

BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
URL: http://ptj.uswr.ac.ir/article-1-246-en.html


1. Introduction
Increasing frequency and depth of breathing are some physiological changes which happen at the beginning of any sport activity to supply the body’s demand of oxygen needed by active muscles and minimize its shortage. Ventilation rate should increase parallel to the cardiac output and the volume of air in the lungs should reach to the extent that oxygen be delivered to the blood and carbon dioxide excreted from it [1]. During physical activities and sport, oxygen consumption in different body organs increases, so as the volume and velocity of blood flow to deliver nutrients and oxygen to various organs and tissues [2]. Therefore, aerobic activities increase the number of breaths and heart beats and put a considerable strain on the cardio-respiratory system. Measurement of respiratory indices provides useful information about the effect of aerobic exercise on the strength of respiratory muscles, airway resistance, and lung function. Dynamic respiratory indices such as Forced Vital Capacity (FVC) and forced expiratory volume in the first second (FEV1) depend on the factors such as age, level of physical activity, body composition, and health condition of people [3].
In this regard, some studies by comparing the lung volume and capacity of the athletes and non-athletes have examined the effects of exercise on these volumes and capacities [4, 5]. According to these studies, FVC values increase by exercise and sport [6]. Similarly, George et al. (2014) examined and compared pulmonary function in 60 athletes and non-athletes and concluded that implementation of physical exercise leads to insignificant difference between the variables of body weight, body surface area, and FVC at the end of the period. However, significant changes and rise in FEV1, the FEV1/FVC ratio, and MVV were observed in athletes compared with non-athletes [7]. There are different methods to estimate the lung volume and capacity, one of which is spirometry. Generally, it is tried to standardize the methods of performing and interpreting spirometry tests [4, 8, 9]. It is so important that the American Thoracic Society (ATS) has initiated many studies to solve this problem [10, 11].
Most formulas derived from studies are based on linear regression and use age and height as independent variables; however, non-linear equations have also been used in some studies [12]. The problem with interpretation of spirometry results is their different results in various studies which sometimes differ up to 20% [13]. For example, the individual spirometry values compared with the values obtained from one study might be lower than normal yet higher than normal compared with the values obtained from another study. Therefore, it is necessary to investigate and determine the normal values for each society. In this case, however, the most common method to determine the vital capacity is using the spirometry device, but its application requires expertise and is very time-consuming. In addition, other devices to evaluate pulmonary functions use direct and indirect methods. Because of the high price of the medical devices, their heaviness (makes their movements difficult), and unfamiliarity of some operators with the devices, using special devices to measure maximum oxygen consumptions is not possible everywhere and for everyone.
Therefore, to rapidly assess the performance of different systems of the human body, the researchers decided to evaluate the athletes’ performance not in the physical education laboratory but in sport fields. In doing so, one way is to use mathematical equations to evaluate functions of various organs of the human body. Accordingly, researchers evaluated physiological indices based on allometric equations [14, 15]. Allometry is a method to express the relationship between physiological and anatomical variables with a unit of body size (usually weight) while increasing the size through mathematical equations [15].
In this regard, Dismoth achieved a formula based on allometric equations and used height index to measure vital capacity of girls and boys. However, due to the differences in race, climate, and characteristics of people in different societies, every country should evaluate Dismoth equation based on the specific characteristics of its society because all the aforementioned factors can influence the value of vital capacity. Overall, in order to estimate the exact maximal aerobic power in activities, we require a valid device with high precision so as to calculate the increase of function and coordination of cardiopulmonary systems. Given that the respiratory gas analysis device could precisely determine the lung volume and capacity, the researchers decided to suggest a model based on the evaluation of lung volume and capacity to estimate the maximum aerobic power by respiratory gas devices as well as mathematical equations. They studied their application in lung function of students as whether it is possible to estimate individual maximal aerobic power through respiratory gas analysis test, and also use Bonin formula to estimate the maximal aerobic power through allometric equation.
2. Materials and Methods
Subjects
This study was a descriptive and correlational research. After obtaining the ethics code of Ferdowsi University of Mashhad (37239.2), the study was conducted according to the Helsinki protocol. After selecting the subjects, their anthropometric measures and cardiorespiratory fitness indexes were collected. The study population included the male students (20 to 25 years old), which were selected by convenience sampling method. In this study, 80 individuals were selected among the available subjects. The subjects’ health status was controlled by self-reported health status questionnaire and medical history. After taking the participants’ consent and in the first stage, some information about the research procedure and objectives along with essential tips on how to hold the Bruce test were given to the subjects.
Anthropometric measurements
During the second stage, the subjects’ heights were measured using an electronic balance with stadiometer (SECA-Germany) to the nearest 0.1 cm and their weight was recorded using a digital scale (Beurer German company, PS07-PS06). Then, the waist-hip ratio was calculated. In-Body-720 (Biospace, Dogok-dong, South Korea) was used to calculate body fat percentage to study fat mass (FM), muscle mass (MM), and total body water (TBW). All these measurements were carried out by refraining volunteers from eating or drinking 4 hours before their tests to have empty bladder, stomach, and bowels.
Diameter of the chest
The chest diameter was measured, after the exhale, by placing the two ends of sliding caliper on the second or third ribs (2.5 cm above the bust line) in the underarm area of the subjects. However, the depth of the chest, after the exhale, was measured by putting one end of the sliding caliper on the tip of the dagger appendage of the sternum and the other end on the 12th rib.
Peak oxygen consumption
In addition, to evaluate the maximal aerobic power, Bruce test for respiratory gas analysis on the treadmill h/p/cosmos was used. This 10-step method starts with the speed of 2.74 km/h and the incline of 10% and the speed and the incline increasingly rises and continues until the subject gets exhausted and is not able to perform the tests anymore. Maximal oxygen consumption (ml.kg.min)=14.76–(1.379×T)+(0.451×T2)–(0.012×T3).
Analysis or allometry ranking is described by this equation: Y=aMb, where Y is a variable which is associated with weight, and “a” is the coefficient of proportionality (proportionality constant). The index b is the allometry coefficient and the main element because this element expresses the intensity and direction of the relationship between the variable b and the body weight. If Y increase has a direct relationship with body weight, then b equals 1 (b=1). If b=0, the body mass does not have any effect on Y and is a variable independent of weight. If Y increases with weight gain but to a lesser degree, in a way that the increase of the variable is less than the weight gain, b will be greater than 0 and smaller than 1. If the value of b is higher than 1, it means that the variable increase is more than weight gain. If Y decreases by the weight gain, as a result, b will be negative [15]. After data collection, the subjects’ maximal oxygen consumption was calculated via allometric equation by using weight replacement in Bonin et al. formula [14] (VO2 max=1.94M0.75).
Data analysis
Finally, the data were analyzed by SPSS 16. After ensuring of the normality of the data distribution by performing Shapiro-Wilk test, the analysis of variance was used for checking homogeneity. In order to predict the values of a variable according to two or more other variables, a multivariate regression model (stepwise method) was used, then using Pearson correlation coefficient, the rate of the correlation of the measured values of VO2 max was determined by two methods of Bruce test and allometric equation. The simplest and the most common model, used for multivariate correlation, is multiple linear models. This model is defined by the following linear relationship: Y=a+b1x1+b2x2+b3x3+...., where Y is a dependent variable, representing the scores of the variable which is measured; “xi”s are the independent variables, representing the scores used to estimate Y; “βi”s are the regression coefficients, representing the amount of changes happening in Y and in relationship with every change unit in x, and β0 is a fixed number, which must be obtained by replacing x and Y in the equation. In this equation, vital capacity, age, and the chests of the subjects were entered as independent or predictor variables. Significant P value of the tests was considered less than 0.05.
3. Results
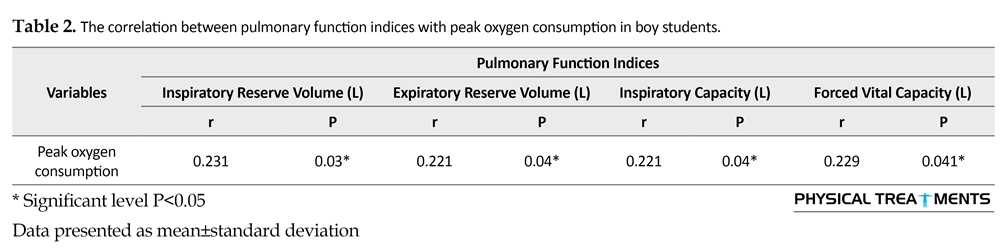
The study subjects’ characteristics are presented in Table 1. According to Table 2, there is a significant positive relationship (P=0.041, r=0.229) between the maximal aerobic power with the values of inspiratory reserve volume (P=0.03, r=0.231), expiratory reserve volume (P=0.042, r=0.228), inspiratory capacity (P=0.048, r=-0.221), and vital capacity with maximal aerobic power in male university students. Furthermore, there is a significant positive relationship (P=0.00, r=1.00) between the device vital capacity and formula vital capacity for male university students. According to the results of Table 3, the following model was developed on the basis of the data obtained from the study: (chest circumference×0.284)+(age×0.319)+(vital capacity×1.761)+inclination=maximal oxygen consumption which for every unit change in the independent variables such as vital capacity, age, and chest circumference, the unit change in the maximal oxygen consumption would be 1.761, 0.319, and 0.284, respectively.

4. Discussion
This study aimed to evaluate pulmonary function for calculating peak oxygen consumption through the respiratory gas analysis and allometric equation in male students. The result of this study shows that between FVC amount and peak oxygen consumption has a positive significant correlation. The findings from the present study are consistent with Fatemi et al. [3], Rabiee et al. [16] and inconsistent with Haji Nia et al. [17] studies. Fatemi et al. [3] reported a significant correlation among the 3 independent variables of FEV1, FVC, FEV1/FVC and projected VO2 max values in 50 healthy males (the mean (SD) age: 22.1(2.47) years). Rabiee et al. [16] investigated the relationship between body composition and maximum oxygen consumption with pulmonary function in 20 subjects. They reported a significant positive correlation between cardiorespiratory fitness and respiratory parameters in light weight group with regard to FEV1 and FVC and heavy weight group with regard to FEV1 and FVC. They also found a significant negative relationship between weight and respiratory parameters in FEV1, FVC of heavy weight group. However, we did not observe any significant relationship between the weight and respiratory parameters of FEV1 in the light weight group.
Haji Nia et al. investigated the relationship between aerobic power to physical activity levels and anthropometric factors among 12-16 years old boys [17]. They concluded that a significant inverse relationship exist between aerobic power and indicators of age, weight, fat percentage, body mass index, WHR, and body surface area. There was no significant correlation between aerobic power and height, but there was significant positive correlation between aerobic power and Physical Activity Levels (PAL). Aerobic power was significantly higher in subjects with high level PAL than subjects with moderate and low PAL. Haines and Wilby examined the relationship between lung function and physical fitness in 605 boys and 566 girls, aged 9-15 years [18]. They reported a significant correlation between aerobic power with FVC and FEV1 values and no relationship between FEV1 to FVC ratio. According to the results, pulmonary function index is directly related to the amount of cardiorespiratory fitness and with the rise in cardiovascular fitness the pulmonary function also increases [19].
The mechanism by which physical activity may affect vital capacity and FEV1 is unclear, but by observing pulmonary function, exercise capacity, and hemodynamic parameters it was found that the amount of vital capacity and FEV1 in pulmonary function at rest situation can

be used as independent variables which are significantly correlated with the amount of peak aerobic power [20].
According to this research, FVC value has a positive significant correlation with height. This finding was supported by Palka et al. [21]. They reported that with increase in age and maturity in boys, especially the vital capacity of the lung volume increases. In this regard, with increasing age and body size, the lung volume also increases, but the airway resistance drops [22]. In other words, with increasing age along with puberty and height increase in boys, the volume and size of organs, especially the heart, lungs, and chest increase. This factor in this age leads to increase in vital and total lung capacity. Therefore, the predicted vital capacity may be related to height. In this context, the height factor can be confirmed as the best predictor of lung function [23, 24]. Generally, it seems that with increasing height, the trunk is equally increases. The consequence of this increase, will be the expansion of the chest size and consequently lung volume that can affect the vital capacity. On the other hand, with increasing age and height, the muscles involved in deep inhaling and exhaling, especially the diaphragm, become more powerful, and for receiving more oxygen, allows vital capacity expansion [25]. In this situation, along with the increase in height, the breathing muscles get stronger and ventilatory responses increase, too [26]. Based on studies, height and body weight equations together, are a better predictor of lung function [27, 28].
The present study results reveal a significant correlation between peak oxygen consumption and chest circumference, and also a positive and significant correlation between FVC of respiratory gas analysis system with FVC of formula. This finding was supported by Shakerin et al. [29] and Beunen et al. [14]. The findings from the present study are inconsistent with those reported in the literature [15]. Shakerin et al. [29] determined the correlation of vital capacity of 11- to 17-year-old female students measured by spirometry and allometry equation on 311 female students with an average (SD) age of 14(3) years. They reported that allometric equation enjoys high validity in determining the vital capacity of 11 to 17 years old female students (r=0.83, α=0.86). Also, there is no difference between mean vital capacity of athlete group and non-athlete one. The result of this research shows that allometric equation can be used for determining the vital capacity of female students when exercise laboratory and spirometer are not available. Analyses of Beunen et al. [14] of intraindividual allometric development of aerobic power in 73 boys followed by annual intervals of 8 to 16 years showed that inter-individual allometry coefficients for body mass exceeded 0.750. Intraindividual coefficients of peak VO2 by body mass varied extensively and ranged from 0.555 to 1.178.
Gaeini et al. determined the reliability of allometric equation in measuring the VO2 max of 12 to 16 years old female students [15]. They reported that allometric equation enjoys high reliability in determining VO2 max, when it was absolute (1/min). However, when VO2 max is relative (ml/kg/min), the reliability between VO2 max by allometric equation and VO2 max by Bruce protocol is r=-0.362 (P=0.01). Therefore, according to the obtained results, allometric equation can be used. In the field, due to an increase in chest size, the pulmonary ventilation increases and these changes can lead to an increase in the better supply of oxygen and suitable release of oxygen to all body parts. Then by implementing appropriate physical activity, the endurance of the respiratory muscles increases which rises chest expansion and lung volume [30, 31].
According to the study results, there is a significant positive correlation between amounts of FVC of respiratory gas analysis system with FVC of formula. According to this result, the following model was developed: VO2 max=inclination+(1.761×FVC)+(0.319×age)+(0.284×chest circumference). Thus, in order to estimate the maximal oxygen uptake of male students, in the absence of other methods, allometric equation can be used in any place. The study limitations included lack of control over the participants’ life style (their amount of sleep, rest, and extra-curricular activities), and the small number of subjects that left the study.
Acknowledgments
This work was supported by a grant from Scientific Research of the Academy of Physical Education under code number 37239.2 at Ferdowsi University of Mashhad, Iran. We would like to offer our appreciation and thanks to all study subjects for their participation.
Conflict of Interest
None of the authors declared a personal or financial conflict of interest.
References
[1]Garrett WE, Kirkendall DT. Exercise and sport science. Philadelphia: Lippincott Williams & Wilkins; 2000.
[2]Batzel JJ, Kappel F, Schneditz D, Tran HT. Cardiovascular and respiratory systems: Modeling, analysis, and control. Philadelphia: Society for Industrial and Applied Mathematics; 2007.
[3]Fatemi R, Ghanbarzadeh M. Relationship between airway resistance indices and maximal oxygen uptake in young adults. Journal of Human Kinetics. 2009; 22(1):29-34. doi: 10.2478/v10078-009-0020-7
[4]Miller MG, Weiler JM, Baker R, Collins J, D'Alonzo G. National athletic trainers' association position statement: Management of asthma in athletes. Journal of Athletic Training. 2005; 40(3):224-45. PMCID: PMC1250269
[5]Kippelen P. Effect of endurance training on lung function: A one year study. British Journal of Sports Medicine. 2005; 39(9):617–21. doi: 10.1136/bjsm.2004.014464
[6]McArdle WD, Katch FI, Katch VL. Exercise physiology: Nutrition, energy, and human performance. Philadelphia: Lippincott Williams & Wilkins; 2010.
[7]George JM, Sen K, Raveendran C. Evaluation of the effect of exercise on pulmonary function in young healthy adults. International Journal of Biomedical and Advance Research. 2014; 5(6):308-12. doi: 10.7439/ijbar.v5i6.711
[8]Morris JF, Koski A, Johnson LC. Spirometric standards for healthy nonsmoking adults 1–3. American Review of Respiratory Disease. 1971; 103(1):57-67. doi: 10.1164/arrd.1971.103.1.57
[9]Intermountain Thoracic Society. Clinical pulmonary function testing: A manual of uniform laboratory procedures for the intermountain area. Salt Lake City: Intermountain Thoracic Society; 1975.
[10]Laszlo G. Standardised lung function testing. Thorax. 1984; 39(12):881-6. PMCID: PMC459947
[11]American Thoracic Society. Standardization of spirometry—1987 Update. American Review of Respiratory Disease. 1987; 136(5):1285–98. doi: 10.1164/ajrccm/136.5.1285
[12]Schoenberg JB, Beck GJ, Bouhuys A. Growth and decay of pulmonary function in healthy blacks and whites. Respiration Physiology. 1978; 33(3):367–93. doi: 10.1016/0034-5687(78)90063-4
[13]Glindmeyer HW. Predictable confusion. Journal of Occupational and Environmental Medicine. 1981; 23(12):845-9.
[14]Beunen G, Baxter-Jones Adg, Mirwald Rl, Thomis M, Lefevre J, Malina Rm, et al. Intraindividual allometric development of aerobic power in 8 to 16 year-old boys. Medicine & Science in Sports & Exercise. 2002; 34(3):503–10. doi: 10.1097/00005768-200203000-00018
[15]Gaeini A, Kashef M, Saberi NZ, Ramezani A. [Determining the validity of allometric equation in estimating maximum oxygen uptake of 12-16 years old non athletes girls students in mashhad (Persian)]. Olympic, 2010. 18(1):107-115.
[16]Francisco CO, Catai AM, Moura-Tonello SCG, Lopes SLB, Benze B, Del Vale AM, et al. Cardiorespiratory fitness, pulmonary function and C-reactive protein levels in nonsmoking individuals with diabetes. Brazilian Journal of Medical and Biological Research. 2014; 47(5):426-31. doi: 10.1590/1414-431X20143370
[17]Hajinia M, Hamedinia MR, Haghighi AH. [The relationship between aerobic power to physical activity levels and anthropometric factors among 12-16 years old boys (Persian)]. Sport Physiology. 2014; 6(23):55-68.
[18]Haines DA, Wilby K. Relationship between lung function and physical fitness in 9 to 15 year old Australian children. Australian Journal of Science and Medicine in Sport. 1993; 25:35-.
[19]Rabiee MA, Ghanbarzadeh M, Habibi A, Marashiyan H. [Relationship between body composition and cardiorespiratory fitness with pulmonary function in light weight and heavy weight (Persian)]. Shomal Journal of Management and Physiology in Sport. 2014; 2(1):13-20.
[20]Bilgin UL, Çetin EB, Pulur AT. Relation between fat distribution and pulmonary function in triathletes. Science, Movement and Health. 2010; 10:429-32.
[21]Palka MJ. [Spirometric predicted values for teenage boys: Relation to body composition and exercise performance (French)]. Bulletin Europeen De Physiopathologie Respiratoire. 1981; 18(1):59-64. PMID: 7053777
[22]Lanteri CJ, Sly PD. Changes in respiratory mechanics with age. Journal of Applied Physiology. 1993; 74(1):369-78. PMID: 8444716
[23]Xuan W, Peat JK, Toelle BG, Marks GB, Berry G, woolcock AJ. Lung function growth and its relation to airway hyperresponsiveness and recent wheeze. American Journal of Respiratory and Critical Care Medicine. 2000; 161(6):1820–4. doi: 10.1164/ajrccm.161.6.9809118
[24]Hagberg JM, Yerg JE, Seals DR. Pulmonary function in young and older athletes and untrained men. Journal of Applied Physiology. 1988; 65(1):101-5. PMID: 3403454
[25]Torres LAGMM, Martinez FE, Manço JC. Correlation between standing height, sitting height, and arm span as an index of pulmonary function in 6-10 year old children. Pediatric Pulmonology. 2003; 36(3):202–8. doi: 10.1002/ppul.10239
[26]Boskabady MH, Tashakory A, Mazloom R, Ghamami G. Prediction equations for pulmonary function values in healthy young Iranians aged 8-18 years. Respirology. 2004; 9(4):535–42. doi: 10.1111/j.1440-1843.2004.00623.x
[27]Golshan M, Nemat Bakhsh M. [Normal prediction equations of spirometric parameters in 799 healthy Iranian children and adolescents. Archives of Iranian Medicine. 2000; 3(3):109-13.
[28]Glew RH. Comparison of pulmonary function between children living in rural and urban areas in northern Nigeria. Journal of Tropical Pediatrics. 2004; 50(4):209–16. doi: 10.1093/tropej/50.4.209
[29]Shakerin A, Ostovan Z. [Determining the correlation of vital capacity of 11 to 17 years old girl students measured by spirometry and Allometry equation in Tehran (Persian)]. Sport Physiology. 2016; 8(29):119-130.
[30]Clarkson HM. Musculoskeletal assessment: Joint range of motion and manual muscle strength. Philadelphia: Lippincott Williams & Wilkins; 2000.
[31]Lee H. Cardiopulmonary physical therapy. Journal of the American Physical Therapy Association. 1996; 76(5):15-25.
Received: 2016/05/4 | Accepted: 2016/08/17 | Published: 2016/10/1
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
