Tue, Aug 11, 2026
Volume 12, Issue 4 (Autumn 2022)
PTJ 2022, 12(4): 269-278 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Rahimi M, Piry H, Monajatipour E. Effect of Six Weeks of Pilates Exercises on the Function of Upper and Lower Extremities of Middle-aged Women With Lower Crossed Syndrome. PTJ 2022; 12 (4) :269-278
URL: http://ptj.uswr.ac.ir/article-1-546-en.html
URL: http://ptj.uswr.ac.ir/article-1-546-en.html



1- Department of Corrective Exercises and Sport Injuries, Faculty of Sport Sciences, Shahid Rajaee Teacher Training University, Tehran, Iran.
2- Department of Exercise Physiology and Sport Injuries, Faculty of Physical Education and Sport Sciences, Allameh Tabatabai University, Tehran, Iran.
3- Department of physical education, Science and Research Branch, Islamic Azad University, Tehran, Iran.
2- Department of Exercise Physiology and Sport Injuries, Faculty of Physical Education and Sport Sciences, Allameh Tabatabai University, Tehran, Iran.
3- Department of physical education, Science and Research Branch, Islamic Azad University, Tehran, Iran.
Full-Text [PDF 3311 kb]
(2831 Downloads)
| Abstract (HTML) (4809 Views)



Full-Text: (1896 Views)
1. Introduction
Women’s physical health is influenced by various factors, such as cultural, social, economic, and political characteristics of the society [1]. Women’s health and its various dimensions are closely related to their living conditions. Therefore, it is essential to pay attention to women’s health issues during their life cycle [2]. Incorrect habits in daily life cause deviation in the upright posture and compensatory movement patterns. Muscle imbalance may affect the body’s natural alignment and make a person suffer from various postural abnormalities [3]. Improper postures during work and job assignments for a long time can lead to musculoskeletal disorders [4]. Muscle imbalance may have serious consequences for the body [3]. Lower crossed syndrome (LCS) is one of the compensatory patterns proposed by Janda.
LCS is an abnormality in which the hip flexors and lower back muscles are tight and the abdominal and gluteal muscles are weak, and it is also known as distal or pelvic crossed syndrome [5]. This abnormality can lead to many problems for patients, including the concentration of stress on specific vertebral structures, pain in the lower back, postural disturbance, and disturbance in the individual’s function [6]. Specific postural changes seen in LCS include anterior pelvic tilt, increased lumbar lordosis, lateral lumbar shift, external rotation of the leg, and knee hyperextension. If the lordosis is deep and short, the imbalance is mainly in the pelvic muscles, and if the lordosis is shallow and extends to the back, the imbalance is dominant in the trunk muscles [5, 7]. This muscle imbalance leads to chronic back pain, which is more difficult to correct in the later stages [5]. If a lordotic posture exists for a long period, it can lead to insufficient rest for normal tissue adaptation and recovery, and as a result, increases the risk of tissue damage [8]. A change in the pattern of neuromuscular control and several changes in the spine can be one of the common causes of LCS. In addition, dysfunction of the deep muscle system and the increase in the activity of more superficial muscles can be the source of noticeable changes in the vertebral arch [6]. The prevalence of LCS in school-aged children was reported to be 21% [9] and this syndrome is more common in women than men [5].
The balance between strength and stability in the upper and lower kinematic chains is very crucial for the prevention of musculoskeletal disorders. Core stability plays a crucial role in preventing sports injuries [10]. Maintaining postural alignment and stability during functional activities is one of the tasks of the central region of the body, which helps in the prevention of inappropriate patterns. Asymmetry in position and movement does not allow the core to be stable [11]. Limitations in the strength, endurance, and stability of the deep muscles lead to incorrect sports techniques related to the upper and lower extremities and make the athlete prone to injury [12]. An optimal central region maintains the natural length-tension relationship of the agonist and antagonist muscles, and this leads to optimal kinematics of the joints in the lumbo-pelvic-hip complex in functional movements and creates maximum stability for the lower and upper extremities movements [13]. The previous research findings suggest that the strength and endurance of the core stabilizer muscles in people with lower extremity injuries are lower than in those without a history of injury [14].
Research has proven the importance of core stability in producing efficient and effective limb and trunk movements to generate, transmit and control force and energy during integrated kinematic chain activities [15], for example, Hodges and Richardson studied the sequence of muscle activation during total body motions and found that some stabilizers of the central region (transversus-abdominis, multifidus, rectus abdominis, and internal and external obliques) are activated before any movement in the limbs [16, 17]. These muscles are also responsible for maintaining the alignment of the pelvis, so that the weakness of these muscles leads to the loss of the correct pelvis alignment, followed by disruption of the length-tension relationship of the muscles of the lower extremity that are connected to this area, and causes a decrease in efficiency and the exposure of the lower extremity to injuries [18].
Typically, musculoskeletal examination focuses on measuring the range of motion and muscular strength of different parts of the body, which cannot provide sufficient information about the overall performance level of those parts [19]. Functional tests can be considered a low-cost clinical tool and a complementary aid to provide quantitative data about the functional ability and function of a body part [20, 21]. The closed kinetic chain upper extremity stability test (CKCUES) is a functional test and is used to assess shoulder function before and after a muscle-strengthening protocol [19, 22].
Various exercises of the core region are performed on a stable and unstable level. Pilates exercises are one of the newest training methods. These exercises emphasize breathing rhythm, strengthening deep muscles, concentration, and mind engagement in the exercise. Today, this sport is widely used to rehabilitate, improve health and help treat various diseases. Pilates also focuses on the body, especially the core muscles, pelvis, and spine [23]. The effect of Pilates exercises has been proven in improving the performance of elderly people [24], improving abdominal strength and endurance and trunk flexibility [25], and decreasing pain in women suffering from back pain and disc herniation patients with symptoms of Lumbosciatalgia [26]. Pilates improves flexibility and strength and develops control and endurance throughout the body. This sport works on body alignment, breathing and building a strong core region, and improving coordination and balance. The core region of the body plays a vital role in maintaining stability [27].
Based on the literature, weakness in the core stability of the trunk as well as weakness in the function of the upper and lower extremities is evident in patients with LCS, and the authors did not find any research in this regard during their literature review. Therefore, considering the popularity of Pilates exercises among different classes of society and the prevalence of LCS among women, the present study was conducted to investigate the effect of Pilates exercises on the function of the upper and lower extremities of women with LCS.
2. Materials and Methods
The present research is quasi-experimental applied research with a pre-test and post-test research design. The statistical population of the study was women with LCS in the age range of 35 to 50 years. The statistical sample included 30 women with LCS from Tiam Sport Club. The number of participants was calculated based on G Power3 sample size software, considering the parameters of alpha coefficient=0.05, and power=0.8. After the initial selection and evaluation, the subjects were randomly divided into Pilates training group (n=15) and a control group (n=15) by dice throwing. Thus, the numbers 1, 2, and 3 of the dice were considered for the control group, and the numbers 4, 5, and 6 of the dice were considered for the Pilates training group.
The research inclusion criteria included female gender, the age range of 35-50 years, willingness to participate in the research, having a lumbar lordosis angle of more than 50 degrees, no history of injuries to the limbs and spine in the last 6 months, not having any type of neuromuscular disorder, the absence of balance disorders, having the criteria of the LCS, including the shortness of the hip flexors (based on Thomas test) [28] and erector spinal muscles straighteners [29, 30] and weakness of abdominal muscles (trunk flexion strength and coordination test) [31] and gluteal muscles (hip extension strength/coordination test in palmar position) [31, 32]. The exclusion criteria included having any specific orthopedic and neurological disorders, such as progressive spinal arthrosis, abdominal and back surgery in the last 3 months, spinal compression fractures or radiculopathy due to spinal canal stenosis or disc herniation, and history of surgery, and other issues, such as intolerance to research tests, irregular participation in training sessions, and pregnancy [9, 33]. It should be noted that this research has a code of ethics from the Islamic Azad University-Science and Research Branch, and the code of ethics is IR.IAU.SRB.REC.1400.292.
Before starting the research, in the familiarization session, the way to conduct the research was explained to the subjects, and before doing the Pilates exercises, the function of the upper and lower extremities was measured. Upper extremity function was evaluated by Y and Davies tests and lower extremity function was evaluated by side hop and square hop tests.
Side hop test: The subject hopped forward and backward 10 times on the dominant leg at a distance of 30 cm marked by two pieces of parallel tape on the ground surface. The subject’s time was recorded by a stopwatch (unique with 0.01 accuracy) before and after the Pilates training protocol. The inter-rater reliability of this test in healthy athletes has been reported to be 0.97 [34] (Figure 1).
Women’s physical health is influenced by various factors, such as cultural, social, economic, and political characteristics of the society [1]. Women’s health and its various dimensions are closely related to their living conditions. Therefore, it is essential to pay attention to women’s health issues during their life cycle [2]. Incorrect habits in daily life cause deviation in the upright posture and compensatory movement patterns. Muscle imbalance may affect the body’s natural alignment and make a person suffer from various postural abnormalities [3]. Improper postures during work and job assignments for a long time can lead to musculoskeletal disorders [4]. Muscle imbalance may have serious consequences for the body [3]. Lower crossed syndrome (LCS) is one of the compensatory patterns proposed by Janda.
LCS is an abnormality in which the hip flexors and lower back muscles are tight and the abdominal and gluteal muscles are weak, and it is also known as distal or pelvic crossed syndrome [5]. This abnormality can lead to many problems for patients, including the concentration of stress on specific vertebral structures, pain in the lower back, postural disturbance, and disturbance in the individual’s function [6]. Specific postural changes seen in LCS include anterior pelvic tilt, increased lumbar lordosis, lateral lumbar shift, external rotation of the leg, and knee hyperextension. If the lordosis is deep and short, the imbalance is mainly in the pelvic muscles, and if the lordosis is shallow and extends to the back, the imbalance is dominant in the trunk muscles [5, 7]. This muscle imbalance leads to chronic back pain, which is more difficult to correct in the later stages [5]. If a lordotic posture exists for a long period, it can lead to insufficient rest for normal tissue adaptation and recovery, and as a result, increases the risk of tissue damage [8]. A change in the pattern of neuromuscular control and several changes in the spine can be one of the common causes of LCS. In addition, dysfunction of the deep muscle system and the increase in the activity of more superficial muscles can be the source of noticeable changes in the vertebral arch [6]. The prevalence of LCS in school-aged children was reported to be 21% [9] and this syndrome is more common in women than men [5].
The balance between strength and stability in the upper and lower kinematic chains is very crucial for the prevention of musculoskeletal disorders. Core stability plays a crucial role in preventing sports injuries [10]. Maintaining postural alignment and stability during functional activities is one of the tasks of the central region of the body, which helps in the prevention of inappropriate patterns. Asymmetry in position and movement does not allow the core to be stable [11]. Limitations in the strength, endurance, and stability of the deep muscles lead to incorrect sports techniques related to the upper and lower extremities and make the athlete prone to injury [12]. An optimal central region maintains the natural length-tension relationship of the agonist and antagonist muscles, and this leads to optimal kinematics of the joints in the lumbo-pelvic-hip complex in functional movements and creates maximum stability for the lower and upper extremities movements [13]. The previous research findings suggest that the strength and endurance of the core stabilizer muscles in people with lower extremity injuries are lower than in those without a history of injury [14].
Research has proven the importance of core stability in producing efficient and effective limb and trunk movements to generate, transmit and control force and energy during integrated kinematic chain activities [15], for example, Hodges and Richardson studied the sequence of muscle activation during total body motions and found that some stabilizers of the central region (transversus-abdominis, multifidus, rectus abdominis, and internal and external obliques) are activated before any movement in the limbs [16, 17]. These muscles are also responsible for maintaining the alignment of the pelvis, so that the weakness of these muscles leads to the loss of the correct pelvis alignment, followed by disruption of the length-tension relationship of the muscles of the lower extremity that are connected to this area, and causes a decrease in efficiency and the exposure of the lower extremity to injuries [18].
Typically, musculoskeletal examination focuses on measuring the range of motion and muscular strength of different parts of the body, which cannot provide sufficient information about the overall performance level of those parts [19]. Functional tests can be considered a low-cost clinical tool and a complementary aid to provide quantitative data about the functional ability and function of a body part [20, 21]. The closed kinetic chain upper extremity stability test (CKCUES) is a functional test and is used to assess shoulder function before and after a muscle-strengthening protocol [19, 22].
Various exercises of the core region are performed on a stable and unstable level. Pilates exercises are one of the newest training methods. These exercises emphasize breathing rhythm, strengthening deep muscles, concentration, and mind engagement in the exercise. Today, this sport is widely used to rehabilitate, improve health and help treat various diseases. Pilates also focuses on the body, especially the core muscles, pelvis, and spine [23]. The effect of Pilates exercises has been proven in improving the performance of elderly people [24], improving abdominal strength and endurance and trunk flexibility [25], and decreasing pain in women suffering from back pain and disc herniation patients with symptoms of Lumbosciatalgia [26]. Pilates improves flexibility and strength and develops control and endurance throughout the body. This sport works on body alignment, breathing and building a strong core region, and improving coordination and balance. The core region of the body plays a vital role in maintaining stability [27].
Based on the literature, weakness in the core stability of the trunk as well as weakness in the function of the upper and lower extremities is evident in patients with LCS, and the authors did not find any research in this regard during their literature review. Therefore, considering the popularity of Pilates exercises among different classes of society and the prevalence of LCS among women, the present study was conducted to investigate the effect of Pilates exercises on the function of the upper and lower extremities of women with LCS.
2. Materials and Methods
The present research is quasi-experimental applied research with a pre-test and post-test research design. The statistical population of the study was women with LCS in the age range of 35 to 50 years. The statistical sample included 30 women with LCS from Tiam Sport Club. The number of participants was calculated based on G Power3 sample size software, considering the parameters of alpha coefficient=0.05, and power=0.8. After the initial selection and evaluation, the subjects were randomly divided into Pilates training group (n=15) and a control group (n=15) by dice throwing. Thus, the numbers 1, 2, and 3 of the dice were considered for the control group, and the numbers 4, 5, and 6 of the dice were considered for the Pilates training group.
The research inclusion criteria included female gender, the age range of 35-50 years, willingness to participate in the research, having a lumbar lordosis angle of more than 50 degrees, no history of injuries to the limbs and spine in the last 6 months, not having any type of neuromuscular disorder, the absence of balance disorders, having the criteria of the LCS, including the shortness of the hip flexors (based on Thomas test) [28] and erector spinal muscles straighteners [29, 30] and weakness of abdominal muscles (trunk flexion strength and coordination test) [31] and gluteal muscles (hip extension strength/coordination test in palmar position) [31, 32]. The exclusion criteria included having any specific orthopedic and neurological disorders, such as progressive spinal arthrosis, abdominal and back surgery in the last 3 months, spinal compression fractures or radiculopathy due to spinal canal stenosis or disc herniation, and history of surgery, and other issues, such as intolerance to research tests, irregular participation in training sessions, and pregnancy [9, 33]. It should be noted that this research has a code of ethics from the Islamic Azad University-Science and Research Branch, and the code of ethics is IR.IAU.SRB.REC.1400.292.
Before starting the research, in the familiarization session, the way to conduct the research was explained to the subjects, and before doing the Pilates exercises, the function of the upper and lower extremities was measured. Upper extremity function was evaluated by Y and Davies tests and lower extremity function was evaluated by side hop and square hop tests.
Side hop test: The subject hopped forward and backward 10 times on the dominant leg at a distance of 30 cm marked by two pieces of parallel tape on the ground surface. The subject’s time was recorded by a stopwatch (unique with 0.01 accuracy) before and after the Pilates training protocol. The inter-rater reliability of this test in healthy athletes has been reported to be 0.97 [34] (Figure 1).
Square hop test: In this test, a square with sides of 40 cm was drawn on the ground with adhesive tape. The subject was asked to hop as fast as possible 5 times along the path drawn in the figure inside and outside the square with the dominant leg (right leg counterclockwise and left leg clockwise). If during the test, the person tripped on the opposite leg, lost balance, or could not hop on the marked strips for landing, or hit the sides, the test was not accepted. Inter-rater reliability of this test has been reported as 0.90 [34].
Davies Test: This test examines muscular strength and endurance and the closed kinetic chain upper extremity stability (CKCUES). Its reliability is reported as 0.92. To perform the test, two pieces of tape with a width of 5 cm were placed parallel to each other at a distance of 91 cm from each other on the ground surface where the measurement was to be performed. The starting position for the test was while the hands were placed on each piece of the tape and the subject was in the push-up position. Subjects were instructed to pass one hand under their body and reach the tape under their opposite hand and return to the starting position after touching the tape. The subject repeated the same movement for the other hand. The repetition of this movement was counted in 15 s. The number of hand contact was the subject’s test score [35] (Figure 2).
Davies Test: This test examines muscular strength and endurance and the closed kinetic chain upper extremity stability (CKCUES). Its reliability is reported as 0.92. To perform the test, two pieces of tape with a width of 5 cm were placed parallel to each other at a distance of 91 cm from each other on the ground surface where the measurement was to be performed. The starting position for the test was while the hands were placed on each piece of the tape and the subject was in the push-up position. Subjects were instructed to pass one hand under their body and reach the tape under their opposite hand and return to the starting position after touching the tape. The subject repeated the same movement for the other hand. The repetition of this movement was counted in 15 s. The number of hand contact was the subject’s test score [35] (Figure 2).
Before the test, the body was warmed up for 5 minutes.
To evaluate the performance of YBT-UQ, the Y balance test was used, which is performed in anterior, posterolateral, and posteromedial directions, and the internal reliability coefficient of this test was reported as 0.99-0.8. This test was repeated three times for both hands, and the average of three repetitions in each direction was used for analysis, and two-minute rest was given between each trial to prevent fatigue. In addition, before the test, the dominant hand of the subjects was determined according to the tendency of the subjects to throw the ball. The length of the upper extremity affects their reach distance; hence, the raw balance scores were normalized based on upper extremity length. To record the length of the upper extremity, the distance from the spinous process of C7 to the end of the middle finger was measured, while the shoulders were abducted 90 degrees, and the elbows, wrists, and fingers were extended (Figure 3).
To evaluate the performance of YBT-UQ, the Y balance test was used, which is performed in anterior, posterolateral, and posteromedial directions, and the internal reliability coefficient of this test was reported as 0.99-0.8. This test was repeated three times for both hands, and the average of three repetitions in each direction was used for analysis, and two-minute rest was given between each trial to prevent fatigue. In addition, before the test, the dominant hand of the subjects was determined according to the tendency of the subjects to throw the ball. The length of the upper extremity affects their reach distance; hence, the raw balance scores were normalized based on upper extremity length. To record the length of the upper extremity, the distance from the spinous process of C7 to the end of the middle finger was measured, while the shoulders were abducted 90 degrees, and the elbows, wrists, and fingers were extended (Figure 3).
The reach distance was divided by the length of the upper extremity in centimeters and multiplied by 100. In addition to considering all three directions separately, an overall score for performance was calculated through the following formula [36].
Total score= (Medial+posterolateral+posteromedial)/(Length of upper extremity multiplied by 3) *100
In the post-test phase, after six weeks of Pilates exercises, the tests conducted in the pre-test conditions were again performed on the subjects in both groups. The Pilates training program included kicks from the side, single leg extension, shoulder bridge, push-up, swan dive, rounding up, single leg circle and double arm extension, and spine rotation (Table 1), which lasted for 6 weeks, 3 a week and each session was 30 minutes [37].

Each exercise was started with 2 sets and 15 repetitions and increased to 3 sets and 30 repetitions in 6 weeks.
Descriptive and inferential statistical methods were used to analyze the collected data. The Shapiro-Wilk test was used to check the normality of data distribution. To compare variables between groups, an analysis of covariance (ANCOVA) was used at a significance level of P≥0.05. The statistical calculations were performed in SPSS software v. 22 (P<0.05).
3. Results
Table 2 presents the descriptive analysis of demographic characteristics (age (year), height (cm), weight (Kgr) and body mass index) of subjects and pre-test data by research groups.

The results showed no significant difference in these variables between the research groups in the pre-test (P>0.05).
Considering the normality of the data, which was determined by the Shapiro-Wilk test, the ANCOVA test was used to compare the research variables between groups, including upper and lower extremities function.
Table 3 presents the results of the ANCOVA test for between-group comparison were presented in Table 3.
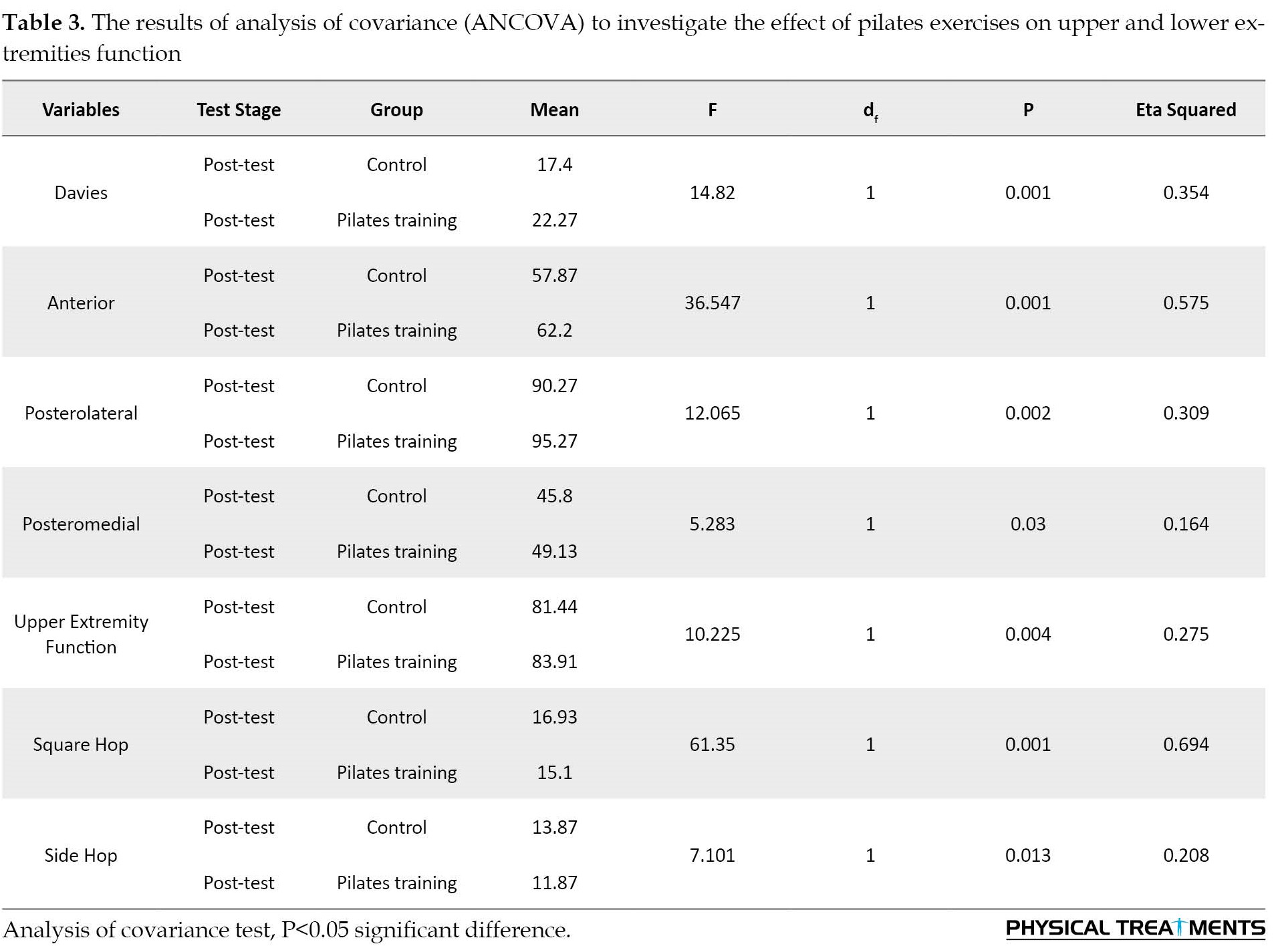
The results of the ANCOVA test showed that after controlling the effect of the pre-test, a significant difference is observed in the variables that show the function of upper and lower extremities (P≤0.05) in the post-test between the Pilates training and control groups. So that upper and lower extremities function in the Pilates training group showed a significant improvement compared to the control group.
4. Discussion
This research was conducted to investigate the effect of six weeks of Pilates exercises on the function of the upper and lower extremities of women with LCS. The results of the present research showed that the Pilates training group obtained better results in the post-test than the pre-test and the control group in the side hop test and the square hop test (lower extremity function tests), while no significant difference was observed between the pre-test and post-test in the control group. Besides, the results indicated that in the Y test and Davies test (upper extremity function tests), the Pilates training group obtained better results in the post-test than the pre-test, while no significant change was observed in the control group.
Since Pilates is one of the new training methods in the world and also the research sources regarding this new training method are not very rich, no research was found to directly compare its results with the results of the current research. Therefore, the results of the research that investigated the effect of a training method on the performance of athletes can be compared with the results of the current research.
Pilates emphasizes breathing rhythm and strengthening of the deep muscles, and concentration and challenges the mind during exercises. Pilates also has a special focus on the muscles, pelvis, and spine [23]. In addition, enhancement of performance in elderly people [24], improved muscular strength, endurance, trunk flexibility [25], and improved pain in women with back pain and symptoms of Lumbosciatalgia have been attributed to participating in Pilates exercises [26].
The continuous activation of the core stabilizer muscles provides a solid and reliable base for the upper and lower extremities when performing various functional tasks, which will play a vital role in injury prevention. The results of previous studies research results have shown a direct relationship between the performance of the core region and the function of the upper and lower extremities and the occurrence of sudden injuries [38].
Several studies proved that a person who has control over the medial muscles of his body and cannot establish stability in the central regions of his body is greatly exposed to sudden injuries [39]. It should be noted that core stability training significantly corrects the defects of the neuromuscular system, and this creates optimal muscle balance and optimal arthrokinematics in the entire lumbar-pelvic-hip region during the functional kinetic chain. It provides the stability of the proximal segment for mobility in the distal segment [40]. Therefore, according to the present research, modern Pilates exercises can be prescribed as a special and appropriate tool to improve performance and even reduce and prevent injuries for everyone.
Improper habits in daily life cause deviations in posture and compensatory movement patterns. Moreover, muscle imbalance can result in postural abnormalities [3]. In addition to core stability, the balance between strength and stability in the kinetic chain of the lower and upper extremities is vital to prevent physical injuries [10].
A possible explanation for improved performance in women with LCS may be an increase in strength and efficiency of core stabilizer muscles due to participation in Pilates training sessions for 6 weeks. Therefore, physiotherapists and physical therapists are suggested to use the Pilates exercises described in this study to improve the function of the upper and lower extremities of women with LCS.
Among the controllable limitations of the present study, we can mention the age, place of training, and the exclusion of injured people. The uncontrollable limitations of the research included the lack of control over the nutritional status of the subjects, the lack of control over the mental and psychological conditions of the subjects, the psychological effects of COVID-19, the variation in the level of interest, and the differences in the level of motivation of the subjects.
5. Conclusion
According to the results, it can be concluded that Pilates exercises can improve the function of the upper and lower extremities, perhaps through increasing the strength and efficiency of the core stabilizer muscles, therefore it seems logical to suggest to the trainers and physiotherapists that Pilates exercises may be used to increase performance in women with LCS.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by ethical committee of the Science and Research Branch, Islamic Azad University (Code: IR.IAU.SRB.REC.1400.292).
Funding
This research received no funding from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Data analysis and writing–review, and editing: All authors; Data collection and investigation: Effat Monajatipour; Supervision: Mohammad Rahimi and Hashem Piry.
Conflict of interest
The authors declared no conflict of interest.
References
Total score= (Medial+posterolateral+posteromedial)/(Length of upper extremity multiplied by 3) *100
In the post-test phase, after six weeks of Pilates exercises, the tests conducted in the pre-test conditions were again performed on the subjects in both groups. The Pilates training program included kicks from the side, single leg extension, shoulder bridge, push-up, swan dive, rounding up, single leg circle and double arm extension, and spine rotation (Table 1), which lasted for 6 weeks, 3 a week and each session was 30 minutes [37].
Each exercise was started with 2 sets and 15 repetitions and increased to 3 sets and 30 repetitions in 6 weeks.
Descriptive and inferential statistical methods were used to analyze the collected data. The Shapiro-Wilk test was used to check the normality of data distribution. To compare variables between groups, an analysis of covariance (ANCOVA) was used at a significance level of P≥0.05. The statistical calculations were performed in SPSS software v. 22 (P<0.05).
3. Results
Table 2 presents the descriptive analysis of demographic characteristics (age (year), height (cm), weight (Kgr) and body mass index) of subjects and pre-test data by research groups.
The results showed no significant difference in these variables between the research groups in the pre-test (P>0.05).
Considering the normality of the data, which was determined by the Shapiro-Wilk test, the ANCOVA test was used to compare the research variables between groups, including upper and lower extremities function.
Table 3 presents the results of the ANCOVA test for between-group comparison were presented in Table 3.
The results of the ANCOVA test showed that after controlling the effect of the pre-test, a significant difference is observed in the variables that show the function of upper and lower extremities (P≤0.05) in the post-test between the Pilates training and control groups. So that upper and lower extremities function in the Pilates training group showed a significant improvement compared to the control group.
4. Discussion
This research was conducted to investigate the effect of six weeks of Pilates exercises on the function of the upper and lower extremities of women with LCS. The results of the present research showed that the Pilates training group obtained better results in the post-test than the pre-test and the control group in the side hop test and the square hop test (lower extremity function tests), while no significant difference was observed between the pre-test and post-test in the control group. Besides, the results indicated that in the Y test and Davies test (upper extremity function tests), the Pilates training group obtained better results in the post-test than the pre-test, while no significant change was observed in the control group.
Since Pilates is one of the new training methods in the world and also the research sources regarding this new training method are not very rich, no research was found to directly compare its results with the results of the current research. Therefore, the results of the research that investigated the effect of a training method on the performance of athletes can be compared with the results of the current research.
Pilates emphasizes breathing rhythm and strengthening of the deep muscles, and concentration and challenges the mind during exercises. Pilates also has a special focus on the muscles, pelvis, and spine [23]. In addition, enhancement of performance in elderly people [24], improved muscular strength, endurance, trunk flexibility [25], and improved pain in women with back pain and symptoms of Lumbosciatalgia have been attributed to participating in Pilates exercises [26].
The continuous activation of the core stabilizer muscles provides a solid and reliable base for the upper and lower extremities when performing various functional tasks, which will play a vital role in injury prevention. The results of previous studies research results have shown a direct relationship between the performance of the core region and the function of the upper and lower extremities and the occurrence of sudden injuries [38].
Several studies proved that a person who has control over the medial muscles of his body and cannot establish stability in the central regions of his body is greatly exposed to sudden injuries [39]. It should be noted that core stability training significantly corrects the defects of the neuromuscular system, and this creates optimal muscle balance and optimal arthrokinematics in the entire lumbar-pelvic-hip region during the functional kinetic chain. It provides the stability of the proximal segment for mobility in the distal segment [40]. Therefore, according to the present research, modern Pilates exercises can be prescribed as a special and appropriate tool to improve performance and even reduce and prevent injuries for everyone.
Improper habits in daily life cause deviations in posture and compensatory movement patterns. Moreover, muscle imbalance can result in postural abnormalities [3]. In addition to core stability, the balance between strength and stability in the kinetic chain of the lower and upper extremities is vital to prevent physical injuries [10].
A possible explanation for improved performance in women with LCS may be an increase in strength and efficiency of core stabilizer muscles due to participation in Pilates training sessions for 6 weeks. Therefore, physiotherapists and physical therapists are suggested to use the Pilates exercises described in this study to improve the function of the upper and lower extremities of women with LCS.
Among the controllable limitations of the present study, we can mention the age, place of training, and the exclusion of injured people. The uncontrollable limitations of the research included the lack of control over the nutritional status of the subjects, the lack of control over the mental and psychological conditions of the subjects, the psychological effects of COVID-19, the variation in the level of interest, and the differences in the level of motivation of the subjects.
5. Conclusion
According to the results, it can be concluded that Pilates exercises can improve the function of the upper and lower extremities, perhaps through increasing the strength and efficiency of the core stabilizer muscles, therefore it seems logical to suggest to the trainers and physiotherapists that Pilates exercises may be used to increase performance in women with LCS.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by ethical committee of the Science and Research Branch, Islamic Azad University (Code: IR.IAU.SRB.REC.1400.292).
Funding
This research received no funding from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Data analysis and writing–review, and editing: All authors; Data collection and investigation: Effat Monajatipour; Supervision: Mohammad Rahimi and Hashem Piry.
Conflict of interest
The authors declared no conflict of interest.
References
- Ahmadi B, Farzadi F, Dejman M, Vameghi M, Mohammadi F, Mohtashami B, et al. [Farmehr model: Iranian women’s health conceptual framework (Persian)]. Hakim Research Journal. 2014; 16(4):337-48. [Link]
- Chuni N, Sreeramareddy CT. Frequency of symptoms, determinants of severe symptoms, validity of and cut-off score for Menopause Rating Scale (MRS) as a screening tool: A cross-sectional survey among midlife Nepalese women. BMC Womens Health. 2011; 11:30. [DOI:10.1186/1472-6874-11-30] [PMID] [PMCID]
- Kargarfard M, Mahdavi-Nejad R, Ghasemi GA, Rouzbehani R, Ghias M, Mahdavi-Jafari Z, et al. Assessment of spinal curvature in isfahan university students. Journal of Isfahan Medical School. 2010; 27(102):762-76. [Link]
- Balogh I, Ohlsson K, Nordander C, Björk J, Hansson GÅ. The importance of work organization on workload and musculoskeletal health--Grocery store work as a model. Applied Ergonomics. 2016; 53 Pt A:143-51 [DOI:10.1016/j.apergo.2015.09.004] [PMID]
- Das S, Sarkar B, Sharma R, Mondal M, Kumar P, Sahay P. Prevalence of lower crossed syndrome in young adults: A cross sectional study. International Journal of Advanced Research. 2017; 5(6):2217-28. [DOI:10.21474/IJAR01/4662]
- Parfrey K, Gibbons SG, Drinkwater EJ, Behm DG. Effect of head and limb orientation on trunk muscle activation during abdominal hollowing in chronic low back pain. BMC Musculoskeletal Disorders. 2014; 15:52. [DOI:10.1186/1471-2474-15-52] [PMID] [PMCID]
- Janda V. Some aspects of extracranial causes of facial pain. The Journal of Prosthetic Dentistry. 1986; 56(4):484-7.[DOI:10.1016/0022-3913(86)90394-X] [PMID]
- Sorensen CJ, Norton BJ, Callaghan JP, Hwang CT, Van Dillen LR. Is lumbar lordosis related to low back pain development during prolonged standing? Manual Therapy. 2015; 20(4):553-7. [DOI:10.1016/j.math.2015.01.001] [PMID] [PMCID]
- Kale SS, Gijare S. Prevalence of lower crossed syndrome in school going children of age 11 to 15 years. Indian Journal of Physiotherapy and Occupational Therapy. 2019; 13(2):176. [DOI:10.5958/0973-5674.2019.00068.6]
- Fredericson M, Moore T. Muscular balance, core stability, and injury prevention for middle- and long-distance runners. Physical Medicine and Rehabilitation Clinics of North America. 2005; 16(3):669-89. [DOI:10.1016/j.pmr.2005.03.001] [PMID]
- Zazulak BT, Hewett TE, Reeves NP, Goldberg B, Cholewicki J. Deficits in neuromuscular control of the trunk predict knee injury risk: A prospective biomechanical-epidemiologic study. The American Journal of Sports Medicine. 2007; 35(7):1123-30. [DOI:10.1177/0363546507301585] [PMID]
- Lederman E. The myth of core stability. Journal of Bodywork and Movement Therapies. 2010; 14(1):84-98.[DOI:10.1016/j.jbmt.2009.08.001] [PMID]
- Sato K, Mokha M. Does core strength training influence running kinetics, lower-extremity stability, and 5000-M performance in runners? Journal of Strength and conditioning Research. 2009; 23(1):133-40. [DOI:10.1519/JSC.0b013e31818eb0c5] [PMID]
- Cichanowski HR, Schmitt JS, Johnson RJ, Niemuth PE. Hip strength in collegiate female athletes with patellofemoral pain. Medicine and Science in Sports and Exercise. 2007; 39(8):1227-32. [DOI:10.1249/mss.0b013e3180601109] [PMID]
- Stickler L, Finley M, Gulgin H. Relationship between hip and core strength and frontal plane alignment during a single leg squat. Physical Therapy in Sport. 2015; 16(1):66-71.[DOI:10.1016/j.ptsp.2014.05.002] [PMID]
- Okada T, Huxel KC, Nesser TW. Relationship between core stability, functional movement, and performance. Journal of Strength and Conditioning Research. 2011; 25(1):252-61. [DOI:10.1519/JSC.0b013e3181b22b3e] [PMID]
- Hodges PW, Richardson CA. Feedforward contraction of transversus abdominis is not influenced by the direction of arm movement. Experimental Brain Research. 1997; 114(2):362-70.[DOI:10.1007/PL00005644] [PMID]
- Arvinen-Barrow M, Massey WV, Hemmings B. Role of sport medicine professionals in addressing psychosocial aspects of sport-injury rehabilitation: Professional athletes' views. Journal of Athletic Training. 2014; 49(6):764-72.[DOI:10.4085/1062-6050-49.3.44] [PMID] [PMCID]
- Schulte-Edelmann JA, Davies GJ, Kernozek TW, Gerberding ED. The effects of plyometric training of the posterior shoulder and elbow. Journal of Strength and Conditioning Research. 2005; 19(1):129-34.[DOI:10.1519/13963.1] [PMID]
- Hollstadt K, Boland M, Mulligan I. Test-retest reliability of the closed kinetic chain upper extremity stability test (ckcuest) in a modified test position in division i collegiate basketball players. International Journal of Sports Physical Therapy. 2020; 15(2):203-9. [DOI:10.26603/ijspt20200203] [PMID] [PMCID]
- Roush JR, Kitamura J, Waits MC. Reference Values for the Closed Kinetic Chain Upper Extremity Stability Test (CKCUEST) for Collegiate Baseball Players. North American Journal of Sports Physical Therapy. 2007; 2(3):159-63. [PMID] [PMCID]
- Lust KR, Sandrey MA, Bulger SM, Wilder N. The effects of 6-week training programs on throwing accuracy, proprioception, and core endurance in baseball. Journal of Sport Rehabilitation. 2009; 18(3):407-26. [DOI:10.1123/jsr.18.3.407] [PMID]
- Caldwell K, Harrison M, Adams M, Triplett NT. Effect of Pilates and taiji quan training on self-efficacy, sleep quality, mood, and physical performance of college students. Journal of Bodywork and Movement Therapies. 2009; 13(2):155-63. [DOI:10.1016/j.jbmt.2007.12.001] [PMID]
- Curi Pérez VS, Haas AN, Wolff SS. Analysis of activities in the daily lives of older adults exposed to the Pilates Method. Journal of Bodywork and Movement Therapies. 2014; 18(3):326-31. [DOI:10.1016/j.jbmt.2013.10.004] [PMID]
- Sekendiz B, Altun Ö, Korkusuz F, Akın S. Effects of pilates exercise on trunk strength, endurance and flexibility in sedentary adult females. Journal of Bodywork and Movement Therapies. 2007;11(4):318-26. [DOI:10.1016/j.jbmt.2006.12.002]
- Golpaygani M, Mahdavi S, Moradi L. [The effects of a pilates training program on the function and pain of patients with disc herniation with lumbosciatalgia (Persian)]. Journal of Exercise Science and Medicine. 2013; 5(1):41-53. [DOI:10.22059/JSMED.2013.32161]
- Srivastav P, Nayak N, Nair S, Sherpa LB, Dsouza D. Swiss ball versus mat exercises for core activation of transverse abdominis in recreational athletes. Journal of Clinical and Diagnostic Research. 2016; 10(12):YC01-3. [DOI:10.7860/JCDR/2016/23102.8972] [PMID] [PMCID]
- Pringle K, Myofascial pain and dysfunction: The trigger point manual: Volume 1. 2nd edition. Journal of Manipulative and Physiological Therapeutics. 1999; 22(5):PA1. [DOI:10.1016/S0161-4754(99)70079-5]
- Chaitow L, Crenshaw K. Muscle energy techniques. Amsterdam: Elsevier Health Sciences; 2006. [Link]
- Robinson HS, Mengshoel AM. Assessments of lumbar flexion range of motion: intertester reliability and concurrent validity of 2 commonly used clinical tests. Spine. 2014; 39(4):E270-5. [DOI:10.1097/BRS.0000000000000131] [PMID]
- Shearer HM. Rehabilitation of the Spine – A Practitioner’s Manual, 2nd Ed. The Journal of the Canadian Chiropractic Association. 2007; 51(1):62. [PMCID]
- Manske R, Magee DJ. Orthopedic physical assessment. Amsterdam: Elsevier Health Sciences; 2018. [Link]
- Dhanani S, Shah DT. A survey on prevalence of lower crossed syndrome in young females. IJPSH. 2014; 4(1):2249-5738. [Link]
- Sharma N, Sharma A, Singh Sandhu J. Functional performance testing in athletes with functional ankle instability. Asian Journal of Sports Medicine. 2011; 2(4):249-58. [DOI:10.5812/asjsm.34741] [PMID] [PMCID]
- Tucci HT, Martins J, Sposito Gde C, Camarini PM, de Oliveira AS. Closed kinetic chain upper extremity stability test (CKCUES test): A reliability study in persons with and without shoulder impingement syndrome. BMC Musculoskeletal Disorders. 2014; 15:1. [DOI:10.1186/1471-2474-15-1] [PMID] [PMCID]
- Gorman PP, Butler RJ, Plisky PJ, Kiesel KB. Upper Quarter Y Balance Test: reliability and performance comparison between genders in active adults. The Journal of Strength & Conditioning Research. 2012; 26(11):3043-8. [DOI:10.1519/JSC.0b013e3182472fdb] [PMID]
- Kamatchi K, Arun B, Tharani G, Yuvarani G, Vaishnavi G, Kaviraja N. Effectss. Biomedicine. 2020; 40(3):377-80. [DOI:10.51248/.v40i3.31]
- Sheikhhassani S, Rajabi R, Minoonejad H. [Effect of core muscle fatigue on measurements of lower extremity functional performance in male athletes (Persian)]. Journal of Research in Rehabilitation Sciences. 2013; 9(4):668-80. [Link]
- Abbasi H, Alizadeh MH, Daneshmandi H, Barati AH. [Comparing the effect of functional, extra-functional and combined exercises on dynamic balance in athletes with functional ankle instability (Persian)]. Studies in Sport Medicine. 2015; 7(17):34-15. [Link]
- Naderi A, Baloochi R, Jabbari F, Eslami R. [Comparison between the effects of core stability exercises and neuromuscular exercises on dynamic balance and lower limb function of athletes with functional ankle instability (Persian)]. Scientific Journal of Kurdistan University of Medical Sciences. 2016; 21(4):61-72. [Link]
Type of Study: Research |
Subject:
General
Received: 2022/12/3 | Accepted: 2023/01/18 | Published: 2022/10/20
Received: 2022/12/3 | Accepted: 2023/01/18 | Published: 2022/10/20
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
