Wed, Jul 22, 2026
Volume 6, Issue 4 (Winter 2017)
PTJ 2017, 6(4): 185-194 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Rezaeian Z, Karimi M T. The Effects of Various Orthotic Treatments on the Standing and Walking Performance of Diabetic Patients. PTJ 2017; 6 (4) :185-194
URL: http://ptj.uswr.ac.ir/article-1-195-en.html
URL: http://ptj.uswr.ac.ir/article-1-195-en.html


1- Department of Orthotics and Prosthetics, School of Rehabilitation Sciences, Isfahan University of Medical Sciences, Isfahan, Iran.
Keywords: Diabetic neuropathy, Orthosis, Plantar pressure, Balance, Energy consumption, Spatial-temporal parameters of gait
Full-Text [PDF 525 kb]
(2728 Downloads)
| Abstract (HTML) (7107 Views)

Full-Text: (2122 Views)
1. Introduction
Diabetes mellitus with its complications like pressure ulcers is an economic, social, and medical problem in most countries and a major cause of non-traumatic amputation in most Western countries [1, 2]. Many damages to diabetic foot are preventable and patient’s awareness is the most important principle in prevention. Numbness, especially the lack of pain sensation is a critical predisposing factor in developing ulcers and ultimately amputation in diabetic foot [3]. In 2005, it was reported that lifelong dangers threaten more than 25% of diabetic patients who have a serious ulcer in foot. Moreover, every 30 seconds a lower limb amputation occurs as a result of diabetes in the world [4]. Neuropathic wound management is done in 3 ways: 1) Removing callus; 2) Eradicating the infection; and 3) Reducing the effect of body weight forces.
There are different strategies to reduce plantar pressure and treat ulcers in diabetic patients with foot numbness, including: casting plaster, corrective orthotic devices like insoles, rocker, and medical shoes [5-7]. Several studies have been conducted to evaluate the effect of orthosis on reducing foot plantar pressure in patients with diabetes. Nick et al. (2006) investigated plantar pressure in toes area of diabetic patients during their daily activities. Plantar pressure was registered while walking on flat surfaces, ramp, stairs as well as rotation while performing these activities. The least pressure was recorded under the fourth and the fifth metatarsal. Pressure during walking compared to other activities was higher on the flat surface. Rotation during these activities compared to other activities creates more pressure to the plantar area. Plantar pressure was higher while walking up the stairs and ramp than while going down. In the thumb area, more pressure was registered while going down the stairs compared to going up [8].
In two studies by Giacomozzi et al. (2008), the effects of vertical forces, shear stresses, and free torques on foot were studied in patients with diabetes and those with peripheral neuropathy during walking. In both studies, soles of the feet were divided into three regions of anterior, middle, and posterior. Findings showed increase in the maximum pressure on the external shear force and under the metatarsals (the middle area of the foot) [9]. In another study in 2010, it was found that diabetic patients are mostly accustomed to the same strategy in walking where gait speed is slower, base of support is wider, and double limb support is longer [10].
Sacco et al. [11] evaluated the plantar pressure in the anterior, middle, and posterior areas. The results showed that diabetic patients have less motion in the ankle joint in the static phase and less ankle flexion in the heel while contacting the ground. The maximum amount of pressure and maximum time for its application in diabetic patients is in the middle part of the foot and separation phase of the heels from the ground, compared to the heel contact with the ground [11]. The results of study by Menez et al. (2004) on the old people with diabetic neuropathy indicate that the gait speed, motion rhythm, and stride length in these people decrease and instances of rhythmic acceleration in the head and pelvis is lower compared to the control group [12].
According to Dingwell et al. [13] study, patients with diabetic neuropathy are more at risk of falling during walking than people with normal sense. Also their walking speed is slower in order to improve stability of motion and to increase motor variability [13]. The amount of energy consumption is different in people and depends on the size and structure of the body. Therefore, people with low metabolic rates are at more risk of weight gain and diabetes. According to Nair study in 1984, base energy consumption was 2042 kcal in diabetic patients in 24 hours, compared to 1774 kcal in normal people in 24 hours (P<0.01). However, insulin therapy decreased energy consumption by 1724 kcal in 24 hours (P<0.01) [14].
To prevent ulcers and its complications in diabetic foot, the pressure must be removed from high pressure areas with the help of foot orthosis, which finally leads to proper plantar pressure distribution and prevention of ulcers. Various devices have been designed to prevent foot ulcers in these patients. However, other aspects of treatment, in particular, the performance of these patients in standing and walking, which are the most important daily activities of individuals, have been neglected in their design and administration. In addition, the difference among available devices and their effects have not been clearly described. Therefore, by reviewing studies in this field, we attempted to interpret and compare appropriate orthosis strategies in the treatment of these patients.
2. Materials and Methods
A thorough search of the scientific literature was carried out in PubMed, Google Scholar, and ISI Web of Knowledge. Different keywords such as “diabetic neuropathy”, “orthosis”, “plantar pressure”, “balance”, “energy consumption”, “spatial-temporal parameters of gait” were used to search for articles. In the next step, the scientific search was done in relation to “the effect of orthotic treatments on each of these factors in patients with diabetes”. Next, all found articles were classified in 6 separate files (including pathology, plantar pressure, standing balance, energy consumption, spatial-temporal parameters of gait, and foot orthotic treatment). Afterwards, the articles were read and their complete summaries were carefully classified and inserted into Microsoft Excel in 6 separate sections.
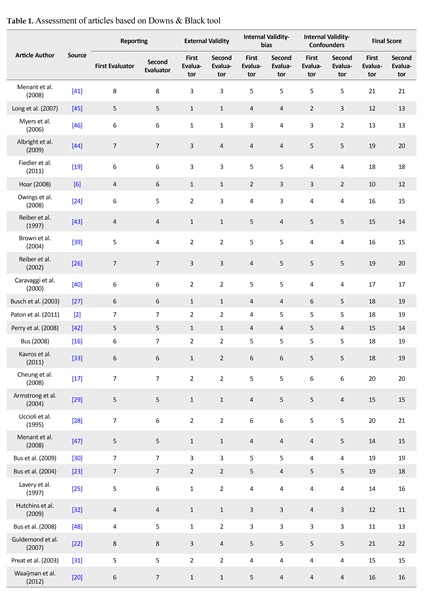
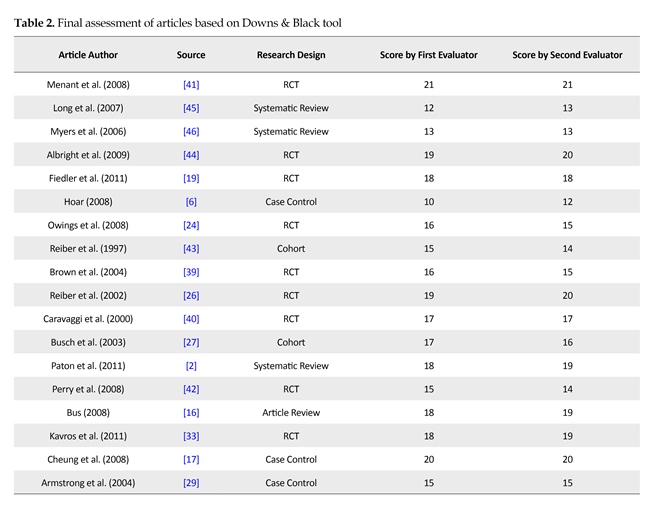
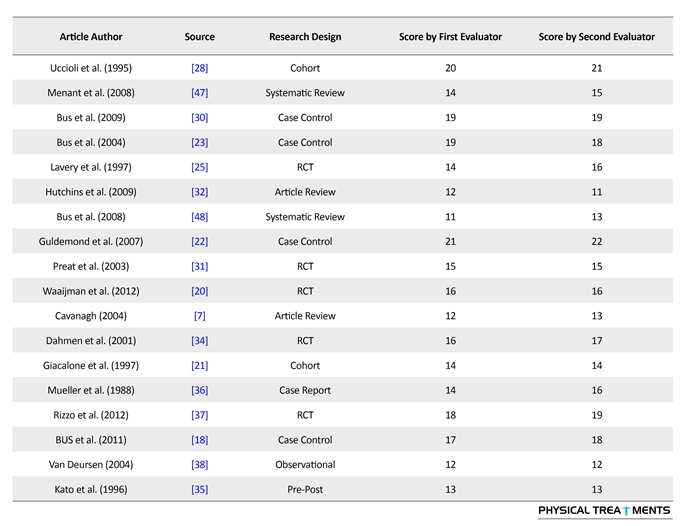
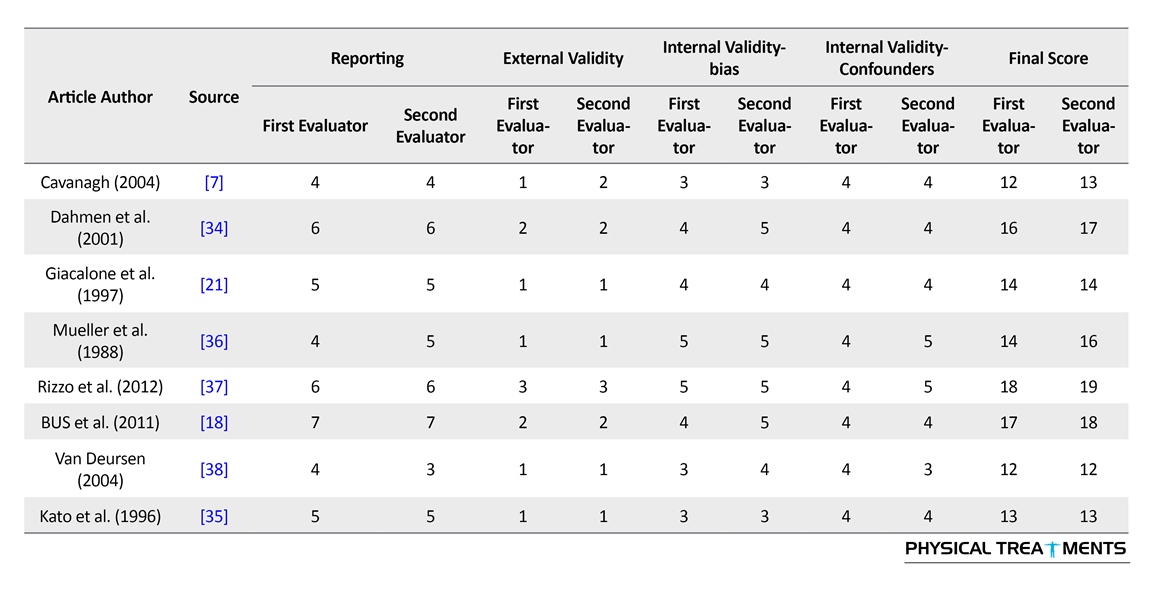
The first step in choosing articles are based on the relevance of article title with criteria and questions of the investigator. The second stage was also based on the following criteria: 1) Article was written in English; 2) Article included information about people with neuropathy diabetes; 3) The study population were more than 20 people; 4) Article design was “pre/post, case series, case report, randomized controlled trial, observational and clinical consensus”; and 5) The main measures included plantar pressure of the feet, standing balance, energy consumption, and spatial-temporal parameters during walking. Then, the assessment of articles was carried out based on the quality of methodology and Downs and Black tool. Saunders et al. compared 18 instruments for assessing the quality of non-randomized trials. After the analysis, they proposed Downs and Black’s as the best instrument, because this instrument has developed methods of testing intelligence and its validity and reliability have been also tested. It includes 27 questions in terms of reporting, external validity, internal validity (bias) and internal validity of confounding factors [15]. Table 1 presents the quality of studies. It seems that quality of studies is weak and their results should be used with caution. Table 2 shows final assessment of articles based on Downs & Black tool in this study.
3. Results
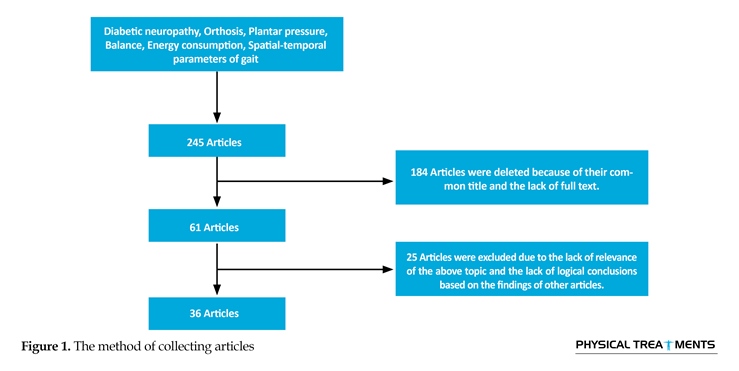
After the scientific search, a total of 245 articles in English were obtained with the keywords of “diabetic neuropathy”, “orthosis”, “plantar pressure”, “balance”, “energy consumption”, “spatial-temporal parameters of gait”. Out of them, 184 articles were removed because of having duplicate title or incomplete text. Twenty-five articles were also excluded from the study, because they were not related to the above subject or had no logical conclusion based on the findings of other articles. Eventually, in the upcoming review article, results of 36 articles were examined and reported (Figure 1). 25 articles were excluded from the study, because they were not related to the study subject or had no logical conclusion based on the findings of other articles.
Of final 36 articles on the effect of foot orthosis on walking and standing of patients with diabetes, 25 articles just noted the effect of orthoses on the plantar pressure in these patients. Of these, 2 were systematic review, 6 case control, 10 RCT, 3 Cohort, 1 pre-post, 1 case report, and 2 article review. Also, 2 articles discussed about some parameters of walking besides foot plantar pressure, one of these articles was case control and the other one was RCT. In an observational article, the effect of foot plantar pressure on standing balance had been studied, too. Of the remaining articles, 5 were related to the balance, where 3 were RCT, 1 systematic review, and 1 cohort. Three articles studied the effect of orthoses on spatial-temporal parameters of gait in which 2 studies were systematic review and 1 article review.
Plantar pressure
Of the studied articles, 7 studies investigated the effect of footwear on plantar pressure in diabetes patients that one article was systematic review [16], 2 case control [17, 18], 2 RCT [19, 20] and 1 article review [7]. In one cohort study [21], the impact of sandals in reducing plantar pressure in most areas of foot was higher in comparison to shoes. The study results indicate that shoes type and its properties is effective in reducing the applied forces exerted on the soles of the feet. Shoes can reduce the maximum pressure and exertion time in all foot areas, especially in the anterior area.
Seven articles were available in relation to the effect of insole alone on the plantar pressure, in which two of them were systematic review [2, 16], 2 case control [22, 23], 2 RCT [24, 25] and 1 article review [16]. Four articles were about use of shoes with insoles and its effect on plantar pressure; that 2 of them were RCT [25, 26], and 2 cohort studies [27, 28]. Four articles examined the effect of rocker in shoes on the plantar pressure in which 2 articles were case control [29, 30], 1 RCT [31], and 1 article review [32]. In this context, there are 4 articles that examined the impact of rocker on shoes with insoles where 2 articles were RCT [33, 34], 1 article case control [6], and 1 systematic review [16]. Reported results of the studies show that using rocker is very effective on healing or preventing the diabetic foot ulcer, especially if the rocker is placed outside the shoes and standard insoles inside it. It is worth noting that type of rocker, its slope and the location of its tip is very effective in reduction or elimination of pressure from wounded areas.
Of the studies reviewed, 4 articles discussed the ankle orthosis on reducing plantar pressure, where a study was pre-post [35], 1 report [36] and 2 RCT [34, 37]. There is little research regarding use of ankle orthosis in reducing the plantar pressure and also available articles were not valid regarding their results. Four articles were found regarding the impact of plaster, where 1 was systematic review [16], 1 observation [38], and 2 RCT [39, 40].
Diabetes mellitus with its complications like pressure ulcers is an economic, social, and medical problem in most countries and a major cause of non-traumatic amputation in most Western countries [1, 2]. Many damages to diabetic foot are preventable and patient’s awareness is the most important principle in prevention. Numbness, especially the lack of pain sensation is a critical predisposing factor in developing ulcers and ultimately amputation in diabetic foot [3]. In 2005, it was reported that lifelong dangers threaten more than 25% of diabetic patients who have a serious ulcer in foot. Moreover, every 30 seconds a lower limb amputation occurs as a result of diabetes in the world [4]. Neuropathic wound management is done in 3 ways: 1) Removing callus; 2) Eradicating the infection; and 3) Reducing the effect of body weight forces.
There are different strategies to reduce plantar pressure and treat ulcers in diabetic patients with foot numbness, including: casting plaster, corrective orthotic devices like insoles, rocker, and medical shoes [5-7]. Several studies have been conducted to evaluate the effect of orthosis on reducing foot plantar pressure in patients with diabetes. Nick et al. (2006) investigated plantar pressure in toes area of diabetic patients during their daily activities. Plantar pressure was registered while walking on flat surfaces, ramp, stairs as well as rotation while performing these activities. The least pressure was recorded under the fourth and the fifth metatarsal. Pressure during walking compared to other activities was higher on the flat surface. Rotation during these activities compared to other activities creates more pressure to the plantar area. Plantar pressure was higher while walking up the stairs and ramp than while going down. In the thumb area, more pressure was registered while going down the stairs compared to going up [8].
In two studies by Giacomozzi et al. (2008), the effects of vertical forces, shear stresses, and free torques on foot were studied in patients with diabetes and those with peripheral neuropathy during walking. In both studies, soles of the feet were divided into three regions of anterior, middle, and posterior. Findings showed increase in the maximum pressure on the external shear force and under the metatarsals (the middle area of the foot) [9]. In another study in 2010, it was found that diabetic patients are mostly accustomed to the same strategy in walking where gait speed is slower, base of support is wider, and double limb support is longer [10].
Sacco et al. [11] evaluated the plantar pressure in the anterior, middle, and posterior areas. The results showed that diabetic patients have less motion in the ankle joint in the static phase and less ankle flexion in the heel while contacting the ground. The maximum amount of pressure and maximum time for its application in diabetic patients is in the middle part of the foot and separation phase of the heels from the ground, compared to the heel contact with the ground [11]. The results of study by Menez et al. (2004) on the old people with diabetic neuropathy indicate that the gait speed, motion rhythm, and stride length in these people decrease and instances of rhythmic acceleration in the head and pelvis is lower compared to the control group [12].
According to Dingwell et al. [13] study, patients with diabetic neuropathy are more at risk of falling during walking than people with normal sense. Also their walking speed is slower in order to improve stability of motion and to increase motor variability [13]. The amount of energy consumption is different in people and depends on the size and structure of the body. Therefore, people with low metabolic rates are at more risk of weight gain and diabetes. According to Nair study in 1984, base energy consumption was 2042 kcal in diabetic patients in 24 hours, compared to 1774 kcal in normal people in 24 hours (P<0.01). However, insulin therapy decreased energy consumption by 1724 kcal in 24 hours (P<0.01) [14].
To prevent ulcers and its complications in diabetic foot, the pressure must be removed from high pressure areas with the help of foot orthosis, which finally leads to proper plantar pressure distribution and prevention of ulcers. Various devices have been designed to prevent foot ulcers in these patients. However, other aspects of treatment, in particular, the performance of these patients in standing and walking, which are the most important daily activities of individuals, have been neglected in their design and administration. In addition, the difference among available devices and their effects have not been clearly described. Therefore, by reviewing studies in this field, we attempted to interpret and compare appropriate orthosis strategies in the treatment of these patients.
2. Materials and Methods
A thorough search of the scientific literature was carried out in PubMed, Google Scholar, and ISI Web of Knowledge. Different keywords such as “diabetic neuropathy”, “orthosis”, “plantar pressure”, “balance”, “energy consumption”, “spatial-temporal parameters of gait” were used to search for articles. In the next step, the scientific search was done in relation to “the effect of orthotic treatments on each of these factors in patients with diabetes”. Next, all found articles were classified in 6 separate files (including pathology, plantar pressure, standing balance, energy consumption, spatial-temporal parameters of gait, and foot orthotic treatment). Afterwards, the articles were read and their complete summaries were carefully classified and inserted into Microsoft Excel in 6 separate sections.
The first step in choosing articles are based on the relevance of article title with criteria and questions of the investigator. The second stage was also based on the following criteria: 1) Article was written in English; 2) Article included information about people with neuropathy diabetes; 3) The study population were more than 20 people; 4) Article design was “pre/post, case series, case report, randomized controlled trial, observational and clinical consensus”; and 5) The main measures included plantar pressure of the feet, standing balance, energy consumption, and spatial-temporal parameters during walking. Then, the assessment of articles was carried out based on the quality of methodology and Downs and Black tool. Saunders et al. compared 18 instruments for assessing the quality of non-randomized trials. After the analysis, they proposed Downs and Black’s as the best instrument, because this instrument has developed methods of testing intelligence and its validity and reliability have been also tested. It includes 27 questions in terms of reporting, external validity, internal validity (bias) and internal validity of confounding factors [15]. Table 1 presents the quality of studies. It seems that quality of studies is weak and their results should be used with caution. Table 2 shows final assessment of articles based on Downs & Black tool in this study.
3. Results
After the scientific search, a total of 245 articles in English were obtained with the keywords of “diabetic neuropathy”, “orthosis”, “plantar pressure”, “balance”, “energy consumption”, “spatial-temporal parameters of gait”. Out of them, 184 articles were removed because of having duplicate title or incomplete text. Twenty-five articles were also excluded from the study, because they were not related to the above subject or had no logical conclusion based on the findings of other articles. Eventually, in the upcoming review article, results of 36 articles were examined and reported (Figure 1). 25 articles were excluded from the study, because they were not related to the study subject or had no logical conclusion based on the findings of other articles.
Of final 36 articles on the effect of foot orthosis on walking and standing of patients with diabetes, 25 articles just noted the effect of orthoses on the plantar pressure in these patients. Of these, 2 were systematic review, 6 case control, 10 RCT, 3 Cohort, 1 pre-post, 1 case report, and 2 article review. Also, 2 articles discussed about some parameters of walking besides foot plantar pressure, one of these articles was case control and the other one was RCT. In an observational article, the effect of foot plantar pressure on standing balance had been studied, too. Of the remaining articles, 5 were related to the balance, where 3 were RCT, 1 systematic review, and 1 cohort. Three articles studied the effect of orthoses on spatial-temporal parameters of gait in which 2 studies were systematic review and 1 article review.
Plantar pressure
Of the studied articles, 7 studies investigated the effect of footwear on plantar pressure in diabetes patients that one article was systematic review [16], 2 case control [17, 18], 2 RCT [19, 20] and 1 article review [7]. In one cohort study [21], the impact of sandals in reducing plantar pressure in most areas of foot was higher in comparison to shoes. The study results indicate that shoes type and its properties is effective in reducing the applied forces exerted on the soles of the feet. Shoes can reduce the maximum pressure and exertion time in all foot areas, especially in the anterior area.
Seven articles were available in relation to the effect of insole alone on the plantar pressure, in which two of them were systematic review [2, 16], 2 case control [22, 23], 2 RCT [24, 25] and 1 article review [16]. Four articles were about use of shoes with insoles and its effect on plantar pressure; that 2 of them were RCT [25, 26], and 2 cohort studies [27, 28]. Four articles examined the effect of rocker in shoes on the plantar pressure in which 2 articles were case control [29, 30], 1 RCT [31], and 1 article review [32]. In this context, there are 4 articles that examined the impact of rocker on shoes with insoles where 2 articles were RCT [33, 34], 1 article case control [6], and 1 systematic review [16]. Reported results of the studies show that using rocker is very effective on healing or preventing the diabetic foot ulcer, especially if the rocker is placed outside the shoes and standard insoles inside it. It is worth noting that type of rocker, its slope and the location of its tip is very effective in reduction or elimination of pressure from wounded areas.
Of the studies reviewed, 4 articles discussed the ankle orthosis on reducing plantar pressure, where a study was pre-post [35], 1 report [36] and 2 RCT [34, 37]. There is little research regarding use of ankle orthosis in reducing the plantar pressure and also available articles were not valid regarding their results. Four articles were found regarding the impact of plaster, where 1 was systematic review [16], 1 observation [38], and 2 RCT [39, 40].

Standing balance
In this study, two articles were obtained regarding the impact of shoes, where one of them was RCT [41] and 1 systematic review [41] and both of them reported the positive effect of the shoes type on improvement of standing balance in people with diabetes. There were two papers regarding the impact of the insole, where one of them was RCT [42] and the other one was cohort [43]. Meanwhile, one RCT study [44] was found regarding the rocker impact
In this study, two articles were obtained regarding the impact of shoes, where one of them was RCT [41] and 1 systematic review [41] and both of them reported the positive effect of the shoes type on improvement of standing balance in people with diabetes. There were two papers regarding the impact of the insole, where one of them was RCT [42] and the other one was cohort [43]. Meanwhile, one RCT study [44] was found regarding the rocker impact


and an observation article [38] was found in relation to the effects of plaster on the improvement of standing balance. Generally, studies are very limited regarding the impact of therapeutic instruments on standing balance, and in most research areas, there is no available study; however, results of current studies show effectiveness of using a standard insole with special shoes on regaining stabilization. Yet, only one paper was found regarding the impact of rocker on the balance of diabetic patients which reminds that using rocker decreases sensation and as a result, increases risk of falling in a persons with diabetes. No valid study was found on using plaster, which on its results can be relied.

Energy consumption
In this regard, there is no article showing that using any orthotic devices in diabetic patients would change energy consumption.
Spatial-temporal parameters of gait
Very few studies are found in the field of spatial-temporal parameters of gait and the effect of orthosis on these people in a way that only two systematic review studies were found on shoes [45, 46]. Only one article was found as case control [22] regarding the effect of the insole in this context. During the researcher’s investigation about rocker, two articles were found, where one of them was article review [32] and the other one was RCT [34]. Only one RCT article was found [34] regarding the ankle orthosis which partially addressed this subject. Eventually, like standing balance, the study results regarding the impact of therapeutic instruments and spatial-temporal parameters on gait are very limited and indicate that these instruments have little effect on gait parameters, especially speed and only partially change range of motion in some joints. Even there are contradictory results regarding the effect of rocker on sagittal plane movements of foot.
4. Discussion
Plantar pressure
Our study results indicate that shoe type and its properties are effective in reducing the applied forces exerted on the plantar area of the feet, and shoes can decrease the maximum pressure and its exertion time on all areas of the foot, especially the anterior area. In addition, it is observed that using insole alone has no significant effect in reducing plantar pressure and yet the best insole is the one that is built customized, based on the individual sizes, and also considering the plantar pressure. Moreover, the greatest effect is noted when the insole is used with an appropriate footwear. Using rocker and its effect is stronger than previous two orthoses. Reported results of the studies show that using rocker is very effective for healing the wound or preventing the ulcer in diabetic foot, especially, if the rocker is placed outside the shoes and standard insoles inside it. It is worth noting that rocker type, slope, and the location of its tip are very effective in reduction or elimination of pressure from wounded areas of the foot. There are few studies about ankle orthosis and reducing the pressure on the plantar area, and available articles are not valid regarding their results. A few studies were found regarding the use of plaster with full contact, but all of them strongly supported the use of plaster. Results show that fiber glass plaster with full contact compare to the other means is more useful in reducing the extent of diabetic ulcers and the recovery rate.
Standing balance
Studies are very limited regarding the impact of therapeutic instruments on standing balance, and in most research areas, there is no study; however, results of available studies show effectiveness of using a standard insole with especial shoe on regaining the lost stabilization. Yet, only one paper was found regarding the impact of rocker on the balance of diabetic patients which reminds that rocker decreases sensation and as a result, increases risk of falling in a person with diabetes. No valid study was found on using plaster, which on its results can be relied.
Energy consumption
There is no article in this regard showing that using any orthotic devices in diabetes patients, changes energy consumption. And given the importance of energy efficiency in patients with diabetes, it is suggested that future studies cover this issue.
Spatial-temporal parameters of gait
Like standing balance, the study results regarding the impact of therapeutic instruments and spatial-temporal parameters on gait are very limited and indicate that these instruments have little effect on gait parameters, especially speed and they only partially change range of motion in some joints. Even there are contradictory results regarding the effect of rocker on sagittal plane movements of the foot.
Our study has some limitations such as lack of access to some sites and articles and unavailability of the full text of some articles. This study has also some suggestions; This research included all sorts of article designs from RCT to case reports. Most studies emphasized treatment of foot plantar ulcers in diabetic patients and the role of orthoses interventions in achieving this goal. Also, most shoes and orthoses aimed at reducing the pressure from the wounded areas and the risk of developing ulcers. There are very few studies on the effect of orthoses on standing balance and gait parameters and even in some areas there was no study. However, no study has been conducted regarding the therapeutic effect of orthoses on energy consumption in these people and it is recommended that further studies be focused on this topic because of its importance.
Acknowledgements
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. We really appreciate Mrs. Arezoo Eshraghi, PhD student of Orthotics and Prosthetics and other colleagues who helped us conducting this study.
Conflict of Interest
The authors declared no conflicts of interest.
References
[1]Boulton AJM. The diabetic foot: Grand overview, epidemiology and pathogenesis. Diabetes/Metabolism Research and Reviews. 2008; 24(S1):3–6. doi: 10.1002/dmrr.833
[2]Paton J, Bruce G, Jones R, Stenhouse E. Effectiveness of insoles used for the prevention of ulceration in the neuropathic diabetic foot: A systematic review. Journal of Diabetes and its Complications. 2011; 25(1):52–62. doi: 10.1016/j.jdiacomp.2009.09.002
[3]Edmonds ME. The diabetic foot: Pathophysiology and treatment. Clinics in Endocrinology and Metabolism. 1986; 15(4):889–916. doi: 10.1016/s0300-595x(86)80079-2
[4]Boulton AJM, Vileikyte L, Ragnarson-Tennvall G, Apelqvist J. The global burden of diabetic foot disease. The Lancet. 2005; 366(9498):1719-24. doi: 10.1016/s0140-6736(05)67698-2
[5]Kwon OY, Mueller MJ. Walking Patterns used to reduce forefoot plantar pressures in people with diabetic neuropathies. Physical Therapy. 2001; 81(2):828–35. doi: 10.1093/ptj/81.2.828
[6]Hoar A. A case study for off-loading. Wound Care Canada. 2008; 6(1):58-59.
[7]Cavanagh PR. Therapeutic footwear for people with diabetes. Diabetes/Metabolism Research and Reviews. 2004; 20(S1):51–55. doi: 10.1002/dmrr.435
[8]Guldemond NA, Leffers P, Sanders AP, Schaper NC, Nieman F, Walenkamp GHIM. Daily-life activities and in-shoe forefoot plantar pressure in patients with diabetes. Diabetes Research and Clinical Practice. 2007; 77(2):203–9. doi: 10.1016/j.diabres.2006.11.006
[9]Giacomozzi C, Sawacha Z, Uccioli L, D’Ambrogi E, Avogaro A, Cobelli C. The role of shear stress in the aetiology of diabetic neuropathic foot ulcers. Journal of Foot and Ankle Research. 2008; 1(Suppl 1):O3. doi: 10.1186/1757-1146-1-s1-o3
[10]Wrobel JS, Najafi B. Diabetic foot biomechanics and gait dysfunction. Journal of Diabetes Science and Technology. 2010; 4(4):833–45. doi:10.1177/193229681000400411
[11]Sacco ICN, Hamamoto AN, Gomes AA, Onodera AN, Hirata RP, Hennig EM. Role of ankle mobility in foot rollover during gait in individuals with diabetic neuropathy. Clinical Biomechanics. 2009; 24(8):687–92. doi: 10.1016/j.clinbiomech.2009.05.003
[12]Menz HB, Lord SR, St George R, Fitzpatrick RC. Walking stability and sensorimotor function in older people with diabetic peripheral neuropathy. Archives of Physical Medicine and Rehabilitation. 2004; 85(2):245–52. doi: 10.1016/j.apmr.2003.06.015
[13]Dingwell J., Cusumano J., Sternad D, Cavanagh P. Slower speeds in patients with diabetic neuropathy lead to improved local dynamic stability of continuous overground walking. Journal of Biomechanics. 2000; 33(10):1269–77. doi: 10.1016/s0021-9290(00)00092-0
[14]Nair KS, Halliday D, Garrow JS. Increased energy expenditure in poorly controlled Type 1 (insulin-dependent) diabetic patients. Diabetologia. 1984; 27(1):13-16. doi: 10.1007/bf00253494
[15]Eng J, Teasell R, Miller W, Wolfe D, Townson A, Aubut J-A, et al. Spinal cord injury rehabilitation evidence: Method of the scire systematic review. Topics in Spinal Cord Injury Rehabilitation. 2007; 13(1):1–10. doi: 10.1310/sci1301-1
[16]Bus SA. Foot structure and footwear prescription in diabetes mellitus. Diabetes/Metabolism Research and Reviews. 2008;24(S1):S90–S95. doi: 10.1002/dmrr.840
[17]Cheung RTH, Ng GYF. Influence of different footwear on force of landing during running. Physical therapy. 2008; 88(5):620-8. doi: 10.2522/ptj.20060323
[18]Bus SA, Haspels R, Busch-Westbroek TE. Evaluation and optimization of therapeutic footwear for neuropathic diabetic foot patients using in-shoe plantar pressure analysis. Diabetes Care. 2011; 34(7):1595–600. doi: 10.2337/dc10-2206
[19]Fiedler KE, Stuijfzand WJA, Harlaar J, Dekker J, Beckerman H. The effect of shoe lacing on plantar pressure distribution and in-shoe displacement of the foot in healthy participants. Gait & Posture. 2011; 33(3):396–400. doi: 10.1016/j.gaitpost.2010.12.011
[20]Waaijman R, Arts MLJ, Haspels R, Busch-Westbroek TE, Nollet F, Bus SA. Pressure-reduction and preservation in custom-made footwear of patients with diabetes and a history of plantar ulceration. Diabetic Medicine. 2012; 29(12):1542–9. doi: 10.1111/j.1464-5491.2012.03700.x
[21]Giacalone VF, Armstrong DG, Ashry HR, Lavery DC, Harkless LB, Lavery LA. A quantitative assessment of healing sandals and postoperative shoes in offloading the neuropathic diabetic foot. The Journal of Foot and Ankle Surgery. 1997; 36(1):28–30. doi: 10.1016/s1067-2516(97)80007-5
[22]Guldemond NA, Leffers P, Schaper NC, Sanders AP, Nieman F, Willems P, et al. The effects of insole configurations on forefoot plantar pressure and walking convenience in diabetic patients with neuropathic feet. Clinical Biomechanics. 2007; 22(1):81–7. doi: 10.1016/j.clinbiomech.2006.08.004
[23]Bus SA, Ulbrecht JS, Cavanagh PR. Pressure relief and load redistribution by custom-made insoles in diabetic patients with neuropathy and foot deformity. Clinical Biomechanics. 2004; 19(6):629–38. doi: 10.1016/j.clinbiomech.2004.02.010
In this regard, there is no article showing that using any orthotic devices in diabetic patients would change energy consumption.
Spatial-temporal parameters of gait
Very few studies are found in the field of spatial-temporal parameters of gait and the effect of orthosis on these people in a way that only two systematic review studies were found on shoes [45, 46]. Only one article was found as case control [22] regarding the effect of the insole in this context. During the researcher’s investigation about rocker, two articles were found, where one of them was article review [32] and the other one was RCT [34]. Only one RCT article was found [34] regarding the ankle orthosis which partially addressed this subject. Eventually, like standing balance, the study results regarding the impact of therapeutic instruments and spatial-temporal parameters on gait are very limited and indicate that these instruments have little effect on gait parameters, especially speed and only partially change range of motion in some joints. Even there are contradictory results regarding the effect of rocker on sagittal plane movements of foot.
4. Discussion
Plantar pressure
Our study results indicate that shoe type and its properties are effective in reducing the applied forces exerted on the plantar area of the feet, and shoes can decrease the maximum pressure and its exertion time on all areas of the foot, especially the anterior area. In addition, it is observed that using insole alone has no significant effect in reducing plantar pressure and yet the best insole is the one that is built customized, based on the individual sizes, and also considering the plantar pressure. Moreover, the greatest effect is noted when the insole is used with an appropriate footwear. Using rocker and its effect is stronger than previous two orthoses. Reported results of the studies show that using rocker is very effective for healing the wound or preventing the ulcer in diabetic foot, especially, if the rocker is placed outside the shoes and standard insoles inside it. It is worth noting that rocker type, slope, and the location of its tip are very effective in reduction or elimination of pressure from wounded areas of the foot. There are few studies about ankle orthosis and reducing the pressure on the plantar area, and available articles are not valid regarding their results. A few studies were found regarding the use of plaster with full contact, but all of them strongly supported the use of plaster. Results show that fiber glass plaster with full contact compare to the other means is more useful in reducing the extent of diabetic ulcers and the recovery rate.
Standing balance
Studies are very limited regarding the impact of therapeutic instruments on standing balance, and in most research areas, there is no study; however, results of available studies show effectiveness of using a standard insole with especial shoe on regaining the lost stabilization. Yet, only one paper was found regarding the impact of rocker on the balance of diabetic patients which reminds that rocker decreases sensation and as a result, increases risk of falling in a person with diabetes. No valid study was found on using plaster, which on its results can be relied.
Energy consumption
There is no article in this regard showing that using any orthotic devices in diabetes patients, changes energy consumption. And given the importance of energy efficiency in patients with diabetes, it is suggested that future studies cover this issue.
Spatial-temporal parameters of gait
Like standing balance, the study results regarding the impact of therapeutic instruments and spatial-temporal parameters on gait are very limited and indicate that these instruments have little effect on gait parameters, especially speed and they only partially change range of motion in some joints. Even there are contradictory results regarding the effect of rocker on sagittal plane movements of the foot.
Our study has some limitations such as lack of access to some sites and articles and unavailability of the full text of some articles. This study has also some suggestions; This research included all sorts of article designs from RCT to case reports. Most studies emphasized treatment of foot plantar ulcers in diabetic patients and the role of orthoses interventions in achieving this goal. Also, most shoes and orthoses aimed at reducing the pressure from the wounded areas and the risk of developing ulcers. There are very few studies on the effect of orthoses on standing balance and gait parameters and even in some areas there was no study. However, no study has been conducted regarding the therapeutic effect of orthoses on energy consumption in these people and it is recommended that further studies be focused on this topic because of its importance.
Acknowledgements
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. We really appreciate Mrs. Arezoo Eshraghi, PhD student of Orthotics and Prosthetics and other colleagues who helped us conducting this study.
Conflict of Interest
The authors declared no conflicts of interest.
References
[1]Boulton AJM. The diabetic foot: Grand overview, epidemiology and pathogenesis. Diabetes/Metabolism Research and Reviews. 2008; 24(S1):3–6. doi: 10.1002/dmrr.833
[2]Paton J, Bruce G, Jones R, Stenhouse E. Effectiveness of insoles used for the prevention of ulceration in the neuropathic diabetic foot: A systematic review. Journal of Diabetes and its Complications. 2011; 25(1):52–62. doi: 10.1016/j.jdiacomp.2009.09.002
[3]Edmonds ME. The diabetic foot: Pathophysiology and treatment. Clinics in Endocrinology and Metabolism. 1986; 15(4):889–916. doi: 10.1016/s0300-595x(86)80079-2
[4]Boulton AJM, Vileikyte L, Ragnarson-Tennvall G, Apelqvist J. The global burden of diabetic foot disease. The Lancet. 2005; 366(9498):1719-24. doi: 10.1016/s0140-6736(05)67698-2
[5]Kwon OY, Mueller MJ. Walking Patterns used to reduce forefoot plantar pressures in people with diabetic neuropathies. Physical Therapy. 2001; 81(2):828–35. doi: 10.1093/ptj/81.2.828
[6]Hoar A. A case study for off-loading. Wound Care Canada. 2008; 6(1):58-59.
[7]Cavanagh PR. Therapeutic footwear for people with diabetes. Diabetes/Metabolism Research and Reviews. 2004; 20(S1):51–55. doi: 10.1002/dmrr.435
[8]Guldemond NA, Leffers P, Sanders AP, Schaper NC, Nieman F, Walenkamp GHIM. Daily-life activities and in-shoe forefoot plantar pressure in patients with diabetes. Diabetes Research and Clinical Practice. 2007; 77(2):203–9. doi: 10.1016/j.diabres.2006.11.006
[9]Giacomozzi C, Sawacha Z, Uccioli L, D’Ambrogi E, Avogaro A, Cobelli C. The role of shear stress in the aetiology of diabetic neuropathic foot ulcers. Journal of Foot and Ankle Research. 2008; 1(Suppl 1):O3. doi: 10.1186/1757-1146-1-s1-o3
[10]Wrobel JS, Najafi B. Diabetic foot biomechanics and gait dysfunction. Journal of Diabetes Science and Technology. 2010; 4(4):833–45. doi:10.1177/193229681000400411
[11]Sacco ICN, Hamamoto AN, Gomes AA, Onodera AN, Hirata RP, Hennig EM. Role of ankle mobility in foot rollover during gait in individuals with diabetic neuropathy. Clinical Biomechanics. 2009; 24(8):687–92. doi: 10.1016/j.clinbiomech.2009.05.003
[12]Menz HB, Lord SR, St George R, Fitzpatrick RC. Walking stability and sensorimotor function in older people with diabetic peripheral neuropathy. Archives of Physical Medicine and Rehabilitation. 2004; 85(2):245–52. doi: 10.1016/j.apmr.2003.06.015
[13]Dingwell J., Cusumano J., Sternad D, Cavanagh P. Slower speeds in patients with diabetic neuropathy lead to improved local dynamic stability of continuous overground walking. Journal of Biomechanics. 2000; 33(10):1269–77. doi: 10.1016/s0021-9290(00)00092-0
[14]Nair KS, Halliday D, Garrow JS. Increased energy expenditure in poorly controlled Type 1 (insulin-dependent) diabetic patients. Diabetologia. 1984; 27(1):13-16. doi: 10.1007/bf00253494
[15]Eng J, Teasell R, Miller W, Wolfe D, Townson A, Aubut J-A, et al. Spinal cord injury rehabilitation evidence: Method of the scire systematic review. Topics in Spinal Cord Injury Rehabilitation. 2007; 13(1):1–10. doi: 10.1310/sci1301-1
[16]Bus SA. Foot structure and footwear prescription in diabetes mellitus. Diabetes/Metabolism Research and Reviews. 2008;24(S1):S90–S95. doi: 10.1002/dmrr.840
[17]Cheung RTH, Ng GYF. Influence of different footwear on force of landing during running. Physical therapy. 2008; 88(5):620-8. doi: 10.2522/ptj.20060323
[18]Bus SA, Haspels R, Busch-Westbroek TE. Evaluation and optimization of therapeutic footwear for neuropathic diabetic foot patients using in-shoe plantar pressure analysis. Diabetes Care. 2011; 34(7):1595–600. doi: 10.2337/dc10-2206
[19]Fiedler KE, Stuijfzand WJA, Harlaar J, Dekker J, Beckerman H. The effect of shoe lacing on plantar pressure distribution and in-shoe displacement of the foot in healthy participants. Gait & Posture. 2011; 33(3):396–400. doi: 10.1016/j.gaitpost.2010.12.011
[20]Waaijman R, Arts MLJ, Haspels R, Busch-Westbroek TE, Nollet F, Bus SA. Pressure-reduction and preservation in custom-made footwear of patients with diabetes and a history of plantar ulceration. Diabetic Medicine. 2012; 29(12):1542–9. doi: 10.1111/j.1464-5491.2012.03700.x
[21]Giacalone VF, Armstrong DG, Ashry HR, Lavery DC, Harkless LB, Lavery LA. A quantitative assessment of healing sandals and postoperative shoes in offloading the neuropathic diabetic foot. The Journal of Foot and Ankle Surgery. 1997; 36(1):28–30. doi: 10.1016/s1067-2516(97)80007-5
[22]Guldemond NA, Leffers P, Schaper NC, Sanders AP, Nieman F, Willems P, et al. The effects of insole configurations on forefoot plantar pressure and walking convenience in diabetic patients with neuropathic feet. Clinical Biomechanics. 2007; 22(1):81–7. doi: 10.1016/j.clinbiomech.2006.08.004
[23]Bus SA, Ulbrecht JS, Cavanagh PR. Pressure relief and load redistribution by custom-made insoles in diabetic patients with neuropathy and foot deformity. Clinical Biomechanics. 2004; 19(6):629–38. doi: 10.1016/j.clinbiomech.2004.02.010
[24]Owings TM, Woerner JL, Frampton JD, Cavanagh PR, Botek G. Custom therapeutic insoles based on both foot shape and plantar pressure measurement provide enhanced pressure relief. Diabetes Care. 2008; 31(5):839–44. doi: 10.2337/dc07-2288
[25]Lavery LA, Vela SA, Fleischli JG, Armstrong DG, Lavery DC. Reducing plantar pressure in the neuropathic foot: A comparison of footwear. Diabetes Care. 1997; 20(11):1706–10. doi: 10.2337/diacare.20.11.1706
[26]Reiber GE, Smith DG, Wallace C, Sullivan K, Hayes S, Vath C, et al. Effect of therapeutic footwear on foot reulceration in patients with diabetes. JAMA. 2002; 287(19):2552-8. doi: 10.1001/jama.287.19.2552
[27]Busch K, Chantelau E. Effectiveness of a new brand of stock ‘diabetic’shoes to protect against diabetic foot ulcer relapse. A prospective cohort study. Diabetic medicine. 2003; 20(8):665-9. doi: 10.1046/j.1464-5491.2003.01003.x
[28]Uccioli L, Faglia E, Monticone G, Favales F, Durola L, Aldeghi A, et al. Manufactured shoes in the prevention of diabetic foot ulcers. Diabetes Care. 1995; 18(10):1376–8. doi: 10.2337/diacare.18.10.1376
[29]Armstrong DG, Lavery LA, Nixon BP, Boulton AJM. It's not what you put on, but what you take off: Techniques for debriding and off-loading the diabetic foot wound. Clinical infectious diseases. 2004; 39(Supplement 2):S92-S9. doi: 10.1086/383269
[30]Bus SA, van Deursen RWM, Kanade RV, Wissink M, Manning EA, van Baal JG, et al. Plantar pressure relief in the diabetic foot using forefoot offloading shoes. Gait & Posture. 2009; 29(4):618–22. doi: 10.1016/j.gaitpost.2009.01.003
[31]Praet SFE, Louwerens J-WK. The influence of shoe design on plantar pressures in neuropathic feet. Diabetes Care. 2003; 26(2):441–5. doi: 10.2337/diacare.26.2.441
[32]Hutchins S, Bowker P, Geary N, Richards J. The biomechanics and clinical efficacy of footwear adapted with rocker profiles—Evidence in the literature. The Foot. 2009; 19(3):165–70. doi: 10.1016/j.foot.2009.01.001
[33]Kavros SJ, Van Straaten MG, Coleman Wood KA, Kaufman KR. Forefoot plantar pressure reduction of off-the-shelf rocker bottom provisional footwear. Clinical Biomechanics. 2011; 26(7):778–82. doi: 10.1016/j.clinbiomech.2011.03.009
[34]Dahmen R, Haspels R, Koomen B, Hoeksma AF. Therapeutic footwear for the neuropathic foot: an algorithm. Diabetes Care. 2001; 24(4):705–9. doi: 10.2337/diacare.24.4.705
[35]Kato H, Takada T, Kawamura T, Hotta N, Torii S. The reduction and redistribution of plantar pressures using foot orthoses in diabetic patients. Diabetes Research and Clinical Practice. 1996; 31(1-3):115–8. doi: 10.1016/0168-8227(96)01214-4
[36]Mueller MJ, Diamond JE. Biomechanical treatment approach to diabetic plantar ulcers. Physical Therapy. 1988; 68(12):1917–20. doi: 10.1093/ptj/68.12.1917
[37]Rizzo L, Tedeschi A, Fallani E, Coppelli A, Vallini V, Iacopi E, et al. Custom-made orthesis and shoes in a structured follow-up program reduces the incidence of neuropathic ulcers in high-risk diabetic foot patients. The International Journal of Lower Extremity Wounds. 2012; 11(1):59–64. doi: 10.1177/1534734612438729
[38]Van Deursen R. Mechanical loading and off-loading of the plantar surface of the diabetic foot. Clinical Infectious Diseases. 2004; 39(Supplement 2):S87–S91. doi: 10.1086/383268
[39]Brown D, Wertsch JJ, Harris GF, Klein J, Janisse D. Effect of rocker soles on plantar pressures. Archives of physical medicine and rehabilitation. 2004; 85(1):81-6. PMID: 14970973
[40]Caravaggi C, Faglia E, De Giglio R, Mantero M, Quarantiello A, Sommariva E, et al. Effectiveness and safety of a nonremovable fiberglass off-bearing cast versus a therapeutic shoe in the treatment of neuropathic foot ulcers: A randomized study. Diabetes Care. 2000; 23(12):1746–51. doi: 10.2337/diacare.23.12.1746
[41]Menant JC, Perry SD, Steele JR, Menz HB, Munro BJ, Lord SR. Effects of shoe characteristics on dynamic stability when walking on even and uneven surfaces in young and older people. Archives of Physical Medicine and Rehabilitation. 2008; 89(10):1970–6. doi: 10.1016/j.apmr.2008.02.031
[42]Perry SD, Radtke A, McIlroy WE, Fernie GR, Maki BE. Efficacy and effectiveness of a balance-enhancing insole. The Journals of Gerontology Series A: Biological Sciences and Medical Sciences. 2008; 63(6):595–602. doi: 10.1093/gerona/63.6.595
[43]Reiber GE, Smith DG, Boone DA, Del Aguila M, Borchers RE, Mathews D, et al. Design and pilot testing of the DVA/Seattle Footwear System for diabetic patients with foot insensitivity. Journal of rehabilitation research and development. 1997; 34(1):1-8. PMID: 9021621
[44]Albright BC, Woodhull-Smith WM. Rocker bottom soles alter the postural response to backward translation during stance. Gait & Posture. 2009; 30(1):45–9. doi: 10.1016/j.gaitpost.2009.02.012
[45]Long JT, Klein JP, Sirota NM, Wertsch JJ, Janisse D, Harris GF. Biomechanics of the double rocker sole shoe: Gait kinematics and kinetics. Journal of Biomechanics. 2007; 40(13):2882–90. doi: 10.1016/j.jbiomech.2007.03.009
[46]Myers KA, Long JT, Klein JP, Wertsch JJ, Janisse D, Harris GF. Biomechanical implications of the negative heel rocker sole shoe: Gait kinematics and kinetics. Gait & Posture. 2006; 24(3):323–30. doi: 10.1016/j.gaitpost.2005.10.006
[47]Menant JC, Steele JR, Menz HB, Munro BJ, Lord SR. Optimizing footwear for older people at risk of falls. Journal of Rehabilitation Research & Development. 2008; 45(8):1167-81. PMID: 19235118
[48]Bus SA, Valk GD, van Deursen RW, Armstrong DG, Caravaggi C, Hlaváček P, et al. The effectiveness of footwear and offloading interventions to prevent and heal foot ulcers and reduce plantar pressure in diabetes: A systematic review. Diabetes/Metabolism Research and Reviews. 2008; 24(S1):S162–S180. doi: 10.1002/dmrr.850
[25]Lavery LA, Vela SA, Fleischli JG, Armstrong DG, Lavery DC. Reducing plantar pressure in the neuropathic foot: A comparison of footwear. Diabetes Care. 1997; 20(11):1706–10. doi: 10.2337/diacare.20.11.1706
[26]Reiber GE, Smith DG, Wallace C, Sullivan K, Hayes S, Vath C, et al. Effect of therapeutic footwear on foot reulceration in patients with diabetes. JAMA. 2002; 287(19):2552-8. doi: 10.1001/jama.287.19.2552
[27]Busch K, Chantelau E. Effectiveness of a new brand of stock ‘diabetic’shoes to protect against diabetic foot ulcer relapse. A prospective cohort study. Diabetic medicine. 2003; 20(8):665-9. doi: 10.1046/j.1464-5491.2003.01003.x
[28]Uccioli L, Faglia E, Monticone G, Favales F, Durola L, Aldeghi A, et al. Manufactured shoes in the prevention of diabetic foot ulcers. Diabetes Care. 1995; 18(10):1376–8. doi: 10.2337/diacare.18.10.1376
[29]Armstrong DG, Lavery LA, Nixon BP, Boulton AJM. It's not what you put on, but what you take off: Techniques for debriding and off-loading the diabetic foot wound. Clinical infectious diseases. 2004; 39(Supplement 2):S92-S9. doi: 10.1086/383269
[30]Bus SA, van Deursen RWM, Kanade RV, Wissink M, Manning EA, van Baal JG, et al. Plantar pressure relief in the diabetic foot using forefoot offloading shoes. Gait & Posture. 2009; 29(4):618–22. doi: 10.1016/j.gaitpost.2009.01.003
[31]Praet SFE, Louwerens J-WK. The influence of shoe design on plantar pressures in neuropathic feet. Diabetes Care. 2003; 26(2):441–5. doi: 10.2337/diacare.26.2.441
[32]Hutchins S, Bowker P, Geary N, Richards J. The biomechanics and clinical efficacy of footwear adapted with rocker profiles—Evidence in the literature. The Foot. 2009; 19(3):165–70. doi: 10.1016/j.foot.2009.01.001
[33]Kavros SJ, Van Straaten MG, Coleman Wood KA, Kaufman KR. Forefoot plantar pressure reduction of off-the-shelf rocker bottom provisional footwear. Clinical Biomechanics. 2011; 26(7):778–82. doi: 10.1016/j.clinbiomech.2011.03.009
[34]Dahmen R, Haspels R, Koomen B, Hoeksma AF. Therapeutic footwear for the neuropathic foot: an algorithm. Diabetes Care. 2001; 24(4):705–9. doi: 10.2337/diacare.24.4.705
[35]Kato H, Takada T, Kawamura T, Hotta N, Torii S. The reduction and redistribution of plantar pressures using foot orthoses in diabetic patients. Diabetes Research and Clinical Practice. 1996; 31(1-3):115–8. doi: 10.1016/0168-8227(96)01214-4
[36]Mueller MJ, Diamond JE. Biomechanical treatment approach to diabetic plantar ulcers. Physical Therapy. 1988; 68(12):1917–20. doi: 10.1093/ptj/68.12.1917
[37]Rizzo L, Tedeschi A, Fallani E, Coppelli A, Vallini V, Iacopi E, et al. Custom-made orthesis and shoes in a structured follow-up program reduces the incidence of neuropathic ulcers in high-risk diabetic foot patients. The International Journal of Lower Extremity Wounds. 2012; 11(1):59–64. doi: 10.1177/1534734612438729
[38]Van Deursen R. Mechanical loading and off-loading of the plantar surface of the diabetic foot. Clinical Infectious Diseases. 2004; 39(Supplement 2):S87–S91. doi: 10.1086/383268
[39]Brown D, Wertsch JJ, Harris GF, Klein J, Janisse D. Effect of rocker soles on plantar pressures. Archives of physical medicine and rehabilitation. 2004; 85(1):81-6. PMID: 14970973
[40]Caravaggi C, Faglia E, De Giglio R, Mantero M, Quarantiello A, Sommariva E, et al. Effectiveness and safety of a nonremovable fiberglass off-bearing cast versus a therapeutic shoe in the treatment of neuropathic foot ulcers: A randomized study. Diabetes Care. 2000; 23(12):1746–51. doi: 10.2337/diacare.23.12.1746
[41]Menant JC, Perry SD, Steele JR, Menz HB, Munro BJ, Lord SR. Effects of shoe characteristics on dynamic stability when walking on even and uneven surfaces in young and older people. Archives of Physical Medicine and Rehabilitation. 2008; 89(10):1970–6. doi: 10.1016/j.apmr.2008.02.031
[42]Perry SD, Radtke A, McIlroy WE, Fernie GR, Maki BE. Efficacy and effectiveness of a balance-enhancing insole. The Journals of Gerontology Series A: Biological Sciences and Medical Sciences. 2008; 63(6):595–602. doi: 10.1093/gerona/63.6.595
[43]Reiber GE, Smith DG, Boone DA, Del Aguila M, Borchers RE, Mathews D, et al. Design and pilot testing of the DVA/Seattle Footwear System for diabetic patients with foot insensitivity. Journal of rehabilitation research and development. 1997; 34(1):1-8. PMID: 9021621
[44]Albright BC, Woodhull-Smith WM. Rocker bottom soles alter the postural response to backward translation during stance. Gait & Posture. 2009; 30(1):45–9. doi: 10.1016/j.gaitpost.2009.02.012
[45]Long JT, Klein JP, Sirota NM, Wertsch JJ, Janisse D, Harris GF. Biomechanics of the double rocker sole shoe: Gait kinematics and kinetics. Journal of Biomechanics. 2007; 40(13):2882–90. doi: 10.1016/j.jbiomech.2007.03.009
[46]Myers KA, Long JT, Klein JP, Wertsch JJ, Janisse D, Harris GF. Biomechanical implications of the negative heel rocker sole shoe: Gait kinematics and kinetics. Gait & Posture. 2006; 24(3):323–30. doi: 10.1016/j.gaitpost.2005.10.006
[47]Menant JC, Steele JR, Menz HB, Munro BJ, Lord SR. Optimizing footwear for older people at risk of falls. Journal of Rehabilitation Research & Development. 2008; 45(8):1167-81. PMID: 19235118
[48]Bus SA, Valk GD, van Deursen RW, Armstrong DG, Caravaggi C, Hlaváček P, et al. The effectiveness of footwear and offloading interventions to prevent and heal foot ulcers and reduce plantar pressure in diabetes: A systematic review. Diabetes/Metabolism Research and Reviews. 2008; 24(S1):S162–S180. doi: 10.1002/dmrr.850
Type of Study: case report |
Subject:
Sport injury and corrective exercises
Received: 2014/12/5 | Accepted: 2017/05/1 | Published: 2017/08/6
Received: 2014/12/5 | Accepted: 2017/05/1 | Published: 2017/08/6
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
This is an open access article distributed under the terms of the Creative Commons Attribution-NonCommercial 4.0 (CC-By-NC 4.0), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
