Wed, Jun 26, 2024
Volume 14, Issue 2 (Spring 2024)
PTJ 2024, 14(2): 125-136 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Babaei H, Alizadeh M H, Minoonezhad H, Movahed A, Maher R. Effectiveness of the Alexander Technique on Quality of Life in Young Men With Upper Crossed Syndrome. PTJ 2024; 14 (2) :125-136
URL: http://ptj.uswr.ac.ir/article-1-576-en.html
URL: http://ptj.uswr.ac.ir/article-1-576-en.html
Effectiveness of the Alexander Technique on Quality of Life in Young Men With Upper Crossed Syndrome



1- Department of Physical Education, Faculty of Psychology and Educational Sciences, Payame Noor University, Tehran, Iran.
2- Department of Sports Pathology and Corrective Movements, Faculty of Sports Sciences, University of Tehran, Tehran, Iran.
3- Department of Music, College of Fine Arts, University of Tehran, Tehran, Iran.
4- Institute of Health & Sport, Victoria University, Melbourne, Australia.
2- Department of Sports Pathology and Corrective Movements, Faculty of Sports Sciences, University of Tehran, Tehran, Iran.
3- Department of Music, College of Fine Arts, University of Tehran, Tehran, Iran.
4- Institute of Health & Sport, Victoria University, Melbourne, Australia.
Keywords: Alexander technique, Quality of life (QoL), Upper crossed syndrome, Physical health, Mental health
Full-Text [PDF 846 kb]
(58 Downloads)
| Abstract (HTML) (542 Views)
Full-Text: (31 Views)
Introduction
In modern life, a vast majority of people are suffering from disorders caused by inappropriate use of muscles and improper daily postures, which consequently lead to deformities in the human body’s posture [1]. Upper-crossed syndrome is currently one of the physical abnormalities that has a high prevalence [2]. The prevalence of upper-crossed syndrome has been reported in 32.4% of employees, 24.3% of drivers, and 27% of housewives [3]. In this deformity, thoracic kyphosis increases because of the decrease in the endurance and strength of the spinal extensor muscles [4]. Moreover, it may generate undesirable consequences in the body, such as reduced physical performance [5], pulmonary dysfunction [6], balance disorder [7], difficulty in doing daily life activities [8], and decrease in health and quality of life (QoL) [9, 10]. The upper crossed syndrome due to poor posture and inappropriate appearance (from an aesthetic point of view) accompanied by the presence of physical complications may lead to anxiety and reduced self-esteem [11]. A combination of these issues negatively affects patients’ physical and mental health and eventually decreases their QoL [10]. Given the high prevalence and various physiological and psychological complications of upper-crossed syndrome, the importance of correcting this deformity is crucial.
A variety of corrective methods have been used for people with upper-crossed syndrome, including manual therapy, exercise, the use of tapes, assistive devices, and posture re-education [12]. In recent years, the attention of health professionals has been focused on posture training as a method to prevent and correct musculoskeletal system disorders, especially head, neck, and trunk abnormalities. One of the relatively common methods of body posture re-education is the Alexander technique [13]. Although the Alexander technique was initially utilized by artists, researchers in the field of health and rehabilitation have recently become interested in the application of this technique in various health-related cases [14]. Despite the current application of the Alexander technique by researchers, it is still under investigation compared to the other methods and interventions.
The purpose of the Alexander technique is to help a person increase body awareness and use this information to achieve a more efficient performance. Alexander technique training sessions include posture exercises from lying down and sitting to more dynamic positions, such as standing up and walking, and special activities like working at a desk, studying, and playing the guitar [15]. This technique uses the teacher-student paradigm instead of the therapist-patient paradigm and its main focus is on education and not treatment [16]. Alexander technique enables people to become aware of their posture in a sensorimotor way and to change their faulty habitual movement patterns [13]. In this method, the person learns to identify the sources causing the tension response in the body, to prevent faulty habitual movement patterns, and to replace it with an efficient movement pattern according to the timing, direction, and stress reduction with an emphasis on the head, neck, and trunk [15]. Frederick Mathias Alexander, the inventor of this method, believed that movement is created not only by the body but also by the mind, and he called the division of the human organism into mental and physical parts a mistake [17]. The Alexander technique has a low degree of commonality with other corrective methods using stretching or muscle-strengthening exercises. In this method, the conscious use of the individual as an active method of psychophysical re-education is desired [18]. The effectiveness of the Alexander technique on various cases, such as back pain [19], neck pain [20], problems of the elderly [21], and Parkinson disease [22] has been investigated so far. Despite the reported findings related to the benefits of the Alexander technique, there is still insufficient scientific evidence to confirm the effectiveness of this technique in most health-related fields and a demand for more comprehensive and controlled studies is evident [14].
Nowadays, QoL is considered a basic index for evaluating various dimensions of people’s health in human societies, and its investigation is of special importance. QoL refers to the concept of how well people consider their daily life in different physical, psychological, and social dimensions to be good and desirable and follow social and universal standards [23]. One of the fields in which the most research on QoL has been conducted is healthcare [24]. The musculoskeletal condition of the spine is one of the main causes of pain that ultimately reduces one’s QoL [25]. The findings of existing research show the relationship between postural defects and QoL and state that correct body posture is one of the most effective indicators of health and QoL [26]; therefore, interventions and methods that help to improve posture will probably enhance the QoL. Furthermore, the Alexander technique can boost the functional quality of movement and amplify the QoL by increasing body awareness [14]. In a study that investigated the effectiveness of the Alexander technique, massage therapy, and exercise therapy on chronic back pain, the researchers concluded that Alexander technique training by trained instructors has created long-term benefits in patients with chronic back pain and improved their QoL significantly [19]. Also, in a review study titled “Alexander technique for chronic asthma,” the authors stated conclusively that clinical studies consisting of controlled and strong methodologies are needed to delve into the effect of the Alexander technique on various aspects of human health and the QoL among those who are exposed to different disorders [27].
A limited number of studies have been conducted on the Alexander technique in the country [22, 28]. We found that the existing studies used the Alexander technique as an exercise or a treatment (this technique is only training). Most importantly, lacking supervision by an Alexander technique expert in the design and implementation of the protocol in these studies attenuated the quality of their research. Therefore, it is necessary to conduct research containing a more efficient methodology by applying the correct training protocol under the supervision of a certified Alexander technique specialist. The majority of the studies in connection with the effect of the Alexander technique consist of diseases, such as back pain [19] and Parkinson [22, 28]. Considering the high prevalence of upper crossed syndrome [2, 3] and the negative effects of this abnormality on various aspects of one’s life, their QoL in particular [9, 10], the necessity of conducting research comprising the Alexander technique, QoL, and upper crossed syndrome was evident; therefore, this study investigated the effect of the Alexander technique on the physical and mental dimensions of QoL in young men with upper crossed syndrome.
Materials and Methods
Study participants
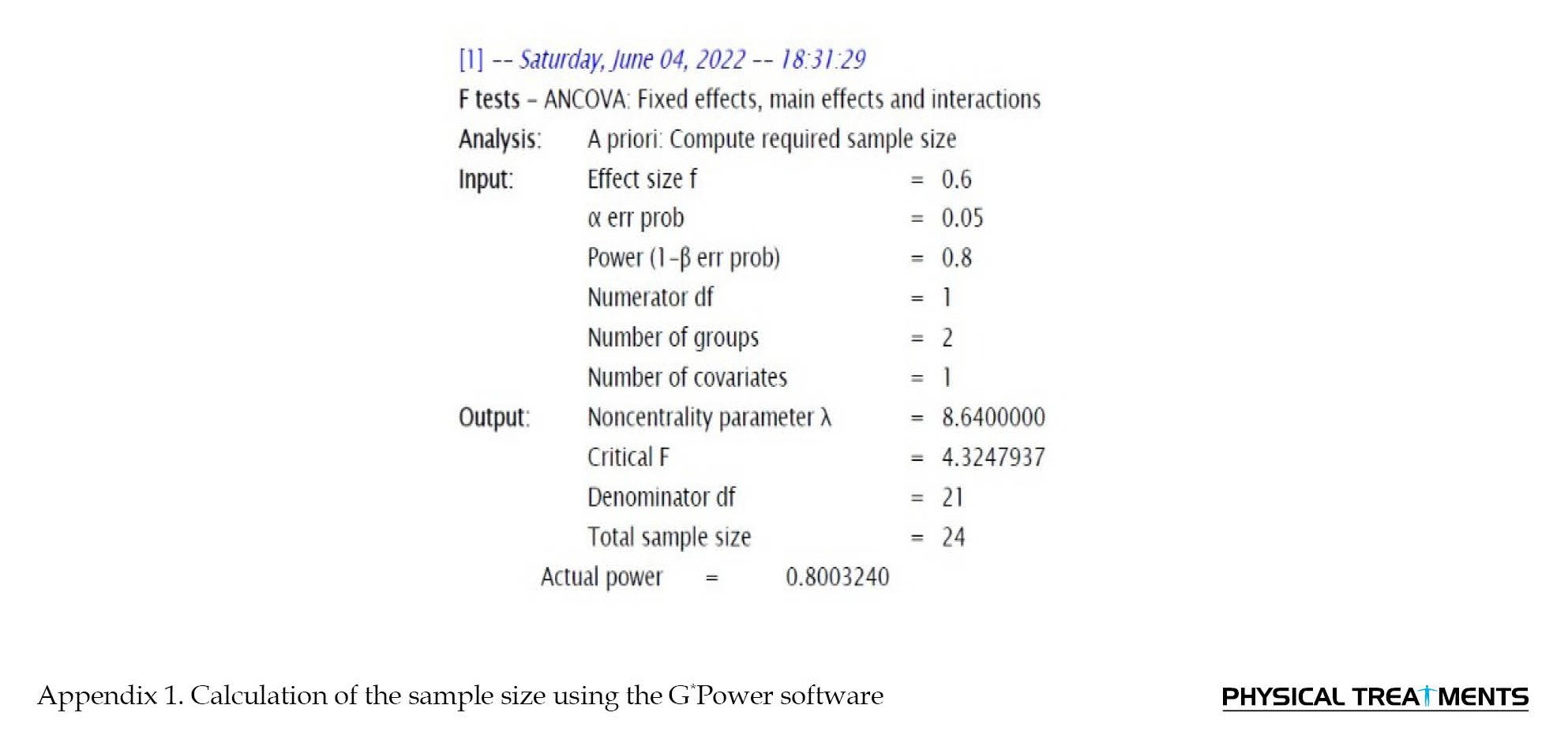
Using the convenience sampling method, we selected 24 male university students aged 19-25 years for the current study and randomly divided them into an experimental (n=12) and a control group (n=12). We distributed the invitations to absorb volunteer male students at the University of Tehran to participate in the first phase of the study. After an initial screening by posture grid, the students with upper crossed syndrome were diagnosed and selected as samples. The criteria for sample size (n=24) were based on the variable of QoL and using the G*Power software [29] with the assumptions of the confidence coefficient of 95% (α=0.05), statistical power 80% (β=0.2), and the effect size (d=0.6) (Appendix 1).
 In addition to the age and gender, the other inclusion criteria were normal body mass index between 18.5 to 24.9 kg/m2, forward head deformity greater than 46 degrees, kyphosis greater than 42 degrees, and forward shoulder greater than 52 degrees [30]. Those volunteers who had a history of fractures, surgery, or problems in the spine, shoulder girdle, and pelvis, visual or hearing impairment, and depression, anxiety, or mental disorders were excluded from the study.
In addition to the age and gender, the other inclusion criteria were normal body mass index between 18.5 to 24.9 kg/m2, forward head deformity greater than 46 degrees, kyphosis greater than 42 degrees, and forward shoulder greater than 52 degrees [30]. Those volunteers who had a history of fractures, surgery, or problems in the spine, shoulder girdle, and pelvis, visual or hearing impairment, and depression, anxiety, or mental disorders were excluded from the study.
Study design
The current research design was semi-experimental containing two conditions: a) An experimental condition, and b) A control condition. A total of 12 participants were allocated in each condition. A pre-test and post-test was conducted before and after interventions. The study was conducted blindly and the information that could cause the deviation of the study results was not presented to the participants till the completion of the study.
Before starting the study, we debriefed the participants about the intervention, the confidentiality of the results, and the right to withdraw at any stage of the research. Subsequently, written consent was obtained from them to participate in the study and participants’ information was collected using demographic questionnaires, a digital scale, and a digital meter (to accurately measure their height and weight and calculate their body mass index). To evaluate the posture of the subjects, the forward head and forward shoulder angles were measured by photogrammetric method and the kyphosis angle was accurately measured using a flexible ruler. The measurements were carried out by the main researcher at the health center of University of Tehran. During the intervention, the participants of the experimental condition received the educational intervention of the Alexander technique according to the predetermined protocol for six weeks. Alexander technique training sessions were held in a classroom with adequate space, ventilation, and light. The control condition was not subjected to any special education and training and the participants of the control condition were only evaluated in the pre-test and post-test.
The goal of the Alexander technique training protocol was to increase body awareness, correct inappropriate movement habits, and help participants function correctly in daily activities. During the experimental condition, the participants were taught the Alexander technique using manual guidance, and verbal, visual, and proprioception feedback. In the first two sessions, we concentrated on the participants’ familiarity with the Alexander technique, explaining goals, and identifying their weak physical habits and inefficient movement patterns. In the following sessions, we instructed the participants about the following items: a) The correct way to hold the head, neck, and spine while sitting, standing, and walking; b) The correct way to sit and stand up; c) The correct way to sit and lift objects; d) The correct way to work in a bent position; e) The correct way to carry bags and equipment; f) The correct posture when writing and reading; g) The correct expressions of the face and eyes; and h) The correct way of breathing [28]. During these sessions, the participants tried to familiarize themselves with the basic concepts of Alexander’s technique, including inhibition, primary control, and direction, in addition to correcting wrong body habits and improving movement patterns. They were also asked to apply the acquired knowledge in their daily activities.
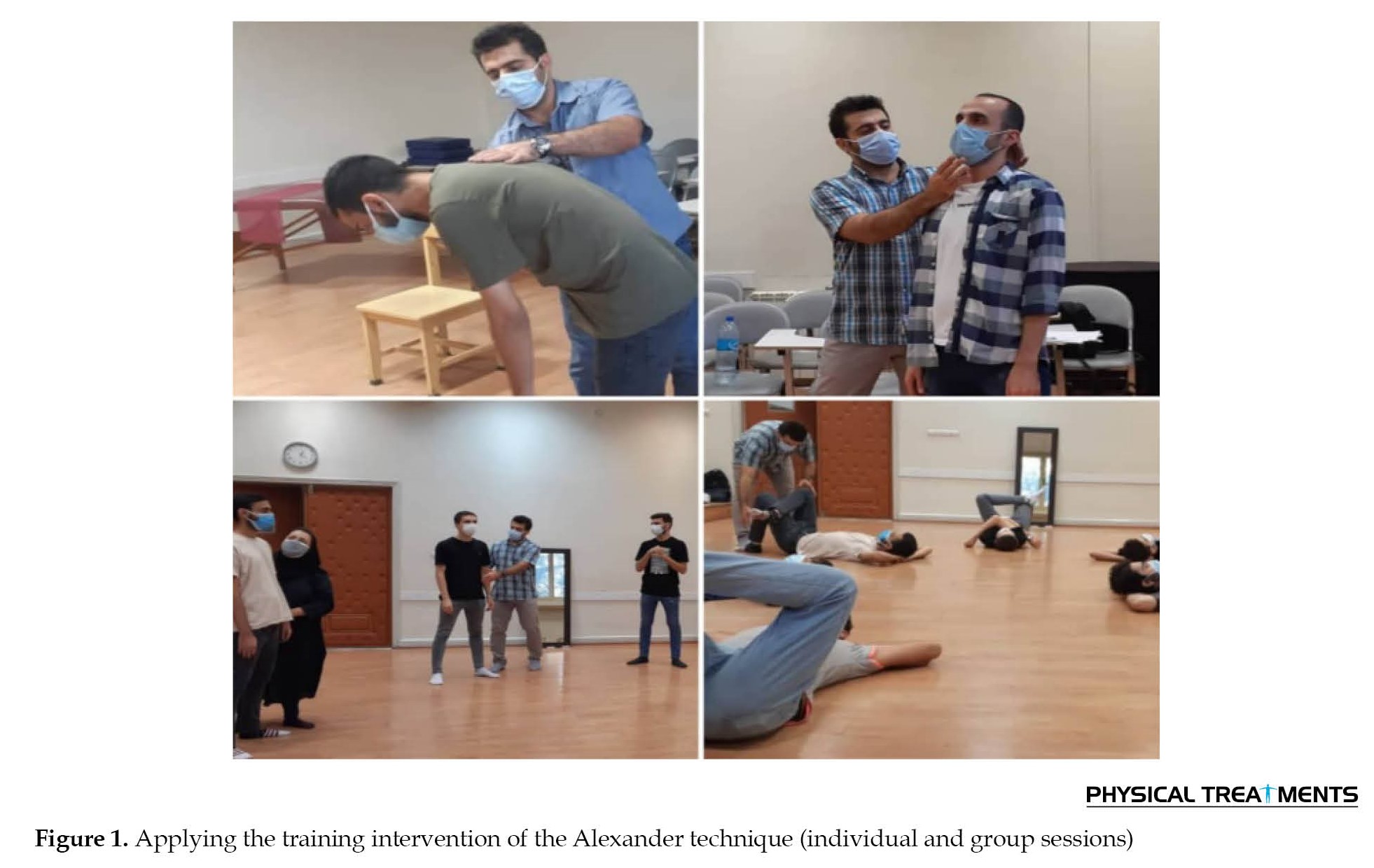
To obtain sufficient expertise for instructing the Alexander technique to the participants, the first author completed the necessary training (24 training sessions within 3 months) under the supervision of an Alexander technique expert and familiarized himself with the core principles of the technique. The training protocol for the current study was then designed by seeking advice from the certified expert. The Alexander technique protocol was applied by the participants under the direct supervision of the first author throughout the study (Figure 1).
 According to the designed Alexander technique protocol, the participants of the experimental condition completed 12 training sessions within 6 weeks (two sessions weekly). Individualized training sessions were conducted during the first four weeks for each participant. The participants attended group sessions instead of individualized sessions during the last two weeks of the interventions. Each individualized session of the Alexander technique was 40 min consisting of the following items: a) Examining body habits and patterns during various activities (5 min); b) Teaching and applying the basic principles of Alexander technique, including inhibition, primary control, and direction in various activities, such as sitting, standing, walking, studying, and lifting objects using tactile and verbal feedback (30 min); and c) Question and answer by the participants and teaching how to use the Alexander technique in daily activities (5 min). After completing eight individualized sessions within four weeks, the participants finalized their intervention phase by completing four 60-min group sessions within the remaining two weeks. The emphasis of the group sessions was on repeating and reminding the basic principles of the Alexander technique using minimal contact and verbal feedback to increase the participants’ independence for the practical use of the Alexander technique in daily activities. A total of 104 training sessions of the Alexander technique composed of 96 individualized training sessions and eight group training sessions were conducted throughout the experimental condition. All participants attended the sessions following the schedule and only one participant missed one of his individualized and one of his group sessions (total attendance rate=0.98). In the group phase of the intervention, the participants were divided into two separate groups (six participants in each group) to comply with the existing health protocols.
According to the designed Alexander technique protocol, the participants of the experimental condition completed 12 training sessions within 6 weeks (two sessions weekly). Individualized training sessions were conducted during the first four weeks for each participant. The participants attended group sessions instead of individualized sessions during the last two weeks of the interventions. Each individualized session of the Alexander technique was 40 min consisting of the following items: a) Examining body habits and patterns during various activities (5 min); b) Teaching and applying the basic principles of Alexander technique, including inhibition, primary control, and direction in various activities, such as sitting, standing, walking, studying, and lifting objects using tactile and verbal feedback (30 min); and c) Question and answer by the participants and teaching how to use the Alexander technique in daily activities (5 min). After completing eight individualized sessions within four weeks, the participants finalized their intervention phase by completing four 60-min group sessions within the remaining two weeks. The emphasis of the group sessions was on repeating and reminding the basic principles of the Alexander technique using minimal contact and verbal feedback to increase the participants’ independence for the practical use of the Alexander technique in daily activities. A total of 104 training sessions of the Alexander technique composed of 96 individualized training sessions and eight group training sessions were conducted throughout the experimental condition. All participants attended the sessions following the schedule and only one participant missed one of his individualized and one of his group sessions (total attendance rate=0.98). In the group phase of the intervention, the participants were divided into two separate groups (six participants in each group) to comply with the existing health protocols.
The emphasis of the Alexander technique training sessions was on the benefits of increasing self-awareness during the activity. The participants were encouraged to self-evaluate while performing their usual daily activities, such as standing, sitting, working with the computer, personal tasks, and housework, and most importantly, to apply the learned principles of the Alexander technique to improve physical and movement habits. We used tactile feedback to teach the subjects how to maintain a coherent connection of different parts of the body during the activities. We also asked them to communicate any problems in understanding and implementing the movements so that the training could be completed correctly and accurately.
The short form (SF-36) health survey was used to assess the participants’ QoL. This self-report questionnaire is a 36-item scale which is designed by Ware and Sherburne [31]. The SF-36 questionnaire evaluates two general dimensions of QoL, which include the physical health dimension (physical function, physical role limitations, bodily pain, and general health perception) and the mental health dimension (energy/vitality, social functioning, emotional role limitations, and mental health). The outcome is evaluated through the score of the physical dimension and the score of the mental dimension, respectively [32]. A Likert scale from 1 (very bad) to 5 (very good) for scoring is used in this questionnaire [33]. The evaluations performed on the dimensions of SF-36 show that this questionnaire is a reliable scale with content validity. In a study by Brazier et al., the validity of the original version of this questionnaire for all subscales was more than 0.85 and the validity of this tool was confirmed concerning the Nottingham health profile [32]. The questionnaire had good validity, reliability, and internal consistency and this has also been confirmed in the Iranian population [33]. In the present study, the reliability of this questionnaire was reported as 0.83 using the Cronbach α coefficient. Descriptive statistics, including Mean±SD were used to describe the research variables. Also, after assessing the normality of data distribution by the Shapiro-Wilk test, the analysis of covariance (ANCOVA) and Correlated t-test was conducted using the SPSS software, version 26, to evaluate research hypotheses. The significance level for all statistical tests was considered equal to 0.05. Furthermore, to evaluate the effectiveness of the Alexander technique intervention on the physical and mental dimensions of QoL, the effect size was also calculated and reported.
Results
In this section, we discuss the collected data, analyses, and results related to 24 young male participants with upper-crossed syndrome. The descriptive findings of the participants are presented in Table 1.
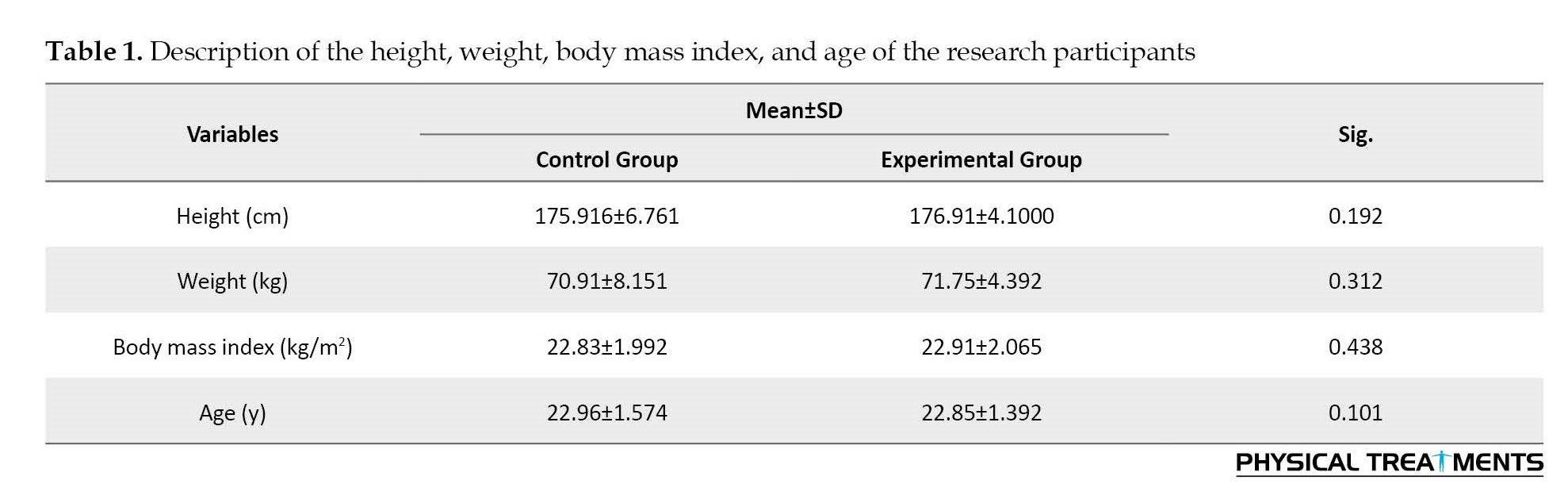
The results of the independent t-test showed no significant difference between the mean demographic variables of height, weight, body mass index, and age of the research participants in the control and experimental conditions (P>0.05).
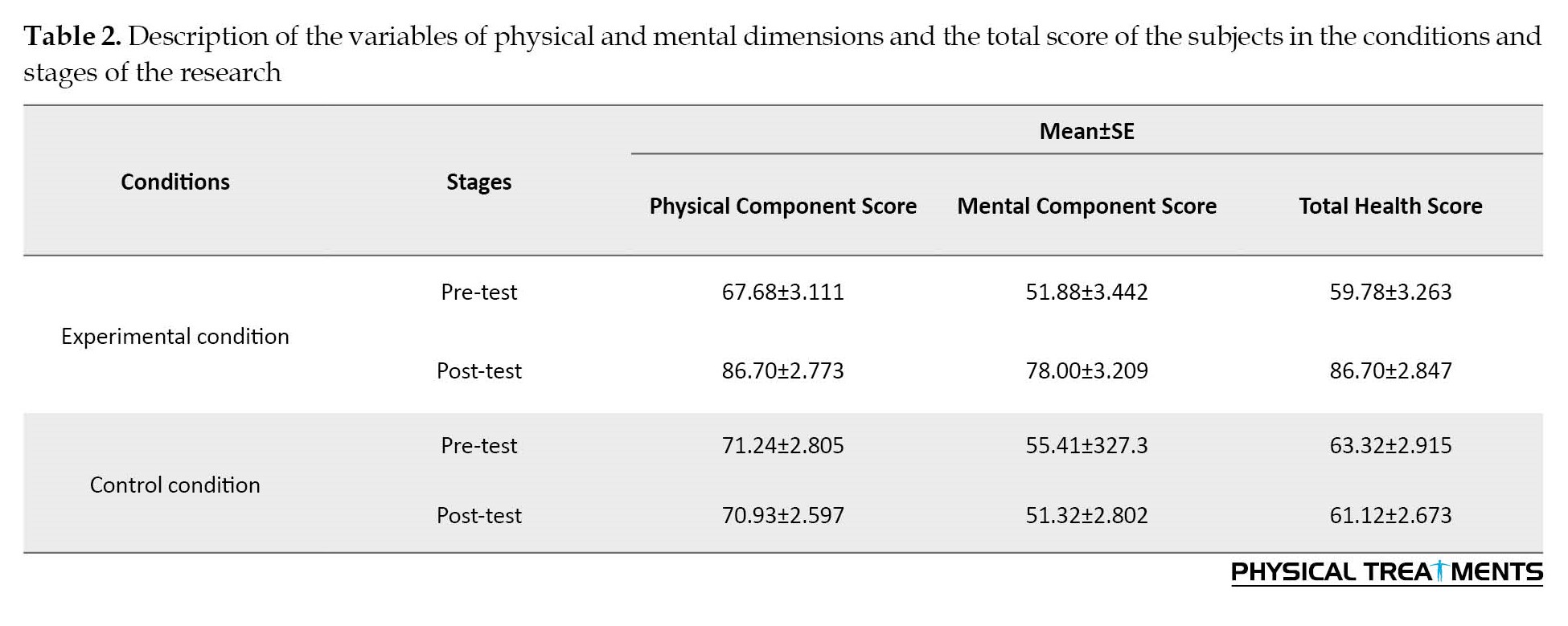
The Shapiro-Wilk test was used to check the normality of data distribution. Based on the results of the Shapiro-Wilk test, the variables had a normal distribution in the control and experimental conditions (P>0.05). The results related to the mean score of the physical and mental dimensions and the total score of the QoL in the pre-test and post-test stages of the experimental and control conditions are illustrated in Table 2.
We used the ANCOVA test to compare the effect of the Alexander technique on the physical dimension of QoL in participants with crossed syndrome between the control and experimental conditions. The results of the ANCOVA test, presented in Table 3, indicated that after controlling for the effect of the pre-test, there is a significant difference between the mean scores of the physical dimension of the QoL of the control and experimental conditions.

Therefore, the Alexander technique has significantly increased the physical dimension of the QoL in young men with upper-crossed syndrome (F(1, 21)=82.303, P<0.001, η2=0.79).
This study used the correlated t-test to compare the intra-group variable of the physical dimension of the QoL. According to the results of the correlated t-test, the mean scores of the physical dimension of the QoL in the experimental condition from the pre-test (Mean±SD 67.68±10.779) to the post-test (Mean±SD 86.70±9.606) significantly increased (T [11]=-12.151, P<0.001).
Similarly, we used the analysis of the covariance test to compare the effect of the Alexander technique on the mental dimension of the QoL in participants with upper-crossed syndrome. The results of the ANCOVA test, presented in Table 4, indicated that after controlling for the effect of the pre-test, there is a significant difference between the mean scores of the mental dimension of the QoL of the control and the experimental conditions.

Therefore, the Alexander technique has significantly increased the mental dimension of the QoL in young men with upper-crossed syndrome (F(1, 21)=109.138, P<0.001, η2=0.83).
This study also used the correlated t-test to compare the intra-group variable of the mental dimension of the QoL. Following the results of the correlated t-test, the mean scores of the mental dimension of the QoL in the experimental condition from the pre-test (Mean±SD 51.88±11.857) to the post-test (Mean±SD 78.00±11.116) significantly increased (T [11]=-11.235, P<0.001).
Discussion
This research was conducted to investigate the effectiveness of the Alexander technique on the physical and mental dimensions of the QoL in young men with upper-crossed syndrome. According to the findings of the current study, the Alexander technique significantly increased the physical aspect of the QoL in young men with upper-crossed syndrome in the experimental condition. After participating in the educational intervention of the Alexander technique, the average physical component score of the participants of the experimental condition was 86.70 which shows an average of 19.02 points increase compared to the pre-test, which is a high score in the SF-36 health survey. This is indicative of the improvement of the physical dimension of participants’ QoL at the end of intervention in the experimental condition. Considering the reported size effect (0.79), Alexander technique training has significantly improved the physical dimension of health in the experimental condition. The greatest improvement in the physical dimension of the QoL of the experimental condition was observed in the general health subscale with a 23.75 points increase compared to the pre-test. The findings of the present study were consistent with the findings of the studies by Little et al. [19] and Kim and Baek [34]; however, they were in contrast with the results of the study by Pourkamali et al. [28]. Pourkamali et al. (2016) compared the effectiveness of massage therapy, Alexander and Dosaho technique on happiness, hope, health, and QoL of elderly people with Parkinson disease. The results of their study showed that the Alexander technique had no significant effect on improving the QoL [28]. The difference between the results of the current study and the study by Pourkamali et al. [28] might be due to various factors, such as the difference in the age of the participants, condition of their participants who were suffering from Parkinson disease (which creates limitations and continuous physical and mental problems), and limited number of training sessions of the Alexander technique in their study compared to the current study. Moreover, the lack of supervision of a certified teacher of the Alexander technique in the study by Pourkamali et al. [28] can have a negative impact on the quality of training by the researchers and lead to translation inefficiency and ineffectiveness of the Alexander technique training during the intervention.
Moreover, based on the findings of the current study, the Alexander technique significantly increased the mental aspect of the QoL in young men with upper crossed syndrome in the experimental condition. After participating in the educational intervention of the Alexander technique, the average mental component score of the participants of the experimental condition was 78.00 which shows an average of 26.12 points increase compared to the pre-test, which is a high score in the SF-36 health survey. According to the reported effect size (0.83), the Alexander technique training significantly improved the mental dimension of health in the experimental condition. The greatest improvement in the mental dimension of the QoL of the experimental condition was observed in the social performance subscale with a 26.04 points increase compared to the pre-test.
A limited number of studies have investigated the effectiveness of the Alexander technique on the mental dimension of QoL. The findings of the recent study were consistent with the results of the study by Kim and Beak [34], but contrary to the results of the study by Little et al. [19]. Little et al. investigated the effectiveness of the Alexander technique, massage therapy, and exercise prescription on chronic back pain. They reported no significant difference related to the mental dimension of QoL (P=0.314) between the Alexander technique (experimental) condition and the control condition [19]. The participants of their study were suffering from chronic back pain that can negatively impact the mental state and relaxation of the patients and consequently lead to the ineffectiveness of the Alexander technique on their mental dimension. Whereas, the participants of the current study were young and healthy, and the quality of the training was improved by the supervision of an expert in the field.
In addition to the quantitative examination of the participants in connection with the effectiveness of the Alexander technique intervention on health in the current study, we qualitatively collected participants’ experiences, attitudes, and feedback regarding the Alexander technique training. This study conducted individual interviews two weeks after the implementation of the protocol. The majority of the participants indicated that they joined the study since they assumed that the Alexander technique training was beneficial. They highlighted other reasons for attending the session, such as the convenience of the training, modest effort, no difficult compared to sports exercises, reasonable cost, attainability, and feasibility (whenever/wherever). They also emphasized that the sessions and training were enjoyable and attractive, and they introduced and highly recommended the Alexander technique training to their family and friends. Furthermore, they stated that after application of the Alexander technique, they feel improvements and lightness in their body actions and freedom of movement besides feeling a sense of physical and mental relaxation. They suggested the introduction of the Alexander technique not only to a wider range of university students but also to the members of society. These findings were consistent with the results of the studies by Cohen et al. [35], Hanefeld et al. [36] and Tunnicliffe [21].
Finally, the 6-week training protocol of the Alexander technique in the present study was effective in improving the physical and mental dimensions of the participants’ QoL. The amount of change in the total score of the QoL in the experimental condition after the intervention was from 59.78 points in the pre-test to 82.35 points in the post-test, which indicated the overall improvement of health and QoL in the experimental condition. The benefits of conducting the Alexander technique intervention were improving the physical condition of the participants, enhancing their body awareness and coordination, and consequently cultivating their health and QoL. Most importantly, based on the scores, the mental dimension of QoL was developed slightly more than the physical dimension of QoL. This might be due to the mental nature of the Alexander technique and more emphasis on the use of the mind while delivering this method.
Conclusion
Based on the results of the present study, the Alexander technique training improves the physical and mental dimensions of QoL in people with upper-crossed syndrome. The Alexander technique can increase individuals’ mental and physical energy levels in their daily lives by removing inappropriate physical habits, eliminating faulty movement patterns, replacing them with correct habits, and improving posture that subsequently leads to cultivating general health. Therefore, the application of the Alexander technique as a practical and effective psychophysical re-education method independently or along with other interventions is highly recommended in the field of health and rehabilitation, to enhance the physical and mental dimensions of health and QoL in people with upper crossed syndrome. We suggest that the effectiveness of the Alexander technique on various dimensions of health and QoL in various ranges of age groups and genders who are suffering from different physical or mental issues should be investigated in future studies along with conducting follow-up sessions.
Study limitations
Considering the timeframe of conducting this study, the COVID-19 pandemic impeded the progress. In addition, there were some limitations throughout this research, including difficulties in finding volunteers to attend the experiments, obligations to reduce the sample and number of Alexander technique training sessions due to the existing risk factors, the conundrum of accessing a safe and suitable place to implement the educational intervention, and the absence of research background. We could not carry out the follow-up phase due to the COVID-19 restrictions and obstacles to re-accessing the participants.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of University of Tehran (Code: IR.UT.SPORT.REC.1400.032 in 1401).
Funding
This article is extracted from Hamid Babaei’s doctoral dissertation (ID: 139840) in the field of corrective exercises at the Department of Sports Medicine, University of Tehran.
Authors' contributions
Conceptualization and supervision: Mohammad Hosein Alizadeh and Houman Minoonezhad; Protocol designing and data collection: Hamid Babaei and Azin Movahed; Data analysis: Hamid Babaei and Houman Minoonezhad; Methodology, investigation and preparing the original draft: All authors; Review and final edition: Roy Maher.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The researchers hereby express their gratitude to the members of the Sports Medicine Department at the University of Tehran and the volunteers who participated in the current study.
References
In modern life, a vast majority of people are suffering from disorders caused by inappropriate use of muscles and improper daily postures, which consequently lead to deformities in the human body’s posture [1]. Upper-crossed syndrome is currently one of the physical abnormalities that has a high prevalence [2]. The prevalence of upper-crossed syndrome has been reported in 32.4% of employees, 24.3% of drivers, and 27% of housewives [3]. In this deformity, thoracic kyphosis increases because of the decrease in the endurance and strength of the spinal extensor muscles [4]. Moreover, it may generate undesirable consequences in the body, such as reduced physical performance [5], pulmonary dysfunction [6], balance disorder [7], difficulty in doing daily life activities [8], and decrease in health and quality of life (QoL) [9, 10]. The upper crossed syndrome due to poor posture and inappropriate appearance (from an aesthetic point of view) accompanied by the presence of physical complications may lead to anxiety and reduced self-esteem [11]. A combination of these issues negatively affects patients’ physical and mental health and eventually decreases their QoL [10]. Given the high prevalence and various physiological and psychological complications of upper-crossed syndrome, the importance of correcting this deformity is crucial.
A variety of corrective methods have been used for people with upper-crossed syndrome, including manual therapy, exercise, the use of tapes, assistive devices, and posture re-education [12]. In recent years, the attention of health professionals has been focused on posture training as a method to prevent and correct musculoskeletal system disorders, especially head, neck, and trunk abnormalities. One of the relatively common methods of body posture re-education is the Alexander technique [13]. Although the Alexander technique was initially utilized by artists, researchers in the field of health and rehabilitation have recently become interested in the application of this technique in various health-related cases [14]. Despite the current application of the Alexander technique by researchers, it is still under investigation compared to the other methods and interventions.
The purpose of the Alexander technique is to help a person increase body awareness and use this information to achieve a more efficient performance. Alexander technique training sessions include posture exercises from lying down and sitting to more dynamic positions, such as standing up and walking, and special activities like working at a desk, studying, and playing the guitar [15]. This technique uses the teacher-student paradigm instead of the therapist-patient paradigm and its main focus is on education and not treatment [16]. Alexander technique enables people to become aware of their posture in a sensorimotor way and to change their faulty habitual movement patterns [13]. In this method, the person learns to identify the sources causing the tension response in the body, to prevent faulty habitual movement patterns, and to replace it with an efficient movement pattern according to the timing, direction, and stress reduction with an emphasis on the head, neck, and trunk [15]. Frederick Mathias Alexander, the inventor of this method, believed that movement is created not only by the body but also by the mind, and he called the division of the human organism into mental and physical parts a mistake [17]. The Alexander technique has a low degree of commonality with other corrective methods using stretching or muscle-strengthening exercises. In this method, the conscious use of the individual as an active method of psychophysical re-education is desired [18]. The effectiveness of the Alexander technique on various cases, such as back pain [19], neck pain [20], problems of the elderly [21], and Parkinson disease [22] has been investigated so far. Despite the reported findings related to the benefits of the Alexander technique, there is still insufficient scientific evidence to confirm the effectiveness of this technique in most health-related fields and a demand for more comprehensive and controlled studies is evident [14].
Nowadays, QoL is considered a basic index for evaluating various dimensions of people’s health in human societies, and its investigation is of special importance. QoL refers to the concept of how well people consider their daily life in different physical, psychological, and social dimensions to be good and desirable and follow social and universal standards [23]. One of the fields in which the most research on QoL has been conducted is healthcare [24]. The musculoskeletal condition of the spine is one of the main causes of pain that ultimately reduces one’s QoL [25]. The findings of existing research show the relationship between postural defects and QoL and state that correct body posture is one of the most effective indicators of health and QoL [26]; therefore, interventions and methods that help to improve posture will probably enhance the QoL. Furthermore, the Alexander technique can boost the functional quality of movement and amplify the QoL by increasing body awareness [14]. In a study that investigated the effectiveness of the Alexander technique, massage therapy, and exercise therapy on chronic back pain, the researchers concluded that Alexander technique training by trained instructors has created long-term benefits in patients with chronic back pain and improved their QoL significantly [19]. Also, in a review study titled “Alexander technique for chronic asthma,” the authors stated conclusively that clinical studies consisting of controlled and strong methodologies are needed to delve into the effect of the Alexander technique on various aspects of human health and the QoL among those who are exposed to different disorders [27].
A limited number of studies have been conducted on the Alexander technique in the country [22, 28]. We found that the existing studies used the Alexander technique as an exercise or a treatment (this technique is only training). Most importantly, lacking supervision by an Alexander technique expert in the design and implementation of the protocol in these studies attenuated the quality of their research. Therefore, it is necessary to conduct research containing a more efficient methodology by applying the correct training protocol under the supervision of a certified Alexander technique specialist. The majority of the studies in connection with the effect of the Alexander technique consist of diseases, such as back pain [19] and Parkinson [22, 28]. Considering the high prevalence of upper crossed syndrome [2, 3] and the negative effects of this abnormality on various aspects of one’s life, their QoL in particular [9, 10], the necessity of conducting research comprising the Alexander technique, QoL, and upper crossed syndrome was evident; therefore, this study investigated the effect of the Alexander technique on the physical and mental dimensions of QoL in young men with upper crossed syndrome.
Materials and Methods
Study participants
Using the convenience sampling method, we selected 24 male university students aged 19-25 years for the current study and randomly divided them into an experimental (n=12) and a control group (n=12). We distributed the invitations to absorb volunteer male students at the University of Tehran to participate in the first phase of the study. After an initial screening by posture grid, the students with upper crossed syndrome were diagnosed and selected as samples. The criteria for sample size (n=24) were based on the variable of QoL and using the G*Power software [29] with the assumptions of the confidence coefficient of 95% (α=0.05), statistical power 80% (β=0.2), and the effect size (d=0.6) (Appendix 1).
Study design
The current research design was semi-experimental containing two conditions: a) An experimental condition, and b) A control condition. A total of 12 participants were allocated in each condition. A pre-test and post-test was conducted before and after interventions. The study was conducted blindly and the information that could cause the deviation of the study results was not presented to the participants till the completion of the study.
Before starting the study, we debriefed the participants about the intervention, the confidentiality of the results, and the right to withdraw at any stage of the research. Subsequently, written consent was obtained from them to participate in the study and participants’ information was collected using demographic questionnaires, a digital scale, and a digital meter (to accurately measure their height and weight and calculate their body mass index). To evaluate the posture of the subjects, the forward head and forward shoulder angles were measured by photogrammetric method and the kyphosis angle was accurately measured using a flexible ruler. The measurements were carried out by the main researcher at the health center of University of Tehran. During the intervention, the participants of the experimental condition received the educational intervention of the Alexander technique according to the predetermined protocol for six weeks. Alexander technique training sessions were held in a classroom with adequate space, ventilation, and light. The control condition was not subjected to any special education and training and the participants of the control condition were only evaluated in the pre-test and post-test.
The goal of the Alexander technique training protocol was to increase body awareness, correct inappropriate movement habits, and help participants function correctly in daily activities. During the experimental condition, the participants were taught the Alexander technique using manual guidance, and verbal, visual, and proprioception feedback. In the first two sessions, we concentrated on the participants’ familiarity with the Alexander technique, explaining goals, and identifying their weak physical habits and inefficient movement patterns. In the following sessions, we instructed the participants about the following items: a) The correct way to hold the head, neck, and spine while sitting, standing, and walking; b) The correct way to sit and stand up; c) The correct way to sit and lift objects; d) The correct way to work in a bent position; e) The correct way to carry bags and equipment; f) The correct posture when writing and reading; g) The correct expressions of the face and eyes; and h) The correct way of breathing [28]. During these sessions, the participants tried to familiarize themselves with the basic concepts of Alexander’s technique, including inhibition, primary control, and direction, in addition to correcting wrong body habits and improving movement patterns. They were also asked to apply the acquired knowledge in their daily activities.
To obtain sufficient expertise for instructing the Alexander technique to the participants, the first author completed the necessary training (24 training sessions within 3 months) under the supervision of an Alexander technique expert and familiarized himself with the core principles of the technique. The training protocol for the current study was then designed by seeking advice from the certified expert. The Alexander technique protocol was applied by the participants under the direct supervision of the first author throughout the study (Figure 1).
The emphasis of the Alexander technique training sessions was on the benefits of increasing self-awareness during the activity. The participants were encouraged to self-evaluate while performing their usual daily activities, such as standing, sitting, working with the computer, personal tasks, and housework, and most importantly, to apply the learned principles of the Alexander technique to improve physical and movement habits. We used tactile feedback to teach the subjects how to maintain a coherent connection of different parts of the body during the activities. We also asked them to communicate any problems in understanding and implementing the movements so that the training could be completed correctly and accurately.
The short form (SF-36) health survey was used to assess the participants’ QoL. This self-report questionnaire is a 36-item scale which is designed by Ware and Sherburne [31]. The SF-36 questionnaire evaluates two general dimensions of QoL, which include the physical health dimension (physical function, physical role limitations, bodily pain, and general health perception) and the mental health dimension (energy/vitality, social functioning, emotional role limitations, and mental health). The outcome is evaluated through the score of the physical dimension and the score of the mental dimension, respectively [32]. A Likert scale from 1 (very bad) to 5 (very good) for scoring is used in this questionnaire [33]. The evaluations performed on the dimensions of SF-36 show that this questionnaire is a reliable scale with content validity. In a study by Brazier et al., the validity of the original version of this questionnaire for all subscales was more than 0.85 and the validity of this tool was confirmed concerning the Nottingham health profile [32]. The questionnaire had good validity, reliability, and internal consistency and this has also been confirmed in the Iranian population [33]. In the present study, the reliability of this questionnaire was reported as 0.83 using the Cronbach α coefficient. Descriptive statistics, including Mean±SD were used to describe the research variables. Also, after assessing the normality of data distribution by the Shapiro-Wilk test, the analysis of covariance (ANCOVA) and Correlated t-test was conducted using the SPSS software, version 26, to evaluate research hypotheses. The significance level for all statistical tests was considered equal to 0.05. Furthermore, to evaluate the effectiveness of the Alexander technique intervention on the physical and mental dimensions of QoL, the effect size was also calculated and reported.
Results
In this section, we discuss the collected data, analyses, and results related to 24 young male participants with upper-crossed syndrome. The descriptive findings of the participants are presented in Table 1.
The results of the independent t-test showed no significant difference between the mean demographic variables of height, weight, body mass index, and age of the research participants in the control and experimental conditions (P>0.05).
The Shapiro-Wilk test was used to check the normality of data distribution. Based on the results of the Shapiro-Wilk test, the variables had a normal distribution in the control and experimental conditions (P>0.05). The results related to the mean score of the physical and mental dimensions and the total score of the QoL in the pre-test and post-test stages of the experimental and control conditions are illustrated in Table 2.
We used the ANCOVA test to compare the effect of the Alexander technique on the physical dimension of QoL in participants with crossed syndrome between the control and experimental conditions. The results of the ANCOVA test, presented in Table 3, indicated that after controlling for the effect of the pre-test, there is a significant difference between the mean scores of the physical dimension of the QoL of the control and experimental conditions.
Therefore, the Alexander technique has significantly increased the physical dimension of the QoL in young men with upper-crossed syndrome (F(1, 21)=82.303, P<0.001, η2=0.79).
This study used the correlated t-test to compare the intra-group variable of the physical dimension of the QoL. According to the results of the correlated t-test, the mean scores of the physical dimension of the QoL in the experimental condition from the pre-test (Mean±SD 67.68±10.779) to the post-test (Mean±SD 86.70±9.606) significantly increased (T [11]=-12.151, P<0.001).
Similarly, we used the analysis of the covariance test to compare the effect of the Alexander technique on the mental dimension of the QoL in participants with upper-crossed syndrome. The results of the ANCOVA test, presented in Table 4, indicated that after controlling for the effect of the pre-test, there is a significant difference between the mean scores of the mental dimension of the QoL of the control and the experimental conditions.
Therefore, the Alexander technique has significantly increased the mental dimension of the QoL in young men with upper-crossed syndrome (F(1, 21)=109.138, P<0.001, η2=0.83).
This study also used the correlated t-test to compare the intra-group variable of the mental dimension of the QoL. Following the results of the correlated t-test, the mean scores of the mental dimension of the QoL in the experimental condition from the pre-test (Mean±SD 51.88±11.857) to the post-test (Mean±SD 78.00±11.116) significantly increased (T [11]=-11.235, P<0.001).
Discussion
This research was conducted to investigate the effectiveness of the Alexander technique on the physical and mental dimensions of the QoL in young men with upper-crossed syndrome. According to the findings of the current study, the Alexander technique significantly increased the physical aspect of the QoL in young men with upper-crossed syndrome in the experimental condition. After participating in the educational intervention of the Alexander technique, the average physical component score of the participants of the experimental condition was 86.70 which shows an average of 19.02 points increase compared to the pre-test, which is a high score in the SF-36 health survey. This is indicative of the improvement of the physical dimension of participants’ QoL at the end of intervention in the experimental condition. Considering the reported size effect (0.79), Alexander technique training has significantly improved the physical dimension of health in the experimental condition. The greatest improvement in the physical dimension of the QoL of the experimental condition was observed in the general health subscale with a 23.75 points increase compared to the pre-test. The findings of the present study were consistent with the findings of the studies by Little et al. [19] and Kim and Baek [34]; however, they were in contrast with the results of the study by Pourkamali et al. [28]. Pourkamali et al. (2016) compared the effectiveness of massage therapy, Alexander and Dosaho technique on happiness, hope, health, and QoL of elderly people with Parkinson disease. The results of their study showed that the Alexander technique had no significant effect on improving the QoL [28]. The difference between the results of the current study and the study by Pourkamali et al. [28] might be due to various factors, such as the difference in the age of the participants, condition of their participants who were suffering from Parkinson disease (which creates limitations and continuous physical and mental problems), and limited number of training sessions of the Alexander technique in their study compared to the current study. Moreover, the lack of supervision of a certified teacher of the Alexander technique in the study by Pourkamali et al. [28] can have a negative impact on the quality of training by the researchers and lead to translation inefficiency and ineffectiveness of the Alexander technique training during the intervention.
Moreover, based on the findings of the current study, the Alexander technique significantly increased the mental aspect of the QoL in young men with upper crossed syndrome in the experimental condition. After participating in the educational intervention of the Alexander technique, the average mental component score of the participants of the experimental condition was 78.00 which shows an average of 26.12 points increase compared to the pre-test, which is a high score in the SF-36 health survey. According to the reported effect size (0.83), the Alexander technique training significantly improved the mental dimension of health in the experimental condition. The greatest improvement in the mental dimension of the QoL of the experimental condition was observed in the social performance subscale with a 26.04 points increase compared to the pre-test.
A limited number of studies have investigated the effectiveness of the Alexander technique on the mental dimension of QoL. The findings of the recent study were consistent with the results of the study by Kim and Beak [34], but contrary to the results of the study by Little et al. [19]. Little et al. investigated the effectiveness of the Alexander technique, massage therapy, and exercise prescription on chronic back pain. They reported no significant difference related to the mental dimension of QoL (P=0.314) between the Alexander technique (experimental) condition and the control condition [19]. The participants of their study were suffering from chronic back pain that can negatively impact the mental state and relaxation of the patients and consequently lead to the ineffectiveness of the Alexander technique on their mental dimension. Whereas, the participants of the current study were young and healthy, and the quality of the training was improved by the supervision of an expert in the field.
In addition to the quantitative examination of the participants in connection with the effectiveness of the Alexander technique intervention on health in the current study, we qualitatively collected participants’ experiences, attitudes, and feedback regarding the Alexander technique training. This study conducted individual interviews two weeks after the implementation of the protocol. The majority of the participants indicated that they joined the study since they assumed that the Alexander technique training was beneficial. They highlighted other reasons for attending the session, such as the convenience of the training, modest effort, no difficult compared to sports exercises, reasonable cost, attainability, and feasibility (whenever/wherever). They also emphasized that the sessions and training were enjoyable and attractive, and they introduced and highly recommended the Alexander technique training to their family and friends. Furthermore, they stated that after application of the Alexander technique, they feel improvements and lightness in their body actions and freedom of movement besides feeling a sense of physical and mental relaxation. They suggested the introduction of the Alexander technique not only to a wider range of university students but also to the members of society. These findings were consistent with the results of the studies by Cohen et al. [35], Hanefeld et al. [36] and Tunnicliffe [21].
Finally, the 6-week training protocol of the Alexander technique in the present study was effective in improving the physical and mental dimensions of the participants’ QoL. The amount of change in the total score of the QoL in the experimental condition after the intervention was from 59.78 points in the pre-test to 82.35 points in the post-test, which indicated the overall improvement of health and QoL in the experimental condition. The benefits of conducting the Alexander technique intervention were improving the physical condition of the participants, enhancing their body awareness and coordination, and consequently cultivating their health and QoL. Most importantly, based on the scores, the mental dimension of QoL was developed slightly more than the physical dimension of QoL. This might be due to the mental nature of the Alexander technique and more emphasis on the use of the mind while delivering this method.
Conclusion
Based on the results of the present study, the Alexander technique training improves the physical and mental dimensions of QoL in people with upper-crossed syndrome. The Alexander technique can increase individuals’ mental and physical energy levels in their daily lives by removing inappropriate physical habits, eliminating faulty movement patterns, replacing them with correct habits, and improving posture that subsequently leads to cultivating general health. Therefore, the application of the Alexander technique as a practical and effective psychophysical re-education method independently or along with other interventions is highly recommended in the field of health and rehabilitation, to enhance the physical and mental dimensions of health and QoL in people with upper crossed syndrome. We suggest that the effectiveness of the Alexander technique on various dimensions of health and QoL in various ranges of age groups and genders who are suffering from different physical or mental issues should be investigated in future studies along with conducting follow-up sessions.
Study limitations
Considering the timeframe of conducting this study, the COVID-19 pandemic impeded the progress. In addition, there were some limitations throughout this research, including difficulties in finding volunteers to attend the experiments, obligations to reduce the sample and number of Alexander technique training sessions due to the existing risk factors, the conundrum of accessing a safe and suitable place to implement the educational intervention, and the absence of research background. We could not carry out the follow-up phase due to the COVID-19 restrictions and obstacles to re-accessing the participants.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of University of Tehran (Code: IR.UT.SPORT.REC.1400.032 in 1401).
Funding
This article is extracted from Hamid Babaei’s doctoral dissertation (ID: 139840) in the field of corrective exercises at the Department of Sports Medicine, University of Tehran.
Authors' contributions
Conceptualization and supervision: Mohammad Hosein Alizadeh and Houman Minoonezhad; Protocol designing and data collection: Hamid Babaei and Azin Movahed; Data analysis: Hamid Babaei and Houman Minoonezhad; Methodology, investigation and preparing the original draft: All authors; Review and final edition: Roy Maher.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The researchers hereby express their gratitude to the members of the Sports Medicine Department at the University of Tehran and the volunteers who participated in the current study.
References
- Kendall FP, McCreary EK, Provance PG, Rodgers MM, Romani WA. Muscles: Testing and function with posture and pain. Philadelphia: Lippincott Williams & Wilkins Baltimore; 2005. [Link]
- Rajalaxmi V, Paul J, Nithya M, Lekha SC, Likitha B. Effectiveness of three dimensional approach of schroth method and yoga on pulmonary function test and posture in upper crossed syndrome with neck Pain-A double blinded study. Research Journal of Pharmacy and Technology. 2018; 11(5):1835-9. [DOI:10.5958/0974-360X.2018.00341.4]
- Naseer R, Tauqeer S. Prevalence of Upper Cross Syndrome in Different Occupations. Pakistan Journal of Physical Therapy (PJPT). 2021; 4(2):03-07. [Link]
- Eum R, Leveille SG, Kiely DK, Kiel DP, Samelson EJ, Bean JF. Is kyphosis related to mobility, balance and disability? American Journal of Physical Medicine & Rehabilitation/Association of Academic Physiatrists. 2013; 92(11):980 -9. [DOI:10.1097/PHM.0b013e31829233ee] [PMID]
- Katzman WB, Huang MH, Lane NE, Ensrud KE, Kado DM. Kyphosis and decline in physical function over 15 years in older community-dwelling women: The Study of Osteoporotic Fractures. Journals of Gerontology Series A: Biomedical Sciences and Medical Sciences. 2013; 68(8):976-83.[DOI:10.1093/gerona/glt009] [PMID]
- Lorbergs AL, O'Connor GT, Zhou Y, Travison TG, Kiel DP, Cupples LA, et al. Severity of kyphosis and decline in lung function: the Framingham study. The Journals of Gerontology: Series A. 2017; 72(5):689-94. [PMID]
- Sinaki M, Brey RH, Hughes CA, Larson DR, Kaufman KR. Balance disorder and increased risk of falls in osteoporosis and kyphosis: Significance of kyphotic posture and muscle strength. Osteoporosis International. 2005; 16(8):1004-10. [DOI:10.1007/s00198-004-1791-2] [PMID]
- Ryan SD, Fried LP. The impact of kyphosis on daily functioning. Journal of the American Geriatrics Society. 1997; 45(12):1479-86. [DOI:10.1111/j.1532-5415.1997.tb03199.x] [PMID]
- Katzman WB, Wanek L, Shepherd JA, Sellmeyer DE. Age-related hyperkyphosis: Its causes, consequences, and management. Journal of Orthopaedic & Sports Physical Therapy. 2010; 40(6):352-60. [DOI:10.2519/jospt.2010.3099] [PMID]
- Soliman HAG. Health-related quality of life of adolescents with severe untreated congenital kyphosis and kyphoscoliosis in a developing country. Spine. 2018; 43(16):E942-8.[DOI:10.1097/BRS.0000000000002598] [PMID]
- Korooshfard N, Ramezanzade H, Arabnarmi B. Relationship of self esteem with forward head posture and round shoulder. Procedia-Social and Behavioral Sciences. 2011; 15:3698-702. [DOI:10.1016/j.sbspro.2011.04.358]
- Kendall FP, McCreary EK, Provance PG, Rodgers MM, Romani WA. Muscles: Testing and function with posture and pain. Philadelphia: Lippincott, Williams, & Wilkins; 2005. [Link]
- Jain S, Janssen K, DeCelle S. Alexander technique and Feldenkrais method: A critical overview. Physical Medicine and Rehabilitation Clinics. 2004; 15(4):811-25. [DOI:10.1016/j.pmr.2004.04.005] [PMID]
- Zuck D. The Alexander technique. In: Davis CM, editor. Complementary therapies in rehabilitation: Holistic approaches for prevention and wellness. Thorofare : Slack Inc. 2009. [Link]
- Kutschke IP. The effects of the Alexander Technique training on neck and shoulder biomechanics and posture in healthy people. Open Archives Initiative; 2010. [Link]
- Dennis RJ. Functional reach improvement in normal older women after Alexander Technique instruction. Journals of Gerontology Series A: Biomedical Sciences and Medical Sciences. 1999; 54(1):M8-11. [DOI:10.1093/gerona/54.1.M8] [PMID]
- Brown R, Alexander FA. Authorised summaries of F.M. Alexander's four books: 'Man's supreme inheritance', 'constructive conscious control of the individual', 'the use of the self' & 'the universal constant in living. Cape Town: STAT Books; 1992. [Link]
- Alexander F. The use of the self. London: Gollancz; 1985. [Link]
- Little P, Lewith G, Webley F, Evans M, Beattie A, Middleton K, et al. Randomised controlled trial of Alexander technique lessons, exercise, and massage (ATEAM) for chronic and recurrent back pain. BMJ. 2008; 337:a884. [DOI:10.1136/bmj.a884] [PMID]
- Becker JJ, McIsaac TL, Copeland SL, Cohen RG. Alexander Technique vs. targeted exercise for neck pain-A Preliminary comparison. Applied Sciences. 2021; 11(10):4640 [DOI:10.3390/app11104640]
- Tunnicliffe E. [Alexander technique: An exploration of overcoming fear of falling in people aged 60 and over [PhD dissertation]. Newcastle: Keele University; 2021. [Link]
- Sedaghati P, Goudarzian M, Daneshmandi H, Ardjmand A. Effects of Alexander-based corrective techniques on forward flexed posture, risk of fall, and fear of falling in idiopathic Parkinson’s disease. Archives of Neuroscience. 2018; 5(2):e61274. [DOI:10.5812/archneurosci.61274]
- Frisch MB. Quality of life therapy: Applying a life satisfaction approach to positive psychology and cognitive therapy. New Jersey: John Wiley & Sons; 2005. [Link]
- Gil I. A new educational program to improve posture and quality of life among students by means of the feldenkrais method and a new program: MAP-Motion and posture. Journal of Education and Training Studies. 2018; 6(11):1-11.[DOI:10.11114/jets.v6i11.3582]
- Hootman JM, Helmick CG, Brady TJ. A public health approach to addressing arthritis in older adults: The most common cause of disability. American Journal of Public Health. 2012; 102(3):426-33. [DOI:10.2105/AJPH.2011.300423] [PMID]
- Chaikin-Bentor N. Correct movement, optimal posture and walking. Israel: Narkisim; 2016.
- Dennis JA, Cates CJ. Alexander technique for chronic asthma. Cochrane Database of Systematic Reviews. 2012; 2012(9):CD000995. [DOI:10.1002/14651858.CD000995.pub2] [PMID]
- Pourkamali T, Yazdkhasti F, Oreizi H, Chitsaz A. [The comparison of the effectiveness of massage therapy, alexander technique, and dohsa-hou treatment on happiness, social adjustment, hope, mental health and quality of life in elderly with Parkinson (Persian)]. Aging Psychology. 2016; 2(1):23-35. [Link]
- Hafezi M, Izadi-Avanji FS, Mirbagher-Ajorpaz N. [The effect of Alexander technique on quality of life in patients with chronic low back pain (Persian)]. Feyz Medical Sciences Journal. 2022; 26(3):282-91. [Link]
- Thigpen CA, Padua DA, Michener LA, Guskiewicz K, Giuliani C, Keener JD, et al. Head and shoulder posture affect scapular mechanics and muscle activity in overhead tasks. Journal of Electromyography and Kinesiology. 2010; 20(4):701-9. [DOI:10.1016/j.jelekin.2009.12.003] [PMID]
- Ware JE. SF-36 health survey. Manual and interpretation guide. Boston: Health Institute, New England Medical Center: 1993. [Link]
- Brazier JE, Harper R, Jones NM, O'Cathain A, Thomas KJ, Usherwood T, et al. Validating the SF-36 Health Survey Questionnaire: New outcome measure for primary care. British Medical Journal. 1992; 305(6846):160-4. [DOI:10.1136/bmj.305.6846.160] [PMID]
- Asghari Moghaddam M, Faghehi S. [Validity of the sf-36 Health Survey Questionnaire in two Iranian samples (Persian)]. Clinical Psychology and Personality. 2003; 1(1):1-10.[Link]
- Kim SY, Baek SG. The effect of Alexander technique training program: A qualitative study of ordinary behavior application. Journal of Exercise Rehabilitation. 2014; 10(6):357 -61. [DOI:10.12965/jer.140177] [PMID]
- Cohen R, Ravichandra R, Trusty W, Moote T, Gross M. Alexander Technique classes are a feasible, cost-effective, and promising intervention for balance in older women. Archives of Physical Medicine and Rehabilitation. 2018; 99(10):e58-9. [DOI:10.1016/j.apmr.2018.07.203]
- Hanefeld N, Glover L, Jomeen J, Wadephul F. Women's experiences of using the Alexander Technique in the postpartum: '…in a way, it's just as beneficial as sleep'. Midwifery. 2021; 103:103155. [DOI:10.1016/j.midw.2021.103155] [PMID]
Type of Study: Research |
Subject:
General
Received: 2023/05/22 | Accepted: 2024/03/9 | Published: 2024/04/1
Received: 2023/05/22 | Accepted: 2024/03/9 | Published: 2024/04/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Attribution-NonCommercial 4.0 International License.
Contact Information
Journal Office Tel: +9821 71732837, 71732220
Publisher Tel: +9821 4535 5555, 4535 5000 (EXT: 108)
Email: physicaltreatments@gmail.com
