Mon, Feb 16, 2026
Volume 14, Issue 1 (Winter 2024)
PTJ 2024, 14(1): 53-64 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Seyedi M, Shahabi M, Elahi A. Musculoskeletal Injuries in Police Enforcement Trainees in the Pre-service Training Course of Iran. PTJ 2024; 14 (1) :53-64
URL: http://ptj.uswr.ac.ir/article-1-616-en.html
URL: http://ptj.uswr.ac.ir/article-1-616-en.html



1- Department of Sport Medicine, Sport Sciences Research Institute, Tehran, Iran.
2- Department of Sport Pathology and Corrective Exercises, Faculty of Physical Education and Sport Sciences, Tehran University, Tehran, Iran.
3- Department of Human Technology in Sport and Medicine, Institute of Biomechanics and Orthopaedics, German Sport University Cologne, Cologne, Germany.
2- Department of Sport Pathology and Corrective Exercises, Faculty of Physical Education and Sport Sciences, Tehran University, Tehran, Iran.
3- Department of Human Technology in Sport and Medicine, Institute of Biomechanics and Orthopaedics, German Sport University Cologne, Cologne, Germany.
Keywords: Injury prevalence, Military, Musculoskeletal disorder, Soldiers, Surveys and questionnaires
Full-Text [PDF 691 kb]
(972 Downloads)
| Abstract (HTML) (2728 Views)
Full-Text: (1443 Views)
Introduction
The military system is a complex system with wide and scattered locations that differ in terms of size, human resources and facilities, tasks, and composition [1]. Human power is considered as the main pillar of this system and their health is directly related to improving the quality of services and is of particular importance. Intensive military training courses are among the programs and special tasks related to the military forces, whose purpose is to improve the specific skills of soldiers at the beginning of their time in these organizations.
Recruits are prone to training-related injuries because they encounter a new living environment with intense training. Training injuries are the main cause of disability, long-term rehabilitation, functional impairment, and early discharge from military service [2-5]. While on duty, police officers must perform various heavy movements, including movements, such as running, jumping, crawling, balancing, climbing, lifting, carrying, pushing, pulling, and fighting in unpredictable environments [6, 7]. The results of all these actions can lead to injuries in various places, such as the back, knees, and shoulders, which have been reported among the injuries known to police officers [8]. Musculoskeletal injuries are the main cause of medical discharge and medical demotion in the UK Armed Forces [9] and are the most common reason why military personnel seek medical and health care [10, 11]. At any time, it is reported that between 15% and 30% of trained military personnel are not medically prepared for deployment due to musculoskeletal injuries [12].
The prevalence rate of musculoskeletal injuries has a wide range and has been reported in different sources from 20% [13] to 48% [14] and 58% [3]. The studies conducted in Iran also confirm the relatively high rate of injuries in the military forces. Farahani et al. reported a prevalence of 27.4% and an incidence of 10.2 injuries per 100 soldiers per month in Iran’s military forces [15]. Also, in 150 men examined by Naja, the most common injured areas were the knee at 45.4%, the waist at 30.7%, and the ankle at 17% [16]. Arshi et al. in a study showed a significant difference between the injuries of the marching group before and after 5 months of the parade. The most injuries were ankle 25.9% and leg 26.9%, which accounted for the highest percentage in the first stage, and in the second stage, it changed to the knee 46.6% [17]. Looking at all the health problems related to the military, musculoskeletal disorders account for a larger share of the total injuries in the military group. These disorders are associated with reduced productivity of the injured person while attending activities as well as loss of duty days and are responsible for 42% of all medical leaves in the Canadian Armed Forces [18, 19]. Musculoskeletal injuries are a major contributor to medical care visits and costs in the US military, accounting for approximately 2.4 million medical visits and $548 million in direct patient care costs [20]. The issue of musculoskeletal injuries and disorders among military groups has been one of the main challenges and concerns of military organizations and personnel since many years ago, in such a way that these injuries cause a lot of financial, physical, and mental costs for the system. The management of this phenomenon brings many challenges for military organizations, including the use of financial resources. The financial costs related to musculoskeletal disorders in military budgets are known globally [21-23].
Materials and Methods
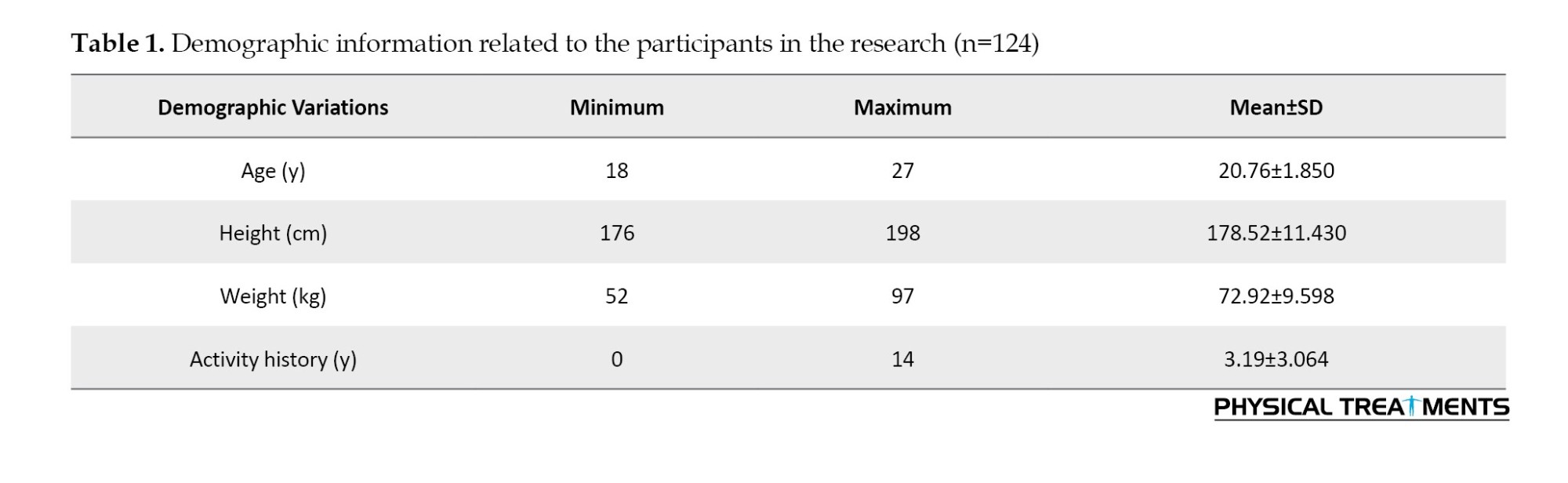
In this study, which is retrospective and descriptive epidemiology, the incidence rate, prevalence, and consequences of musculoskeletal injuries in newly enlisted soldiers who entered the pre-service training course during 6 months have been investigated. A total of 124 male soldiers with a mean age of 20.76 years, mean height of 178.52 cm, mean weight of 72.92 kg and mean activity per week for 3 hours and 19 minutes participated in this study. The participants were selected by convenience method and from one of the specialized training barracks affiliated with the Tehran police forces. All subjects were informed about the coordinates of the study and its implementation, recorded their demographic information, and read and signed the written consent form. Soldiers with severe injuries and a history of surgery in the last 6 months were prohibited from entering the plan. Also, the participants who were not eligible to participate in the project due to unwillingness to cooperate and failure to complete the questionnaire during the project were excluded. The main exercises and activities that the soldiers did in the 6-month training course included self-defense combat, arresting the accused, running and stopping consecutively, deep squats, parading, standing still without moving, and physical fitness class.
The participants completed a questionnaire related to the registration of musculoskeletal injuries, known as Oslo Sports Trauma Research Center (OSTRC), through the relevant worksheet and every month [24]. The OSTRC questionnaire, which is related to musculoskeletal injuries and diseases and can be adapted to a wide range of sports, and according to the results of the self-reporting of the participants, monitors variables, such as symptoms, severity, and impact of physical injuries [25]. This questionnaire has been approved in the groups of athletes and has been prepared from the questionnaire related to the registration of injuries caused by excessive use of OSTRC [26]. Also, Mirkarimpour et al. have investigated and presented the validity, reliability, and localization of this questionnaire [27]. In this regard, the results of the content validity index (CVI) indicated that all questions had a CVI score higher than 0.79 (on the scale of communication 0.92, clarity 0.98, simplicity 0.99, and ambiguity 0.94). It is worth mentioning that the average content validity index (scale CVI [S-CVI]/Ave) of the questionnaire was 0.95 (0.85-1). Statistical analysis showed that the internal consistency of the first 4 questions of the questionnaire has Cronbach’s α equal to 0.89. Kappa agreement coefficient (P=0.001) was also obtained from 0.71 to 0.81.
The participants completed the questionnaire monthly on Thursday afternoon of the last week of each month using a printed questionnaire with the supervision of the researcher. They were asked to report information about the injuries they had experienced in the past month and could only report a maximum of two different injuries each month. The revised local version of the OSTRC questionnaire included four key questions (Figure 1) and seven additional questions [24] and diseases were not examined in this study.
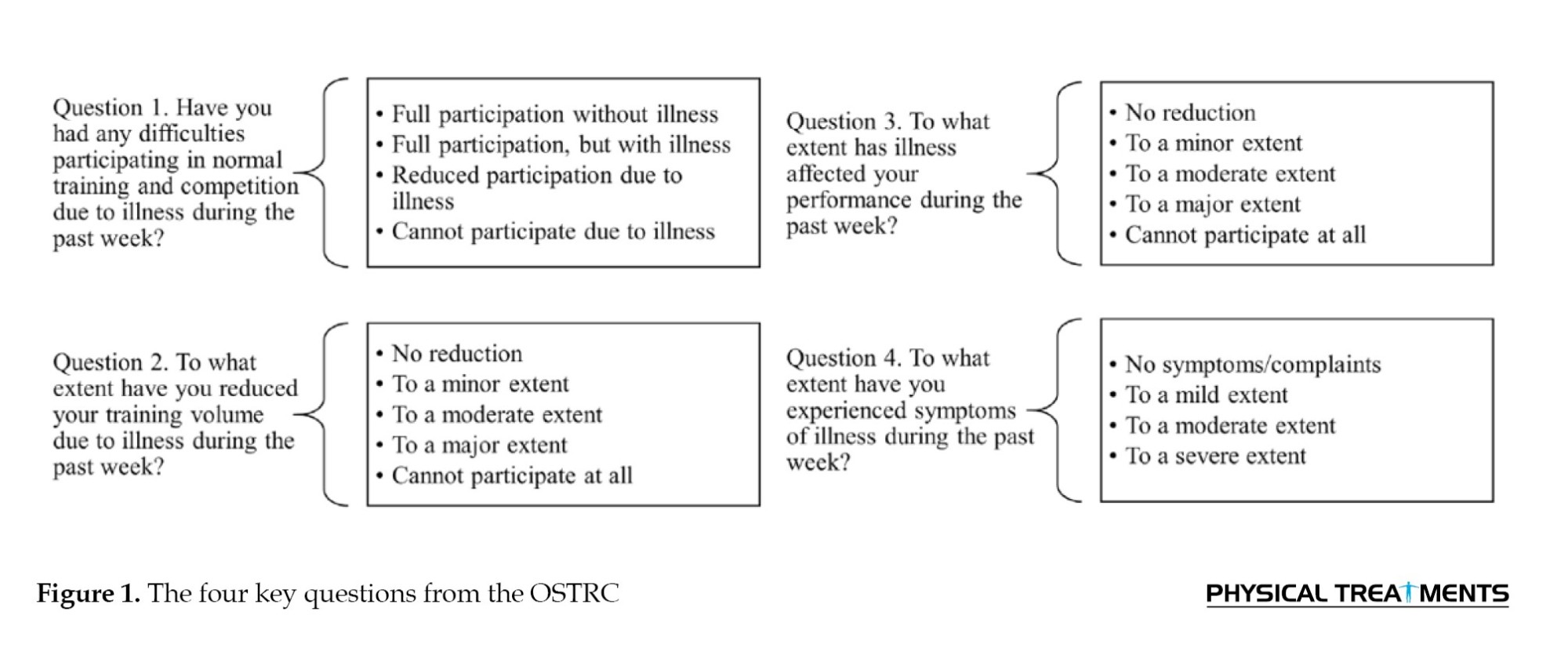
In this questionnaire, the participants were asked about the effect of physical injury on participation in sports classes, training volume, physical performance status, and severity of symptoms experienced due to injury in the past month. If the participants reported the first options in the first four key questions of the questionnaire, i.e. full participation without injury, participation without reducing the amount of training, full participation without reducing performance, and finally, full participation without symptoms, the questionnaire would be completed for the last month. If participants answered any of the four initial key questions other than the first option, they were directed to additional questions. Also, an open question was added to the mentioned questionnaire to identify any damage with its consequences that were not included in the worksheet. Participants who reported worrisome and serious injuries lasting more than 4–6 weeks were referred to a physician by the researcher. Similar injuries reported that were located in the vicinity of each other were considered as a case and analyzed [26, 28]. Before the start of the 6 months, questionnaire data was collected on a trial basis for one month to determine the possibility of false reporting and to remind the participants of the problems related to how to complete the questionnaire. The mentioned data were not used in calculations and analyses. Descriptive data were presented as Mean±SD. Prevalence was defined as the proportion of the study population that had cases of physical injury each month and was also calculated by dividing the number of participants who reported an injury by the number of questionnaire respondents in that month.
In the following, the prevalence of effective musculoskeletal injuries was calculated and defined as injuries that lead to a moderate or severe reduction in exercise volume and performance, as well as a complete inability to participate in exercise or physical activity [24]. After collecting the research information, the data related to the characteristics of the subjects, such as age, height, and weight, as well as the variables related to the prevalence of musculoskeletal injuries and other subordinate cases in the descriptive statistics section and in the Excel software with the relevant charts and also using SPSS software, version 24 was analyzed.
Results
In the descriptive results section, according to the information in the Table 1, the participants had a mean age of 20.7 years, a mean height of 178.5 cm, a mean weight of 72.9 kg, and a mean activity per week for 3 hours and 19 minutes.
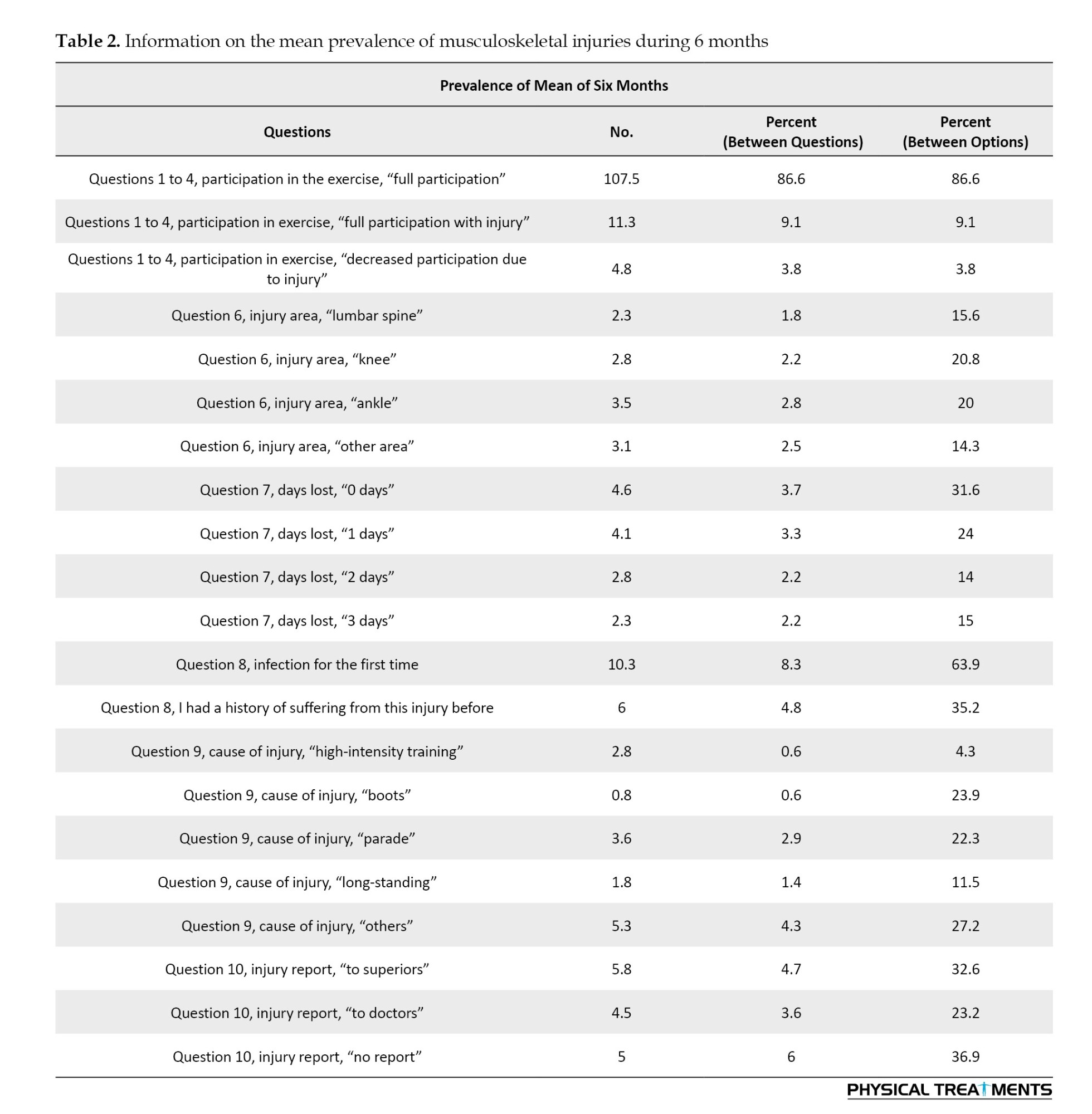
Regarding the prevalence of musculoskeletal injuries, the data was extracted and analyzed separately for each month, and below only the table related to the average of 6 months is presented. Among the critical information in Table 2, we can mention the quality of soldiers’ participation in practical classes, the crucial damaged parts of the body, the number of days affected due to the presence of injuries, and the cause of injuries from the soldiers’ point of view.
One of the variables investigated in prevalence reports is the quality and participation rate of soldiers in practical classes. According to Figure 2 on average, 86% of the soldiers managed to fully participate in practical classes without injury during the 6 months. Likewise, 9.1% of them were able to fully participate in the class even though they were injured, but they somehow carried the pain and hardship of the injury with them. Among them, only 3.8% could not attend the classes properly and completely due to injuries and had to leave the class for a while.
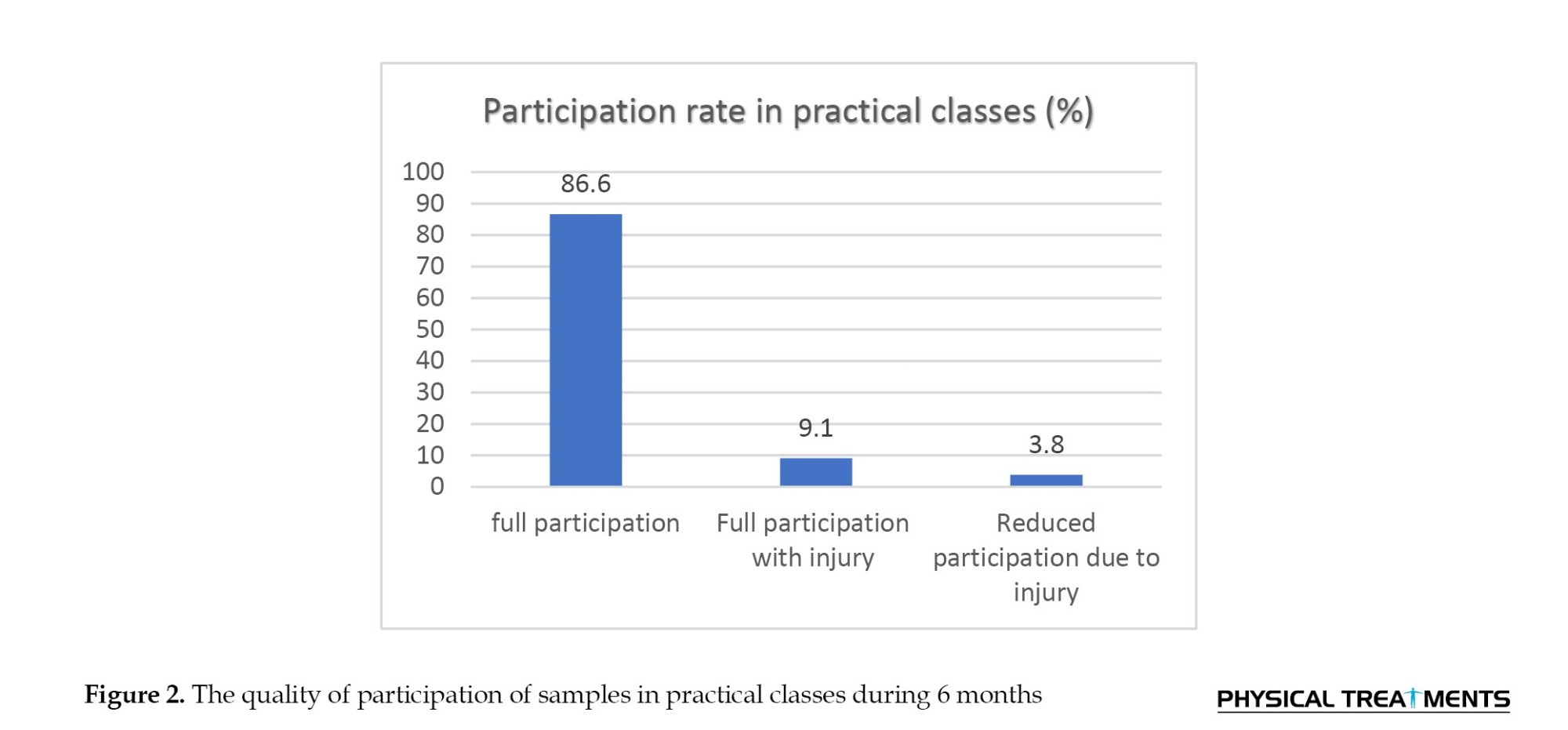
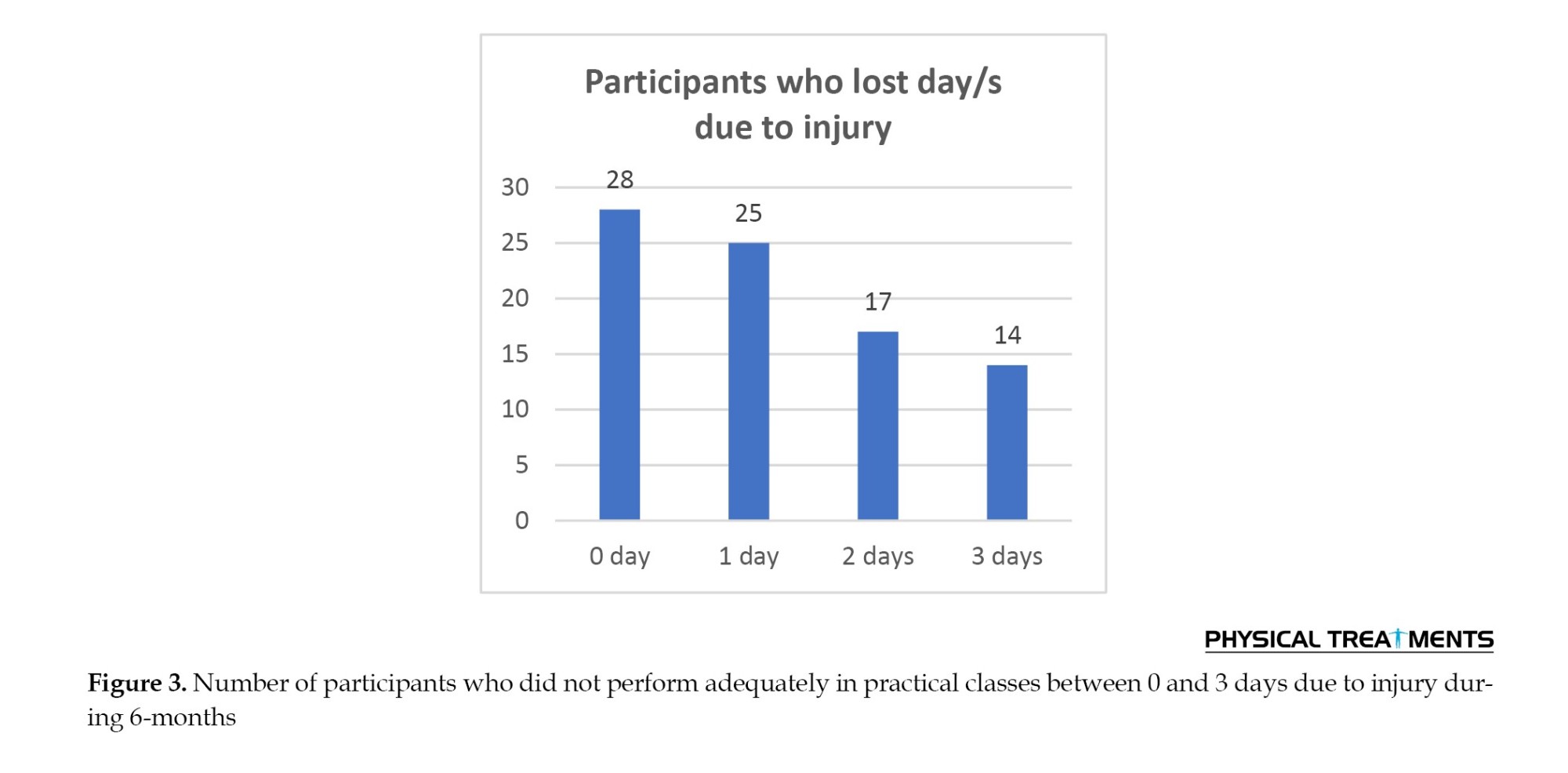
Figure 3 shows that some soldiers had at least one injury for 101 days during the 6 months, and at the same time, they attended practical classes but failed to perform properly. About a quarter of the soldiers, despite having physical injuries, could fully participate in the practical classes without any problems or missing a day.
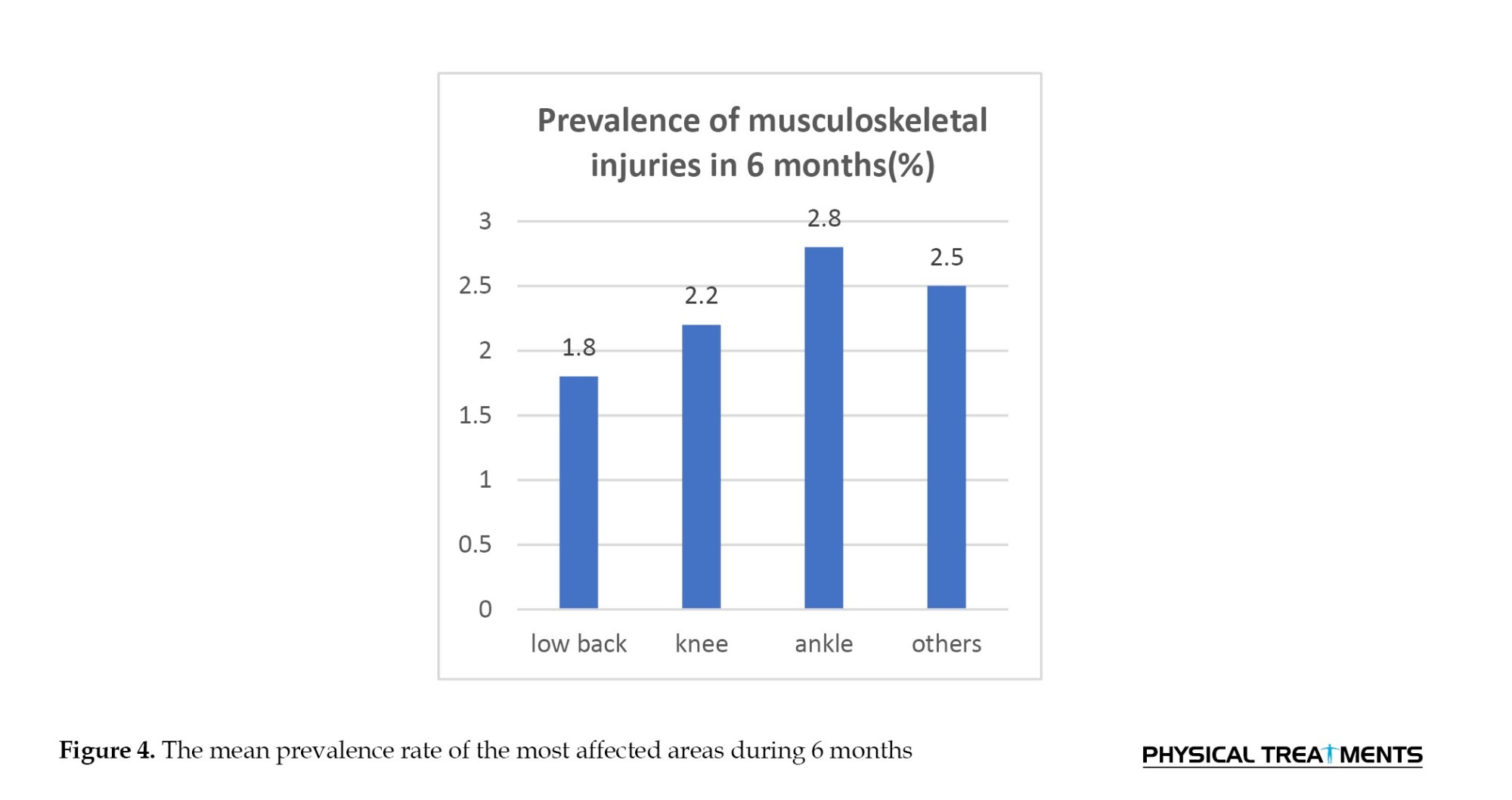
As it is clear from Figure 4 the ankle area with 2.8% damage on a monthly average took the largest share among the damaged areas. Also, the lumbar spine had the lowest share with 1.8% and, finally, the knee was the second most affected area with 2.2%. A significant number of soldiers chose the other option but did not mention the exact area they wanted.
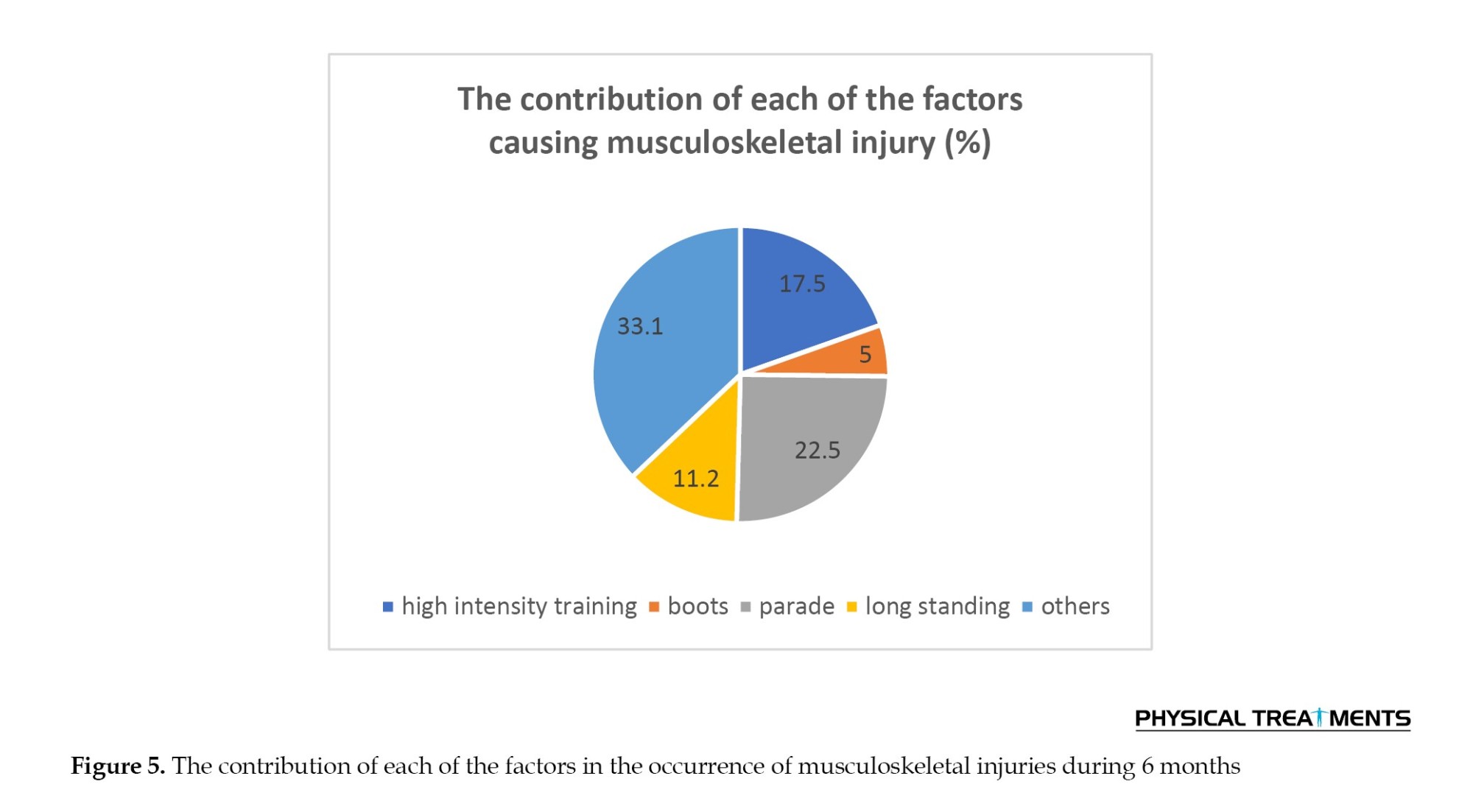
Also, looking at Figure 5, among the traumatic factors recorded by the soldiers, the parade was the vital factor with 22.5%. Also, among the mentioned cases, Putin had the lowest share among the factors with 5%. The interesting thing to note is the option of Sayer with 33.1%, which has the largest share among the factors, although, as before, the name of the desired factor was not mentioned by the soldiers. Finally, high-intensity training with 17.5%, and long-term standing with 11.2% were among other factors.
Finally, according to Figure 6 in the frequency of damaged areas by month, the sixth month had the lowest injury rate with 6 cases. In contrast, the second month with 17 cases of injury reports accounted for the highest amount among the months. On the other hand, other months did not show much difference in the number of injuries compared to each other.

Discussion
According to the obtained results, ankles with 2.8%, knees with 2.2% and lumbar spine with 1.8% had the highest prevalence rates among the participants. What is clear is that the lower limbs and the central region are the most damaged areas, and the spine of the back, head, neck, and upper limbs were not among the most damaged areas. This issue can also be seen in the results of past research, which identified the lumbar spine at 22.2% and the ankle at 15.1% as the most common injured areas [29]. Other recent research has confirmed the higher frequency of lower limb injuries, especially in the ankle area, during complex dynamic activities with military uniforms [30]. Also, Yavnai et al.’s research reported that the injured areas with pain in soldiers were the ankle area at 32.8%, knee area at 17.2%, calf area at 17.2%, and finally other lower limb areas at 32.8% [31]. In terms of the damaged points, the results obtained are consistent with the research of Nodehimoghadam et al. [16], but no alignment is observed in terms of the order of the damaged points and the prevalence rate. Of course, considering that the questionnaire was completed monthly and the prevalence rate of musculoskeletal injuries was calculated as an average of 6 months, this percentage difference related to the prevalence is justified. In other words, this difference can be caused by the difference in the type of questionnaire and the number of data collection times. In another study, Zarei et al. [32] reported the incidence of musculoskeletal injuries in military training on an average of 6 to 12 injuries per 100 male soldiers per month, which is an average of 16 injuries per month and the results are consistent. Also, among the mentioned risk factors, low physical fitness, running long distances and excessive training were among the things that were similar to the causes of physical injuries mentioned by the soldiers.
According to the demographic data, most soldiers showed favorable conditions in terms of physical activity and the amount of activity in sports before the training course. But what is clear is that the high volume of theoretical and practical classes and the significant reduction in the volume of sports training with the beginning of the training course have led to a decrease in physical fitness and consequently an increase in the risk of injury among soldiers. It seems necessary to re-examine the topics and time of theoretical and practical classes to improve the physical condition of soldiers in the form of physical fitness classes and injury prevention exercises to increase their performance efficiency. According to Zarei et al.’s research, factors, such as correct implementation of exercises, prevention of overtraining, performing neuromuscular and sensory and depth exercises, and agility can provide positive effects on soldiers’ physical health during the training period [32].
Looking at the obtained information related to the frequency of musculoskeletal injuries by month, the highest incidence rate of injuries is in the second month and the lowest is in the sixth month. In the first, third, fourth, and fifth months, we see a balanced incidence rate. It seems that after the beginning of the practical classes, factors, such as lack of proper physical preparation and exposure to new and relatively intense exercises, which was the second traumatic factor mentioned by the soldiers, caused them to face physical injuries at the beginning of the course. After that, he adapted to the exercises, and in the third to fifth months, the injury rate was stable. Of course, this case can indicate another problem called damage caused by repeated use. Considering that according to the results, about 35% of people with injuries have already suffered from injuries, it is emphasized that a significant part of the soldiers entered the cycle of repetitive use injury and did not get enough opportunity to improve their physical condition. Also, the exercises that have led to the occurrence of injuries remain strong due to the lack of a rehabilitation and recovery program and strengthen and complete the injury cycle. But the point is that this cycle of injuries caused by repeated use at the end of the training period did not lead to acute injuries. Rather, the rate of musculoskeletal injuries in the last month was lower than in other months, which could probably be related to the reduction in training volume in the last month of the year.
Regarding the factors affecting the occurrence of injuries, Arshi et al. showed that the parade factor can increase the rate of injury in the lower limbs during the training period. In this respect, the ankle and leg areas had the highest rate of injury, and the results of the present study also confirm this issue [17]. Since the way of marching the soldiers had a wrong and traumatic pattern and movement corrections had not been made, the landing regiments hit the ground with relatively high intensity in the heel area and the force was exerted directly on the wrist joint. The foot enters and then it manifests as compressive force and hyperextension in the knee joint. Heavy and non-standard boots increase the severity of damage to the mentioned joints. It seems that shortening the time and intensity of the parade can greatly help to reduce the rate of lower limb injuries and improve the performance of learners in practical classes. Continuing the discussion of the cause of injuries, this issue can be related to the main activities performed by the learners, including running, parade, and running, which are part of the dominant exercises. According to the results of this research, parades, intense exercises, and standing for a long time had the largest share among the existing causes. Najafi et al. also stated that the most common cause of musculoskeletal injuries is slipping or falling during physical activity, which is relatively consistent with the second factor obtained in the results of this research. However, on the other hand, the most common type of musculoskeletal injury in their research was superficial injury, which is caused by the same common cause mentioned [33]; while it is clear that the injuries that occurred in the society of this research are mostly caused by frequent activity and lack of physical fitness, especially regarding general physical fitness. Also, the weakness in the stability and proper functioning of the muscles of the central region and lower limbs and finally the wrong training patterns are due to the lack of sufficient information of trainers and soldiers.
During the 101-day training period, some people did exercises and activities in the practical class despite suffering from physical injuries. In other words, on a monthly average, 9.1% of soldiers could not participate well in physical activity classes due to injuries. In this regard, on average, the number of injured soldiers per month who experienced an injury for the first time was nearly double compared to the soldiers who were injured for the second time or more. This issue shows that in addition to the training and activities of soldiers being traumatic, the lack of recovery from injury and the existence of a cycle of re-injury are other problems of soldiers’ activities.
Conclusion
What is clear in the first place is that the prevalence rate of musculoskeletal injuries in the community of this research did not show a high number. Of course, this issue is partly related to the type of questionnaire used and the limitations mentioned in the research. Also, the lack of attention to maintaining and improving the physical fitness of soldiers during the course and the lack of control of traumatic factors have caused a significant part of the soldiers to finish the training course with chronic injuries and weak physical fitness. The existence of a cycle of prevention and recovery from physical injury is the missing link of military training courses and is the main responsible for the cost of human and financial capital.
Finally, factors, such as lack of access to a higher number of samples, the impossibility of conducting research in the first half of the year, and the warmer seasons of the year can be mentioned. The impossibility of measuring the present prevalence in all educational barracks related to the organization in question to compare the results and also some considerations of soldiers in providing information related to physical injuries and health are among the limitations of the present research.
Ethical Considerations
Compliance with ethical guidelines
All ethical principles are considered in this article. The participants were informed of the purpose of the research and its implementation stages. They were also assured about the confidentiality of their information and were free to leave the study whenever they wished, and if desired, the research results would be available to them. A written consent has been obtained from the subjects.
Funding
The current research is taken from the military service project of Mohammad Shahabi in the Vice-President of Education and Training of the Police Command of the Islamic Republic of Iran.
Authors' contributions
All authors equally contributed to the present study.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors thank all the participants of the research, as well as all the personnel who helped us with this research, especially the employees of the Education and Training Department of the Police Command of the Islamic Republic of Iran.
References
The military system is a complex system with wide and scattered locations that differ in terms of size, human resources and facilities, tasks, and composition [1]. Human power is considered as the main pillar of this system and their health is directly related to improving the quality of services and is of particular importance. Intensive military training courses are among the programs and special tasks related to the military forces, whose purpose is to improve the specific skills of soldiers at the beginning of their time in these organizations.
Recruits are prone to training-related injuries because they encounter a new living environment with intense training. Training injuries are the main cause of disability, long-term rehabilitation, functional impairment, and early discharge from military service [2-5]. While on duty, police officers must perform various heavy movements, including movements, such as running, jumping, crawling, balancing, climbing, lifting, carrying, pushing, pulling, and fighting in unpredictable environments [6, 7]. The results of all these actions can lead to injuries in various places, such as the back, knees, and shoulders, which have been reported among the injuries known to police officers [8]. Musculoskeletal injuries are the main cause of medical discharge and medical demotion in the UK Armed Forces [9] and are the most common reason why military personnel seek medical and health care [10, 11]. At any time, it is reported that between 15% and 30% of trained military personnel are not medically prepared for deployment due to musculoskeletal injuries [12].
The prevalence rate of musculoskeletal injuries has a wide range and has been reported in different sources from 20% [13] to 48% [14] and 58% [3]. The studies conducted in Iran also confirm the relatively high rate of injuries in the military forces. Farahani et al. reported a prevalence of 27.4% and an incidence of 10.2 injuries per 100 soldiers per month in Iran’s military forces [15]. Also, in 150 men examined by Naja, the most common injured areas were the knee at 45.4%, the waist at 30.7%, and the ankle at 17% [16]. Arshi et al. in a study showed a significant difference between the injuries of the marching group before and after 5 months of the parade. The most injuries were ankle 25.9% and leg 26.9%, which accounted for the highest percentage in the first stage, and in the second stage, it changed to the knee 46.6% [17]. Looking at all the health problems related to the military, musculoskeletal disorders account for a larger share of the total injuries in the military group. These disorders are associated with reduced productivity of the injured person while attending activities as well as loss of duty days and are responsible for 42% of all medical leaves in the Canadian Armed Forces [18, 19]. Musculoskeletal injuries are a major contributor to medical care visits and costs in the US military, accounting for approximately 2.4 million medical visits and $548 million in direct patient care costs [20]. The issue of musculoskeletal injuries and disorders among military groups has been one of the main challenges and concerns of military organizations and personnel since many years ago, in such a way that these injuries cause a lot of financial, physical, and mental costs for the system. The management of this phenomenon brings many challenges for military organizations, including the use of financial resources. The financial costs related to musculoskeletal disorders in military budgets are known globally [21-23].
Materials and Methods
In this study, which is retrospective and descriptive epidemiology, the incidence rate, prevalence, and consequences of musculoskeletal injuries in newly enlisted soldiers who entered the pre-service training course during 6 months have been investigated. A total of 124 male soldiers with a mean age of 20.76 years, mean height of 178.52 cm, mean weight of 72.92 kg and mean activity per week for 3 hours and 19 minutes participated in this study. The participants were selected by convenience method and from one of the specialized training barracks affiliated with the Tehran police forces. All subjects were informed about the coordinates of the study and its implementation, recorded their demographic information, and read and signed the written consent form. Soldiers with severe injuries and a history of surgery in the last 6 months were prohibited from entering the plan. Also, the participants who were not eligible to participate in the project due to unwillingness to cooperate and failure to complete the questionnaire during the project were excluded. The main exercises and activities that the soldiers did in the 6-month training course included self-defense combat, arresting the accused, running and stopping consecutively, deep squats, parading, standing still without moving, and physical fitness class.
The participants completed a questionnaire related to the registration of musculoskeletal injuries, known as Oslo Sports Trauma Research Center (OSTRC), through the relevant worksheet and every month [24]. The OSTRC questionnaire, which is related to musculoskeletal injuries and diseases and can be adapted to a wide range of sports, and according to the results of the self-reporting of the participants, monitors variables, such as symptoms, severity, and impact of physical injuries [25]. This questionnaire has been approved in the groups of athletes and has been prepared from the questionnaire related to the registration of injuries caused by excessive use of OSTRC [26]. Also, Mirkarimpour et al. have investigated and presented the validity, reliability, and localization of this questionnaire [27]. In this regard, the results of the content validity index (CVI) indicated that all questions had a CVI score higher than 0.79 (on the scale of communication 0.92, clarity 0.98, simplicity 0.99, and ambiguity 0.94). It is worth mentioning that the average content validity index (scale CVI [S-CVI]/Ave) of the questionnaire was 0.95 (0.85-1). Statistical analysis showed that the internal consistency of the first 4 questions of the questionnaire has Cronbach’s α equal to 0.89. Kappa agreement coefficient (P=0.001) was also obtained from 0.71 to 0.81.
The participants completed the questionnaire monthly on Thursday afternoon of the last week of each month using a printed questionnaire with the supervision of the researcher. They were asked to report information about the injuries they had experienced in the past month and could only report a maximum of two different injuries each month. The revised local version of the OSTRC questionnaire included four key questions (Figure 1) and seven additional questions [24] and diseases were not examined in this study.
In this questionnaire, the participants were asked about the effect of physical injury on participation in sports classes, training volume, physical performance status, and severity of symptoms experienced due to injury in the past month. If the participants reported the first options in the first four key questions of the questionnaire, i.e. full participation without injury, participation without reducing the amount of training, full participation without reducing performance, and finally, full participation without symptoms, the questionnaire would be completed for the last month. If participants answered any of the four initial key questions other than the first option, they were directed to additional questions. Also, an open question was added to the mentioned questionnaire to identify any damage with its consequences that were not included in the worksheet. Participants who reported worrisome and serious injuries lasting more than 4–6 weeks were referred to a physician by the researcher. Similar injuries reported that were located in the vicinity of each other were considered as a case and analyzed [26, 28]. Before the start of the 6 months, questionnaire data was collected on a trial basis for one month to determine the possibility of false reporting and to remind the participants of the problems related to how to complete the questionnaire. The mentioned data were not used in calculations and analyses. Descriptive data were presented as Mean±SD. Prevalence was defined as the proportion of the study population that had cases of physical injury each month and was also calculated by dividing the number of participants who reported an injury by the number of questionnaire respondents in that month.
In the following, the prevalence of effective musculoskeletal injuries was calculated and defined as injuries that lead to a moderate or severe reduction in exercise volume and performance, as well as a complete inability to participate in exercise or physical activity [24]. After collecting the research information, the data related to the characteristics of the subjects, such as age, height, and weight, as well as the variables related to the prevalence of musculoskeletal injuries and other subordinate cases in the descriptive statistics section and in the Excel software with the relevant charts and also using SPSS software, version 24 was analyzed.
Results
In the descriptive results section, according to the information in the Table 1, the participants had a mean age of 20.7 years, a mean height of 178.5 cm, a mean weight of 72.9 kg, and a mean activity per week for 3 hours and 19 minutes.
Regarding the prevalence of musculoskeletal injuries, the data was extracted and analyzed separately for each month, and below only the table related to the average of 6 months is presented. Among the critical information in Table 2, we can mention the quality of soldiers’ participation in practical classes, the crucial damaged parts of the body, the number of days affected due to the presence of injuries, and the cause of injuries from the soldiers’ point of view.
One of the variables investigated in prevalence reports is the quality and participation rate of soldiers in practical classes. According to Figure 2 on average, 86% of the soldiers managed to fully participate in practical classes without injury during the 6 months. Likewise, 9.1% of them were able to fully participate in the class even though they were injured, but they somehow carried the pain and hardship of the injury with them. Among them, only 3.8% could not attend the classes properly and completely due to injuries and had to leave the class for a while.
Figure 3 shows that some soldiers had at least one injury for 101 days during the 6 months, and at the same time, they attended practical classes but failed to perform properly. About a quarter of the soldiers, despite having physical injuries, could fully participate in the practical classes without any problems or missing a day.
As it is clear from Figure 4 the ankle area with 2.8% damage on a monthly average took the largest share among the damaged areas. Also, the lumbar spine had the lowest share with 1.8% and, finally, the knee was the second most affected area with 2.2%. A significant number of soldiers chose the other option but did not mention the exact area they wanted.
Also, looking at Figure 5, among the traumatic factors recorded by the soldiers, the parade was the vital factor with 22.5%. Also, among the mentioned cases, Putin had the lowest share among the factors with 5%. The interesting thing to note is the option of Sayer with 33.1%, which has the largest share among the factors, although, as before, the name of the desired factor was not mentioned by the soldiers. Finally, high-intensity training with 17.5%, and long-term standing with 11.2% were among other factors.
Finally, according to Figure 6 in the frequency of damaged areas by month, the sixth month had the lowest injury rate with 6 cases. In contrast, the second month with 17 cases of injury reports accounted for the highest amount among the months. On the other hand, other months did not show much difference in the number of injuries compared to each other.
Discussion
According to the obtained results, ankles with 2.8%, knees with 2.2% and lumbar spine with 1.8% had the highest prevalence rates among the participants. What is clear is that the lower limbs and the central region are the most damaged areas, and the spine of the back, head, neck, and upper limbs were not among the most damaged areas. This issue can also be seen in the results of past research, which identified the lumbar spine at 22.2% and the ankle at 15.1% as the most common injured areas [29]. Other recent research has confirmed the higher frequency of lower limb injuries, especially in the ankle area, during complex dynamic activities with military uniforms [30]. Also, Yavnai et al.’s research reported that the injured areas with pain in soldiers were the ankle area at 32.8%, knee area at 17.2%, calf area at 17.2%, and finally other lower limb areas at 32.8% [31]. In terms of the damaged points, the results obtained are consistent with the research of Nodehimoghadam et al. [16], but no alignment is observed in terms of the order of the damaged points and the prevalence rate. Of course, considering that the questionnaire was completed monthly and the prevalence rate of musculoskeletal injuries was calculated as an average of 6 months, this percentage difference related to the prevalence is justified. In other words, this difference can be caused by the difference in the type of questionnaire and the number of data collection times. In another study, Zarei et al. [32] reported the incidence of musculoskeletal injuries in military training on an average of 6 to 12 injuries per 100 male soldiers per month, which is an average of 16 injuries per month and the results are consistent. Also, among the mentioned risk factors, low physical fitness, running long distances and excessive training were among the things that were similar to the causes of physical injuries mentioned by the soldiers.
According to the demographic data, most soldiers showed favorable conditions in terms of physical activity and the amount of activity in sports before the training course. But what is clear is that the high volume of theoretical and practical classes and the significant reduction in the volume of sports training with the beginning of the training course have led to a decrease in physical fitness and consequently an increase in the risk of injury among soldiers. It seems necessary to re-examine the topics and time of theoretical and practical classes to improve the physical condition of soldiers in the form of physical fitness classes and injury prevention exercises to increase their performance efficiency. According to Zarei et al.’s research, factors, such as correct implementation of exercises, prevention of overtraining, performing neuromuscular and sensory and depth exercises, and agility can provide positive effects on soldiers’ physical health during the training period [32].
Looking at the obtained information related to the frequency of musculoskeletal injuries by month, the highest incidence rate of injuries is in the second month and the lowest is in the sixth month. In the first, third, fourth, and fifth months, we see a balanced incidence rate. It seems that after the beginning of the practical classes, factors, such as lack of proper physical preparation and exposure to new and relatively intense exercises, which was the second traumatic factor mentioned by the soldiers, caused them to face physical injuries at the beginning of the course. After that, he adapted to the exercises, and in the third to fifth months, the injury rate was stable. Of course, this case can indicate another problem called damage caused by repeated use. Considering that according to the results, about 35% of people with injuries have already suffered from injuries, it is emphasized that a significant part of the soldiers entered the cycle of repetitive use injury and did not get enough opportunity to improve their physical condition. Also, the exercises that have led to the occurrence of injuries remain strong due to the lack of a rehabilitation and recovery program and strengthen and complete the injury cycle. But the point is that this cycle of injuries caused by repeated use at the end of the training period did not lead to acute injuries. Rather, the rate of musculoskeletal injuries in the last month was lower than in other months, which could probably be related to the reduction in training volume in the last month of the year.
Regarding the factors affecting the occurrence of injuries, Arshi et al. showed that the parade factor can increase the rate of injury in the lower limbs during the training period. In this respect, the ankle and leg areas had the highest rate of injury, and the results of the present study also confirm this issue [17]. Since the way of marching the soldiers had a wrong and traumatic pattern and movement corrections had not been made, the landing regiments hit the ground with relatively high intensity in the heel area and the force was exerted directly on the wrist joint. The foot enters and then it manifests as compressive force and hyperextension in the knee joint. Heavy and non-standard boots increase the severity of damage to the mentioned joints. It seems that shortening the time and intensity of the parade can greatly help to reduce the rate of lower limb injuries and improve the performance of learners in practical classes. Continuing the discussion of the cause of injuries, this issue can be related to the main activities performed by the learners, including running, parade, and running, which are part of the dominant exercises. According to the results of this research, parades, intense exercises, and standing for a long time had the largest share among the existing causes. Najafi et al. also stated that the most common cause of musculoskeletal injuries is slipping or falling during physical activity, which is relatively consistent with the second factor obtained in the results of this research. However, on the other hand, the most common type of musculoskeletal injury in their research was superficial injury, which is caused by the same common cause mentioned [33]; while it is clear that the injuries that occurred in the society of this research are mostly caused by frequent activity and lack of physical fitness, especially regarding general physical fitness. Also, the weakness in the stability and proper functioning of the muscles of the central region and lower limbs and finally the wrong training patterns are due to the lack of sufficient information of trainers and soldiers.
During the 101-day training period, some people did exercises and activities in the practical class despite suffering from physical injuries. In other words, on a monthly average, 9.1% of soldiers could not participate well in physical activity classes due to injuries. In this regard, on average, the number of injured soldiers per month who experienced an injury for the first time was nearly double compared to the soldiers who were injured for the second time or more. This issue shows that in addition to the training and activities of soldiers being traumatic, the lack of recovery from injury and the existence of a cycle of re-injury are other problems of soldiers’ activities.
Conclusion
What is clear in the first place is that the prevalence rate of musculoskeletal injuries in the community of this research did not show a high number. Of course, this issue is partly related to the type of questionnaire used and the limitations mentioned in the research. Also, the lack of attention to maintaining and improving the physical fitness of soldiers during the course and the lack of control of traumatic factors have caused a significant part of the soldiers to finish the training course with chronic injuries and weak physical fitness. The existence of a cycle of prevention and recovery from physical injury is the missing link of military training courses and is the main responsible for the cost of human and financial capital.
Finally, factors, such as lack of access to a higher number of samples, the impossibility of conducting research in the first half of the year, and the warmer seasons of the year can be mentioned. The impossibility of measuring the present prevalence in all educational barracks related to the organization in question to compare the results and also some considerations of soldiers in providing information related to physical injuries and health are among the limitations of the present research.
Ethical Considerations
Compliance with ethical guidelines
All ethical principles are considered in this article. The participants were informed of the purpose of the research and its implementation stages. They were also assured about the confidentiality of their information and were free to leave the study whenever they wished, and if desired, the research results would be available to them. A written consent has been obtained from the subjects.
Funding
The current research is taken from the military service project of Mohammad Shahabi in the Vice-President of Education and Training of the Police Command of the Islamic Republic of Iran.
Authors' contributions
All authors equally contributed to the present study.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors thank all the participants of the research, as well as all the personnel who helped us with this research, especially the employees of the Education and Training Department of the Police Command of the Islamic Republic of Iran.
References
- Mior SA, Vogel E, Sutton D, French S, Côté P, Nordin M, et al. Exploring chiropractic services in the Canadian Forces Health Services-perceptions of facilitators and barriers among key informants. Military Medicine. 2019; 184(5-6):e344-e51. [DOI:10.1093/milmed/usy319] [PMID]
- Taanila H, Suni J, Pihlajamäki H, Mattila VM, Ohrankämmen O, Vuorinen P, et al. Musculoskeletal disorders in physically active conscripts: A one-year follow-up study in the Finnish Defence Forces. BMC Musculoskeletal Disorders. 2009; 10:89. [DOI:10.1186/1471-2474-10-89] [PMID]
- Sharma J, Greeves JP, Byers M, Bennett AN, Spears IR. Musculoskeletal injuries in British Army recruits: A prospective study of diagnosis-specific incidence and rehabilitation times. BMC Musculoskeletal Disorders. 2015; 16:106.[DOI:10.1186/s12891-015-0558-6] [PMID]
- Taanila H, Suni J, Pihlajamäki H, Mattila VM, Ohrankämmen O, Vuorinen P, et al. Aetiology and risk factors of musculoskeletal disorders in physically active conscripts: A follow-up study in the Finnish Defence Forces. BMC Musculoskeletal Disorders. 2010; 11:146. [DOI:10.1186/1471-2474-11-146] [PMID]
- Taanila H, Suni JH, Kannus P, Pihlajamäki H, Ruohola JP, Viskari J, et al. Risk factors of acute and overuse musculoskeletal injuries among young conscripts: A population-based cohort study. BMC Musculoskeletal Disorders. 2015; 16:104. [DOI:10.1186/s12891-015-0557-7] [PMID]
- Blacker SD, Carter JM, Wilkinson DM, Richmond VL, Rayson MP, Peattie M. Physiological responses of Police Officers during job simulations wearing chemical, biological, radiological and nuclear personal protective equipment. Ergonomics. 2013; 56(1):137-47. [DOI:10.1080/00140139.2012.734335] [PMID]
- Carlton SD, Orr RM, Stierli M, Carbone PD. The impact of load carriage on mobility and marksmanship of the tactical response officer. Paper presented at: 2013 Australian strength and conditioning association international conference on applied strength and conditioning. 8-10 November 2013; Australia: Melbourne. [Link]
- Orr R, Stierli M. Injuries common to tactical personnel (A multidisciplinary review). Paper presented at: 2013 Australian Strength and Conditioning Association International Conference on Applied Strength and Conditioning. Melbourne, Australia. [Link]
- Department of manning (army). Interim report on the health risks to women in ground close combat roles. Department of manning (army). England: Hampshire; 2016. [Link]
- Hauret KG, Jones BH, Bullock SH, Canham-Chervak M, Canada S. Musculoskeletal injuries description of an under-recognized injury problem among military personnel. American Journal of Preventive Medicine. 2010; 38(1 Suppl):S61-70. [DOI:10.1016/j.amepre.2009.10.021] [PMID]
- Jones BH, Canham-Chervak M, Canada S, Mitchener TA, Moore S. Medical surveillance of injuries in the US militarydescriptive epidemiology and recommendations for improvement. American Journal of Preventive Medicine. 2010; 38(1 Suppl):S42-60. [DOI:10.1016/j.amepre.2009.10.014] [PMID]
- Heagerty R, Sharma J. Musculoskeletal training injury in military recruit populations: An integrated prevention strategy-project OMEGA-(Part 1). International Journal of Physical Medicine & Rehabilitation. 2018; 6(1):1-11. [Link]
- Franklyn-Miller A, Wilson C, Bilzon J, McCrory P. Foot orthoses in the prevention of injury in initial military training: A randomized controlled trial. The American Journal of Sports Medicine. 2011; 39(1):30-7. [DOI:10.1177/0363546510382852] [PMID]
- Sharma J. The development and evaluation of a management plan for musculoskeletal injuries in British army recruits: A series of exploratory trials on medial tibial stress syndrome PhD dissertation. Middlesbrough: Teesside University; 2013. [Link]
- Farahani H, Sanei S, Naji M, Sadr S, Khakpoor S, Divandari H. [The investigation of incidence rate and causes of physical injuries in sport activities and military parade and developing strategies to prevent them (Persian)]. Military Medicine Journal. 2009; 2(5):21-32. [Link]
- Nodehimoghadam A, Hossein Zade A. [Determination of the most common sites of musculoskeletal injuries and the relationship between sports history with musculoskeletal injuries during the course of 6 months police military exercises (Persian)]. Journal of Police Medicine. 2017; 6(2):143-9. [Link]
- Arshi AR, Hosseini SM, Alizadeh Sh, Bakhshi E. [The effect of 5 month Military marchon injuries of police university male students (Persian)]. Journal for Research in Sport Rehabilitation. 2017; 4(8):96-89. [Link]
- Born J, Bogaert L, Payne E, Wiens M. Results from health and lifestyle information survey of Canadian forces personnel 2008/2009. Ottawa-Ontario: Department of National Defence; 2010. [Link]
- Rowe P, Hébert L. The impact of musculoskeletal conditions on the Canadian Forces. In: Aiken AB, Bélanger SAH, editors. Shaping the future: Military and veteran health research. Ontario: Canadian Defence Academy Press; 2011. [Link]
- Teyhen DS, Goffar SL, Shaffer SW, Kiesel K, Butler RJ, Tedaldi AM, et al. Incidence of musculoskeletal injury in US Army unit types: A prospective cohort study. Journal of Orthopaedic & Sports Physical Therapy. 2018; 48(10):749-57. [DOI:10.2519/jospt.2018.7979] [PMID]
- Heagerty RG, Sharma J, Clayton JC. Musculoskeletal injuries in British Army recruits: A retrospective study of incidence and training outcome in different infantry regiments over five consecutive training years. International Journal of Physical Medicine & Rehabilitation. 2017; 5(6):1-11. [Link]
- Cowan DN, Jones BH, Shaffer RA. Musculoskeletal injuries in the military training environment. In: Kelley PW, editor. Military preventative medicine: Mobilization and deployment. Texas: Borden Institute, Walter Reed Army Medical Center; 2003. [Link]
- Songer TJ, LaPorte RE. Disabilities due to injury in the military. American Journal of Preventive Medicine. 2000; 18(3 Suppl):33-40. [DOI:10.1016/S0749-3797(00)00107-0] [PMID]
- Clarsen B, Rønsen O, Myklebust G, Flørenes TW, Bahr R. The Oslo Sports Trauma Research Center questionnaire on health problems: A new approach to prospective monitoring of illness and injury in elite athletes. British Journal of Sports Medicine. 2014; 48(9):754-60. [DOI:10.1136/bjsports-2012-092087] [PMID]
- Gallagher J, Needleman I, Ashley P, Sanchez RG, Lumsden R. Self-reported outcome measures of the impact of injury and illness on athlete performance: A systematic review. Sports Medicine. 2017; 47(7):1335-48. [DOI:10.1007/s40279-016-0651-5] [PMID]
- Clarsen B, Myklebust G, Bahr R. Development and validation of a new method for the registration of overuse injuries in sports injury epidemiology: The Oslo Sports Trauma Research Centre (OSTRC) overuse injury questionnaire. British Journal of Sports Medicine. 2013; 47(8):495-502. [DOI:10.1136/bjsports-2012-091524] [PMID]
- Mirkarimpour SH, Alizadeh MH, Rajabi R, Kazemnejad A. [Validity and reliability of the Persian Version of Oslo Sport Trauma Research Center Questionnaire on Health Problems (OSTRC) (Persian)]. Sport Sciences and Health Research. 2018; 10(1):1-17. [Link]
- Moseid CH, Myklebust G, Fagerland MW, Clarsen B, Bahr R. The prevalence and severity of health problems in youth elite sports: A 6-month prospective cohort study of 320 athletes. Scandinavian Journal of Medicine & Science in Sports. 2018; 28(4):1412-23. [DOI:10.1111/sms.13047] [PMID]
- Strowbridge NF, Burgess KR. Sports and training injuries in British soldiers: The Colchester Garrison Sports Injury and Rehabilitation Centre. Journal of the Royal Army Medical Corps. 2002; 148(3):236-43. [DOI:10.1136/jramc-148-03-03] [PMID]
- Sell TC, Pederson JJ, Abt JP, Nagai T, Deluzio J, Wirt MD, et al. The addition of body amor diminishes dynamic postural stability in military soldiers. Military Medicine. 2013; 178(1):76-81. [DOI:10.7205/MILMED-D-12-00185] [PMID]
- Yavnai N, Bar-Sela S, Pantanowitz M, Funk S, Waddington G, Simchas L, et al. Incidence of injuries and factors related to injuries in combat soldiers. BMJ Military Health. 2021; 167(6):418-23. [DOI:10.1136/jramc-2019-001312] [PMID]
- Zarei M, Rahemi M. [Military physical training-related injuries: A review of epidemiology and risk factor and prevention strategy studies (Persian)]. EBNESINA. 2015; 17(2):52-64. [Link]
- Najafi Mehris S, Sadeghian M, Tayibi A, Karimi Zarchi A, Asgari A. [Epidemiology of physical injuries caused by military training (Persian)]. Journal of Military Medicine. 2022; 12(2):89-92. [Link]
Type of Study: Research |
Subject:
General
Received: 2023/11/25 | Accepted: 2023/12/4 | Published: 2024/01/1
Received: 2023/11/25 | Accepted: 2023/12/4 | Published: 2024/01/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
