Wed, Jun 10, 2026
Volume 10, Issue 1 (Winter 2020)
PTJ 2020, 10(1): 41-48 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Fakoor Rashid H, Fadaei Dehcheshmeh T, Daneshmandi H, Norasteh A A. Investigating Knee Joint Position Sense After Anterior Cruciate Ligament Reconstruction in Male Soccer Players. PTJ 2020; 10 (1) :41-48
URL: http://ptj.uswr.ac.ir/article-1-426-en.html
URL: http://ptj.uswr.ac.ir/article-1-426-en.html



1- Faculty of Physical Education, Department of Sports Injury and Corrective Exercises, University of Guilan, Guilan, Iran.
Full-Text [PDF 543 kb]
(1897 Downloads)
| Abstract (HTML) (4572 Views)
To passively reproduce the angles by the subject, the speed of the isokinetic device was set at 30°/sec [12]. Descriptive and inferential statistics were used in this research to analyze the collected data. Shapiro-Wilk test was used to examine the normality of data, and the Independent Samples t-test was used for between-group comparisons. Moreover, the significance level for this test was considered at 0.05. SPSS was used to analyze the obtained data.
3. Results
Demographic data (age, height, weight, and sports history) of the study subjects are presented in Table 1.
.jpg)
The present study results revealed that the mean reproduction value of the 30° angle operated knee was significantly higher than that of the non-operated knee (P=0.003). There was no significant difference between the mean scores of 45° angle reproduction in the non-operated and operated knees (P=0.99). Additionally, the mean value of the 60° angle reproduction test in the operated knee was significantly lower than that of the non-operated knee (P=0.01) (Table 2).
.jpg)
In addition, the mean value of a passive reproduction angle test was significantly higher than that of the operated knee at a 30° angle (P=0.001). The difference between the results of passive and active reproduction operated knee tests were significant at a 45° angle; the study subjects demonstrated a higher mean score in the passive reproduction of this angle (P=0.02). There was no significant difference between the test results at a 60° angle in the active and passive reproduction in the operated knee (P=0.22) (Table 3).
.jpg)
Discussion The present research aimed to evaluate the knee joint position sense in the non-operated and operated knees of elite soccer players after the reconstruction of the anterior cruciate ligament. The relevant results revealed a significant difference in the sense of the joint position of the non-operated and operated knees as well as active and passive reproduction tests at some angles. Some studies reported a reduction in proprioception and instability in lower limb joints after an ACL injury. In this regard, Zhang et al. reported that ACL injury reduced the number of proprioception receptors in monkeys, and ultimately, decreased proprioception in them [13]. Moreover, Relph et al. reviewed the studies on reduced proprioception after an ACL injury [14].
They reported a reduction in proprioception following ACL ligament injury. The current study results indicated that the sense of knee joint position of the operated knee was weaker than that of the non-operated knee in elite soccer players after the reconstruction of the ACL. In this regard, Muaidi et al. examined the knee joint proprioception three months after rebuilding the ACL using a single-cut technique with auto-graft of 4-string hamstring tendon in 15 athlete soccer players and skiers with a one-sided tear of the anterior cruciate ligament [15].
They concluded that knee joint proprioception had improved 3 months after rebuilding. Their results are inconsistent with those of the present study. A reason for such inconsistency might be the difference in the time of measurement of knee joint proprioception after reconstruction; the knee joint proprioception was measured three months after the reconstruction in the mentioned study. However, it was measured 6-12 months after the reconstruction in this study. Another reason for this discrepancy might be the differences in statistical samples and the different levels of activity in the subjects of these two studies [15].
Yosmaoglu et al. examined the knee joint proprioception after rebuilding ACL using a hamstring graft in patients with a torn ligament [16]. They revealed no significant improvement in knee joint proprioception 12 months after the reconstruction. These results are consistent with those of the current study. In contrast, a review study by Nakamae et al. suggested no evidence on a difference between the proprioception of the injured group and ACL tear after reconstruction and the non-injured group [17]. Besides, Kaya et al., assessed the effect of knee ACL reconstruction on improving the knee joint proprioception of individuals with a torn ligament [18]. Their results provided contradictory evidence on the effect of the reconstruction of a cruciate ligament on improving knee joints. In these studies, the surgical method was mainly hamstring tendon transplantation or patella tendon transplantation.
Moreover, the time to examine the knee position has been reported 3-6 months in most of these studies. Postoperative time seems to be a key factor involved in improving the sense of joint position in people with ACL tear; the best time to increase the mechanical stability of the ligament and to improve the knee joint position sense has been reported to be 3-6 months [18]. ACL directs the knee movement during non-physiological movements. After the cruciate ligament injury, only a few receptors remain within the articular capsule; such a reduction in the number of receptors results in joint laxity.
After reconstructing, some of the mechanoreceptors improved by restoring mechanical stability, resulting in reduced joint laxity, especially in the more extensive range of physiological movements. However, it fails to resolve this defect completely [19]. Furthermore, according to the phenomenon of remove afferent, spinal reflexes lead to motor nerves and muscular spindles, as well as cortical pathways, i.e., necessary for the conscious and unconscious recognition of proprioception and the sense of joint movement; removing afferent were disrupted following ligament tear and the feedback and the feedforward control was disturbed, and this defect was not compensated even after reconstruction [20]. Muscle receptors, such as muscle spindles and Golgi apparatus, could significantly affect the proprioception. With ACL injury, the lack of afferent information from ACL mechanoreceptors leads to a weaker balance [21].
In this regard, coaches are recommended to gain the required knowledge on the importance and the role of joint position sense, implement the knee joint position sense exercises to improve the joint position sense, and use follow-up exercises to maintain the effectiveness of these exercises.
4. Conclusion
The obtained data revealed that the knee joint position sense of the operated knee joint, compared to the non-operated knee in elite soccer players, along with the reconstruction of the ACL, was weaker than those of the non-operated knee.
Ethical Considerations
Compliance with ethical guidelines
All ethical principles were considered in this article, and all of the study participants provided the written consent.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Authors' contributions
All authors contributed in preparing this article.
Conflict of interest
The authors declared no conflict of interest.
References
Biedert, RM. Contribution of the three levels of nervous system motor control: Spinal cord, lower brain, cerebral cortex. Proprioception and Neuromuscular Control in Joint Stability. 2000; 23-31.
Schultz RA, Miller DC, Kerr CS, Micheli L. Mechanoreceptors in human cruciate ligaments. A histological study. The Journal of Bone and Joint Surgery. American Volume. 1984; 66(7):1072-6. [DOI:10.2106/00004623-198466070-00014] [PMID]
Biedert RM, Stauffer E, Friederich NF. (Occurrence of free nerve endings in the soft tissue of the knee joint. A histologic investigation. The American Journal of Sports Medicine. 1992; 20(4):430-3. [DOI:10.1177/036354659202000411] [PMID]
Jerosch J, Hoffstetter I, Bork H, Bischof M. The influence of orthoses on the proprioception of the ankle joint. Knee Surgery, Sports Traumatology, Arthroscopy. 1995; 3(1):39-46. [DOI:10.1007/BF01553524] [PMID]
Relph N, Herrington L, Tyson S. The effects of ACL injury on knee proprioception: A meta-analysis. Physiotherapy. 2014; 100(3):187-95. [DOI:10.1016/j.physio.2013.11.002] [PMID]
Nagai T, Schilaty ND, Strauss JD, Crowley EM, Hewett TE. Analysis of lower extremity proprioception for anterior cruciate ligament injury prevention: Current opinion. Sports Medicine. 2018; 48(6):1303-9. [DOI:10.1007/s40279-018-0889-1] [PMID] [PMCID]
Park JH, Jeong WK, Lee JH, Cho JJ, Lee DH. Postural stability in patients with anterior cruciate ligament tears with and without medial meniscus tears. Knee Surgery, Sports Traumatology, Arthroscopy. 2015; 23(1):240-5. [DOI:10.1007/s00167-013-2675-9] [PMID]
Fremerey RW, Lobenhoffer P, Zeichen J, Skutek M, Bosch U, Tscherne H. Proprioception after rehabilitation and reconstruction in knees with deficiency of the anterior cruciate ligament: A prospective, longitudinal study. The Journal of Bone and Joint Surgery. British Volume. 2000; 82(6):801-6. [DOI:10.1302/0301-620X.82B6.0820801] [PMID]
Dhillon MS, Prabhakar S, Bali K. No evidence that remnant-preserving anterior cruciate ligament reconstruction ensures better proprioceptive function than a standard single-bundle reconstruction: A systematic review of randomised controlled trials. Journal of ISAKOS: Joint Disorders & Orthopaedic Sports Medicine. 2016; 1(6):316-20. [DOI:10.1136/jisakos-2015-000036]
Relph N, Herrington L. The effect of conservatively treated ACL injury on knee joint position sense. International Journal of Sports Physical Therapy. 2016; 11(4):536-43.
Rahnama N, Reilly T, Lees A, Graham-Smith P. A comparison of musculoskeletal function in elite and sub-elite English soccer players. In: Reilly T, Marfell-Jones M, editors. Kinanthropometry VIII: Proceedings of the 8th International Conference of the International Society for the Advancement of Kinanthropometry (ISAK). Abingdon: Routledge; 2003.
Rashid HF, Zarandi Z, Norashteh AA. Comparison of knee proprioception between congenitally and late blind people. Medicina dello Sport. 2017; 70(1):93-103.
Zhang L, Qi J, Zeng Y, Zhang S, Fu S, Zhou X, et al. Proprioceptive changes in bilateral knee joints following unilateral anterior cruciate ligament injury in cynomolgus monkeys. Medical science monitor: International medical Journal of Experimental and Clinical Research. 2018; 24:105-13. [DOI:10.12659/MSM.905160]
Relph N, Herrington L, Tyson S. The effects of ACL injury on knee proprioception: A meta-analysis. Physiotherapy. 2014; 100(3):187-95. [DOI:10.1016/j.physio.2013.11.002] [PMID]
Muaidi QI, Nicholson LL, Refshauge KM, Adams RD, Roe JP. Effect of anterior cruciate ligament injury and reconstruction on proprioceptive acuity of knee rotation in the transverse plane. The American Journal of Sports Medicine. 2009; 37(8):1618-26. [DOI:10.1177/0363546509332429] [PMID]
Yosmaoğlu HB, Baltacı G, Kaya D, Ozer H, Atay A. Comparison of functional outcomes of two anterior cruciate ligament reconstruction methods with hamstring tendon graft. Acta Orthopaedica et Traumatologica Turcica. 2011; 45(4):240-7. [DOI:10.3944/AOTT.2011.2402] [PMID]
Nakamae A, Adachi N, Ishikawa M, Nakasa T, Ochi M. No evidence of impaired proprioceptive function in subjects with anterior cruciate ligament reconstruction: A systematic review. Journal of ISAKOS: Joint Disorders & Orthopaedic Sports Medicine. 2017; 2(4):191-9. [DOI:10.1136/jisakos-2016-000087]
Kaya D, Calik M, Callaghan MJ, Yosmaoglu B, Doral, MN. Proprioception after knee injury, surgery and rehabilitation. Proprioception in Orthopaedics, Sports Medicine and Rehabilitation. Cham: Springer; 2018. [DOI:10.1007/978-3-319-66640-210]
Georgoulis AD, Ristanis S, Moraiti CO, Paschos N, Zampeli F, Xergia S, et al. ACL injury and reconstruction: Clinical related in vivo biomechanics. Revue de Chirurgie Orthopédique et Traumatologique. 2010; 96(8):S339-48. [DOI:10.1016/j.rcot.2010.09.015]
Bonsfills N, Gómez-Barrena E, Raygoza JJ, Núñez A. Loss of neuromuscular control related to motion in the acutely ACL-injured knee: An experimental study. European Journal of Applied Physiology. 2008; 104(3):567-77. [DOI:10.1007/s00421-008-0729-3] [PMID]
Bonnette S, Diekfuss JA, Grooms DR, Kiefer AW, Riley MA, Riehm C, et al. Electrocortical dynamics differentiate athletes exhibiting low‐and high‐ACL injury risk biomechanics. Psychophysiology. 2020; 57(4):e13530 [DOI:10.1111/psyp.13530] [PMID]
Full-Text: (1992 Views)
1. Introduction
Proprioception involves any position or motion information transmitted by sensory receptors in the muscle, tendon, joint, and even the skin to the central nervous system. It is involved in muscular reflex, joint dynamic stability, and motion planning for neuromuscular control [1]. It provides us information on the position and motion of the knee and significantly impacts muscle control. Ruffini nerve endings, Pacinian corpuscles, and Golgi tendon organs are mechanoreceptors identified in various intra-articular structures of the knee with free nerve endings [2, 3]. Any factor which reduces proprioception may lead to mechanical instability and ultimately increased stress on the joint, which could make it prone to injury. Some of these factors include injury to ligaments, muscle imbalance, the lack of flexibility, aging, overuse injuries, pain, diseases, and fatigue [4]. Anterior Cruciate Ligament (ACL) significantly affects the knee joint proprioception. However, the effect of ACL injury on knee proprioception remains unclear [5].
An ACL injury is the most prevalent knee ligament injury associated with exercising. Its frequency is 36.9 per 100000 individuals, and most of these injuries are of non-collision type [6]. ACL tear is the most common cause of knee treatment in soccer players.
Park et al. explored patients with ACL tear with and without an internal cervical tear; they concluded that the balance of the leg with ACL ligament injury was significantly less than that of the non-injured knee [7]. Thus, the ACL contributes to maintaining the static and dynamic balance and stability, and the coordination of knee joints. Patients may perform their daily living activities without having healthy anterior cruciate ligament. However, most athletes decide to undergo surgery to return to the previous level and improve their physical fitness to an ideal level [7]. The pattern for the recovery of proprioception after reconstruction remains unclear [8]. A review article by Dhillon et al. reported no evidence suggesting that the reconstruction of ACL improves the function of individuals affected by this ligament injury [9].
Fremerey et al. examined the knee joint proprioception after the reconstruction and rehabilitation of ACL. They found that the sense of joint position in the operated knee joint was significantly higher than that of the non-operated knee while performing the single-leg stance test [8]. However, Ralph et al. examined the effect of conservatively treated ACL injury on knee joint position. Knee joint position sense was measured using a seated passive-active reproductive angle technique. The average absolute angle of error score was determined to be 10°-30° of knee flexion. This error score was derived from the difference between the target and repositioning angle.
This study supported that a static proprioceptive deficiency exists in the knee joint following ACL injury and rehabilitation, potentially due to a reduction in functioning mechanoreceptors in the ligament over time [10]. As noted, studies conducted in this area have reported contradictory data. In addition, the role of ACL in the knee joint position sense is essential; however, there is a lack of studies in this area on elite athletes, especially soccer players. Thus, the present study aimed to examine the knee proprioception in the non-operated knee and operated knee after the reconstruction of anterior cruciate ligament among elite soccer players.
2. Materials and Methods
This research was a quasi-experimental study. The study participants were selected using the purposive non-randomized method. The research sample included 20 elite sorcerers in Mashhad City, Iran, with a cruciate ligament injury, who underwent ACL reconstruction in the form of arthroscopic with auto-graft with a patellar ligament.
The inclusion criteria included passing a minimum of 6 months and a maximum of 12 months of surgery, being a soccer player (membership of the Premier League or League 1 club team, performing soccer exercises for at least 3 sessions per week before the injury), the lack of atrophy in the lower limb muscles by the comparison of healthy limbs and inflammation on the knee, complete painless motion range, the lack of knee joint laxity, and significant orthopedic and hematological and neurological injuries in other joints in both operated and healthy limbs. All of these cases were examined by an orthopedic specialist.
To perform the test, the study participants warmed up on a stationary bike without applying resistance (level 3, 60 rpm) for 5 minutes. Then, they performed stretching exercise of knee joint and quadriceps and hamstring muscles [11]. The level of knee joint position sense was measured by angle reconstruction method using an isokinetic device (Gymnex; made in Florence, Italy). The following protocol was performed for accurate measurement of the knee joint position sense.
The subject was held tightly using the seat belt inserted on the seat of the device. The rotation axis of the lever arm of the dynamometer was aligned with the knee rotation axis, and the lever arm cushion was placed on the lower third of the leg after measuring the leg length of the subjects [12]. The study subject was requested to complete perform the knee joint extension motion (the motion limitation of the device was set on 360°).
The complete knee extension degree was read on the monitor screen, and the numbers 30, 45, and 60 were deducted from the number obtained to determine the articular angle reproduction at 30°,45°, and 60° of knee flexion. For example, if the screen of the monitor shows a complete angle extension of the knee joint at 180°, the angles selected for reproduction are 150°, 135°, and 120°, respectively; these are the reconstruction of the articular angle at the considered angles. First, angles’ reproduction was performed at each angle. Then, the study participant rested for 5 minutes to prevent fatigue. This process was repeated 3 times for each angle, and the mean value of them was recorded in a particular form.
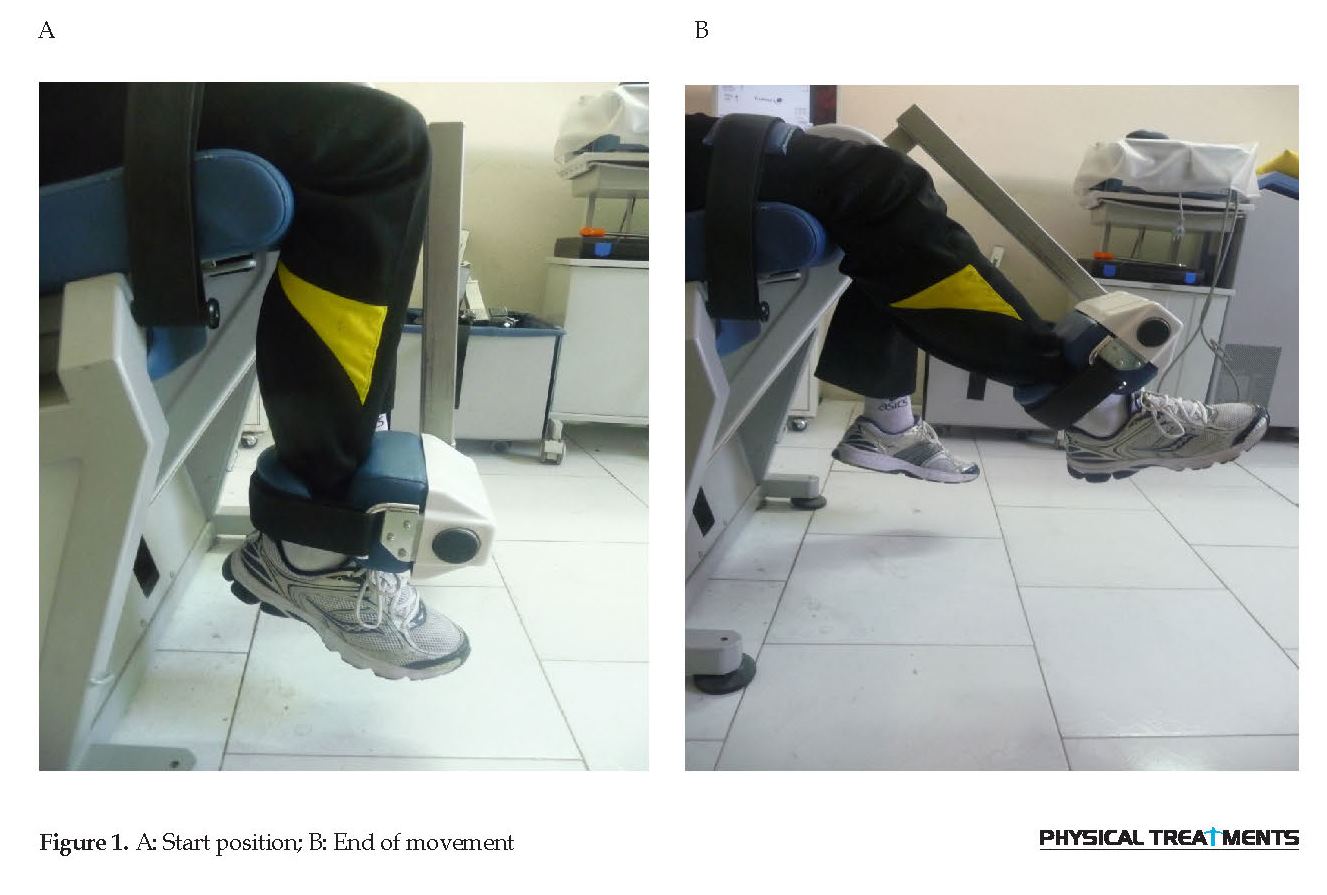
Next, the study subject was requested to detect the angles’ active reproduction by bringing the joint to the target angle and returning the limb to its initial position (angle: 30°). The patient’s limb was moved at a fixed speed, and he was requested to announce it after the knee was brought to the target position. Besides, the study sample was requested to announce it to the researcher again when he felt that the leg had reached the initial angle. At all stages of the test (active and passive), the patient’s eyes were closed, and the angles were reconstructed actively and passively. The reproduction of the angles was respectively 30°, 45°, and 60° of knee flexion to the extension (Figure 1).
Proprioception involves any position or motion information transmitted by sensory receptors in the muscle, tendon, joint, and even the skin to the central nervous system. It is involved in muscular reflex, joint dynamic stability, and motion planning for neuromuscular control [1]. It provides us information on the position and motion of the knee and significantly impacts muscle control. Ruffini nerve endings, Pacinian corpuscles, and Golgi tendon organs are mechanoreceptors identified in various intra-articular structures of the knee with free nerve endings [2, 3]. Any factor which reduces proprioception may lead to mechanical instability and ultimately increased stress on the joint, which could make it prone to injury. Some of these factors include injury to ligaments, muscle imbalance, the lack of flexibility, aging, overuse injuries, pain, diseases, and fatigue [4]. Anterior Cruciate Ligament (ACL) significantly affects the knee joint proprioception. However, the effect of ACL injury on knee proprioception remains unclear [5].
An ACL injury is the most prevalent knee ligament injury associated with exercising. Its frequency is 36.9 per 100000 individuals, and most of these injuries are of non-collision type [6]. ACL tear is the most common cause of knee treatment in soccer players.
Park et al. explored patients with ACL tear with and without an internal cervical tear; they concluded that the balance of the leg with ACL ligament injury was significantly less than that of the non-injured knee [7]. Thus, the ACL contributes to maintaining the static and dynamic balance and stability, and the coordination of knee joints. Patients may perform their daily living activities without having healthy anterior cruciate ligament. However, most athletes decide to undergo surgery to return to the previous level and improve their physical fitness to an ideal level [7]. The pattern for the recovery of proprioception after reconstruction remains unclear [8]. A review article by Dhillon et al. reported no evidence suggesting that the reconstruction of ACL improves the function of individuals affected by this ligament injury [9].
Fremerey et al. examined the knee joint proprioception after the reconstruction and rehabilitation of ACL. They found that the sense of joint position in the operated knee joint was significantly higher than that of the non-operated knee while performing the single-leg stance test [8]. However, Ralph et al. examined the effect of conservatively treated ACL injury on knee joint position. Knee joint position sense was measured using a seated passive-active reproductive angle technique. The average absolute angle of error score was determined to be 10°-30° of knee flexion. This error score was derived from the difference between the target and repositioning angle.
This study supported that a static proprioceptive deficiency exists in the knee joint following ACL injury and rehabilitation, potentially due to a reduction in functioning mechanoreceptors in the ligament over time [10]. As noted, studies conducted in this area have reported contradictory data. In addition, the role of ACL in the knee joint position sense is essential; however, there is a lack of studies in this area on elite athletes, especially soccer players. Thus, the present study aimed to examine the knee proprioception in the non-operated knee and operated knee after the reconstruction of anterior cruciate ligament among elite soccer players.
2. Materials and Methods
This research was a quasi-experimental study. The study participants were selected using the purposive non-randomized method. The research sample included 20 elite sorcerers in Mashhad City, Iran, with a cruciate ligament injury, who underwent ACL reconstruction in the form of arthroscopic with auto-graft with a patellar ligament.
The inclusion criteria included passing a minimum of 6 months and a maximum of 12 months of surgery, being a soccer player (membership of the Premier League or League 1 club team, performing soccer exercises for at least 3 sessions per week before the injury), the lack of atrophy in the lower limb muscles by the comparison of healthy limbs and inflammation on the knee, complete painless motion range, the lack of knee joint laxity, and significant orthopedic and hematological and neurological injuries in other joints in both operated and healthy limbs. All of these cases were examined by an orthopedic specialist.
To perform the test, the study participants warmed up on a stationary bike without applying resistance (level 3, 60 rpm) for 5 minutes. Then, they performed stretching exercise of knee joint and quadriceps and hamstring muscles [11]. The level of knee joint position sense was measured by angle reconstruction method using an isokinetic device (Gymnex; made in Florence, Italy). The following protocol was performed for accurate measurement of the knee joint position sense.
The subject was held tightly using the seat belt inserted on the seat of the device. The rotation axis of the lever arm of the dynamometer was aligned with the knee rotation axis, and the lever arm cushion was placed on the lower third of the leg after measuring the leg length of the subjects [12]. The study subject was requested to complete perform the knee joint extension motion (the motion limitation of the device was set on 360°).
The complete knee extension degree was read on the monitor screen, and the numbers 30, 45, and 60 were deducted from the number obtained to determine the articular angle reproduction at 30°,45°, and 60° of knee flexion. For example, if the screen of the monitor shows a complete angle extension of the knee joint at 180°, the angles selected for reproduction are 150°, 135°, and 120°, respectively; these are the reconstruction of the articular angle at the considered angles. First, angles’ reproduction was performed at each angle. Then, the study participant rested for 5 minutes to prevent fatigue. This process was repeated 3 times for each angle, and the mean value of them was recorded in a particular form.
Next, the study subject was requested to detect the angles’ active reproduction by bringing the joint to the target angle and returning the limb to its initial position (angle: 30°). The patient’s limb was moved at a fixed speed, and he was requested to announce it after the knee was brought to the target position. Besides, the study sample was requested to announce it to the researcher again when he felt that the leg had reached the initial angle. At all stages of the test (active and passive), the patient’s eyes were closed, and the angles were reconstructed actively and passively. The reproduction of the angles was respectively 30°, 45°, and 60° of knee flexion to the extension (Figure 1).
To passively reproduce the angles by the subject, the speed of the isokinetic device was set at 30°/sec [12]. Descriptive and inferential statistics were used in this research to analyze the collected data. Shapiro-Wilk test was used to examine the normality of data, and the Independent Samples t-test was used for between-group comparisons. Moreover, the significance level for this test was considered at 0.05. SPSS was used to analyze the obtained data.
3. Results
Demographic data (age, height, weight, and sports history) of the study subjects are presented in Table 1.
The present study results revealed that the mean reproduction value of the 30° angle operated knee was significantly higher than that of the non-operated knee (P=0.003). There was no significant difference between the mean scores of 45° angle reproduction in the non-operated and operated knees (P=0.99). Additionally, the mean value of the 60° angle reproduction test in the operated knee was significantly lower than that of the non-operated knee (P=0.01) (Table 2).
In addition, the mean value of a passive reproduction angle test was significantly higher than that of the operated knee at a 30° angle (P=0.001). The difference between the results of passive and active reproduction operated knee tests were significant at a 45° angle; the study subjects demonstrated a higher mean score in the passive reproduction of this angle (P=0.02). There was no significant difference between the test results at a 60° angle in the active and passive reproduction in the operated knee (P=0.22) (Table 3).
Discussion The present research aimed to evaluate the knee joint position sense in the non-operated and operated knees of elite soccer players after the reconstruction of the anterior cruciate ligament. The relevant results revealed a significant difference in the sense of the joint position of the non-operated and operated knees as well as active and passive reproduction tests at some angles. Some studies reported a reduction in proprioception and instability in lower limb joints after an ACL injury. In this regard, Zhang et al. reported that ACL injury reduced the number of proprioception receptors in monkeys, and ultimately, decreased proprioception in them [13]. Moreover, Relph et al. reviewed the studies on reduced proprioception after an ACL injury [14].
They reported a reduction in proprioception following ACL ligament injury. The current study results indicated that the sense of knee joint position of the operated knee was weaker than that of the non-operated knee in elite soccer players after the reconstruction of the ACL. In this regard, Muaidi et al. examined the knee joint proprioception three months after rebuilding the ACL using a single-cut technique with auto-graft of 4-string hamstring tendon in 15 athlete soccer players and skiers with a one-sided tear of the anterior cruciate ligament [15].
They concluded that knee joint proprioception had improved 3 months after rebuilding. Their results are inconsistent with those of the present study. A reason for such inconsistency might be the difference in the time of measurement of knee joint proprioception after reconstruction; the knee joint proprioception was measured three months after the reconstruction in the mentioned study. However, it was measured 6-12 months after the reconstruction in this study. Another reason for this discrepancy might be the differences in statistical samples and the different levels of activity in the subjects of these two studies [15].
Yosmaoglu et al. examined the knee joint proprioception after rebuilding ACL using a hamstring graft in patients with a torn ligament [16]. They revealed no significant improvement in knee joint proprioception 12 months after the reconstruction. These results are consistent with those of the current study. In contrast, a review study by Nakamae et al. suggested no evidence on a difference between the proprioception of the injured group and ACL tear after reconstruction and the non-injured group [17]. Besides, Kaya et al., assessed the effect of knee ACL reconstruction on improving the knee joint proprioception of individuals with a torn ligament [18]. Their results provided contradictory evidence on the effect of the reconstruction of a cruciate ligament on improving knee joints. In these studies, the surgical method was mainly hamstring tendon transplantation or patella tendon transplantation.
Moreover, the time to examine the knee position has been reported 3-6 months in most of these studies. Postoperative time seems to be a key factor involved in improving the sense of joint position in people with ACL tear; the best time to increase the mechanical stability of the ligament and to improve the knee joint position sense has been reported to be 3-6 months [18]. ACL directs the knee movement during non-physiological movements. After the cruciate ligament injury, only a few receptors remain within the articular capsule; such a reduction in the number of receptors results in joint laxity.
After reconstructing, some of the mechanoreceptors improved by restoring mechanical stability, resulting in reduced joint laxity, especially in the more extensive range of physiological movements. However, it fails to resolve this defect completely [19]. Furthermore, according to the phenomenon of remove afferent, spinal reflexes lead to motor nerves and muscular spindles, as well as cortical pathways, i.e., necessary for the conscious and unconscious recognition of proprioception and the sense of joint movement; removing afferent were disrupted following ligament tear and the feedback and the feedforward control was disturbed, and this defect was not compensated even after reconstruction [20]. Muscle receptors, such as muscle spindles and Golgi apparatus, could significantly affect the proprioception. With ACL injury, the lack of afferent information from ACL mechanoreceptors leads to a weaker balance [21].
In this regard, coaches are recommended to gain the required knowledge on the importance and the role of joint position sense, implement the knee joint position sense exercises to improve the joint position sense, and use follow-up exercises to maintain the effectiveness of these exercises.
4. Conclusion
The obtained data revealed that the knee joint position sense of the operated knee joint, compared to the non-operated knee in elite soccer players, along with the reconstruction of the ACL, was weaker than those of the non-operated knee.
Ethical Considerations
Compliance with ethical guidelines
All ethical principles were considered in this article, and all of the study participants provided the written consent.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Authors' contributions
All authors contributed in preparing this article.
Conflict of interest
The authors declared no conflict of interest.
References
Biedert, RM. Contribution of the three levels of nervous system motor control: Spinal cord, lower brain, cerebral cortex. Proprioception and Neuromuscular Control in Joint Stability. 2000; 23-31.
Schultz RA, Miller DC, Kerr CS, Micheli L. Mechanoreceptors in human cruciate ligaments. A histological study. The Journal of Bone and Joint Surgery. American Volume. 1984; 66(7):1072-6. [DOI:10.2106/00004623-198466070-00014] [PMID]
Biedert RM, Stauffer E, Friederich NF. (Occurrence of free nerve endings in the soft tissue of the knee joint. A histologic investigation. The American Journal of Sports Medicine. 1992; 20(4):430-3. [DOI:10.1177/036354659202000411] [PMID]
Jerosch J, Hoffstetter I, Bork H, Bischof M. The influence of orthoses on the proprioception of the ankle joint. Knee Surgery, Sports Traumatology, Arthroscopy. 1995; 3(1):39-46. [DOI:10.1007/BF01553524] [PMID]
Relph N, Herrington L, Tyson S. The effects of ACL injury on knee proprioception: A meta-analysis. Physiotherapy. 2014; 100(3):187-95. [DOI:10.1016/j.physio.2013.11.002] [PMID]
Nagai T, Schilaty ND, Strauss JD, Crowley EM, Hewett TE. Analysis of lower extremity proprioception for anterior cruciate ligament injury prevention: Current opinion. Sports Medicine. 2018; 48(6):1303-9. [DOI:10.1007/s40279-018-0889-1] [PMID] [PMCID]
Park JH, Jeong WK, Lee JH, Cho JJ, Lee DH. Postural stability in patients with anterior cruciate ligament tears with and without medial meniscus tears. Knee Surgery, Sports Traumatology, Arthroscopy. 2015; 23(1):240-5. [DOI:10.1007/s00167-013-2675-9] [PMID]
Fremerey RW, Lobenhoffer P, Zeichen J, Skutek M, Bosch U, Tscherne H. Proprioception after rehabilitation and reconstruction in knees with deficiency of the anterior cruciate ligament: A prospective, longitudinal study. The Journal of Bone and Joint Surgery. British Volume. 2000; 82(6):801-6. [DOI:10.1302/0301-620X.82B6.0820801] [PMID]
Dhillon MS, Prabhakar S, Bali K. No evidence that remnant-preserving anterior cruciate ligament reconstruction ensures better proprioceptive function than a standard single-bundle reconstruction: A systematic review of randomised controlled trials. Journal of ISAKOS: Joint Disorders & Orthopaedic Sports Medicine. 2016; 1(6):316-20. [DOI:10.1136/jisakos-2015-000036]
Relph N, Herrington L. The effect of conservatively treated ACL injury on knee joint position sense. International Journal of Sports Physical Therapy. 2016; 11(4):536-43.
Rahnama N, Reilly T, Lees A, Graham-Smith P. A comparison of musculoskeletal function in elite and sub-elite English soccer players. In: Reilly T, Marfell-Jones M, editors. Kinanthropometry VIII: Proceedings of the 8th International Conference of the International Society for the Advancement of Kinanthropometry (ISAK). Abingdon: Routledge; 2003.
Rashid HF, Zarandi Z, Norashteh AA. Comparison of knee proprioception between congenitally and late blind people. Medicina dello Sport. 2017; 70(1):93-103.
Zhang L, Qi J, Zeng Y, Zhang S, Fu S, Zhou X, et al. Proprioceptive changes in bilateral knee joints following unilateral anterior cruciate ligament injury in cynomolgus monkeys. Medical science monitor: International medical Journal of Experimental and Clinical Research. 2018; 24:105-13. [DOI:10.12659/MSM.905160]
Relph N, Herrington L, Tyson S. The effects of ACL injury on knee proprioception: A meta-analysis. Physiotherapy. 2014; 100(3):187-95. [DOI:10.1016/j.physio.2013.11.002] [PMID]
Muaidi QI, Nicholson LL, Refshauge KM, Adams RD, Roe JP. Effect of anterior cruciate ligament injury and reconstruction on proprioceptive acuity of knee rotation in the transverse plane. The American Journal of Sports Medicine. 2009; 37(8):1618-26. [DOI:10.1177/0363546509332429] [PMID]
Yosmaoğlu HB, Baltacı G, Kaya D, Ozer H, Atay A. Comparison of functional outcomes of two anterior cruciate ligament reconstruction methods with hamstring tendon graft. Acta Orthopaedica et Traumatologica Turcica. 2011; 45(4):240-7. [DOI:10.3944/AOTT.2011.2402] [PMID]
Nakamae A, Adachi N, Ishikawa M, Nakasa T, Ochi M. No evidence of impaired proprioceptive function in subjects with anterior cruciate ligament reconstruction: A systematic review. Journal of ISAKOS: Joint Disorders & Orthopaedic Sports Medicine. 2017; 2(4):191-9. [DOI:10.1136/jisakos-2016-000087]
Kaya D, Calik M, Callaghan MJ, Yosmaoglu B, Doral, MN. Proprioception after knee injury, surgery and rehabilitation. Proprioception in Orthopaedics, Sports Medicine and Rehabilitation. Cham: Springer; 2018. [DOI:10.1007/978-3-319-66640-210]
Georgoulis AD, Ristanis S, Moraiti CO, Paschos N, Zampeli F, Xergia S, et al. ACL injury and reconstruction: Clinical related in vivo biomechanics. Revue de Chirurgie Orthopédique et Traumatologique. 2010; 96(8):S339-48. [DOI:10.1016/j.rcot.2010.09.015]
Bonsfills N, Gómez-Barrena E, Raygoza JJ, Núñez A. Loss of neuromuscular control related to motion in the acutely ACL-injured knee: An experimental study. European Journal of Applied Physiology. 2008; 104(3):567-77. [DOI:10.1007/s00421-008-0729-3] [PMID]
Bonnette S, Diekfuss JA, Grooms DR, Kiefer AW, Riley MA, Riehm C, et al. Electrocortical dynamics differentiate athletes exhibiting low‐and high‐ACL injury risk biomechanics. Psychophysiology. 2020; 57(4):e13530 [DOI:10.1111/psyp.13530] [PMID]
Type of Study: Research |
Subject:
Sport injury and corrective exercises
Received: 2019/08/18 | Accepted: 2020/01/1 | Published: 2020/05/31
Received: 2019/08/18 | Accepted: 2020/01/1 | Published: 2020/05/31
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
