Thu, Aug 6, 2026
Volume 12, Issue 4 (Autumn 2022)
PTJ 2022, 12(4): 249-260 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Yalfani A, Lotfi F, Ahmadi M, Asgarpoor A. The Effect of Sensorimotor Training on the Plantar Pressure Distribution Symmetry in Healthy Elderly: A Field Trial Study. PTJ 2022; 12 (4) :249-260
URL: http://ptj.uswr.ac.ir/article-1-556-en.html
URL: http://ptj.uswr.ac.ir/article-1-556-en.html



1- Department of Sports injuries and corrective exercise, Faculty of Physical Education and Sport Sciences, Bu-Ali Sina University, Hamadan, Iran.
Full-Text [PDF 1213 kb]
(1268 Downloads)
| Abstract (HTML) (3439 Views)
Sample size
The G*power software was used to determine the sample size. After entering the software environment, F test option (ANCOVA: Fixed effects, main effect, and interactions) was selected from the test family section. The numerical values applied in the software environment included α=0.05, power=95, and effect size=80. The output of the software reported a total of 32 people (16 people in each group). However, to increase the statistical power and the probability of a 30% dropout, a total of 40 people (20 people in each group) were considered.
Study participants
The statistical population of the current study was healthy elderly women (age (year): 68.05±4.81, height (cm): 156.05±5.02, weight (kg): 72.52±9.18, body mass index (BMI): 30.73±3.11) who were selected from Hamedan province. The inclusion criteria included the right dominant leg, the normal posture of the upper and lower limbs, non-participation in sports activities, no history of surgery, no musculoskeletal pain in the past year, normal vision, and no specific diseases. The exclusion criteria included upper and lower limb deformity, participation in sports activities regularly or recreationally, poor eyesight, history of surgery or fracture, musculoskeletal pain, and left dominant leg. Finally, the subjects were randomly assigned to two groups of experimental and control using the random allocation software and allocation concealment using the Sequentially Numbered, Opaque, Sealed Envelope (SNOSE) method.
Study tool
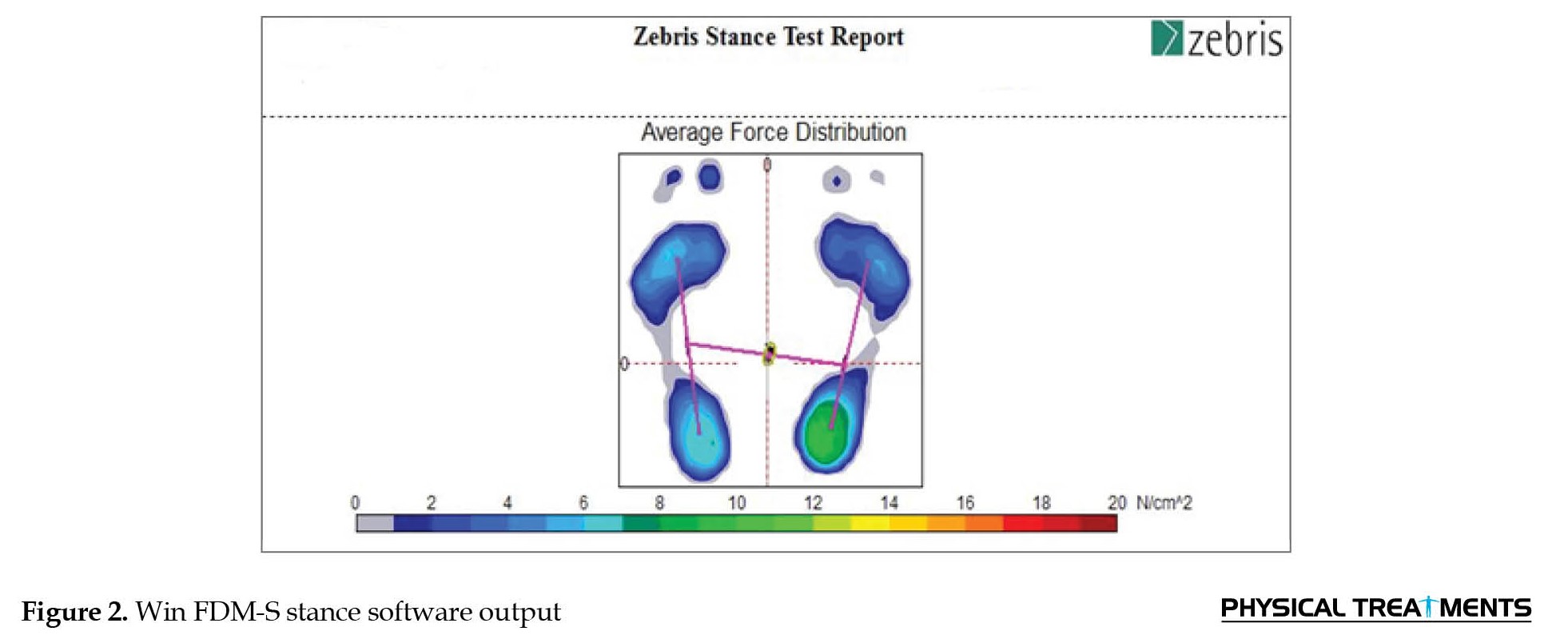
The FDM-S plantar pressures device manufactured by Zebris company of Germany was used to record the plantar pressure distribution (intraclass correlation coefficient [ICC]=0.91). This device has a platform with dimensions of 54x34 cm and 2560 active sensors with high sensitivity (1 sensor per square centimeter) and a sampling rate of 50 Hz and an error level of 5%, which records the pressure in the range of 1 to 120 N. Data analysis related to pressure distribution variables was calculated by Win FDM-S software, version 01.02.09 in the static condition and model of double-legs (Figure 2).

Full-Text: (1556 Views)
1. Introduction
Over the past 50 years, the population of people aged 60 and higher had increased by 2 % [1]. Researchers estimated that this amount will reach 22% by 2050 [1]. For example, according to Brazilian national epidemiological data in 2010, about 20.5 million elderly people live in this country [2]. It is predicted that this number will reach 64 million people in 2025. At this point, Brazil will be the sixth country with the highest number of elderly people in the world [2]. The biological processes of the elderly are associated with changes in the sensorimotor system [3]. Sensorimotor impairment related to the elderly can lead to increased postural sway, fall risk, hospitalizations, and mortality [4]. In addition, the elderly leads to physical changes, such as foot posture, reduced foot muscle strength and joint flexibility, and reduced plantar sensation [5]. As a result, due to the rapid increase in the elderly population and the high medical costs, preventive care for the elderly has received more attention [6].
The touch sense decreases during the elderly process [7]. Decreased plantar touch sense can change the plantar loading patterns [8]. Plantar mechanical receptors are vital in maintaining and restoring balance during standing. The main sensorimotor factor that helps balance in normal conditions is the lower limb sense [9]. Due to sensorimotor impairment associated with the elderly, the feedback of touch mechanical receptors of the plantar decreases and leads to increased postural sway [5]. In this regard, the studies conducted on center of pressure oscillation reported the imbalance of the elderly in the anterior-posterior and medial-lateral directions. Increased postural sway leads to asymmetric loading of the lower limbs. Plantar pressure technology determines the amount and location of ground reaction forces in different parts of the plantar and is used to infer the strategy of the foot movement chain during motion [10]. This technique is a crucial approach because changes in plantar pressure are related to changes in applied forces on proximal joints, such as the knee.
According to the study's results, elderly people show significant changes in plantar pressure distribution compared to young people [5]. For example, Machado et al. (2016) reported that the elderly compared to the young restore balance, transfer pressure to the forward of the foot, and an asymmetric pressure is observed in different parts of the plantar [11]. In this regard, Hilton (2006) reported that plantar pressure distribution asymmetric can lead to pathological foot conditions, including forefoot pain, neuropathic plantar ulcers, and metatarsal stress fractures [12]. These pathological conditions are associated with a decrease in physical activity, an increase in posture sway, and the risk of falling [13]. The symmetry of human movement is often considered as the matching of the action of lower limbs [14]. Evaluation of the plantar pressure distribution symmetry provides useful information to prevent body imbalance and is used to evaluate the progress of the rehabilitation program [14, 15]. Despite the above, limited information exists about plantar pressure distribution symmetry in the elderly population [11]; and the effect of rehabilitation protocols on the plantar pressure distribution symmetry has not been well analyzed. The foot and ankle joints include several joints mechanisms and are one of the key aspects of human movement [16]. Therefore, attention to plantar sensation and pressure in elderly people provides crucial clinical information [11]. As a result, knowing the effects of the elderly on foot and ankle biomechanics is vital for health professionals and researchers [16].
Sensorimotor training is a special form of proprioception and balance training [17]. These trainings are designed for pain management in patients with chronic musculoskeletal pain syndrome, correction of muscle imbalance, and correct movement program at the level of the central nervous system. These trainings through adaptation of the neuromuscular system lead to the improvement of proprioception, muscle coordination, balance, and reduction of postural sway [18]. In other words, sensorimotor training is defined with the priority of improving the function of the central nervous system through sensory awareness, coordination, quality of motor control, and motor reprogramming [17]. Previous research has provided evidence that increasing skin information can reduce postural sway and improve postural stability [4]. For example, Azarpaykan (2018) reported in a study that sensorimotor training improves postural stability in healthy elderly [19]. However, the effect of this approach on the plantar pressure distribution symmetry has not been investigated. Therefore, the present study aims to examine the effect of sensorimotor training on the plantar pressure distribution symmetry in healthy elderly.
2. Materials and Methods
Ethical considerations
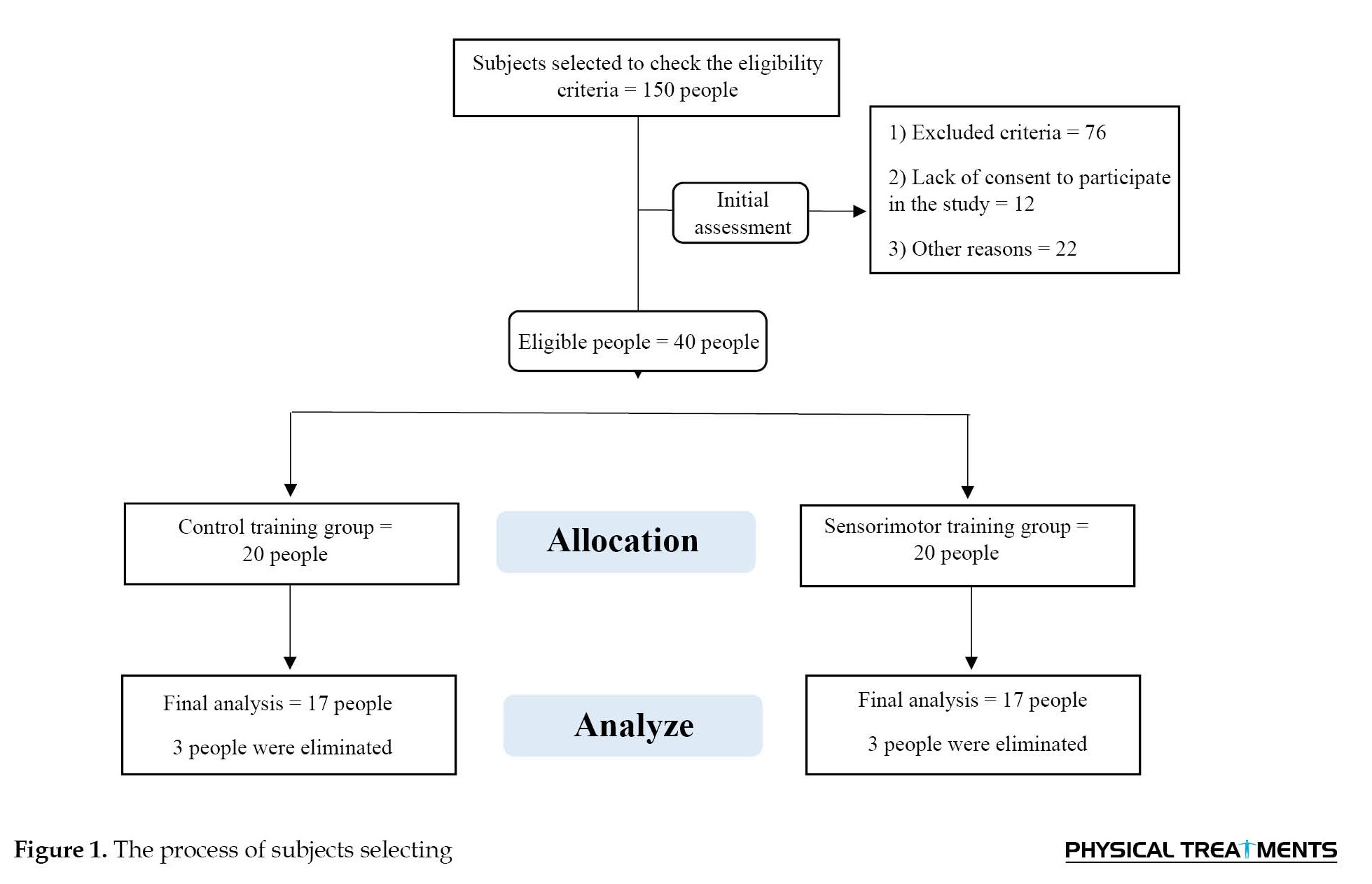
Before login into the laboratory, all participants were informed about the purpose and tests of the research and declared their informed consent by the Declaration of Helsinki. This research had been approved by the Research Ethics Committee of Bu-Ali Sina (Code: IR.BASU.REC.1401.027). Figure 1 shows the subject’s selection process. IR.BASU.REC.1401.027 Universit
Over the past 50 years, the population of people aged 60 and higher had increased by 2 % [1]. Researchers estimated that this amount will reach 22% by 2050 [1]. For example, according to Brazilian national epidemiological data in 2010, about 20.5 million elderly people live in this country [2]. It is predicted that this number will reach 64 million people in 2025. At this point, Brazil will be the sixth country with the highest number of elderly people in the world [2]. The biological processes of the elderly are associated with changes in the sensorimotor system [3]. Sensorimotor impairment related to the elderly can lead to increased postural sway, fall risk, hospitalizations, and mortality [4]. In addition, the elderly leads to physical changes, such as foot posture, reduced foot muscle strength and joint flexibility, and reduced plantar sensation [5]. As a result, due to the rapid increase in the elderly population and the high medical costs, preventive care for the elderly has received more attention [6].
The touch sense decreases during the elderly process [7]. Decreased plantar touch sense can change the plantar loading patterns [8]. Plantar mechanical receptors are vital in maintaining and restoring balance during standing. The main sensorimotor factor that helps balance in normal conditions is the lower limb sense [9]. Due to sensorimotor impairment associated with the elderly, the feedback of touch mechanical receptors of the plantar decreases and leads to increased postural sway [5]. In this regard, the studies conducted on center of pressure oscillation reported the imbalance of the elderly in the anterior-posterior and medial-lateral directions. Increased postural sway leads to asymmetric loading of the lower limbs. Plantar pressure technology determines the amount and location of ground reaction forces in different parts of the plantar and is used to infer the strategy of the foot movement chain during motion [10]. This technique is a crucial approach because changes in plantar pressure are related to changes in applied forces on proximal joints, such as the knee.
According to the study's results, elderly people show significant changes in plantar pressure distribution compared to young people [5]. For example, Machado et al. (2016) reported that the elderly compared to the young restore balance, transfer pressure to the forward of the foot, and an asymmetric pressure is observed in different parts of the plantar [11]. In this regard, Hilton (2006) reported that plantar pressure distribution asymmetric can lead to pathological foot conditions, including forefoot pain, neuropathic plantar ulcers, and metatarsal stress fractures [12]. These pathological conditions are associated with a decrease in physical activity, an increase in posture sway, and the risk of falling [13]. The symmetry of human movement is often considered as the matching of the action of lower limbs [14]. Evaluation of the plantar pressure distribution symmetry provides useful information to prevent body imbalance and is used to evaluate the progress of the rehabilitation program [14, 15]. Despite the above, limited information exists about plantar pressure distribution symmetry in the elderly population [11]; and the effect of rehabilitation protocols on the plantar pressure distribution symmetry has not been well analyzed. The foot and ankle joints include several joints mechanisms and are one of the key aspects of human movement [16]. Therefore, attention to plantar sensation and pressure in elderly people provides crucial clinical information [11]. As a result, knowing the effects of the elderly on foot and ankle biomechanics is vital for health professionals and researchers [16].
Sensorimotor training is a special form of proprioception and balance training [17]. These trainings are designed for pain management in patients with chronic musculoskeletal pain syndrome, correction of muscle imbalance, and correct movement program at the level of the central nervous system. These trainings through adaptation of the neuromuscular system lead to the improvement of proprioception, muscle coordination, balance, and reduction of postural sway [18]. In other words, sensorimotor training is defined with the priority of improving the function of the central nervous system through sensory awareness, coordination, quality of motor control, and motor reprogramming [17]. Previous research has provided evidence that increasing skin information can reduce postural sway and improve postural stability [4]. For example, Azarpaykan (2018) reported in a study that sensorimotor training improves postural stability in healthy elderly [19]. However, the effect of this approach on the plantar pressure distribution symmetry has not been investigated. Therefore, the present study aims to examine the effect of sensorimotor training on the plantar pressure distribution symmetry in healthy elderly.
2. Materials and Methods
Ethical considerations
Before login into the laboratory, all participants were informed about the purpose and tests of the research and declared their informed consent by the Declaration of Helsinki. This research had been approved by the Research Ethics Committee of Bu-Ali Sina (Code: IR.BASU.REC.1401.027). Figure 1 shows the subject’s selection process. IR.BASU.REC.1401.027 Universit
Sample size
The G*power software was used to determine the sample size. After entering the software environment, F test option (ANCOVA: Fixed effects, main effect, and interactions) was selected from the test family section. The numerical values applied in the software environment included α=0.05, power=95, and effect size=80. The output of the software reported a total of 32 people (16 people in each group). However, to increase the statistical power and the probability of a 30% dropout, a total of 40 people (20 people in each group) were considered.
Study participants
The statistical population of the current study was healthy elderly women (age (year): 68.05±4.81, height (cm): 156.05±5.02, weight (kg): 72.52±9.18, body mass index (BMI): 30.73±3.11) who were selected from Hamedan province. The inclusion criteria included the right dominant leg, the normal posture of the upper and lower limbs, non-participation in sports activities, no history of surgery, no musculoskeletal pain in the past year, normal vision, and no specific diseases. The exclusion criteria included upper and lower limb deformity, participation in sports activities regularly or recreationally, poor eyesight, history of surgery or fracture, musculoskeletal pain, and left dominant leg. Finally, the subjects were randomly assigned to two groups of experimental and control using the random allocation software and allocation concealment using the Sequentially Numbered, Opaque, Sealed Envelope (SNOSE) method.
Study tool
The FDM-S plantar pressures device manufactured by Zebris company of Germany was used to record the plantar pressure distribution (intraclass correlation coefficient [ICC]=0.91). This device has a platform with dimensions of 54x34 cm and 2560 active sensors with high sensitivity (1 sensor per square centimeter) and a sampling rate of 50 Hz and an error level of 5%, which records the pressure in the range of 1 to 120 N. Data analysis related to pressure distribution variables was calculated by Win FDM-S software, version 01.02.09 in the static condition and model of double-legs (Figure 2).
This software reported the data related to the peak plantar pressure in the forward, and backward foot and the total pressure of each foot.
Study assessment
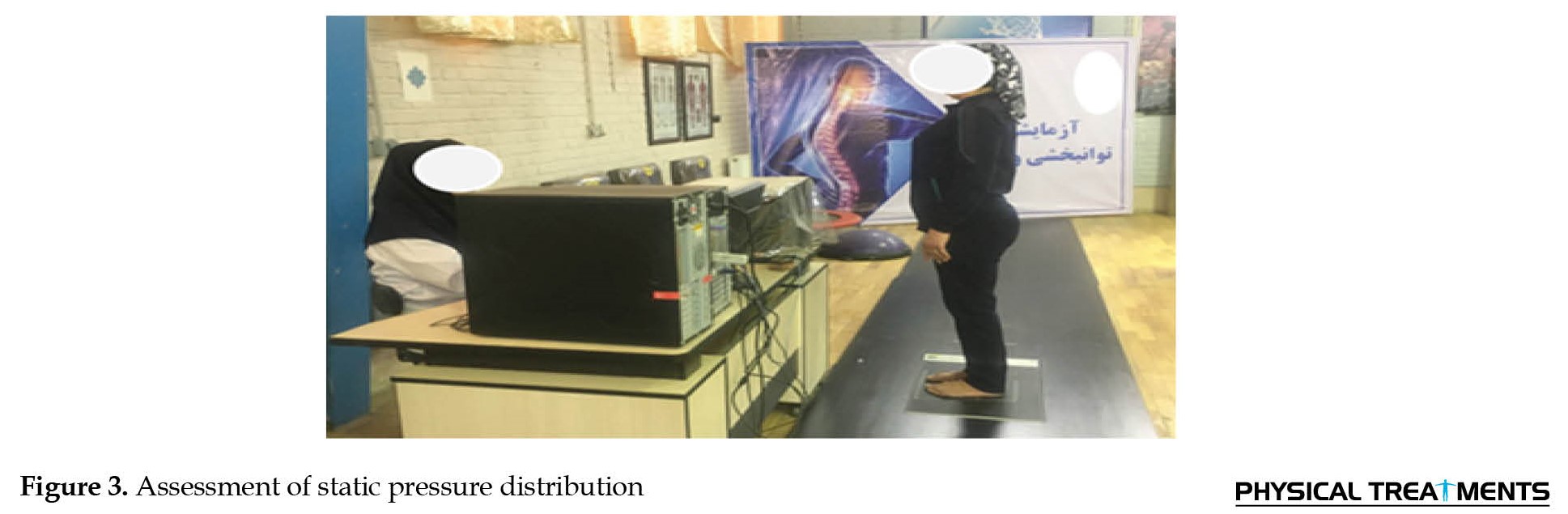
With the guidance of the evaluator, the subjects stand with bare feet upon part marked on the platform with eyes closed. The ankle and foot were in a neutral position and both arms resting by the trunk sides. Before starting the evaluation, to prevent disturbances in the vestibular system and head movements, the subjects were taught to look at a marker with a diameter of 10 cm, which was located on the wall at a distance of 2 m from the subject, and to maintain this position from the time closing the eyes until the end of the evaluation. The evaluation was executed 3 times with a time of 30 s, and the rest time between each test was set at 2 minutes (Figure 3) [17].
Study assessment
With the guidance of the evaluator, the subjects stand with bare feet upon part marked on the platform with eyes closed. The ankle and foot were in a neutral position and both arms resting by the trunk sides. Before starting the evaluation, to prevent disturbances in the vestibular system and head movements, the subjects were taught to look at a marker with a diameter of 10 cm, which was located on the wall at a distance of 2 m from the subject, and to maintain this position from the time closing the eyes until the end of the evaluation. The evaluation was executed 3 times with a time of 30 s, and the rest time between each test was set at 2 minutes (Figure 3) [17].
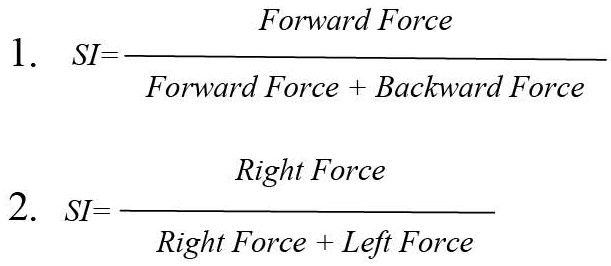
The average of 3 tests was recorded for the final analysis. Equation 1 was used to calculate the plantar pressure Symmetry Index (SI) of the forward-backward of foot and Equation 2 was used for SI between the right and left of the foot [17]. Also, the normal pressure distribution in each foot is determined to be 50% [17]. All assessment procedures were performed by an expert in the rehabilitation laboratory of Bu-Ali Sina University (Equation 1 and 2).
Sensorimotor training
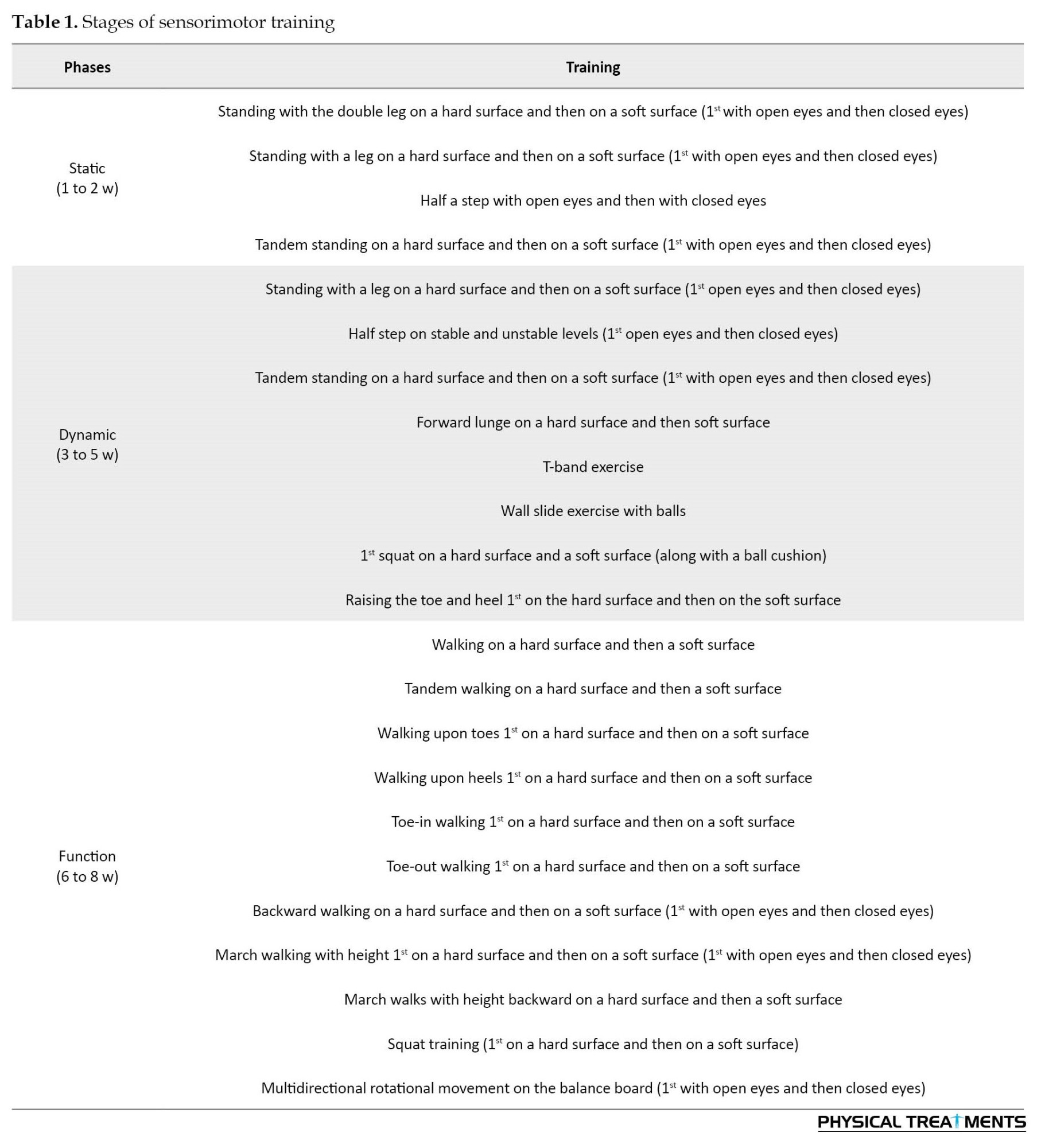
Sensorimotor training in the present study was performed based on previous studies [17, 20, 21] (nerve function, and muscle activation in Diabetic Peripheral Neuropathy (DPN). The training was performed for eight weeks, three sessions a week, and each session lasted for one hour. The training was performed in three stages, static, dynamic, and functional. The first static stage is that the practice of controlling the center of gravity on the support surface during maintaining postures is related to static or balance activities. This stage develops tonic function or simultaneous activation and stability of the axial skeleton, which includes correction of body position, sensory stimulation, and progressive challenges for the support surface and center of gravity. The dynamic stage through limb movements focuses on the body core. In this stage, the preliminary and reactive muscle contractions can be achieved, as well as the order and sequence of muscle activation, which is mainly achieved through training on unstable surfaces. The purpose of the functional stage is to automate synergies more complex involving multiple joints, muscles, and movement surfaces that require movement in space (Figure 4) [17, 22].
Sensorimotor training
Sensorimotor training in the present study was performed based on previous studies [17, 20, 21] (nerve function, and muscle activation in Diabetic Peripheral Neuropathy (DPN). The training was performed for eight weeks, three sessions a week, and each session lasted for one hour. The training was performed in three stages, static, dynamic, and functional. The first static stage is that the practice of controlling the center of gravity on the support surface during maintaining postures is related to static or balance activities. This stage develops tonic function or simultaneous activation and stability of the axial skeleton, which includes correction of body position, sensory stimulation, and progressive challenges for the support surface and center of gravity. The dynamic stage through limb movements focuses on the body core. In this stage, the preliminary and reactive muscle contractions can be achieved, as well as the order and sequence of muscle activation, which is mainly achieved through training on unstable surfaces. The purpose of the functional stage is to automate synergies more complex involving multiple joints, muscles, and movement surfaces that require movement in space (Figure 4) [17, 22].
Table 1 presents sensorimotor training.
Statistical analysis
All statistical analyzes were performed using SPSS software, version 26. The Shapiro-Wilk test was used to check the normal distribution of the data. Also, Levine’s test was used to check the homogeneity of the variance. Then, the ANCOVA test was used with the pre-test as a covariate to compare the results between the two groups. The Cohen’s index was used to check the effect size, (0.01 to 0.059 small effect size, 0.06 to 0.14 medium effect size, and more than 0.14 large effect size) [23].
3. Results
In Table 2, the results of the Shapiro-Wilk test showed that the data distribution is normal (P>0.05).

Also, the result of Levin’s test showed that the variances are homogeneous (P>0.05). As a result, ANCOVA parametric test was used to compare the results between the two groups. Three people from the experimental group were excluded from the research process due to their absence from the training sessions. Also, 3 people from the control group were excluded from the research process due to not being present in the laboratory. Finally, the statistical data of 34 subjects (17 people in each group) were used for statistical analysis (Figure 1).
Plantar pressure distribution symmetry
The results of the analysis of covariance (ANCOVA) show that after controlling the pre-test effect (η2=0.471, P=0.000, F(1, 31)=27.549) the main effect of the group (η2=0.466, P=0.000, F(1, 31)=0.181) with a high effect size had a significant effect on the plantar pressure distribution symmetry of the forward and backward in the right foot (Tables 3 and 4).

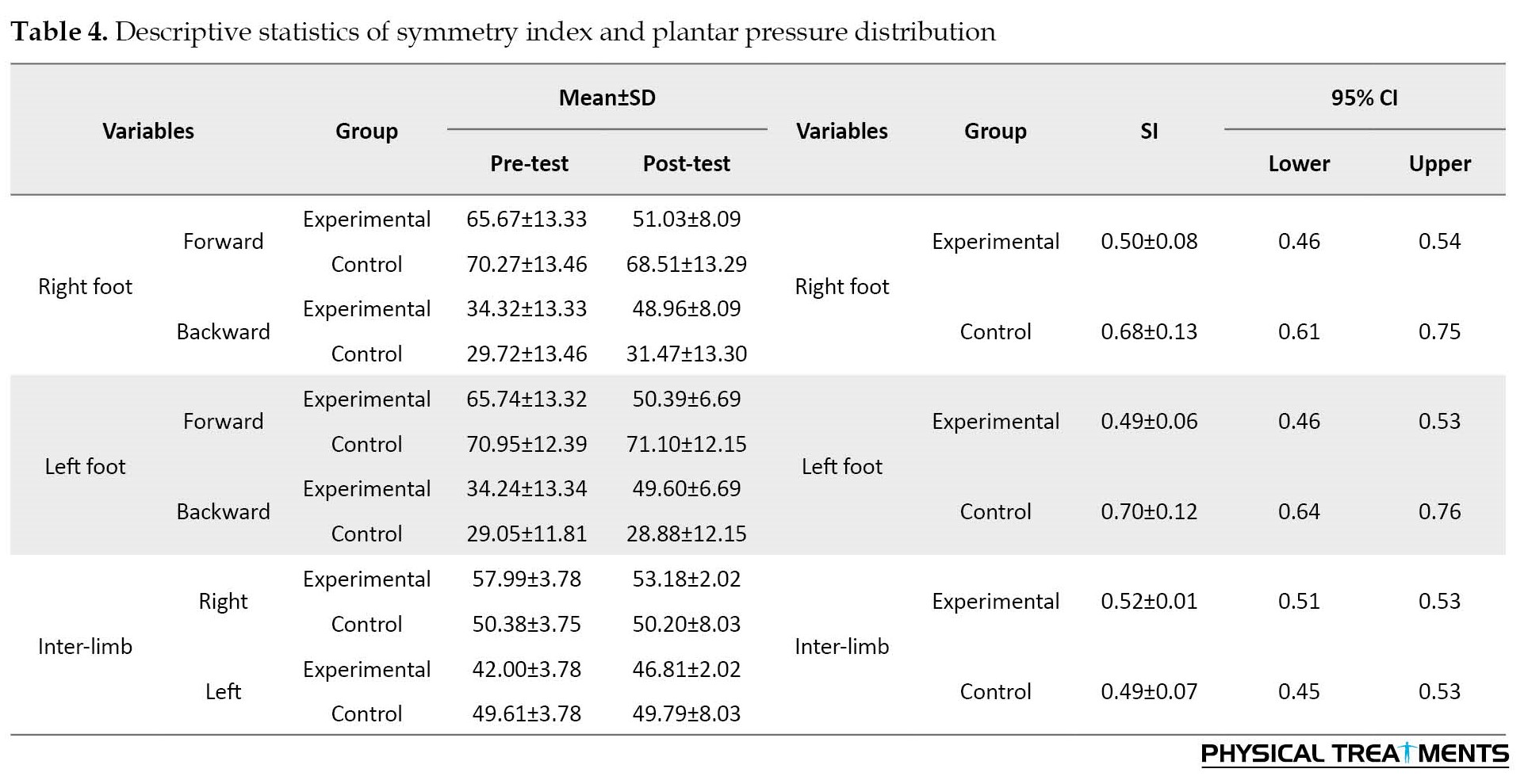
In addition, the results of the analysis of covariance (ANCOVA) show that after controlling the effect of the pre-test (η2=0.397, P=0.000, F(1, 31)=20.398), the main effect of the group (η2=0.589, P=0.000, F(1, 31)=44.430) with a high effect size had a significant effect on the plantar pressure distribution symmetry of the forward and backward in the left foot (Tables 3 and 4).
Also, after controlling the pre-test effect (η2=0.541, P=0.000, F(1, 31)=36.562), the main effect of group (η2=0.177, P=0.015, F(1, 31)=6.645) with high effect size had a significant effect on the plantar pressure distribution symmetry of the right and left foot (Tables 3 and 4).
4. Discussion
This study was conducted to examine the effect of sensorimotor training on the plantar pressure distribution symmetry in healthy elderly. The results showed that sensorimotor training develops a loading pattern symmetrical in the forward-backward of the foot and between the right-left feet. In the following part, the mechanism of training on the plantar pressure distribution symmetry is described.
The results of Equation 1 analysis showed that the plantar pressure distribution of the elderly had increased in the forward of the foot, which is consistent with the results of the study by Machado et al. (2016) [11]. Two strategies of hip and ankle are used to control posture. However, the elderly rely more on the hip strategy compared to young people due to biomechanical and sensorimotor impairment in the ankle [24]. The pressure distribution asymmetrical in the elderly may be explained by the effects of the elderly on the mechanical properties of the ankle and foot [25]. The plantar flexors muscles act to prevent from moving the center of mass to a forward direction [9]. During standing, the plantar muscles, especially the soleus muscle, are activated at low levels to control the ankle torque and limit the anterior-posterior oscillations of the center of pressure and the center of mass around the support surface center [26] 5 women, 6 men. In this regard, Don et al. (2006) reported a 25-ms response delay of the soleus muscle in elderly subjects, which could be due to a decrease in type II fast-twitch fibers due to elderly [27]. In addition, the impairment of peripheral sensation and afferents and efferents leads to a prolonged delay in muscle response [27]. Delayed muscle responses in the elderly may be due to impaired central processing associated with cortical and subcortical integration to coordinate visual, vestibular, and sensory inputs [27]. Therefore, impairment in the plantar flexor can lead to postural instability and increase the fall risk in the anterior-posterior direction and cause pathological conditions, such as wrist fracture [28]. As a result, since the anterior-posterior oscillations are controlled and corrected by the ankle strategy, the impairment of this strategy increases the anterior-posterior oscillations; as a result, loads are applied to the forward of the foot [18, 28]. In addition, higher pressure values in healthy elderly may be due to changes in elastic tissue properties during the elderly process that may affect the stiffness of the fat pad and lead to asymmetric pressure [29]. Therefore, increased loading in the middle and forward of the foot may be due to decreased plantar sensation in the backward of the foot [5].
Yalfani et al. reported that sensorimotor training plays several roles in motor responses by facilitating afferents sent from sensory receptors, including reflex responses, voluntary programmed responses, coordination and integration of feedforward and feedback mechanisms [17]. A consensus in scientific evidence shows that plantar sensory change affects plantar pressure distribution [5]. Stimulation of plantar receptors can improve the sensorimotor system [19]. In sensorimotor training, the stimulation of joint afferent impulses is increased and balance strategies provide more accurate information about the postural sway velocity [17, 30]. Therefore, the strengthening of these receptors transmits a more accurate feedback of the acceleration and posture sway velocity to the brain and leads to the recovery of postural stability [31]. On the other hand, the stretching reflex improves with the increase of sensory impulses. This reflex is the first mechanism to activate the muscles around a joint following the applied external torque [17]. Often, ankle rotation is the most important stretching reflex and the key reaction in the leg muscles, caused by postural instability. It seems that stimulating the plantar mechanical receptors which have reflex connections with the muscles around the ankle, causes reflex contraction in the leg muscles and leads to posture stability [17, 23]. Therefore, providing more sensory feedback on motor efferent improves the reactive ability of muscle activation and responds to external forces faster, leading to joint dynamic stability [18].
The results of Equation 2 analysis showed that the plantar pressure distribution in the elderly is one-sided and is more in the dominant leg. The one-sided pressure distribution is due to posture instability; because static posture control requires the integration of the sensorimotor system. In this regard, Jason et al. reported hip proprioception impairment in elderly people. The hip proprioception impairment may negatively affect postural stability and lead to increased fall risk in the elderly [28]. The hip strategies are primarily responsible for controlling medial-lateral oscillations. The medial-lateral stability during balance reactions predicts the fall risk in the future, and most hip fractures are associated with falls in medial-lateral directions [28]. Due to the biomechanical advantage of the hip abductor muscles, which is the largest hip abductor muscle and had 60% of the cross-sectional area, it has contributed more to maintaining medial-lateral stability [32]. A delay in activation or decrease in strength in this muscle increases the movements of the hip and pelvis in the frontal plane and makes the plantar pressure distribution asymmetric in the inter-limb [17, 33]. In this regard, Breuer et al. reported delayed activation of the gluteus medius muscle in the elderly [34]. In addition to the above, Nolan et al. reported in a study that most elderly people use the dominant legs during standing [35]. This mechanism causes the loading pattern asymmetric of the inter-limb in the movement chain. In other words, this behavior leads to the loading/unloading mechanism. It seems that this mechanism causes an increase in the loading rate on the dominant leg and over time leads to joint cartilage destruction and osteoarthritis [17, 23, 36–38]. In this regard, previous studies reported a relationship between increased plantar pressure, stance time, and cautious movement pattern with the occurrence of osteoarthritis [29, 39].
It seems that the correction of the pressure distribution asymmetry of the inter-limb can be due to facilitating the activity of the hip abductor muscle. Rehabilitation interventions focusing on the sensorimotor approach, including training in different positions and functional movements, are crucial [17]. Progressing from the static phase to the dynamic and functional phase improves muscle contraction reaction, order and synergistic contraction [17, 22]. Sensorimotor training focuses on the sequence, and order of proper muscle activation. This training approach enables the sensorimotor system to develop unconscious movement programs to stabilize the movement chain during functional activities [17, 18, 22]. As a result, to improve proper recruitment and muscle activation, training aimed at complex movements, including synergies involving several joints, muscles, and planes of motion was used [22]. Therefore, increasing the sensory input about joint position and length changing and tension muscles in the central nervous system improves the ability of the nervous system to create a pattern of rapid recruitment and optimal use of muscles, increase the number of active motor units and increase muscle coordination. Consequently, reflex stabilization responses of the joint can be improved by activities that focus on sudden changes in joint position and stimulate the reflex neuromuscular control [17, 18, 22].
Limitations
Limitations exist in this study, including the low sample size and lack of high participation due to the COVID-19 pandemic, the lack of evaluation of the plantar pressure distribution symmetry during challenging daily activities, the lack of evaluation of other kinematic and kinetic variables during dynamic activities, and the sample size of the present study is only the elderly female population. As a result, it is recommended that researchers evaluate the plantar pressure distribution symmetry during daily challenging activities in future studies with a large sample size in the population of men and women.
5. Conclusion
The results of the present study showed that sensorimotor training improves balance strategies and sensorimotor coordination by improving neuromuscular coordination, and subsequently decreasing postural sway. As a result, by reducing the postural sway and improving the transmission of afferent information from mechanical receptors, and adjusting the balance strategies, the pressure distribution in different areas of the plantar is balanced.
Ethical Considerations
Compliance with ethical guidelines
This project was approved and registered at the National Committee for Ethics in Biomedical Research of Bu-Ali Sina (Code: IR.BASU.REC.1401.027).
Funding
The present paper was extracted from the MA. thesis ofFatemeh Lotfi at the Department of Corrective Exercises and Sports Injury, Faculty of Physical Education and Sport Sciences, Bu-Ali Sina University, Hamedan.
Authors' contributions
All authors contributed in preparing this article.
Conflict of interest
The authors declared no conflict of interest.
References
Statistical analysis
All statistical analyzes were performed using SPSS software, version 26. The Shapiro-Wilk test was used to check the normal distribution of the data. Also, Levine’s test was used to check the homogeneity of the variance. Then, the ANCOVA test was used with the pre-test as a covariate to compare the results between the two groups. The Cohen’s index was used to check the effect size, (0.01 to 0.059 small effect size, 0.06 to 0.14 medium effect size, and more than 0.14 large effect size) [23].
3. Results
In Table 2, the results of the Shapiro-Wilk test showed that the data distribution is normal (P>0.05).
Also, the result of Levin’s test showed that the variances are homogeneous (P>0.05). As a result, ANCOVA parametric test was used to compare the results between the two groups. Three people from the experimental group were excluded from the research process due to their absence from the training sessions. Also, 3 people from the control group were excluded from the research process due to not being present in the laboratory. Finally, the statistical data of 34 subjects (17 people in each group) were used for statistical analysis (Figure 1).
Plantar pressure distribution symmetry
The results of the analysis of covariance (ANCOVA) show that after controlling the pre-test effect (η2=0.471, P=0.000, F(1, 31)=27.549) the main effect of the group (η2=0.466, P=0.000, F(1, 31)=0.181) with a high effect size had a significant effect on the plantar pressure distribution symmetry of the forward and backward in the right foot (Tables 3 and 4).
In addition, the results of the analysis of covariance (ANCOVA) show that after controlling the effect of the pre-test (η2=0.397, P=0.000, F(1, 31)=20.398), the main effect of the group (η2=0.589, P=0.000, F(1, 31)=44.430) with a high effect size had a significant effect on the plantar pressure distribution symmetry of the forward and backward in the left foot (Tables 3 and 4).
Also, after controlling the pre-test effect (η2=0.541, P=0.000, F(1, 31)=36.562), the main effect of group (η2=0.177, P=0.015, F(1, 31)=6.645) with high effect size had a significant effect on the plantar pressure distribution symmetry of the right and left foot (Tables 3 and 4).
4. Discussion
This study was conducted to examine the effect of sensorimotor training on the plantar pressure distribution symmetry in healthy elderly. The results showed that sensorimotor training develops a loading pattern symmetrical in the forward-backward of the foot and between the right-left feet. In the following part, the mechanism of training on the plantar pressure distribution symmetry is described.
The results of Equation 1 analysis showed that the plantar pressure distribution of the elderly had increased in the forward of the foot, which is consistent with the results of the study by Machado et al. (2016) [11]. Two strategies of hip and ankle are used to control posture. However, the elderly rely more on the hip strategy compared to young people due to biomechanical and sensorimotor impairment in the ankle [24]. The pressure distribution asymmetrical in the elderly may be explained by the effects of the elderly on the mechanical properties of the ankle and foot [25]. The plantar flexors muscles act to prevent from moving the center of mass to a forward direction [9]. During standing, the plantar muscles, especially the soleus muscle, are activated at low levels to control the ankle torque and limit the anterior-posterior oscillations of the center of pressure and the center of mass around the support surface center [26] 5 women, 6 men. In this regard, Don et al. (2006) reported a 25-ms response delay of the soleus muscle in elderly subjects, which could be due to a decrease in type II fast-twitch fibers due to elderly [27]. In addition, the impairment of peripheral sensation and afferents and efferents leads to a prolonged delay in muscle response [27]. Delayed muscle responses in the elderly may be due to impaired central processing associated with cortical and subcortical integration to coordinate visual, vestibular, and sensory inputs [27]. Therefore, impairment in the plantar flexor can lead to postural instability and increase the fall risk in the anterior-posterior direction and cause pathological conditions, such as wrist fracture [28]. As a result, since the anterior-posterior oscillations are controlled and corrected by the ankle strategy, the impairment of this strategy increases the anterior-posterior oscillations; as a result, loads are applied to the forward of the foot [18, 28]. In addition, higher pressure values in healthy elderly may be due to changes in elastic tissue properties during the elderly process that may affect the stiffness of the fat pad and lead to asymmetric pressure [29]. Therefore, increased loading in the middle and forward of the foot may be due to decreased plantar sensation in the backward of the foot [5].
Yalfani et al. reported that sensorimotor training plays several roles in motor responses by facilitating afferents sent from sensory receptors, including reflex responses, voluntary programmed responses, coordination and integration of feedforward and feedback mechanisms [17]. A consensus in scientific evidence shows that plantar sensory change affects plantar pressure distribution [5]. Stimulation of plantar receptors can improve the sensorimotor system [19]. In sensorimotor training, the stimulation of joint afferent impulses is increased and balance strategies provide more accurate information about the postural sway velocity [17, 30]. Therefore, the strengthening of these receptors transmits a more accurate feedback of the acceleration and posture sway velocity to the brain and leads to the recovery of postural stability [31]. On the other hand, the stretching reflex improves with the increase of sensory impulses. This reflex is the first mechanism to activate the muscles around a joint following the applied external torque [17]. Often, ankle rotation is the most important stretching reflex and the key reaction in the leg muscles, caused by postural instability. It seems that stimulating the plantar mechanical receptors which have reflex connections with the muscles around the ankle, causes reflex contraction in the leg muscles and leads to posture stability [17, 23]. Therefore, providing more sensory feedback on motor efferent improves the reactive ability of muscle activation and responds to external forces faster, leading to joint dynamic stability [18].
The results of Equation 2 analysis showed that the plantar pressure distribution in the elderly is one-sided and is more in the dominant leg. The one-sided pressure distribution is due to posture instability; because static posture control requires the integration of the sensorimotor system. In this regard, Jason et al. reported hip proprioception impairment in elderly people. The hip proprioception impairment may negatively affect postural stability and lead to increased fall risk in the elderly [28]. The hip strategies are primarily responsible for controlling medial-lateral oscillations. The medial-lateral stability during balance reactions predicts the fall risk in the future, and most hip fractures are associated with falls in medial-lateral directions [28]. Due to the biomechanical advantage of the hip abductor muscles, which is the largest hip abductor muscle and had 60% of the cross-sectional area, it has contributed more to maintaining medial-lateral stability [32]. A delay in activation or decrease in strength in this muscle increases the movements of the hip and pelvis in the frontal plane and makes the plantar pressure distribution asymmetric in the inter-limb [17, 33]. In this regard, Breuer et al. reported delayed activation of the gluteus medius muscle in the elderly [34]. In addition to the above, Nolan et al. reported in a study that most elderly people use the dominant legs during standing [35]. This mechanism causes the loading pattern asymmetric of the inter-limb in the movement chain. In other words, this behavior leads to the loading/unloading mechanism. It seems that this mechanism causes an increase in the loading rate on the dominant leg and over time leads to joint cartilage destruction and osteoarthritis [17, 23, 36–38]. In this regard, previous studies reported a relationship between increased plantar pressure, stance time, and cautious movement pattern with the occurrence of osteoarthritis [29, 39].
It seems that the correction of the pressure distribution asymmetry of the inter-limb can be due to facilitating the activity of the hip abductor muscle. Rehabilitation interventions focusing on the sensorimotor approach, including training in different positions and functional movements, are crucial [17]. Progressing from the static phase to the dynamic and functional phase improves muscle contraction reaction, order and synergistic contraction [17, 22]. Sensorimotor training focuses on the sequence, and order of proper muscle activation. This training approach enables the sensorimotor system to develop unconscious movement programs to stabilize the movement chain during functional activities [17, 18, 22]. As a result, to improve proper recruitment and muscle activation, training aimed at complex movements, including synergies involving several joints, muscles, and planes of motion was used [22]. Therefore, increasing the sensory input about joint position and length changing and tension muscles in the central nervous system improves the ability of the nervous system to create a pattern of rapid recruitment and optimal use of muscles, increase the number of active motor units and increase muscle coordination. Consequently, reflex stabilization responses of the joint can be improved by activities that focus on sudden changes in joint position and stimulate the reflex neuromuscular control [17, 18, 22].
Limitations
Limitations exist in this study, including the low sample size and lack of high participation due to the COVID-19 pandemic, the lack of evaluation of the plantar pressure distribution symmetry during challenging daily activities, the lack of evaluation of other kinematic and kinetic variables during dynamic activities, and the sample size of the present study is only the elderly female population. As a result, it is recommended that researchers evaluate the plantar pressure distribution symmetry during daily challenging activities in future studies with a large sample size in the population of men and women.
5. Conclusion
The results of the present study showed that sensorimotor training improves balance strategies and sensorimotor coordination by improving neuromuscular coordination, and subsequently decreasing postural sway. As a result, by reducing the postural sway and improving the transmission of afferent information from mechanical receptors, and adjusting the balance strategies, the pressure distribution in different areas of the plantar is balanced.
Ethical Considerations
Compliance with ethical guidelines
This project was approved and registered at the National Committee for Ethics in Biomedical Research of Bu-Ali Sina (Code: IR.BASU.REC.1401.027).
Funding
The present paper was extracted from the MA. thesis ofFatemeh Lotfi at the Department of Corrective Exercises and Sports Injury, Faculty of Physical Education and Sport Sciences, Bu-Ali Sina University, Hamedan.
Authors' contributions
All authors contributed in preparing this article.
Conflict of interest
The authors declared no conflict of interest.
References
- Kasović M, Štefan L, Zvonař M. Domain-specific and total sedentary behavior associated with gait velocity in older adults: The mediating role of physical fitness. International Journal of Environmental Research and Public Health. 2020; 17(2):5 [DOI:10.3390/ijerph17020593] [PMID] [PMCID]
- Marques NR, Camilo GF, de Martini Lopes Dos Santos AP, Cardoso BC, Navega MT, de Abreu DCC. The ability of gait kinematic parameters to predict falls in older adults with cognitive impairments living in long term institutions. Clinical Biomechanics. 2019; 65:123-7. [DOI:10.1016/j.clinbiomech.2019.04.011] [PMID]
- Brown KE, Neva JL, Feldman SJ, Staines WR, Boyd LA. Sensorimotor integration in healthy aging: Baseline differences and response to sensory training. Experimental Gerontology. 2018; 112:1-8. [DOI:10.1016/j.exger.2018.08.004] [PMID]
- Qiu F, Cole MH, Davids KW, Hennig EM, Silburn PA, Netscher H, et al. Enhanced somatosensory information decreases postural sway in older people. Gait & Posture. 2012; 35(4):630-5. [DOI:10.1016/j.gaitpost.2011.12.013] [PMID]
- Unver B, Bek N. Plantar sensation, plantar pressure, and postural stability alterations and effects of visual status in older adults. Somatosensory & Motor Research. 2022; 39(1):55-61. [DOI:10.1080/08990220.2021.1994940] [PMID]
- Wong AM, Lin YC, Chou SW, Tang FT, Wong PY. Coordination exercise and postural stability in elderly people: Effect of tai chi chuan. Archives of Physical Medicine and Rehabilitation. 2001; 82(5):608-12. [DOI:10.1053/apmr.2001.22615] [PMID]
- Kalisch T, Tegenthoff M, Dinse HR. Improvement of sensorimotor functions in old age by passive sensory stimulation. Clinical Interventions in Aging. 2008; 3(4):673-90. [DOI:10.2147/CIA.S3174] [PMID] [PMCID]
- Scott G, Menz HB, Newcombe L. Age-related differences in foot structure and function. Gait & Posture. 2007; 26(1):68-75. [DOI:10.1016/j.gaitpost.2006.07.009] [PMID]
- Svoboda Z, Bizovska L, Gonosova Z, Linduska P, Kovacikova Z, Vuillerme N. Effect of aging on the association between ankle muscle strength and the control of bipedal stance. Plos One. 2019; 14(10):e0223434. [DOI:10.1371/journal.pone.0223434] [PMID] [PMCID]
- Yalfani A, Ahmadi M, Asgarpoor A. [Investigate the plantar pressure distribution in PFP patients: A systematic review (Persian)]. Journal for Research in Sport Rehabilitation. 2022; 9(17):73-83. [DOI:10.22084/RSR.2022.25484.1610]
- Machado ÁS, Bombach GD, Duysens J, Carpes FP. Differences in foot sensitivity and plantar pressure between young adults and elderly. Archives of Gerontology and Geriatrics. 2016; 63:67-71. [DOI:10.1016/j.archger.2015.11.005] [PMID]
- Menz HB, Morris ME. Clinical determinants of plantar forces and pressures during walking in older people. Gait & Posture. 2006; 24(2):229-36. [DOI:10.1016/j.gaitpost.2005.09.002] [PMID]
- Sanchis-Sanchis R, Blasco-Lafarga C, Encarnación-Martínez A, Pérez-Soriano P. Changes in plantar pressure and spatiotemporal parameters during gait in older adults after two different training programs.Gait & Posture. 2020; 77:250-6. [DOI:10.1016/j.gaitpost.2020.01.015] [PMID]
- Gawronska K, Lorkowski J. Evaluating the symmetry in plantar pressure distribution under the toes during standing in a postural pedobarographic examination. Symmetry. 2021; 13(8):1476. [DOI:10.3390/sym13081476]
- Wong PL, Chamari K, Chaouachi A, Mao DW, Wisløff U, Hong Y. Difference in plantar pressure between the preferred and non-preferred feet in four soccer-related movements. British Journal of Sports Medicine. 2007; 41(2):84-92. [DOI:10.1136/bjsm.2006.030908] [PMID] [PMCID]
- Pol F, Baharlouei H, Taheri A, Menz HB, Forghany S. Foot and ankle biomechanics during walking in older adults: A systematic review and meta-analysis of observational studies. Gait & Posture. 2021; 89:14-24. [DOI:10.1016/j.gaitpost.2021.06.018] [PMID]
- Yalfani A, Ahmadi M, Gandomi F. [The effect of twelve weeks of sensorimotor exercises on distribution plantar pressure variables and symmetry index in patients with patellofemoral pain syndrome: A randomized double-blind clinical trial (Persian)]. Studies in Medical Sciences. 2020; 31(6):445-58. [Link]
- Yalfani A, Ahmadi M, Gandomi F. [The effects of 12-weeks of senso- rimotor exercise on pain, strength, pelvic drop, and dynamic knee valgus in males with patellofemoral pain syndrome (Persian)]. Physical Treatment Journal. 2020; 10(3):159-68. [DOI:10.32598/ptj.10.3.442.1]
- Azarpaikan A, Taheri Torbati H. Effect of somatosensory and neurofeedback training on balance in older healthy adults: A preliminary investigation. Aging Clinical and Experimental Research. 2018; 30(7):745-53. [DOI:10.1007/s40520-017-0835-3] [PMID]
- Ahmad I, Verma S, Noohu MM, Shareef MY, Hussain ME. Sensorimotor and gait training improves proprioception, nerve function, and muscular activation in patients with diabetic peripheral neuropathy: A randomized control trial. Journal of Musculoskeletal & Neuronal Interactions. 2020; 20(2):234-48. [PMID] [PMCID]
- Fransen M, Crosbie J, Edmonds J. Physical therapy is effective for patients with osteoarthritis of the knee: A randomized controlled clinical trial. The Journal of Rheumatology. 2001; 28(1):156-64. [PMID]
- Ahmadi M, Yalfani A, Gandomi F. [Effect of twelve weeks of sensorimotor training on pain, improvement proprioception, muscle strength, and postural control in men with patellofemoral pain syndrome: A randomized single-blind clinical trial (Persian)]. Scientific Journal of Rehabilitation Medicine. 2021; 10(1):1-13. [DOI:10.22037/JRM.2020.112859.2271]
- Ahmadi M, Yalfani A, Gandomi F, Rashid K. The effect of twelve-week neurofeedback training on pain, proprioception, strength and postural balance in men with patellofemoral pain syndrome: A double-blind randomized control trial. Journal of Rehabilitation Sciences & Research. 2020; 7(2):66-74. [DOI:10.30476/jrsr.2020.84868.1067]
- Chiacchiero M, Dresely B, Silva U, Delosreyes R, Vorik B. The relationship between range of movement, flexibility, and balance in the elderly. Topics in Geriatric Rehabilitation. 2010; 26(2):148-55. [DOI:10.1097/TGR.0b013e3181e854bc]
- McKay MJ, Baldwin JN, Ferreira P, Simic M, Vanicek N, Wojciechowski E, et al. Spatiotemporal and plantar pressure patterns of 1000 healthy individuals aged 3-101 years. Gait & Posture. 2017; 58:78-87. [DOI:10.1016/j.gaitpost.2017.07.004] [PMID]
- Tracy BL. Force control is impaired in the ankle plantarflexors of elderly adults. European Journal of Applied Physiology. 2007; 101(5):629-36. [DOI:10.1007/s00421-007-0538-0] [PMID]
- Mackey DC, Robinovitch SN. Mechanisms underlying age-related differences in ability to recover balance with the ankle strategy. Gait & Posture. 2006; 23(1):59-68. [DOI:10.1016/j.gaitpost.2004.11.009] [PMID]
- Wingert JR, Welder C, Foo P. Age-related hip proprioception declines: Effects on postural sway and dynamic balance. Archives of Physical Medicine and Rehabilitation. 2014; 95(2):253-61. [DOI:10.1016/j.apmr.2013.08.012] [PMID]
- Bosch K, Nagel A, Weigend L, Rosenbaum D. From "first" to "last" steps in life--pressure patterns of three generations.Clinical Biomechanics. 2009; 24(8):676-81. [DOI:10.1016/j.clinbiomech.2009.06.001] [PMID]
- McCaskey MA, Schuster-Amft C, Wirth B, de Bruin ED. Effects of postural specific sensorimotor training in patients with chronic low back pain: Study protocol for randomised controlled trial. Trials. 2015; 16:571. [DOI:10.1186/s13063-015-1104-4] [PMID] [PMCID]
- Jeka J, Kiemel T, Creath R, Horak F, Peterka R. Controlling human upright posture: Velocity information is more accurate than position or acceleration. Journal of Neurophysiology. 2004; 92(4):2368-79. [DOI:10.1152/jn.00983.2003] [PMID]
- Porto JM, Freire Júnior RC, Bocarde L, Fernandes JA, Marques NR, Rodrigues NC, et al. Contribution of hip abductor-adductor muscles on static and dynamic balance of community-dwelling older adults. Aging Clinical and Experimental Research. 2019; 31(5):621-7. [DOI:10.1007/s40520-018-1025-7] [PMID]
- Ahmadi MR, Yalfani A, Gandomi F, Rashid K. [The effect of twelve week neurofeedback training on perceptual pain intensity, fear of pain, pelvic drop, and dynamic knee valgus index in men with patellofemoral pain syndrome: A randomized double-blind clinical trial (Persian)]. Sadra Medical Journal. 2020; 8(2):151-64. [DOI:10.30476/smsj.2020.85151.1108]
- Brauer SG, Burns YR, Galley P. A prospective study of laboratory and clinical measures of postural stability to predict community-dwelling fallers. The Journals of Gerontology. 2000; 55(8):M469-76. [DOI:10.1093/gerona/55.8.M469] [PMID]
- Nolan M, Nitz J, Choy NL, Illing S. Age-related changes in musculoskeletal function, balance and mobility measures in men aged 30-80 years. The Aging Male. 2010; 13(3):194-201.[DOI:10.3109/13685531003657818] [PMID]
- Ahmadi MR, Yalfani A. [Interlimb asymmetry of vertical ground reaction force as a risk factor for re-injury and knee oseteoarthritis following anterior cruciate ligament reconstruction: A systematic review (Persian)]. Journal of Research in Orthopedic Science. 2022; 9(1):15-24. [DOI:10.32598/JROSJ.9.1.857.1]
- Yalfani A, Ahmadi MR. Patients with patellofemoral pain exhibiting decrease vertical ground reaction force compared to healthy individuals during weight bearing tasks: A systematic reviews and meta-analysis. Iranian Journal of Public Health. 2023; 52(2):254-64. [DOI:10.18502/ijph.v52i2.11879]
- Ahmadi MR, Yalfani A. Do patellofemoral pain patients have higher loading rate compared to healthy indivalues? A systematic review and meta-analysis. Physical Treatment Journal. 2022; 12(1):13-22. [DOI:10.32598/ptj.12.1.442.2]
- Herssens N, Verbecque E, Hallemans A, Vereeck L, Van Rompaey V, Saeys W. Do spatiotemporal parameters and gait variability differ across the lifespan of healthy adults? A systematic review. Gait & Posture. 2018; 64:181-90.[DOI:10.1016/j.gaitpost.2018.06.012] [PMID]
Type of Study: Research |
Subject:
Sport injury and corrective exercises
Received: 2023/01/21 | Accepted: 2023/02/12 | Published: 2022/10/20
Received: 2023/01/21 | Accepted: 2023/02/12 | Published: 2022/10/20
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
