This systematic review was conducted to investigate the effects of IPPs on muscle flexibility in children and adolescents. We included five studies with 641 participants (580 boys, 61 girls), and the results showed that the methodological quality of one study was “good” [26], three studies were “fair” [23, 25, 27], and one study was “poor” [24]. Similar studies face difficulties in achieving blinding, concealed allocation, adequate follow-up, and intention-to-treat analysis when the investigator actively participates in the training. Therefore, we recommend that in future research, both the researcher and the subjects be blinded. Therefore, it is necessary to pay attention to double blindness, code names, careful design of the program, use of experts, and continuous communication with the participants to improve the quality of the evidence. The ratio of boy-to-girl samples was higher, which may be due to the availability of boys, cultural limitations for girls, or the chosen sports field in the studies since most studies were conducted on soccer players. We hypothesize that greater risk factors, popularity, and more media advertising were the reasons for choosing soccer in most studies. The increase in girl samples and diversity in the studied sports should be considered in future studies. The results of the studies showed that the IPPs were selected according to the type of sport studied and the common injuries in those tasks, based on this, tests to measure flexibility and related muscles have been used. It is suggested to use and compare similar programs and tests in future studies.
The results of the study showed that stretching training for 12 weeks (36 sessions) among boy soccer players in IG improves muscle flexibility [23]. Review articles reported that stretching decreases injury incidence and musculoskeletal injury risk [34-38]. Therefore, stretching exercises are one of the components of injury prevention programs. The evidence on the effect of stretching exercises on muscle flexibility is conflicting. In this regard, Magnusson et al. reported that 10 static stretches during 3 weeks (21 sessions) for each stretch of 45s in women do not affect the stretching properties of hamstrings; also, Klinge et al. showed the same result with 4 static stretches, twice a day, during 13 weeks (182 sessions) [39, 40]. However, Mahieu et al. stated that after 6 weeks of a stretching program consisting of five static and ballistic stretches (20s stretch, 20s rest), a significant reduction in passive stiffness in plantar flexors occurred [41]. According to the above-mentioned evidence, the effect of stretching training on muscle flexibility to prevent sports injuries depends on factors, such as intensity, duration, frequency, type of stretching, and the gender, level of activity, and individual characteristics of the subjects studied, which should be considered in future studies. The results of this literature review are consistent with studies conducted by Coledam et al. [42], Needham et al. [43], and Mayorga-Vega [44]. However, they diverge from the research conducted by Faigenbaum et al. [45], Pearce et al. [46], and Duncan et al. [47]. This disparity can be attributed to factors, such as the focus on non-athlete children and youth and the examination of acute effects or specific types of flexibility in their studies.
After the trunk prevention exercise program (correct posture, stretching, static exercise on an unstable surface, dynamic exercise on a stable surface, resistance exercise, proprioceptive exercise) on the kayak-canoe boy and girl athletes for 6 months (5 d/w, 30 min), the muscle flexibility of the left and right pectoralis major in the IG improved significantly, but in the CG, it changed, but not significantly. Muscle flexibility of quadriceps femoris in IG, the distance of the heel, and the ischial tuberosity on the left and right leg significantly reduced, in CG on the left the change was not significant, on the right leg it was significant. Comparing the two groups after the program, the results of the IG were significantly better than those of the CG [24]. The stretching program included the hip flexor, hip extensor, and pectoralis major muscles [24]. No evidence was found regarding the effect of the trunk injury prevention program on flexibility, but this program examines the core muscle more [24]. In a study on female professional golfers, Kim showed that 12 weeks (3 d/w, 60 min) of core training had a positive effect on flexibility [48]. Although the sample size in Kim’s study was small, the results were similar to Kiss’s study [24, 48]. Considering that trunk prevention exercises focus more on the trunk muscles and the studies conducted are on sports where the trunk muscles are crucial, the sex and level of physical fitness of the subjects are significant. Although the exercises were different in terms of follow-up and prevention time, it is suggested to be done with different intensity, duration, and frequency in the next research.
Sports injury prevention program on female soccer players for 6 weeks (2 d/w) had no significant effect on muscle flexibility (rectus femoris, hamstring, gastrocnemius) on the left side, but it was significant on the right side. The most significant length was gastrocnemius muscle. In CG, a significant increase occurred only in the gastrocnemius muscle flexibility [25]. Lim et al. reported that an 8-week (20 min) injury prevention program in female basketball players increased flexibility [49]. The SIPP included stretching, strength, and polymetric exercises of the lower limbs, which, despite stretching exercises, is expected to have a positive effect on muscle flexibility. According to the research results, the sample size, dominant/non-dominant leg, and intensity, duration, and frequency of the program play a role in improving flexibility. It is to do this program for boys and other sports.
In a study conducted by Rahlf et al. on the effect of the 11+ program on boy soccer players in two groups (INT10, INT20) with different durations (10 min, 20 min) for 10 months (2 d/w), they stated that 11+ with a duration of 20 min had a positive effect on flexibility compared to 11+ with a time of 10 m [26]. Arede et al. reported that 11+ for 6 weeks (2 d/w) improves flexibility in boy soccer players [50]; although in the study conducted by Zarei et al., the effect was not significant [51]. FIFA 11+ comprises 15 distinct workouts, including six running exercises, three body stability exercises, two strength exercises, one jumping exercise, and three cooling-down exercises. Although 11+ excludes stretching exercises, the results showed that it has a positive effect on flexibility. According to the results of the studies, 11+ with less duration and number of sessions had less effect than 11+ with more duration, and this indicates that the duration, and frequency of the program are effective on the flexibility, which should be given more attention.
The 11+ kids program for 10 weeks (3 d/w, 20 min) on boy soccer players showed no effect on flexibility [27]. Tseng et al. stated that 11+ kids for 8 weeks (5 d/w) improves flexibility in elementary school students [52]. Anam et al. showed that 11+ kids have a significant increase in the muscle flexibility of boy soccer players in 12 weeks (2 d/w) [53]. The reason for the inconsistency in the results may be the level of activity and number of samples, the duration, and frequency of the program. Also, the 11+ Kids program does not have stretching exercises and focuses more on coordination, balance, landing technique, strengthening the leg muscles, and core stability muscles and is for children under 13 years old. Perhaps the reason for not being significant is the lack of stretching exercises in the program, although, in a meta-analysis, Alizadeh et al. showed that resistance training alone improves range of motion, this improvement was not significantly different compared to stretching training alone [54], and this means that more studies should be conducted in this field. Therefore, it is essential to pay attention to the activity level of the samples and their gender and frequency and duration program in future studies.
Conclusion
Injury prevention programs can improve the muscle flexibility of children and adolescents (significant improvement between before and after the intervention), although no improvement was observed in the control group. Therefore, factors, such as duration, frequency and intensity of the program, gender, activity level, type of sport, and sample size are decisive in muscle flexibility.
Limitations
Considering the diversity of injury prevention programs (for example, 11+ and 11+ kids, etc.) and searching with the keyword “prevention program”, using two databases for searching, it some articles may not have been used in this study. Another limitation that can be stated is that due to the variety of preventive programs in this study and the non-similarity of the programs and tests to measure flexibility, statistical analysis of the impact of the programs on flexibility was not possible. The current systematic review only includes articles in language English, which limits the language in the search strategy and the number of articles, therefore, it is suggested to use different languages in future studies.
Ethical Considerations
Compliance with ethical guidelines
There were no ethical considerations to be considered in this research.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization, study search, data collection and original draft preparation: Foad Mahmoudi; Methodology, validation, study selection, review and editing: Foad Mahmoudi and Abdolhamid Daneshjoo; Software and formal analysis: Foad Mahmoudi and Saeid Bahiraei; Risk of bias assessment and certainty assessmen: Foad Mahmoudi, Abdolhamid Daneshjoo, and Saeid Bahiraei; Supervision, Abdolhamid Daneshjoo and Mansour Sahebozamani.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors thank the authors of the articles used in this study.
References
Participation of children and adolescents in sports is known as a major cause of pain and injury [1, 2]. The medical, financial, and human resources associated with the economic burden of injury have different levels that are related to the individual and the society [3, 4, 5]. Injury prevention programs (IPPs) in children and adolescents are necessary to prevent sports injuries and reduce individual and social costs related to treatment and rehabilitation.
Injury prevention strategies mainly focus on risk factors. Athletes’ risk factors can be classified as either extrinsic or intrinsic, as well as modifiable or non-modifiable [6]. Shoe type, competition or skill level, level of play, or use of tape or brace equipment are examples of extrinsic risk factors [6]. In contrast, intrinsic factors influencing athletes’ risk encompass variables, such as age, sex, body dimensions, anatomical alignment challenges, muscle performance deficiencies, limited flexibility, impaired balance, coordination, endurance, previous injuries, foot morphology, and psychological or social considerations [7]. Any intrinsic or extrinsic factors can affect movement and performance. Some intrinsic risk factors, such as muscle flexibility are modifiable and thus can be targeted in IPPs [8]. IPPs are essential for the safety of youth sports. Multifaceted interventions with systematic frameworks are often used in standardized IPPs for youth [9]. In contrast to individualized programs, standardized IPPs are implemented either fully or partially on the field before training or competition begins, and regularly throughout the season [10].
The lack of flexibility is one of the most common possible intrinsic risk factors for developing muscle and ligament injuries [11]. The available data are insufficient to substantiate a connection between increased flexibility and a reduced risk of injury [12]. In reality, both excessive and insufficient flexibility can lead to injury, and, in certain situations, enhancing flexibility may increase injury susceptibility [13]. Injuries to muscles occurring within the normal range of motion are not attributed to a lack of flexibility [14]. However, athletes with imbalances in flexibility may be at a higher risk of injury [15]. In several prospective cohort studies, restricted range of motion due to muscle tightness [16, 17, 18, 19] and muscle asymmetry or interlimb range of motion asymmetry [20-22] have been associated with sports injuries.
Several randomized control trials (RCTs) have been published on the effect of injury prevention programs on flexibility in children and adolescents [23-27], and no systematic review study has been conducted in this field. As mentioned above, IPPs focus on risk factors, and muscle flexibility is a modifiable risk factor; therefore, the present systematic review was conducted to investigate the effects of IPPs on muscle flexibility in children and adolescents.
Materials and Methods
Search strategy and selection of studies
The International prospective register of systematic reviews has the protocol for this systematic review available online. This study is a systematic review based on the PRISMA checklist, and all relevant articles were extracted using a search strategy [28]. One of the reviewers (FM) searched the following electronic databases for relevant studies published up to December 2022 in PubMed and Scopus. Search terms were linked using Boolean logic (and [between categories], or [within categories]). Table 1 presents how to search all databases.
Following established inclusion and exclusion criteria, two reviewers (FM and SB) independently further reviewed studies for title and abstract content, and read the full text of studies meeting the criteria to determine final inclusion. In cases where the content was still ambiguous, the complete text was obtained for additional scrutiny, and suitable studies were pinpointed. After screening, the two reviewers (FM and SB) results were compared by another author (AD). Studies were reviewed by one of the reviewers (MS) collectively according to the eligibility criteria to resolve any disagreements.
Eligibility criteria
Relevant studies were identified using predetermined selection criteria and the population intervention comparison outcome study design (PICOS) technique [28]. The inclusion criteria included population: Subjects were children and adolescents with an average age under 17 years old, intervention: The intervention program was an injury prevention program (IPP), comparison: The study assessed an intervention group enrolled in a supervised warm-up prevention program and control the group, outcome: One of the primary outcomes was the muscle flexibility, study design: The types of studies were RCTs. The exclusion criteria included studies of other interventions, non-English language research, summaries of case reports, systematic reviews, interviews, and conferences, and a quasi-random assignment study with no available data.
Risk of bias assessment
Two reviewers (AD and MS) used the physiotherapy evidence database scale (PEDro) to assess the quality of studies [29]. The scoring of this scale was done according to 11 factors from the Delphi list to evaluate the quality of RCTs, from 0 (high risk of bias) to 10 (low risk of bias) [30]. This scale assesses factors associated with the risk of bias in studies. The PEDro total score for items 2 to 11 was obtained as a total score from 0 to 10 [29]. Thus, PEDro scores <4 (0-3) are considered “poor”, 4-5 “fair”, 6-8 “good” and 9-10 “excellent” [31].
Data extraction
The reviewer (FM) used an Excel software, version 2019 (Microsoft, Redmond, WA, USA) to extract the necessary data from the included research. The retrieved data comprised two main types of information, basic study information, such as the author and research publication time, and study experimental parameters, including sample size, age, intervention type, frequency, duration, and outcome measures. An IPP is defined as “activities aimed at preventing, ameliorating, treating, and or reducing injury-related disability and mortality” [32]. Flexibility was defined as the result, representing an intrinsic property of body tissues that determines the achievable range of motion at a joint or group of joints without risk of injury [33].
Synthesis and analysis of data
According to the studies in this review, the data of the studies were derived from several different types of IPPs. On the other hand, the tests used to assess flexibility and the areas and muscles measured in the studies were different, which may affect the sample heterogeneity for each type of analysis. For these reasons, the final number of studies was considered insufficient for any type of meta-analysis.
Results
Search results
Up until December 1,2022,3563 studies were first obtained from several databases (PubMed and Scopus). After excluding 1009 duplicate and non-RCT studies, 2554 studies were obtained, and the following five studies were selected. The PRISMA standards were adhered to during the screening of specific studies. Figure 1 shows the selection process.
Characteristics of the included studies
One of the five studies was a cluster-randomized trial [23], and the other 4 studies were RCTs [24-27]. A total of 641 participants (580 boys, and 61 girls) were included in this analysis. All players were below 17 years old. Three studies only included boys [23, 26, 27], one study included girls [25], and one study included 538 boys and girls [24] who were soccer players [23, 25-27], and 103 boys and girls who were kayak-canoe players [24]. The number of 489 participants (459 boys and 30 girls) (76%) received IPPs. The IPPs of these studies were stretching intervention (without the use of any equipment) [23], trunk prevention program (TPP) [24], sports injury prevention program (SIPP) [25], FIFA 11+ and modification FIFA 11+ [26], and FIFA 11+ for kids [27]. Table 2 presents a summary of the exercise elements of IPPs.
Normal and usual warm-up training was used in 4 studies [23-25, 27] and another study did not have a control group [26]. The IPP duration was 6 weeks to 10 months, the IPP frequency was 2 to 5 sessions per week, and the time per session was 10-30 minutes. Outcome indicators included the flexibility that was measured with heel-buttock distance (HBD), straight leg-raise (SLR) (quadriceps femoris, hamstring and hip rotator muscles) [23], Kempf-test (pectoralis major and quadriceps femoris) [24], BEP-VLL electronic inclinometer (iliopsoas, rectus femoris, hamstring and gastrocnemius) [25], Thomas test (TT) (hip flexibility), sit and reach test (S and RT) (hamstring and lower back flexibility) [26, 27], weight-bearing lunge test (WBLT) (dorsiflexion range of ankle) [26]. Table 3 summarizes the characteristics of the five included studies.
Risk of bias assessment
The range of PEDro scores was from three to six out of ten. The methodological quality of one study was “good” [26], three studies were “fair” [23, 25, 27], and one study was “poor” [24]. According to these PEDro ratings, the five included studies have a low risk of bias (Table 4).
Main results
Most injury prevention programs (three out of five articles) showed improvement in the muscle flexibility of children and adolescents (significant improvement between before and after the intervention). However, Azuma et al. showed no significant difference between IG and CG. The IG showed a significant improvement in HBD (decreased) and SLR (increased) after the stretching intervention [23]. As a result, TPP, the flexibility of the pectoralis major muscle on the right and left side improved (decreased) significantly in IG, but no significant change was observed in CG. Also, quadriceps flexibility in IG showed a significant improvement (decreased), although the change in the left leg of CG was not significant, but it was significant in the right leg. The effect of the program was significantly better in IG than in CG [24]. The SIPP showed that the flexibility of the rectus femoris, hamstring, and gastrocnemius muscles did not change significantly on the left side, but it showed improvement in flexibility on the right side, which had the greatest effect on the gastrocnemius. The IG group exhibited a significant increase in gastrocnemius muscle flexibility [25]. A significant difference was observed in S and RT and WBLT between the two 11+ programs, with 10 minutes (IG10) and 20 minutes (IG20). In IG20, a significant increase was observed in the pre- and Post-tests after 30 training sessions [26]. No significant difference was observed between IG and CG in S and RT [27].
Discussion
This systematic review was conducted to investigate the effects of IPPs on muscle flexibility in children and adolescents. We included five studies with 641 participants (580 boys, 61 girls), and the results showed that the methodological quality of one study was “good” [26], three studies were “fair” [23, 25, 27], and one study was “poor” [24]. Similar studies face difficulties in achieving blinding, concealed allocation, adequate follow-up, and intention-to-treat analysis when the investigator actively participates in the training. Therefore, we recommend that in future research, both the researcher and the subjects be blinded. Therefore, it is necessary to pay attention to double blindness, code names, careful design of the program, use of experts, and continuous communication with the participants to improve the quality of the evidence. The ratio of boy-to-girl samples was higher, which may be due to the availability of boys, cultural limitations for girls, or the chosen sports field in the studies since most studies were conducted on soccer players. We hypothesize that greater risk factors, popularity, and more media advertising were the reasons for choosing soccer in most studies. The increase in girl samples and diversity in the studied sports should be considered in future studies. The results of the studies showed that the IPPs were selected according to the type of sport studied and the common injuries in those tasks, based on this, tests to measure flexibility and related muscles have been used. It is suggested to use and compare similar programs and tests in future studies.
The results of the study showed that stretching training for 12 weeks (36 sessions) among boy soccer players in IG improves muscle flexibility [23]. Review articles reported that stretching decreases injury incidence and musculoskeletal injury risk [34-38]. Therefore, stretching exercises are one of the components of injury prevention programs. The evidence on the effect of stretching exercises on muscle flexibility is conflicting. In this regard, Magnusson et al. reported that 10 static stretches during 3 weeks (21 sessions) for each stretch of 45s in women do not affect the stretching properties of hamstrings; also, Klinge et al. showed the same result with 4 static stretches, twice a day, during 13 weeks (182 sessions) [39, 40]. However, Mahieu et al. stated that after 6 weeks of a stretching program consisting of five static and ballistic stretches (20s stretch, 20s rest), a significant reduction in passive stiffness in plantar flexors occurred [41]. According to the above-mentioned evidence, the effect of stretching training on muscle flexibility to prevent sports injuries depends on factors, such as intensity, duration, frequency, type of stretching, and the gender, level of activity, and individual characteristics of the subjects studied, which should be considered in future studies. The results of this literature review are consistent with studies conducted by Coledam et al. [42], Needham et al. [43], and Mayorga-Vega [44]. However, they diverge from the research conducted by Faigenbaum et al. [45], Pearce et al. [46], and Duncan et al. [47]. This disparity can be attributed to factors, such as the focus on non-athlete children and youth and the examination of acute effects or specific types of flexibility in their studies.
After the trunk prevention exercise program (correct posture, stretching, static exercise on an unstable surface, dynamic exercise on a stable surface, resistance exercise, proprioceptive exercise) on the kayak-canoe boy and girl athletes for 6 months (5 d/w, 30 min), the muscle flexibility of the left and right pectoralis major in the IG improved significantly, but in the CG, it changed, but not significantly. Muscle flexibility of quadriceps femoris in IG, the distance of the heel, and the ischial tuberosity on the left and right leg significantly reduced, in CG on the left the change was not significant, on the right leg it was significant. Comparing the two groups after the program, the results of the IG were significantly better than those of the CG [24]. The stretching program included the hip flexor, hip extensor, and pectoralis major muscles [24]. No evidence was found regarding the effect of the trunk injury prevention program on flexibility, but this program examines the core muscle more [24]. In a study on female professional golfers, Kim showed that 12 weeks (3 d/w, 60 min) of core training had a positive effect on flexibility [48]. Although the sample size in Kim’s study was small, the results were similar to Kiss’s study [24, 48]. Considering that trunk prevention exercises focus more on the trunk muscles and the studies conducted are on sports where the trunk muscles are crucial, the sex and level of physical fitness of the subjects are significant. Although the exercises were different in terms of follow-up and prevention time, it is suggested to be done with different intensity, duration, and frequency in the next research.
Sports injury prevention program on female soccer players for 6 weeks (2 d/w) had no significant effect on muscle flexibility (rectus femoris, hamstring, gastrocnemius) on the left side, but it was significant on the right side. The most significant length was gastrocnemius muscle. In CG, a significant increase occurred only in the gastrocnemius muscle flexibility [25]. Lim et al. reported that an 8-week (20 min) injury prevention program in female basketball players increased flexibility [49]. The SIPP included stretching, strength, and polymetric exercises of the lower limbs, which, despite stretching exercises, is expected to have a positive effect on muscle flexibility. According to the research results, the sample size, dominant/non-dominant leg, and intensity, duration, and frequency of the program play a role in improving flexibility. It is to do this program for boys and other sports.
In a study conducted by Rahlf et al. on the effect of the 11+ program on boy soccer players in two groups (INT10, INT20) with different durations (10 min, 20 min) for 10 months (2 d/w), they stated that 11+ with a duration of 20 min had a positive effect on flexibility compared to 11+ with a time of 10 m [26]. Arede et al. reported that 11+ for 6 weeks (2 d/w) improves flexibility in boy soccer players [50]; although in the study conducted by Zarei et al., the effect was not significant [51]. FIFA 11+ comprises 15 distinct workouts, including six running exercises, three body stability exercises, two strength exercises, one jumping exercise, and three cooling-down exercises. Although 11+ excludes stretching exercises, the results showed that it has a positive effect on flexibility. According to the results of the studies, 11+ with less duration and number of sessions had less effect than 11+ with more duration, and this indicates that the duration, and frequency of the program are effective on the flexibility, which should be given more attention.
The 11+ kids program for 10 weeks (3 d/w, 20 min) on boy soccer players showed no effect on flexibility [27]. Tseng et al. stated that 11+ kids for 8 weeks (5 d/w) improves flexibility in elementary school students [52]. Anam et al. showed that 11+ kids have a significant increase in the muscle flexibility of boy soccer players in 12 weeks (2 d/w) [53]. The reason for the inconsistency in the results may be the level of activity and number of samples, the duration, and frequency of the program. Also, the 11+ Kids program does not have stretching exercises and focuses more on coordination, balance, landing technique, strengthening the leg muscles, and core stability muscles and is for children under 13 years old. Perhaps the reason for not being significant is the lack of stretching exercises in the program, although, in a meta-analysis, Alizadeh et al. showed that resistance training alone improves range of motion, this improvement was not significantly different compared to stretching training alone [54], and this means that more studies should be conducted in this field. Therefore, it is essential to pay attention to the activity level of the samples and their gender and frequency and duration program in future studies.
Conclusion
Injury prevention programs can improve the muscle flexibility of children and adolescents (significant improvement between before and after the intervention), although no improvement was observed in the control group. Therefore, factors, such as duration, frequency and intensity of the program, gender, activity level, type of sport, and sample size are decisive in muscle flexibility.
Limitations
Considering the diversity of injury prevention programs (for example, 11+ and 11+ kids, etc.) and searching with the keyword “prevention program”, using two databases for searching, it some articles may not have been used in this study. Another limitation that can be stated is that due to the variety of preventive programs in this study and the non-similarity of the programs and tests to measure flexibility, statistical analysis of the impact of the programs on flexibility was not possible. The current systematic review only includes articles in language English, which limits the language in the search strategy and the number of articles, therefore, it is suggested to use different languages in future studies.
Ethical Considerations
Compliance with ethical guidelines
There were no ethical considerations to be considered in this research.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization, study search, data collection and original draft preparation: Foad Mahmoudi; Methodology, validation, study selection, review and editing: Foad Mahmoudi and Abdolhamid Daneshjoo; Software and formal analysis: Foad Mahmoudi and Saeid Bahiraei; Risk of bias assessment and certainty assessmen: Foad Mahmoudi, Abdolhamid Daneshjoo, and Saeid Bahiraei; Supervision, Abdolhamid Daneshjoo and Mansour Sahebozamani.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors thank the authors of the articles used in this study.
References
- Emery C, Tyreman H. Sport participation, sport injury, risk factors and sport safety practices in Calgary and area junior high schools. Paediatrics & Child Health. 2009; 14(7):439-44. [DOI:10.1093/pch/14.7.439] [PMID]
- Emery CA, Meeuwisse WH, McAllister JR. Survey of sport participation and sport injury in Calgary and area high schools. Clinical Journal of Sport Medicine. 2006; 16(1):20-6. [DOI:10.1097/01.jsm.0000184638.72075.b7] [PMID]
- Caine D, Caine C, Maffulli N. Incidence and distribution of pediatric sport-related injuries. Clinical Journal of Sport Medicine. 2006; 16(6):500-13. [DOI:10.1097/01.jsm.0000251181.36582.a0] [PMID]
- Collard DC, Verhagen EA, Van Mechelen W, Heymans MW, Chinapaw MJ. Economic burden of physical activity-related injuries in Dutch children aged 10-12. British Journal of Sports Medicine. 2011; 45(13):1058-63. [DOI:10.1136/bjsm.2010.082545] [PMID]
- Ozturk S, Kilic D. What is the economic burden of sports injuries? Eklem Hastaliklari ve Cerrahisi. 2013; 24(2):108-11. [DOI:10.5606/ehc.2013.24] [PMID]
- Gore GC, Magdalinos H, Pless IB. School injuries and preventive policies and programs. Canadian Journal of Public Health. 2004; 95(6):424-8. [DOI:10.1007/BF03403986] [PMID]
- Emery CA. Risk factors for injury in child and adolescent sport: A systematic review of the literature. Clinical Journal of Sport Medicine. 2003; 13(4):256-68. [DOI:10.1097/00042752-200307000-00011] [PMID]
- Lauersen JB, Bertelsen DM, Andersen LB. The effectiveness of exercise interventions to prevent sports injuries: A systematic review and meta-analysis of randomised controlled trials. British Journal of Sports Medicine. 2014; 48(11):871-7. [DOI:10.1136/bjsports-2013-092538] [PMID]
- Pressley JC, Barlow B, Durkin M, Jacko SA, Dominguez DR, Johnson L. A national program for injury prevention in children and adolescents: The injury free coalition for kids. Journal of Urban Health. 2005; 82(3):389-402. [DOI:10.1093/jurban/jti078] [PMID]
- Steffen K, Bakka HM, Myklebust G, Bahr R. Performance aspects of an injury prevention program: a ten-week intervention in adolescent female football players. Scandinavian Journal of Medicine & Science in Sports. 2008; 18(5):596-604. [DOI:10.1111/j.1600-0838.2007.00708.x] [PMID]
- Gleim GW, McHugh MP. Flexibility and its effects on sports injury and performance. Sports Medicine. 1997; 24(5):289-99. [DOI:10.2165/00007256-199724050-00001] [PMID]
- Van Mechelen W, Twisk J, Molendijk A, Blom B, Snel J, Kemper HC. Subject-related risk factors for sports injuries: A 1-yr prospective study in young adults. Medicine & Science in Sports & Exercise. 1996; 28(9):1171-9. [DOI:10.1097/00005768-199609000-00014] [PMID]
- Jones BH, Knapik JJ. Physical training and exercise-related injuries. Surveillance, research and injury prevention in military populations. Sports Medicine. 1999; 27(2):111-25. [DOI:10.2165/00007256-199927020-00004] [PMID]
- Wilson GJ, Wood GA, Elliott BC. The relationship between stiffness of the musculature and static flexibility: An alternative explanation for the occurrence of muscular injury. International Journal of Sports Medicine. 1991; 12(4):403-7. [DOI:10.1055/s-2007-1024702] [PMID]
- Knapik JJ, Bauman CL, Jones BH, Harris JM, Vaughan L. Preseason strength and flexibility imbalances associated with athletic injuries in female collegiate athletes. The American Journal of Sports Medicine. 1991; 19(1):76-81. [DOI:10.1177/036354659101900113] [PMID]
- Cejudo A, Ginés-Díaz A, Sainz de Baranda P. Asymmetry and tightness of lower limb muscles in equestrian athletes: Are they predictors for back pain? Symmetry. 2020; 12(10):1679. [DOI:10.3390/sym12101679]
- Ruiz-Pérez I, López-Valenciano A, Hernández-Sánchez S, Puerta-Callejón JM, De Ste Croix M, Sainz de Baranda P, et al. A field-based approach to determine soft tissue injury risk in elite futsal using novel machine learning techniques. Frontiers in Psychology. 2021; 12:610210. [DOI:10.3389/fpsyg.2021.610210] [PMID]
- Cejudo A, Moreno-Alcaraz VJ, Izzo R, Santonja-Medina F, Sainz de Baranda P. External and total hip rotation ranges of motion predispose to low back pain in elite Spanish inline hockey players. International Journal of Environmental Research and Public Health. 2020; 17(13):4858. [DOI:10.3390/ijerph17134858] [PMID]
- Tak I, Engelaar L, Gouttebarge V, Barendrecht M, Van den Heuvel S, Kerkhoffs G, et al. Is lower hip range of motion a risk factor for groin pain in athletes? A systematic review with clinical applications. British Journal of Sports Medicine. 2017; 51(22):1611-21. [DOI:10.1136/bjsports-2016-096619] [PMID]
- Fousekis K, Tsepis E, Poulmedis P, Athanasopoulos S, Vagenas G. Intrinsic risk factors of non-contact quadriceps and hamstring strains in soccer: A prospective study of 100 professional players. British Journal of Sports Medicine. 2011; 45(9):709-14. [DOI:10.1136/bjsm.2010.077560] [PMID]
- Almeida GPL, de Souza VL, Sano SS, Saccol MF, Cohen M. Comparison of hip rotation range of motion in judo athletes with and without history of low back pain. Manual Therapy. 2012; 17(3):231-5. [DOI:10.1016/j.math.2012.01.004] [PMID]
- Hjelm N, Werner S, Renstrom P. Injury risk factors in junior tennis players: A prospective 2-year study. Scandinavian Journal of Medicine & Science in Sports. 2012; 22(1):40-8. [DOI:10.1111/j.1600-0838.2010.01129.x] [PMID]
- Azuma N, Someya F. Injury prevention effects of stretching exercise intervention by physical therapists in male high school soccer players. Scandinavian Journal of Medicine & Science in Sports. 2020; 30(11):2178-92. [DOI:10.1111/sms.13777] [PMID]
- Kiss G, Kovácsné VB, Tóth ÁL, Jeges S, Makai A, Szilágyi B, et al. Efficiency examination of a 6-month trunk prevention program among recruitment kayak-canoe athletes: A randomized control trial. Journal of Back and Musculoskeletal Rehabilitation. 2019; 32(3):367-78. [DOI:10.3233/BMR-181297] [PMID]
- Ortiz A, Trudelle-Jackson E, McConnell K, Wylie S. Effectiveness of a 6-week injury prevention program on kinematics and kinetic variables in adolescent female soccer players: A pilot study. Puerto Rico Health Sciences Journal. 2010; 29(1):40-8. [PMID]
- Rahlf AL, John C, Hamacher D, Zech A. Effects of a 10 vs. 20-min injury prevention program on neuromuscular and functional performance in adolescent football players. Frontiers in Physiology. 2020; 11:578866. [DOI:10.3389/fphys.2020.578866] [PMID]
- Zarei M, Namazi P, Abbasi H, Noruzyan M, Mahmoodzade S, Seifbarghi T. The effect of ten-week FIFA 11+ injury prevention program for kids on performance and fitness of adolescent soccer players. Asian Journal of Sports Medicine. 2018; 9(3):e61013. [DOI:10.5812/asjsm.61013]
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Systematic Reviews. 2021; 10(1):89. [DOI:10.1186/s13643-021-01626-4] [PMID]
- Maher CG, Sherrington C, Herbert RD, Moseley AM, Elkins M. Reliability of the PEDro scale for rating quality of randomized controlled trials. Physical Therapy. 2003; 83(8):713-21. [DOI:10.1093/ptj/83.8.713] [PMID]
- Verhagen AP, de Vet HC, de Bie RA, Kessels AG, Boers M, Bouter LM, et al. The Delphi list: A criteria list for quality assessment of randomized clinical trials for conducting systematic reviews developed by Delphi consensus. Journal of Clinical Epidemiology. 1998; 51(12):1235-41. [DOI:10.1016/S0895-4356(98)00131-0] [PMID]
- Foley NC, Teasell RW, Bhogal SK, Speechley MR. Stroke rehabilitation evidence-based review: Methodology. Topics in Stroke Rehabilitation. 2003; 10(1):1-7. [DOI:10.1310/Y6TG-1KQ9-LEDQ-64L8]
- Hemenway D, Aglipay GS, Helsing KL, Raskob GE. Injury prevention and control research and training in accredited schools of public health: A CDC/ASPH assessment. Public Health Reports. 2006; 121(3):349-51. [DOI:10.1177/003335490612100321] [PMID]
- Holt J, Holt LE, Pelham TW. Flexibility redefined. Paper presented at: ISBS-Conference Proceedings Archive; 18-22 July 1995; Ontario, Canada. [Link]
- Behm DG, Kay AD, Trajano GS, Alizadeh S, Blazevich AJ. Effects of stretching on injury risk reduction and balance. Journal of Clinical Exercise Physiology. 2021; 10(3):106-16. [DOI:10.31189/2165-6193-10.3.106]
- de la Motte SJ, Lisman P, Gribbin TC, Murphy K, Deuster PA. Systematic review of the association between physical fitness and musculoskeletal injury risk: Part 3-flexibility, power, speed, balance, and agility. The Journal of strength & Conditioning Research. 2019; 33(6):1723-35. [DOI:10.1519/JSC.0000000000002382] [PMID]
- Stojanovic MD, Ostojic SM. Stretching and injury prevention in football: Current perspectives. Research in Sports Medicine. 2011; 19(2):73-91. [DOI:10.1080/15438627.2011.556476] [PMID]
- Thacker SB, Gilchrist J, Stroup DF, Kimsey CD Jr. The impact of stretching on sports injury risk: A systematic review of the literature. Medicine & Science in Sports & Exercise. 2004; 36(3):371-8. [DOI:10.1249/01.MSS.0000117134.83018.F7] [PMID]
- Witvrouw E, Mahieu N, Danneels L, McNair P. Stretching and injury prevention: An obscure relationship. Sports Medicine. 2004; 34(7):443-9. [DOI:10.2165/00007256-200434070-00003] [PMID]
- Magnusson SP, Simonsen EB, Aagaard P, Sørensen H, Kjaer M. A mechanism for altered flexibility in human skeletal muscle. The Journal of Physiology. 1996; 497(1):291-8. [DOI:10.1113/jphysiol.1996.sp021768] [PMID]
- Klinge K, Magnusson SP, Simonsen EB, Aagaard P, Klausen K, Kjaer M. The effect of strength and flexibility training on skeletal muscle electromyographic activity, stiffness, and viscoelastic stress relaxation response. The American Journal of Sports Medicine. 1997; 25(5):710-6. [DOI:10.1177/036354659702500522] [PMID]
- Mahieu NN, McNair P, De Muynck M, Stevens V, Blanckaert I, Smits N, et al. Effect of static and ballistic stretching on the muscle-tendon tissue properties. Medicine and Science in Sports and Exercise. 2007; 39(3):494-501. [PMID]
- Coledam DHC, Arruda GAd, Oliveira AR. Chronic effect of static stretching performed during warm-up on flexibility in children. Revista Brasileira de Cineantropometria & Desempenho Humano. 2012; 14:296-304. [Link]
- Needham RA, Morse CI, Degens H. The acute effect of different warm-up protocols on anaerobic performance in elite youth soccer players. The Journal of Strength & Conditioning Research. 2009; 23(9):2614-20. [DOI:10.1519/JSC.0b013e3181b1f3ef] [PMID]
- Mayorga-Vega D, Merino-Marban R, Garrido FJ, Viciana J. Comparison between warm-up and cool-down stretching programs on hamstring extensibility gains in primary schoolchildren. Physical Activity Review. 2014; 2:16-24.
- Faigenbaum AD, Bellucci M, Bernieri A, Bakker B, Hoorens K. Acute effects of different warm-up protocols on fitness performance in children. The Journal of Strength & Conditioning Research. 2005; 19(2):376-81. [PMID]
- Pearce AJ, Kidgell DJ, Zois J, Carlson JS. Effects of secondary warm up following stretching. European Journal of Applied Physiology. 2009; 105(2):175-83. [DOI:10.1007/s00421-008-0887-3] [PMID]
- Duncan MJ, Woodfield L. Acute effects of warm up protocol on flexibility and vertical jump in children. Journal of Exercise Physiology online. 2006; 9(3):9-16. [Link]
- Kim KJ. Effects of core muscle strengthening training on flexibility, muscular strength and driver shot performance in female professional golfers. International Journal of Applied Sports Sciences. 2010; 22(1):111-27. [DOI:10.24985/ijass.2010.22.1.111]
- Lim BO, Lee YS, Kim JG, An KO, Yoo J, Kwon YH. Effects of sports injury prevention training on the biomechanical risk factors of anterior cruciate ligament injury in high school female basketball players. The American Journal of Sports Medicine. 2009; 37(9):1728-34. [DOI:10.1177/0363546509334220] [PMID]
- Arede J, Fernandes J, Moran J, Leite N, Romero-Rodriguez D, Madruga-Parera M. Effects of an integrative neuromuscular training protocol vs. FIFA 11+ on sprint, change of direction performance and inter-limb asymmetries in young soccer players. International Journal of Sports Science & Coaching. 2022; 17(1):54-62. [DOI:10.1177/17479541211011438]
- Zarei M, Abbasi H, Daneshjoo A, Barghi TS, Rommers N, Faude O, et al. Long-term effects of the 11+ warm-up injury prevention programme on physical performance in adolescent male football players: A cluster-randomised controlled trial. Journal of Sports Sciences. 2018; 36(21):2447-54. [DOI:10.1080/02640414.2018.1462001] [PMID]
- Tseng WY, Rekik G, Chen CH, Clemente FM, Bezerra P, Crowley-McHattan ZJ, et al. Effects of 8-week FIFA 11+ for Kids intervention on physical fitness and attention in elementary school children. Journal of Physical Activity and Health. 2021; 18(6):686-93. [DOI:10.1123/jpah.2020-0823] [PMID]
- Anam K, Nurrachmad L, Setiowati A, Indardi N, Irawan FA, Gulsirirat P, et al. Application of FIFA 11+ Kids: Method to minimize sports injuries in youth football. Journal Sport Area. 2022; 7(2):262-70. [DOI:10.25299/sportarea.2022.vol7(2).9467]
- Alizadeh S, Daneshjoo A, Zahiri A, Anvar SH, Goudini R, Hicks JP, et al. Resistance training induces improvements in range of motion: A systematic review and meta-analysis. Sports Medicine. 2023; 53(3):707-22. [DOI:10.1007/s40279-022-01804-x] [PMID]
Type of Study: Research |
Subject:
General
Received: 2023/09/13 | Accepted: 2023/11/24 | Published: 2024/01/1
Received: 2023/09/13 | Accepted: 2023/11/24 | Published: 2024/01/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
