Mon, Jul 27, 2026
Volume 7, Issue 4 (Winter 2018)
PTJ 2018, 7(4): 205-214 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Fatahi F, Mongashti Joni Y, Najafi A, Hossein Pour E. Investigating Tibialis Anterior Muscle Activity Levels in Patients With Genu Varum During Single-Leg Jump-Landing Task. PTJ 2018; 7 (4) :205-214
URL: http://ptj.uswr.ac.ir/article-1-293-en.html
URL: http://ptj.uswr.ac.ir/article-1-293-en.html



1- Department of Sport Injuries and Corrective Exercises, Faculty of Physical Education and Sport Sciences, University of Isfahan, Isfahan, Iran.
2- Department of Sport Management, Faculty of Sport Sciences, Urmia University, Urmia, Iran.
3- Department of Physical Education and Sport Sciences, Faculty of Physical Education and Sport Sciences, University of Isfahan, Isfahan, Iran.
4- Department of Sport Management, Faculty of Physical Education and Sports Sciences, University of Tehran, Tehran, Iran.
2- Department of Sport Management, Faculty of Sport Sciences, Urmia University, Urmia, Iran.
3- Department of Physical Education and Sport Sciences, Faculty of Physical Education and Sport Sciences, University of Isfahan, Isfahan, Iran.
4- Department of Sport Management, Faculty of Physical Education and Sports Sciences, University of Tehran, Tehran, Iran.
Full-Text [PDF 643 kb]
(2538 Downloads)
| Abstract (HTML) (8969 Views)


Full-Text: (4074 Views)
1. Introduction
Postural control is the ability to maintain balance in the center of gravity area [1]. Studies indicate that postural control may be affected by genu varum disorder through created torque pronation in the ankle and foot joints [2], which can lead to a change in postural control [3]. Genu varum is one of the most frequent lower limb abnormalities. In normal standing status, the center of gravity line or lower limb mechanical axis passes through the center of the knee joint, so that the weight is approximately and evenly divided between the inner and outer parts of the knee [4].
The genu varum causes change in the force applied to the knee and makes the weight bearing line move to the inner side of the knee [5]. Abnormality of the genu varum also changes the foot posture, increases the pronation torque of subtalar joint during contact with the ground, and increases the postural sway [2, 6]. Previous studies indicate that people with genu varum have a weak stability. Nyland et al. reported that genu varum abnormality would affect the location of the pressure center and postural control during one-leg standing. People with this abnormality use different postural dynamic control strategies during single-leg standing [7]. Sama’ei et al. also reported that genu varum abnormality increases postural sway in the mediolateral direction in both static and dynamic modes, compared to those with normal knee [8].
Besides the effect of anatomical orientation on stability, another factor influencing stability is muscular activity. Muscles play an important role in stability and balance control [9, 10]. When the relationship between muscle function and stability is considered, the muscles around the knee are usually investigated [11, 12]. However, the structure of the lower extremity distal muscles can play an important role in maintaining stability. Studies indicate that the muscles around the leg such as tibialis anterior muscle are important in balance, especially in single-leg movements [13, 14].
Individuals use different balance strategies when performing balance movements. The afferent nerves of the ankle, knee, and thigh are responsible for starting the postural control through three different movement strategies. There are several well-known strategies for maintaining balance [15]. The most commonly used strategies are ankle, hip, thigh and stepping [16]. Ankle strategy is used in slow and small disturbances on flat surfaces. The order of muscular activity starts from distal section (ankle muscles) towards proximal section (thigh and trunk muscles).
This is the most effective and most commonly used strategy and is applied when the center of gravity is within the limits of stability. Therefore, the ineffectiveness or weakness of the leg muscles during the movements may affect stability. Because genu varum abnormality is a change that occurs in the lower extremity, it seems possible that the activity of the leg muscles like the tibialis anterior muscle in patients with this abnormality changes in order to maintain balance. Unfortunately, no study has been conducted in this regard. Therefore, the present study aimed to investigate the level of activity of tibialis anterior muscle in people with genu varum during the one-leg jump-landing task.
2. Materials and Methods
Study subjects
This was a descriptive and quasi-experimental study. The statistical population included all male students of Physical Education Faculty of Tarbiat Moallem University, studying during 2013-2014 academic year. The statistical sample included 28 people (Mean±SD age: 21.53±1.65 y, weight: 66.76±7.51 kg, height: 173.38±4.54 cm) in the two groups of the genu varum (14 people) and normal knee (14 people). Subjects were selected by non-random purposive sampling method.
Subjects with the history of neuromuscular skeletal disorders, history of operation or fracture in the lower extremity over the past year, and other lower limb abnormalities were excluded from the study. All tests were conducted in Biomechanics and Corrective Movements laboratory of Tehran University of Tarbiat Moallem. To evaluate the genu varum, the subjects were asked to stand against the wall bare feet and in anatomical condition with the back, hips and heels of both feet stuck to the wall. Then, the subjects were asked to put their feet together. If the distance between their two knee epicondyles was more than 3 cm, they were considered as a case of genu varum [8]. The subjects were assigned to each group according to their knee conditions.
Data collection
Study tools
Triaxial force plate (Model 4060 NC, Beterc Inc; Columbus, OH) was used for recording and measuring ground reaction force. Ground reaction force was used to detect the first contact of the foot with the ground. Data of ground reaction forces were recorded by the force plate at 200 Hz sampling frequency [17]. Sargent jump digital device was used to measure the maximum vertical jump. Electromyographic data of tibialis anterior muscle was collected using an Electromyography (EMG) (CT8 model, MIE Medical Research Ltd, UK). This data was collected at 1000 Hz sampling frequency [18]. For simultaneous data collection, the EMG was synchronized with the force plate.
Test run method
Preparing the subjects: After measuring and recording descriptive data of subjects, skin surface hair of anterior tibialis was shaved and then the skin was cleansed with alcohol. Then, the bipolar surface (Ag/AgCl) electrodes with a diameter of 10 mm and center-to-center distance of 2 cm were placed on the anterior leg calf muscle ventricle. Electrodes were placed on the muscle ventricle of the dominant foot, parallel to the direction of muscle fiber at one third of the distance between the fibula head and tip the ankle malleolus [19]. The electrodes were attached to the skin with adhesive to fix the location of the electrodes during the test. We were mostly concerned that the electrodes were placed on the skin with no movements. To check the correct location of the electrode, EMG muscle signals were evaluated during manual muscle testing.
Jump-landing protocol: To perform the jump-landing task on the force plate, first 50% maximum height jump of the subject must be calculated. For this purpose, the subjects performed maximum vertical jump by using the Sargent jump digital device. The subjects stood under the Sargent jump device and rose their hands to their maximum possible height without the heels coming off the ground. This measure was considered as the standing height of the subjects. Then, the subjects were asked to perform the maximum jump and land on two feet.
This height was recorded as maximum vertical jump and each subject was asked to perform a vertical jump 3 times, and the maximum score of 3 jumps was recorded as the maximum vertical jump of the subjects. After this step, maximal voluntary isometric contraction test of the tibialis anterior muscle was taken to normalize the electromyographic data. To test the maximum contraction of the tibialis anterior muscle, the subjects were asked to sit on a chair in without relying on the back of the chair, and keep the dominant leg knee in extension mode, ankle in plantar flexion mode, and the other leg in 90º flexion. In the meantime, the examiner applied resistance on the back of the foot in order to prevent foot dorsiflexion.
Then the subjects performed the jump-landing task. After measuring the maximum vertical jump of subjects and testing maximal voluntary contraction, the subjects were prepared for the jump-landing task. The maximum height jump of the subject was divided by 2 to calculate 50% of the maximum height jump of the subject. Then, a mark was placed on the 50% of the maximum height jump of subjects, next to the force plate device. The subjects were asked to stand with bare feet behind the mark, at 70 cm from the center of the force plate [20].
Then, they were asked to jump with 2 feet and touch the mark of 50% of the maximum height jump with one hand and land on the force plate on the dominant foot. The dominant foot was the one used by subjects to throw the ball. Upon landing on the force plate, the subjects were trained to put their hands on the pelvic area, hold their heads high, look before, and stand motionless for 20 seconds [21]. If the subject hoped on the force plate or touched the force plate with the other leg or did not touch the sign of 50% of maximum height jump, that jump would be removed from analysis. Before executing the protocol, the subjects were allowed to practice the landing jump several times to get familiar with the conditions and procedures for conducting the test.
Overall, the subjects needed to jump 3-5 times to get familiar with the protocol. Each subject performed the jump-landing task 3 times. In order to prevent fatigue, 2 minutes of rest was given between each jump. The obtained data on ground reaction forces were registered by force plate and at the same time EMG data of the tibialis anterior muscle was recorded, too.
Data analysis
EMG data were processed by MATLB mathematical software (Mathworks software, version 7.12.0, R2011a). The RMS calculation method was used for the analysis of electromagnetic waves. RMS electromyography data were obtained to demonstrate muscular activity during single-leg jump-landing task, at 100 ms before [22] and 200 ms after the initial contact of the foot with the ground [18]. Initial contact of the ground was defined as the time when the force plate shows the vertical component of ground reaction force [23]. RMS was taken also from the maximal isometric voluntary contraction data at the same interval (100 and 200 ms). Then RMS before and after contacting the ground, was normalized by divided over RMS of the maximal isometric voluntary contraction.
Time to stabilization
MATLAB was used to calculate the stabilization time. The medial-lateral and anterior-posterior stability time were calculated using the range variation method defined by Rose et al. [24]. To calculate the stabilization using response forces, at first two intervals of 5-10, 10-15 seconds were considered. Then, the range of these 2 intervals, which included changes in response forces, was
Postural control is the ability to maintain balance in the center of gravity area [1]. Studies indicate that postural control may be affected by genu varum disorder through created torque pronation in the ankle and foot joints [2], which can lead to a change in postural control [3]. Genu varum is one of the most frequent lower limb abnormalities. In normal standing status, the center of gravity line or lower limb mechanical axis passes through the center of the knee joint, so that the weight is approximately and evenly divided between the inner and outer parts of the knee [4].
The genu varum causes change in the force applied to the knee and makes the weight bearing line move to the inner side of the knee [5]. Abnormality of the genu varum also changes the foot posture, increases the pronation torque of subtalar joint during contact with the ground, and increases the postural sway [2, 6]. Previous studies indicate that people with genu varum have a weak stability. Nyland et al. reported that genu varum abnormality would affect the location of the pressure center and postural control during one-leg standing. People with this abnormality use different postural dynamic control strategies during single-leg standing [7]. Sama’ei et al. also reported that genu varum abnormality increases postural sway in the mediolateral direction in both static and dynamic modes, compared to those with normal knee [8].
Besides the effect of anatomical orientation on stability, another factor influencing stability is muscular activity. Muscles play an important role in stability and balance control [9, 10]. When the relationship between muscle function and stability is considered, the muscles around the knee are usually investigated [11, 12]. However, the structure of the lower extremity distal muscles can play an important role in maintaining stability. Studies indicate that the muscles around the leg such as tibialis anterior muscle are important in balance, especially in single-leg movements [13, 14].
Individuals use different balance strategies when performing balance movements. The afferent nerves of the ankle, knee, and thigh are responsible for starting the postural control through three different movement strategies. There are several well-known strategies for maintaining balance [15]. The most commonly used strategies are ankle, hip, thigh and stepping [16]. Ankle strategy is used in slow and small disturbances on flat surfaces. The order of muscular activity starts from distal section (ankle muscles) towards proximal section (thigh and trunk muscles).
This is the most effective and most commonly used strategy and is applied when the center of gravity is within the limits of stability. Therefore, the ineffectiveness or weakness of the leg muscles during the movements may affect stability. Because genu varum abnormality is a change that occurs in the lower extremity, it seems possible that the activity of the leg muscles like the tibialis anterior muscle in patients with this abnormality changes in order to maintain balance. Unfortunately, no study has been conducted in this regard. Therefore, the present study aimed to investigate the level of activity of tibialis anterior muscle in people with genu varum during the one-leg jump-landing task.
2. Materials and Methods
Study subjects
This was a descriptive and quasi-experimental study. The statistical population included all male students of Physical Education Faculty of Tarbiat Moallem University, studying during 2013-2014 academic year. The statistical sample included 28 people (Mean±SD age: 21.53±1.65 y, weight: 66.76±7.51 kg, height: 173.38±4.54 cm) in the two groups of the genu varum (14 people) and normal knee (14 people). Subjects were selected by non-random purposive sampling method.
Subjects with the history of neuromuscular skeletal disorders, history of operation or fracture in the lower extremity over the past year, and other lower limb abnormalities were excluded from the study. All tests were conducted in Biomechanics and Corrective Movements laboratory of Tehran University of Tarbiat Moallem. To evaluate the genu varum, the subjects were asked to stand against the wall bare feet and in anatomical condition with the back, hips and heels of both feet stuck to the wall. Then, the subjects were asked to put their feet together. If the distance between their two knee epicondyles was more than 3 cm, they were considered as a case of genu varum [8]. The subjects were assigned to each group according to their knee conditions.
Data collection
Study tools
Triaxial force plate (Model 4060 NC, Beterc Inc; Columbus, OH) was used for recording and measuring ground reaction force. Ground reaction force was used to detect the first contact of the foot with the ground. Data of ground reaction forces were recorded by the force plate at 200 Hz sampling frequency [17]. Sargent jump digital device was used to measure the maximum vertical jump. Electromyographic data of tibialis anterior muscle was collected using an Electromyography (EMG) (CT8 model, MIE Medical Research Ltd, UK). This data was collected at 1000 Hz sampling frequency [18]. For simultaneous data collection, the EMG was synchronized with the force plate.
Test run method
Preparing the subjects: After measuring and recording descriptive data of subjects, skin surface hair of anterior tibialis was shaved and then the skin was cleansed with alcohol. Then, the bipolar surface (Ag/AgCl) electrodes with a diameter of 10 mm and center-to-center distance of 2 cm were placed on the anterior leg calf muscle ventricle. Electrodes were placed on the muscle ventricle of the dominant foot, parallel to the direction of muscle fiber at one third of the distance between the fibula head and tip the ankle malleolus [19]. The electrodes were attached to the skin with adhesive to fix the location of the electrodes during the test. We were mostly concerned that the electrodes were placed on the skin with no movements. To check the correct location of the electrode, EMG muscle signals were evaluated during manual muscle testing.
Jump-landing protocol: To perform the jump-landing task on the force plate, first 50% maximum height jump of the subject must be calculated. For this purpose, the subjects performed maximum vertical jump by using the Sargent jump digital device. The subjects stood under the Sargent jump device and rose their hands to their maximum possible height without the heels coming off the ground. This measure was considered as the standing height of the subjects. Then, the subjects were asked to perform the maximum jump and land on two feet.
This height was recorded as maximum vertical jump and each subject was asked to perform a vertical jump 3 times, and the maximum score of 3 jumps was recorded as the maximum vertical jump of the subjects. After this step, maximal voluntary isometric contraction test of the tibialis anterior muscle was taken to normalize the electromyographic data. To test the maximum contraction of the tibialis anterior muscle, the subjects were asked to sit on a chair in without relying on the back of the chair, and keep the dominant leg knee in extension mode, ankle in plantar flexion mode, and the other leg in 90º flexion. In the meantime, the examiner applied resistance on the back of the foot in order to prevent foot dorsiflexion.
Then the subjects performed the jump-landing task. After measuring the maximum vertical jump of subjects and testing maximal voluntary contraction, the subjects were prepared for the jump-landing task. The maximum height jump of the subject was divided by 2 to calculate 50% of the maximum height jump of the subject. Then, a mark was placed on the 50% of the maximum height jump of subjects, next to the force plate device. The subjects were asked to stand with bare feet behind the mark, at 70 cm from the center of the force plate [20].
Then, they were asked to jump with 2 feet and touch the mark of 50% of the maximum height jump with one hand and land on the force plate on the dominant foot. The dominant foot was the one used by subjects to throw the ball. Upon landing on the force plate, the subjects were trained to put their hands on the pelvic area, hold their heads high, look before, and stand motionless for 20 seconds [21]. If the subject hoped on the force plate or touched the force plate with the other leg or did not touch the sign of 50% of maximum height jump, that jump would be removed from analysis. Before executing the protocol, the subjects were allowed to practice the landing jump several times to get familiar with the conditions and procedures for conducting the test.
Overall, the subjects needed to jump 3-5 times to get familiar with the protocol. Each subject performed the jump-landing task 3 times. In order to prevent fatigue, 2 minutes of rest was given between each jump. The obtained data on ground reaction forces were registered by force plate and at the same time EMG data of the tibialis anterior muscle was recorded, too.
Data analysis
EMG data were processed by MATLB mathematical software (Mathworks software, version 7.12.0, R2011a). The RMS calculation method was used for the analysis of electromagnetic waves. RMS electromyography data were obtained to demonstrate muscular activity during single-leg jump-landing task, at 100 ms before [22] and 200 ms after the initial contact of the foot with the ground [18]. Initial contact of the ground was defined as the time when the force plate shows the vertical component of ground reaction force [23]. RMS was taken also from the maximal isometric voluntary contraction data at the same interval (100 and 200 ms). Then RMS before and after contacting the ground, was normalized by divided over RMS of the maximal isometric voluntary contraction.
Time to stabilization
MATLAB was used to calculate the stabilization time. The medial-lateral and anterior-posterior stability time were calculated using the range variation method defined by Rose et al. [24]. To calculate the stabilization using response forces, at first two intervals of 5-10, 10-15 seconds were considered. Then, the range of these 2 intervals, which included changes in response forces, was
calculated and the smaller time range of response forces was selected as the time period in which the subject has a favorable stability.
The largest number of this time interval was equivalent to the horizontal line applied to the response forces. In fact, this horizontal line represents the subject’s stable state. Then, the response force information was set one way and from the maximum response point a cubic polynomial graph was plotted on the components of the response force. Time to stabilization in each component of the reaction force, was a point that cubic polynomial graph intersects the horizontal line.
The exact calculation of the time to stabilization was carried out as follows: the polynomial formula obtained from the cubic polynomial graph was set equivalent to the horizontal number placed on the response forces. By solving this cubic polynomial function using MATLAB software, the time to stabilization was accurately calculated. The variation range of ground reaction forces was calculated within the last 10-second part of standing in the single-leg jump-landing task for medial-lateral and anterior-posterior components.
To control the weight variable, response forces in both directions were divided on the weight of the subject and considered as a reference variable. Horizontal variation range line, which shows the smallest amount of full range component of the ground reaction force, was drawn on the data. Then the cubic polynomial graph was plotted. Time to stabilization in each component of the reaction force was the point which cubic polynomial graph intersected the horizontal variation range line (Figure 1).
Time to stabilization in each 3 times subject’s performance was calculated in Medial-Lateral Time to Stabilization (MLTTS) and Anterior-Posterior Time to Stabilization (APTTS). Then, the average time in 3 runs was recorded as the time to stabilization of the subject in that direction. After calculation of both APTTS and MLTTS, the Resultant Vector Time to Stabilization (RVTTS) was calculated using Formula (1):

Although APTTS and MLTTS are usually reported separately, recently the time to reach the overall stability is reported in order to provide an overall stability assessment from both movement planes [24]. It is believed that overall stability index is the best determinant of the general ability of individuals to maintain balance [25]. Mean scores of RVTTS were calculated for each subject.
EMG data were processed by MATLAB software. RMS methods were used to analyze raw EMG waves. RMS EMG data were obtained to show the muscles activities during one-leg jump-landing from 100 ms before [26] to 200 ms after the initial contact of the foot with the ground [27].Time interval was selected as 100 ms before and 200 ms after landing, because pre-landing muscular activity is a predictive measure of muscle contraction. Before the foot contact with the ground in the landing motion, the muscles of the lower limbs are activated to absorb the forces applied at the time of contact. In order to reduce the amount of ground reaction forces, the body should predict landing and prepare itself for it. This is achieved through muscle contraction. The inability of the body to produce external contractions and prediction of lower limb muscles significantly increases ground reaction forces and the stabilization time.
Initial ground contact was defined as the time when force plate showed vertical component of ground reaction force [28]. RMS was obtained from the maximal isometric voluntary contraction data at the same time interval (100 and 200 ms). Then, RMS before and after the contact was normalized by being divided over RMS of maximal isometric voluntary contraction. EMG data was filtered using high-pass and low-pass filters.
Statistical analysis
The t test statistics method was used to compare muscular activity level of the 2 groups. SPSS V. 19 was used for data analysis. P≤0.05 was set as significant for all statistical tests.
3. Results
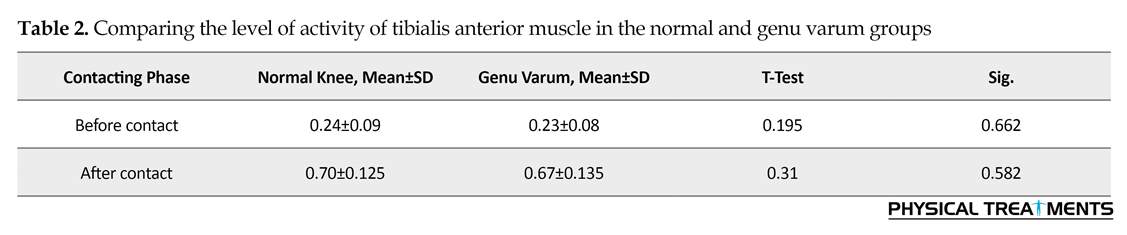
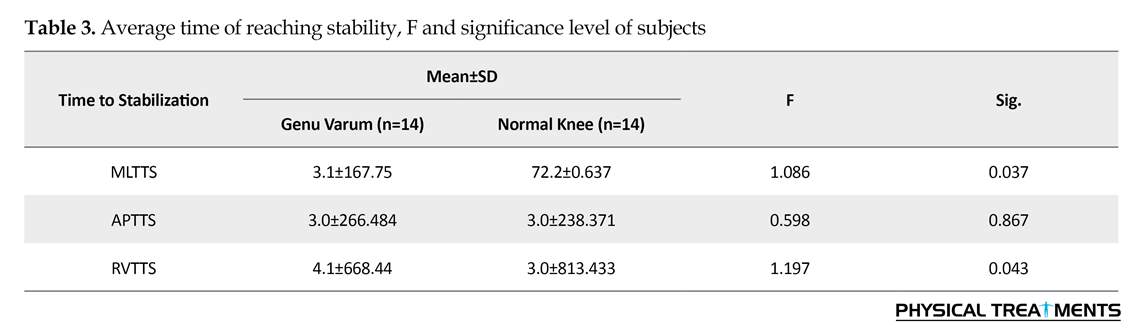
There was no significant differences in the demographic data of the subjects including age, height and weight (Table 1). The activity level of tibialis anterior muscle 100 ms before and 200 ms after initial contact in normal knee group was not significantly higher than that in the genu varum group (P>0.05) (Table 2). Moreover, the activity level of tibialis anterior muscle in both groups after initial contact was significantly higher than before the initial contact. Comparing values of reaching the stability time showed no significant differences between the 2 groups in anterior-posterior direction (P>0.05) (Table 2). However, the medial-lateral and resultant vector time to stabilization in the genu varum group was significantly higher than those in normal knee group (P<0.05) (Table 3).
The largest number of this time interval was equivalent to the horizontal line applied to the response forces. In fact, this horizontal line represents the subject’s stable state. Then, the response force information was set one way and from the maximum response point a cubic polynomial graph was plotted on the components of the response force. Time to stabilization in each component of the reaction force, was a point that cubic polynomial graph intersects the horizontal line.
The exact calculation of the time to stabilization was carried out as follows: the polynomial formula obtained from the cubic polynomial graph was set equivalent to the horizontal number placed on the response forces. By solving this cubic polynomial function using MATLAB software, the time to stabilization was accurately calculated. The variation range of ground reaction forces was calculated within the last 10-second part of standing in the single-leg jump-landing task for medial-lateral and anterior-posterior components.
To control the weight variable, response forces in both directions were divided on the weight of the subject and considered as a reference variable. Horizontal variation range line, which shows the smallest amount of full range component of the ground reaction force, was drawn on the data. Then the cubic polynomial graph was plotted. Time to stabilization in each component of the reaction force was the point which cubic polynomial graph intersected the horizontal variation range line (Figure 1).
Time to stabilization in each 3 times subject’s performance was calculated in Medial-Lateral Time to Stabilization (MLTTS) and Anterior-Posterior Time to Stabilization (APTTS). Then, the average time in 3 runs was recorded as the time to stabilization of the subject in that direction. After calculation of both APTTS and MLTTS, the Resultant Vector Time to Stabilization (RVTTS) was calculated using Formula (1):
Although APTTS and MLTTS are usually reported separately, recently the time to reach the overall stability is reported in order to provide an overall stability assessment from both movement planes [24]. It is believed that overall stability index is the best determinant of the general ability of individuals to maintain balance [25]. Mean scores of RVTTS were calculated for each subject.
EMG data were processed by MATLAB software. RMS methods were used to analyze raw EMG waves. RMS EMG data were obtained to show the muscles activities during one-leg jump-landing from 100 ms before [26] to 200 ms after the initial contact of the foot with the ground [27].Time interval was selected as 100 ms before and 200 ms after landing, because pre-landing muscular activity is a predictive measure of muscle contraction. Before the foot contact with the ground in the landing motion, the muscles of the lower limbs are activated to absorb the forces applied at the time of contact. In order to reduce the amount of ground reaction forces, the body should predict landing and prepare itself for it. This is achieved through muscle contraction. The inability of the body to produce external contractions and prediction of lower limb muscles significantly increases ground reaction forces and the stabilization time.
Initial ground contact was defined as the time when force plate showed vertical component of ground reaction force [28]. RMS was obtained from the maximal isometric voluntary contraction data at the same time interval (100 and 200 ms). Then, RMS before and after the contact was normalized by being divided over RMS of maximal isometric voluntary contraction. EMG data was filtered using high-pass and low-pass filters.
Statistical analysis
The t test statistics method was used to compare muscular activity level of the 2 groups. SPSS V. 19 was used for data analysis. P≤0.05 was set as significant for all statistical tests.
3. Results
There was no significant differences in the demographic data of the subjects including age, height and weight (Table 1). The activity level of tibialis anterior muscle 100 ms before and 200 ms after initial contact in normal knee group was not significantly higher than that in the genu varum group (P>0.05) (Table 2). Moreover, the activity level of tibialis anterior muscle in both groups after initial contact was significantly higher than before the initial contact. Comparing values of reaching the stability time showed no significant differences between the 2 groups in anterior-posterior direction (P>0.05) (Table 2). However, the medial-lateral and resultant vector time to stabilization in the genu varum group was significantly higher than those in normal knee group (P<0.05) (Table 3).
4. Discussion
Present study showed that the activity level of tibialis anterior muscle may not be affected by genu varum abnormality. Samaei et al. reported that people with genu varum have weaker dynamic and static stability in medial-lateral direction, but their dynamic and static stability is not different from the same in people with normal knee in anterior-posterior and overall status [8]. Nyland et al. also reported that people with genu varum use different dynamic postural control strategies during single-leg stand [7]. According to these studies, genu varum abnormality disturbs stability. Previous studies investigated the effect of genu varum abnormality on postural control. These studies on stability in people with genu varum are conducted mostly with tests which were taken either in standing position [7] or tests which were not mostly functional [8]. In the current study, jump-landing test was used, which is a common practice in most sports and a completely functional activity.
Stability is influenced by different factors. One of which is weak neural-muscular control [9, 29]. Therefore, one of the reasons other than biomechanical and anatomical position, which could justify weak stability in the group with genu varum is less muscular activity; however, the role of certain muscle groups in equilibrium is not well defined. However, little attention has been paid to the role of the calf muscles in dynamic stability. Our main finding was that there were no significant differences between the genu varum and normal groups regarding the electromyographic activity of tibialis anterior muscle before and after landing.
For several reasons, we investigated the muscular activity before and after landing. Pre-landing muscular activity was a measure of predictive muscle contraction. While delaying in muscle response to stimulating stretch was related to the response time needed to react appropriately for the knee abduction; predictive muscular activity was an important variable to be considered. Post-landing muscular activity is how muscles respond to applied forces and torques in response to the ground
Present study showed that the activity level of tibialis anterior muscle may not be affected by genu varum abnormality. Samaei et al. reported that people with genu varum have weaker dynamic and static stability in medial-lateral direction, but their dynamic and static stability is not different from the same in people with normal knee in anterior-posterior and overall status [8]. Nyland et al. also reported that people with genu varum use different dynamic postural control strategies during single-leg stand [7]. According to these studies, genu varum abnormality disturbs stability. Previous studies investigated the effect of genu varum abnormality on postural control. These studies on stability in people with genu varum are conducted mostly with tests which were taken either in standing position [7] or tests which were not mostly functional [8]. In the current study, jump-landing test was used, which is a common practice in most sports and a completely functional activity.
Stability is influenced by different factors. One of which is weak neural-muscular control [9, 29]. Therefore, one of the reasons other than biomechanical and anatomical position, which could justify weak stability in the group with genu varum is less muscular activity; however, the role of certain muscle groups in equilibrium is not well defined. However, little attention has been paid to the role of the calf muscles in dynamic stability. Our main finding was that there were no significant differences between the genu varum and normal groups regarding the electromyographic activity of tibialis anterior muscle before and after landing.
For several reasons, we investigated the muscular activity before and after landing. Pre-landing muscular activity was a measure of predictive muscle contraction. While delaying in muscle response to stimulating stretch was related to the response time needed to react appropriately for the knee abduction; predictive muscular activity was an important variable to be considered. Post-landing muscular activity is how muscles respond to applied forces and torques in response to the ground
reaction force [18]. Post-landing muscular activity may be responsible for differences between the 2 groups in terms of balance (if there is a difference). Landing was selected because this task shows the body activity in sports. Limbs supporting activities is important because the injuries also occur in these areas.
Winter et al. explained the application of the hip and ankle strategies during standing on both feet in connection with the movement of the center of pressure in both medial-lateral and anterior-posterior motion plates [30]. They stated that dorsiflexors or plantar flexors have an important role in reducing anterior-posterior movements. However, maintaining the sagittal plane balance in standing on both feet was mostly related to the movements of the ankle joint. According to them, abductors and adductors of the hip seem to control the internal and external sway of the pressure center and have a greater role in controlling the postural movements of the frontal plate.
Research studies indicate that certain strategies are used for continuous postural control under different circumstances. For example, ankle muscles (i.e. plantar flexors or dorsiflexors) have an important role in single leg and both leg standing, especially on the sagittal plane. However, the more difficult the task, the role of the proximal muscles of the hip increases [31]. Hip muscles mainly provide frontal plane postural control [32]. People use three different movement strategies to maintain balance.
The most common and effective strategy is ankle strategy which is used when postural sway is little. However, when the center of pressure is near sway range, hip strategy is used to prevent excessive ankle movements which includes quick and large movements in the hip. The ankle strategy may be used during tests near the stability range, because this strategy enables people to move and control their center of pressure on the flat and movable surface with minimal joint movement without changing the supporting surface [15]. The used task might justify the study results. The jump-landing task was used in the current study, which was a challenging dynamic task, which involved large muscular movements. Therefore, it seems that during the jump-landing task, which is a dynamic action, the hip strategy is used more than ankle strategy. For this reason, people probably used calf muscles less which leads to non-significant differences between the groups.
Overall, these findings suggest that other muscles or muscle groups are probably responsible for weaker balance observed in people with genu varum. Probably, the hip abducting muscles have a greater role in maintaining balance control during dynamic movements. The middle gluteal muscle is the main hip abductor and necessary for hip stability. Malfunction of this muscle was accompanied by the lower limb dynamic dysfunction in single-leg standing [22].
From a biomechanical point of view, the middle gluteal muscle torque arm is longer than those of the other muscles of the lower limb (i.e. inverters and evertor muscles) which control the movement of the frontal plate. Moreover, hip abductors are more effective in responding to medial-lateral disorders, in changing the position of the body gravity center [30, 33]. In fact, it is assumed that these muscles play a more important role in maintaining balance than the calf muscles. Further studies are required to examine the effect of lower limb muscles on balance.
Ethical Considerations
Compliance with ethical guidelines
All ethical principles were considered in this article. The participants were informed about the purpose of the research and its implementation stages; They were also assured about the confidentiality of their information; Moreover, They were allowed to leave the study whenever they wish, and if desired, the results of the research would be available to them. Also, After describing test protocol to all subjects before participating in the study, they all signed the informed consent form.
Funding
This study was extracted from an MSc. thesis authored by Faraj Fatahi approved by Faculty of Physical Education, University of Isfahan, Isfahan, Iran.
Conflict of interest
The authors certify that they have no affiliation with or involvement in any organization or entity with any financial interest, or non-financial interest in the subject matter or materials discussed in this manuscript.
Acknowledgments
The authors would like to thank the officials of the Faculty of Physical Education at the University of Isfahan for their valuable cooperation and all students participated in this study.
References
Winter et al. explained the application of the hip and ankle strategies during standing on both feet in connection with the movement of the center of pressure in both medial-lateral and anterior-posterior motion plates [30]. They stated that dorsiflexors or plantar flexors have an important role in reducing anterior-posterior movements. However, maintaining the sagittal plane balance in standing on both feet was mostly related to the movements of the ankle joint. According to them, abductors and adductors of the hip seem to control the internal and external sway of the pressure center and have a greater role in controlling the postural movements of the frontal plate.
Research studies indicate that certain strategies are used for continuous postural control under different circumstances. For example, ankle muscles (i.e. plantar flexors or dorsiflexors) have an important role in single leg and both leg standing, especially on the sagittal plane. However, the more difficult the task, the role of the proximal muscles of the hip increases [31]. Hip muscles mainly provide frontal plane postural control [32]. People use three different movement strategies to maintain balance.
The most common and effective strategy is ankle strategy which is used when postural sway is little. However, when the center of pressure is near sway range, hip strategy is used to prevent excessive ankle movements which includes quick and large movements in the hip. The ankle strategy may be used during tests near the stability range, because this strategy enables people to move and control their center of pressure on the flat and movable surface with minimal joint movement without changing the supporting surface [15]. The used task might justify the study results. The jump-landing task was used in the current study, which was a challenging dynamic task, which involved large muscular movements. Therefore, it seems that during the jump-landing task, which is a dynamic action, the hip strategy is used more than ankle strategy. For this reason, people probably used calf muscles less which leads to non-significant differences between the groups.
Overall, these findings suggest that other muscles or muscle groups are probably responsible for weaker balance observed in people with genu varum. Probably, the hip abducting muscles have a greater role in maintaining balance control during dynamic movements. The middle gluteal muscle is the main hip abductor and necessary for hip stability. Malfunction of this muscle was accompanied by the lower limb dynamic dysfunction in single-leg standing [22].
From a biomechanical point of view, the middle gluteal muscle torque arm is longer than those of the other muscles of the lower limb (i.e. inverters and evertor muscles) which control the movement of the frontal plate. Moreover, hip abductors are more effective in responding to medial-lateral disorders, in changing the position of the body gravity center [30, 33]. In fact, it is assumed that these muscles play a more important role in maintaining balance than the calf muscles. Further studies are required to examine the effect of lower limb muscles on balance.
Ethical Considerations
Compliance with ethical guidelines
All ethical principles were considered in this article. The participants were informed about the purpose of the research and its implementation stages; They were also assured about the confidentiality of their information; Moreover, They were allowed to leave the study whenever they wish, and if desired, the results of the research would be available to them. Also, After describing test protocol to all subjects before participating in the study, they all signed the informed consent form.
Funding
This study was extracted from an MSc. thesis authored by Faraj Fatahi approved by Faculty of Physical Education, University of Isfahan, Isfahan, Iran.
Conflict of interest
The authors certify that they have no affiliation with or involvement in any organization or entity with any financial interest, or non-financial interest in the subject matter or materials discussed in this manuscript.
Acknowledgments
The authors would like to thank the officials of the Faculty of Physical Education at the University of Isfahan for their valuable cooperation and all students participated in this study.
References
- Horak FB. Clinical measurement of postural control in adults. Physical Therapy. 1987; 67(12):1881-5. [DOI:10.1093/ptj/67.12.1881] [PMID]
- Van Gheluwe B, Kirby KA, Hagman F. Effects of simulated genu valgum and genu varum on ground reaction forces and subtalar joint function during gait. Journal of the American Podiatric Medical Association. 2005; 95(6):531-41. [DOI:10.7547/0950531] [PMID]
- Cote KP, Brunet ME, II BMG, Shultz SJ. Effects of pronated and supinated foot postures on static and dynamic postural stability. Journal of Athletic Training. 2005; 40(1):41-6. [PMID] [PMCID]
- Johnson F, Leitl S, Waugh W. The distribution of load across the knee. The Bone & Joint Journal. 1980; 62(3):346-9. [DOI:10.1302/0301-620X.62B3.7410467] [PMID]
- Witvrouw E, Danneels L, Thijs Y, Cambier D, Bellemans J. Does soccer participation lead to genu varum? Knee Surgery, Sports Traumatology, Arthroscopy. 2009; 17(4):422-7. [DOI:10.1007/s00167-008-0710-z] [PMID]
- Subotnick SI, Newell SG. Podiatric sports medicine. Texas: Futura Publishing Company; 1975.
- Nyland J, Smith S, Beickman K, Armsey T, Caborn DNM. Frontal plane knee angle affects dynamic postural control strategy during unilateral stance. Medicine & Science in Sports & Exercise. 2002; 34(7):1150-7. [DOI:10.1097/00005768-200207000-00016] [PMID]
- Samaei A, Bakhtiary A, Elham F, Rezasoltani A. Effects of genu varum deformity on postural stability. International Journal of Sports Medicine. 2012; 33(6):469-73. [DOI:10.1055/s-0031-1301331] [PMID]
- Prentice WE. Rehabilitation techniques for sports medicine and athletic training with laboratory manual and esims password card. New York: McGraw-Hill; 2004.
- Horlings CG, van Engelen BG, Allum JH, Bloem BR. A weak balance: The contribution of muscle weakness to postural instability and falls. Nature Clinical Practice Neurology. 2008; 4(9):504-15. [DOI:10.1038/ncpneuro0886] [PMID]
- Moxley Scarborough D, Krebs DE, Harris BA. Quadriceps muscle strength and dynamic stability in elderly persons. Gait & Posture. 1999; 10(1):10-20. [DOI:10.1016/S0966-6362(99)00018-1]
- Ikezoe T, Asakawa Y, Tsutou A. The relationship between quadriceps strength and balance to fall of elderly admitted to a nursing home. Journal of Physical Therapy Science. 2003; 15(2):75-9. [DOI:10.1589/jpts.15.75]
- McKinley P, Pedotti A. Motor strategies in landing from a jump: The role of skill in task execution. Experimental Brain Research. 1992; 90(2):427-40. [DOI:10.1007/BF00227257] [PMID]
- Aniss A, Gandevia S, Burke D. Reflex responses in active muscles elicited by stimulation of low-threshold afferents from the human foot. Journal of Neurophysiology. 1992; 67(5):1375-84. [DOI:10.1152/jn.1992.67.5.1375] [PMID]
- Huber FE, Wells CL. Therapeutic exercise: Treatment planning for progression. Amsterdam: Elsevier; 2006.
- Nashner L. Sensory, neuromuscular, and biomechanical contributions to human balance. In: duncun PW, editor. Balance: Proceeding of APTA Forum. Virginia: American Physical Therapy Association; 1990.
- Gribble PA, Mitterholzer J, Myers AN. Normalizing considerations for time to stabilization assessment. Journal of Science and Medicine in Sport. 2012; 15(2):159-63. [DOI:10.1016/j.jsams.2011.07.012] [PMID]
- Carcia CR, Martin RL. The influence of gender on gluteus medius activity during a drop jump. Physical Therapy in Sport. 2007; 8(4):169-76. [DOI:10.1016/j.ptsp.2007.06.002]
- Boyd RN, Graham HK. Objective measurement of clinical findings in the use of botulinum toxin type A for the management of children with cerebral palsy. European Journal of Neurology. 1999; 6(S4):s23-s35. [DOI:10.1111/j.1468-1331.1999.tb00031.x]
- Ross SE, Guskiewicz K. Time to stabilization: A method for analyzing dynamic postural stability. International Journal of Athletic Therapy and Training. 2003; 8(3):37-39. [DOI:10.1123/att.8.3.37]
- Ross SE, Guskiewicz KM, Yu B. Single-leg jump-landing stabilization times in subjects with functionally unstable ankles. Journal of Athletic Training. 2005; 40(4):298-304. [PMID] [PMCID]
- Russell KA, Palmieri RM, Zinder SM, Ingersoll CD. Sex differences in valgus knee angle during a single-leg drop jump. Journal of Athletic Training. 2006; 41(2):166-71. [PMID] [PMCID]
- Hart JM, Garrison JC, Kerrigan DC, Palmieri-Smith R, Ingersoll CD. Gender differences in gluteus medius muscle activity exist in soccer players performing a forward jump. Research in Sports Medicine. 2007; 15(2):147-55. [DOI:10.1080/15438620701405289] [PMID]
- Ross SE, Guskiewicz KM, Gross MT, Yu B. Assessment tools for identifying functional limitations associated with functional ankle instability. Journal of Athletic Training. 2008; 43(1):44-50. [DOI:10.4085/1062-6050-43.1.44] [PMID] [PMCID]
- Perron M, Hébert LJ, McFadyen BJ, Belzile S, Regnieàre M. The ability of the Biodex Stability System to distinguish level of function in subjects with a second-degree ankle sprain. Clinical Rehabilitation. 2007; 21(1):73-81. [DOI:10.1177/0269215506071288] [PMID]
- Russell KA, Palmieri RM, Zinder SM, Ingersoll CD. Sex differences in valgus knee angle during a single-leg drop jump. Journal of Athletic Training. 2006; 41(2):166-71. [PMID] [PMCID]
- Carcia CR, Martin RL. The influence of gender on gluteus medius activity during a drop jump. Physical Therapy in Sport. 2007; 8(4):169-76. [DOI:10.1016/j.ptsp.2007.06.002]
- Hart JM, Garrison JC, Kerrigan DC, Palmieri-Smith R, Ingersoll CD. Gender differences in gluteus medius muscle activity exist in soccer players performing a forward jump. Research in Sports Medicine. 2007; 15(2):147-55. [DOI:10.1080/15438620701405289] [PMID]
- Orr R. Contribution of muscle weakness to postural instability in the elderly. A systematic review. European Journal of Physical and Rehabilitation Medicine. 2010; 46(2):183-220. [PMID]
- Winter DA, Prince F, Frank J, Powell C, Zabjek KF. Unified theory regarding A/P and M/L balance in quiet stance. Journal of Neurophysiology. 1996; 75(6):2334-43. [DOI:10.1152/jn.1996.75.6.2334] [PMID]
- Riemann BL, Myers JB, Lephart SM. Comparison of the ankle, knee, hip, and trunk corrective action shown during single-leg stance on firm, foam, and multiaxial surfaces. Archives of Physical Medicine and Rehabilitation. 2003; 84(1):90-5. [DOI:10.1053/apmr.2003.50004] [PMID]
- Deniskina N, Levik Y. Relative contribution of ankle and hip muscles in regulation of the human orthograde posture in a frontal plane. Neuroscience Letters. 2001; 310(2):165-8. [DOI:10.1016/S0304-3940(01)02131-0]
- Hoy MG, Zajac FE, Gordon ME. A musculoskeletal model of the human lower extremity: The effect of muscle, tendon, and moment arm on the moment-angle relationship of musculotendon actuators at the hip, knee, and ankle. Journal of Biomechanics. 1990; 23(2):157-69. [DOI:10.1016/0021-9290(90)90349-8]
Type of Study: Research |
Subject:
Sport injury and corrective exercises
Received: 2017/06/22 | Accepted: 2017/11/15 | Published: 2018/01/1
Received: 2017/06/22 | Accepted: 2017/11/15 | Published: 2018/01/1
References
1. Horak FB. Clinical measurement of postural control in adults. Physical Therapy. 1987; 67(12):1881-5. [DOI:10.1093/ptj/67.12.1881] [PMID] [DOI:10.1093/ptj/67.12.1881]
2. Van Gheluwe B, Kirby KA, Hagman F. Effects of simulated genu valgum and genu varum on ground reaction forces and subtalar joint function during gait. Journal of the American Podiatric Medical Association. 2005; 95(6):531-41. [DOI:10.7547/0950531] [PMID] [DOI:10.7547/0950531]
3. Cote KP, Brunet ME, II BMG, Shultz SJ. Effects of pronated and supinated foot postures on static and dynamic postural stability. Journal of Athletic Training. 2005; 40(1):41-6. [PMID] [PMCID] [PMID] [PMCID]
4. Johnson F, Leitl S, Waugh W. The distribution of load across the knee. The Bone & Joint Journal. 1980; 62(3):346-9. [DOI:10.1302/0301-620X.62B3.7410467] [PMID] [DOI:10.1302/0301-620X.62B3.7410467]
5. Witvrouw E, Danneels L, Thijs Y, Cambier D, Bellemans J. Does soccer participation lead to genu varum? Knee Surgery, Sports Traumatology, Arthroscopy. 2009; 17(4):422-7. [DOI:10.1007/s00167-008-0710-z] [PMID] [DOI:10.1007/s00167-008-0710-z]
6. Subotnick SI, Newell SG. Podiatric sports medicine. Texas: Futura Publishing Company; 1975.
7. Nyland J, Smith S, Beickman K, Armsey T, Caborn DNM. Frontal plane knee angle affects dynamic postural control strategy during unilateral stance. Medicine & Science in Sports & Exercise. 2002; 34(7):1150-7. [DOI:10.1097/00005768-200207000-00016] [PMID] [DOI:10.1097/00005768-200207000-00016]
8. Samaei A, Bakhtiary A, Elham F, Rezasoltani A. Effects of genu varum deformity on postural stability. International Journal of Sports Medicine. 2012; 33(6):469-73. [DOI:10.1055/s-0031-1301331] [PMID] [DOI:10.1055/s-0031-1301331]
9. Prentice WE. Rehabilitation techniques for sports medicine and athletic training with laboratory manual and esims password card. New York: McGraw-Hill; 2004.
10. Horlings CG, van Engelen BG, Allum JH, Bloem BR. A weak balance: The contribution of muscle weakness to postural instability and falls. Nature Clinical Practice Neurology. 2008; 4(9):504-15. [DOI:10.1038/ncpneuro0886] [PMID] [DOI:10.1038/ncpneuro0886]
11. Moxley Scarborough D, Krebs DE, Harris BA. Quadriceps muscle strength and dynamic stability in elderly persons. Gait & Posture. 1999; 10(1):10-20. [DOI:10.1016/S0966-6362(99)00018-1] [DOI:10.1016/S0966-6362(99)00018-1]
12. Ikezoe T, Asakawa Y, Tsutou A. The relationship between quadriceps strength and balance to fall of elderly admitted to a nursing home. Journal of Physical Therapy Science. 2003; 15(2):75-9. [DOI:10.1589/jpts.15.75] [DOI:10.1589/jpts.15.75]
13. McKinley P, Pedotti A. Motor strategies in landing from a jump: The role of skill in task execution. Experimental Brain Research. 1992; 90(2):427-40. [DOI:10.1007/BF00227257] [PMID] [DOI:10.1007/BF00227257]
14. Aniss A, Gandevia S, Burke D. Reflex responses in active muscles elicited by stimulation of low-threshold afferents from the human foot. Journal of Neurophysiology. 1992; 67(5):1375-84. [DOI:10.1152/jn.1992.67.5.1375] [PMID] [DOI:10.1152/jn.1992.67.5.1375]
15. Huber FE, Wells CL. Therapeutic exercise: Treatment planning for progression. Amsterdam: Elsevier; 2006.
16. Nashner L. Sensory, neuromuscular, and biomechanical contributions to human balance. In: duncun PW, editor. Balance: Proceeding of APTA Forum. Virginia: American Physical Therapy Association; 1990.
17. Gribble PA, Mitterholzer J, Myers AN. Normalizing considerations for time to stabilization assessment. Journal of Science and Medicine in Sport. 2012; 15(2):159-63. [DOI:10.1016/j.jsams.2011.07.012] [PMID] [DOI:10.1016/j.jsams.2011.07.012]
18. Carcia CR, Martin RL. The influence of gender on gluteus medius activity during a drop jump. Physical Therapy in Sport. 2007; 8(4):169-76. [DOI:10.1016/j.ptsp.2007.06.002] [DOI:10.1016/j.ptsp.2007.06.002]
19. Boyd RN, Graham HK. Objective measurement of clinical findings in the use of botulinum toxin type A for the management of children with cerebral palsy. European Journal of Neurology. 1999; 6(S4):s23-s35. [DOI:10.1111/j.1468-1331.1999.tb00031.x] [DOI:10.1111/j.1468-1331.1999.tb00031.x]
20. Ross SE, Guskiewicz K. Time to stabilization: A method for analyzing dynamic postural stability. International Journal of Athletic Therapy and Training. 2003; 8(3):37-39. [DOI:10.1123/att.8.3.37] [DOI:10.1123/att.8.3.37]
21. Ross SE, Guskiewicz KM, Yu B. Single-leg jump-landing stabilization times in subjects with functionally unstable ankles. Journal of Athletic Training. 2005; 40(4):298-304. [PMID] [PMCID] [PMID] [PMCID]
22. Russell KA, Palmieri RM, Zinder SM, Ingersoll CD. Sex differences in valgus knee angle during a single-leg drop jump. Journal of Athletic Training. 2006; 41(2):166-71. [PMID] [PMCID] [PMID] [PMCID]
23. Hart JM, Garrison JC, Kerrigan DC, Palmieri-Smith R, Ingersoll CD. Gender differences in gluteus medius muscle activity exist in soccer players performing a forward jump. Research in Sports Medicine. 2007; 15(2):147-55. [DOI:10.1080/15438620701405289] [PMID] [DOI:10.1080/15438620701405289]
24. Ross SE, Guskiewicz KM, Gross MT, Yu B. Assessment tools for identifying functional limitations associated with functional ankle instability. Journal of Athletic Training. 2008; 43(1):44-50. [DOI:10.4085/1062-6050-43.1.44] [PMID] [PMCID] [DOI:10.4085/1062-6050-43.1.44]
25. Perron M, Hébert LJ, McFadyen BJ, Belzile S, Regnieàre M. The ability of the Biodex Stability System to distinguish level of function in subjects with a second-degree ankle sprain. Clinical Rehabilitation. 2007; 21(1):73-81. [DOI:10.1177/0269215506071288] [PMID] [DOI:10.1177/0269215506071288]
26. Russell KA, Palmieri RM, Zinder SM, Ingersoll CD. Sex differences in valgus knee angle during a single-leg drop jump. Journal of Athletic Training. 2006; 41(2):166-71. [PMID] [PMCID] [PMID] [PMCID]
27. Carcia CR, Martin RL. The influence of gender on gluteus medius activity during a drop jump. Physical Therapy in Sport. 2007; 8(4):169-76. [DOI:10.1016/j.ptsp.2007.06.002] [DOI:10.1016/j.ptsp.2007.06.002]
28. Hart JM, Garrison JC, Kerrigan DC, Palmieri-Smith R, Ingersoll CD. Gender differences in gluteus medius muscle activity exist in soccer players performing a forward jump. Research in Sports Medicine. 2007; 15(2):147-55. [DOI:10.1080/15438620701405289] [PMID] [DOI:10.1080/15438620701405289]
29. Orr R. Contribution of muscle weakness to postural instability in the elderly. A systematic review. European Journal of Physical and Rehabilitation Medicine. 2010; 46(2):183-220. [PMID] [PMID]
30. Winter DA, Prince F, Frank J, Powell C, Zabjek KF. Unified theory regarding A/P and M/L balance in quiet stance. Journal of Neurophysiology. 1996; 75(6):2334-43. [DOI:10.1152/jn.1996.75.6.2334] [PMID] [DOI:10.1152/jn.1996.75.6.2334]
31. Riemann BL, Myers JB, Lephart SM. Comparison of the ankle, knee, hip, and trunk corrective action shown during single-leg stance on firm, foam, and multiaxial surfaces. Archives of Physical Medicine and Rehabilitation. 2003; 84(1):90-5. [DOI:10.1053/apmr.2003.50004] [PMID] [DOI:10.1053/apmr.2003.50004]
32. Deniskina N, Levik Y. Relative contribution of ankle and hip muscles in regulation of the human orthograde posture in a frontal plane. Neuroscience Letters. 2001; 310(2):165-8. [DOI:10.1016/S0304-3940(01)02131-0] [DOI:10.1016/S0304-3940(01)02131-0]
33. Hoy MG, Zajac FE, Gordon ME. A musculoskeletal model of the human lower extremity: The effect of muscle, tendon, and moment arm on the moment-angle relationship of musculotendon actuators at the hip, knee, and ankle. Journal of Biomechanics. 1990; 23(2):157-69. [DOI:10.1016/0021-9290(90)90349-8] [DOI:10.1016/0021-9290(90)90349-8]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
