Thu, May 28, 2026
Volume 13, Issue 4 (Autumn 2023)
PTJ 2023, 13(4): 279-286 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Bohunicky S, Franklin R, Scribbans T D. Baseline Has no Effect on Change in Forward Shoulder Posture, Range of Motion, and Muscle Excitation Following Myofascial Release: A Velocity-dependent Investigation. PTJ 2023; 13 (4) :279-286
URL: http://ptj.uswr.ac.ir/article-1-603-en.html
URL: http://ptj.uswr.ac.ir/article-1-603-en.html



1- Faculty of Kinesiology and Recreation Management, University of Manitoba, Winnipeg, Canada.
Keywords: Myofascial release therapy, pectoralis muscles, Massage, Fascia, Posture, Range of motion, Electromyography
Full-Text [PDF 1317 kb]
(977 Downloads)
| Abstract (HTML) (3221 Views)
Full-Text: (745 Views)
1. Introduction
Systematic clinical investigations (i.e. randomized controlled trials) aim to establish if patients report outcomes or disease status changes following a given intervention by testing for mean differences in outcomes before and after treatment. If no difference is observed between groups or time points, investigators often conclude that an intervention was ineffective. For example, recently a massage therapy intervention did not alter pectoralis major length (PECL) and muscle excitation in individuals with forward shoulder posture (FSP) due to a lack of difference in group means [1]. However, when our data was examined on an individual basis, a range of responses was present for all variables, where some individuals experienced larger responses and others experienced little or no response (e.g. mean range: -1% (-9 to 10) change in PECL). The heterogeneity in our group data suggests that some individuals experienced substantial, potentially clinically important effects from the massage therapy treatment that were concealed by analyses of the mean values of the groups. While a variety of factors contribute to an individual’s response to an intervention, individual participants’ baseline values are known to influence changes in the same outcome variable post-treatment [2]. Thus, it is plausible that the massage therapy intervention we employed was effective at improving FSP, PECL, and/or muscle excitation for a particular subgroup within our study population.
It is well established that the magnitude and direction of response or change in an outcome variable following an intervention is affected by the baseline level of that variable [2, 3]. This phenomenon, often referred to as rate dependence, has been observed in many investigations and contexts, including drug and non-drug interventions [1]. While many previous reports have correlated pre-intervention to change scores to explore if baseline level impacts individual response [4], the correlation between these variables induces mathematical coupling and regression to the mean [1, 5]. An alternative approach, the Oldham method, determines the rate dependence of treatment effects without mathematical coupling and regression to the mean [6].
Thus, the current study determined whether there is a rate-dependent effect on FSP, PECL (as measured via shoulder horizontal abduction range of motion (ROM)), and muscle excitation of the upper (UT), middle (MT), and lower trapezius (LT), and pectoralis major (PEC) following 4 minutes of myofascial release (MFR) to the pectoral fascia. Given that restricted pectoral soft tissues are associated with FSP [7], which increases scapular protractor excitation [8] and is hypothesized to decrease scapular retractor excitation, therapists often use manual techniques, like MFR to lengthen pectoral soft tissues, reduce FSP, and correct alterations in muscle excitation. Thus, while the results of our preliminary between-group analyses indicated that MFR reduced FSP but did not affect PECL or the excitability of UT, MT, LT, and PEC, it is plausible that there were unobserved rate-dependent effects on these outcomes. For example, those with greater FSP at baseline might have experienced a larger change in FSP, while those with lesser FSP experience a smaller or no change in FSP following MFR. Therefore, we hypothesized that a rate-dependant effect will be observed for all variables examined. The results of this study may identify subpopulations that benefited from the MFR intervention, which will inform the methodological design of future massage therapy research regarding participant demographics and baseline characteristics. Further, to determine the rate-dependent effect on FSP, PECL, and muscle excitation following MFR, the first attempt is to define whether a patient’s baseline characteristics affect individual responses to a massage intervention.
2. Materials and Methods
Research design
A within-subjects, repeated-measures single-blinded crossover study was conducted where participants attended two 1-hour sessions (MFR and control [CON]) in random order (Research Randomizer 4.0, Social Psychology Network, USA). Only data from the MFR session were used. The University of Manitoba Education/ Nursing Research Ethics Board approved all experimental procedures that were conducted in compliance with the Declaration of Helsinki [9]. Informed consent was given by participants following written and verbal details of the experimental procedures.
Before (PRE) and after (POST) the MFR intervention, FSP, PECL, and excitation of the UT, MT, LT, and PEC during a reaching task were measured. A researcher took all measurements on the right side and all treatments were performed by a registered massage therapist (RMT). The current study was a retrospective analysis of data from a previous study exploring the effect of 4 minutes of MFR or soft-touch control treatment on FSP, PECL, and excitation of the UT, MT, LT, and PEC during a reaching task [1].
Participants
Sixty-six individuals were recruited from the University of Manitoba and neighboring communities via convenience sampling. Potential participants were screened for eligibility using the following inclusion criteria: the age of 18-60 years, right-hand dominant cases, no experience of recent (<6 months) pain, injury, or orthopedic disorders to the shoulders, upper back, or neck (e.g. rotator cuff tear and whiplash), and no previous diagnosis of any neurological or musculoskeletal disorders (e.g. muscular dystrophy). A minimum of 1 cm of anterior deviation of the acromion process from the lateral plum line was additionally required for participants to be considered to have FSP [10]. After attrition, 59 participants (27±9 years old, 30 females) were eligible and included in the current analysis. Participants were instructed to abstain from intense physical activity of the upper body for 48 hours leading up to each session.
FSP measurement
The double-square method was used to measure FSP. Participants stood in a relaxed position against a wall where a modified combination square (Swanson Tool Company 12-in Combo Square, Frankfurt, IL, United States) was used to measure the distance from the wall to their anterior acromion [11]. The mean of three measurements was used for analysis, and participants were instructed to step forward and shake their arms in order to reset their posture before returning to the wall for each measurement.
PECL
Since there is no standardized way to measure pectoralis major length, it was found by measuring horizontal abduction ROM (i.e. the pectoral stretch position). Participants laid supine on a plinth and horizontally abducted their right shoulder with their elbow and shoulder flexed at 90°. A meter stick was used to measure the distance between the participant’s olecranon process and the ground. The mean of three separate measurements was used for analysis. Participants horizontally adducted their arms between each measurement to the starting position.
Muscle excitation: Surface electromyography
During a goal-directed reaching task, bipolar surface electromyography (sEMG) was collected from the UT, MT, LT, and sternal fibers of PEC (Figure 1).
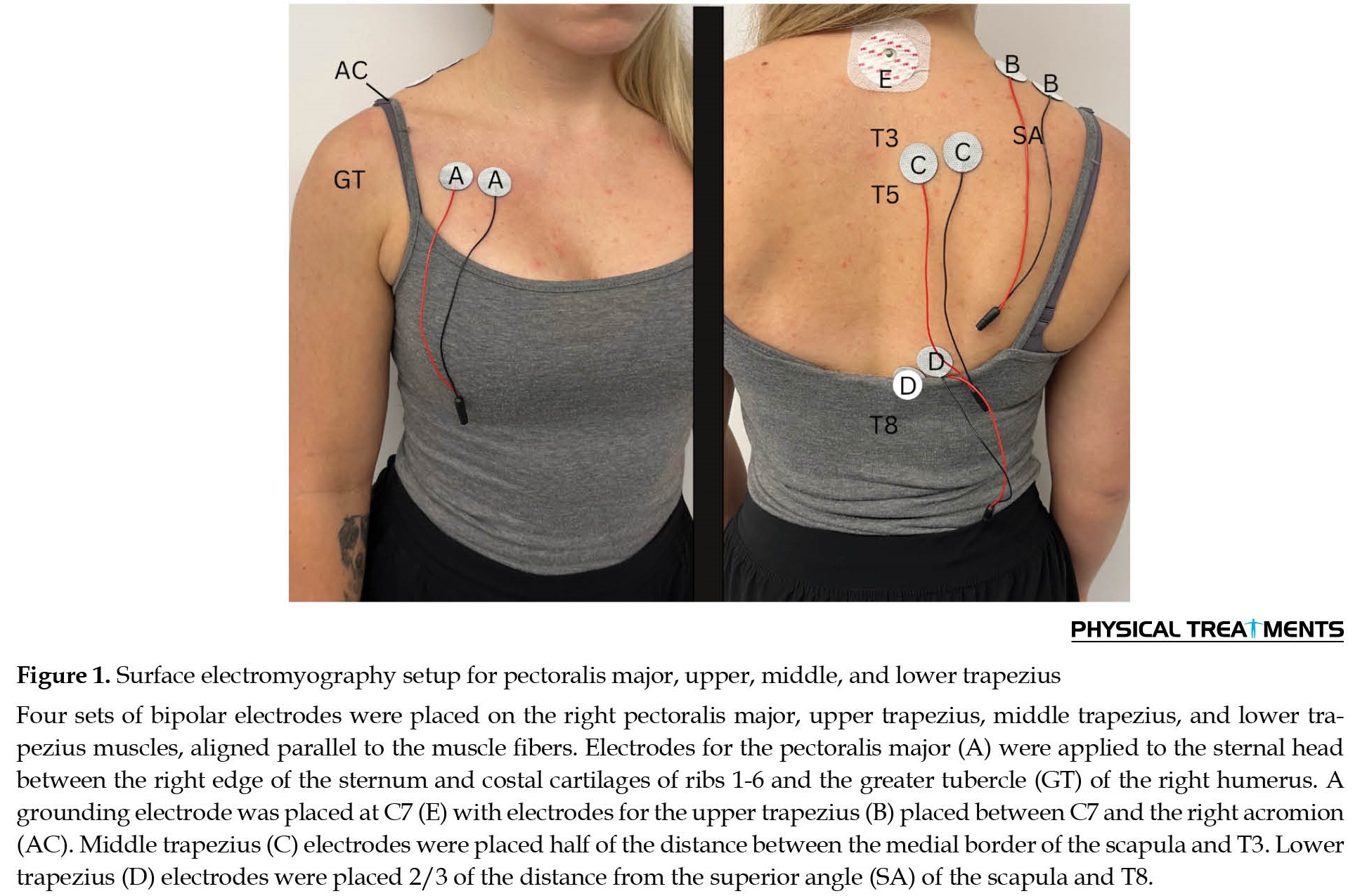 Electrode locations were landmarked, and the skin was prepared by shaving (if necessary), buffing with an abrasive paste (Nuprep, Weaver and Company, Aurora, CO, USA), and cleaning with a 70% isopropyl alcohol swab. Bipolar electrodes (CDE-C, OT Bioelettronica, Torino, Italy) were applied running approximately parallel to the direction of the muscle fibers in accordance with the surface EMG for non-invasive assessment of muscles (SENIAM) recommendations [12]. A grounding electrode was placed on the participant’s C7 spinous process, and a grounding strap was placed around their left wrist.
Electrode locations were landmarked, and the skin was prepared by shaving (if necessary), buffing with an abrasive paste (Nuprep, Weaver and Company, Aurora, CO, USA), and cleaning with a 70% isopropyl alcohol swab. Bipolar electrodes (CDE-C, OT Bioelettronica, Torino, Italy) were applied running approximately parallel to the direction of the muscle fibers in accordance with the surface EMG for non-invasive assessment of muscles (SENIAM) recommendations [12]. A grounding electrode was placed on the participant’s C7 spinous process, and a grounding strap was placed around their left wrist.
Maximal voluntary contractions (MVCs)
Participants performed one familiarization maximal voluntary contraction (MVC), followed by three MVCs for the trapezius, and then the PEC to use as a reference contraction for excitation during the reaching task.
For the trapezius MVC, participants assumed an LT-MVC prone position on a plinth with their shoulder abducted to 120°. Participants were instructed to extend their arms, pulling up on an inextensible handle towards the ceiling. Compared to individual test positions for the UT and MT, the LT MVC position provides the greatest excitation for all three regions of the trapezius and was therefore used for the trapezius MVC. For the PEC MVC, participants attempted to horizontally adduct the handle while lying supine on the plinth with their shoulder abducted at 90° [13]. For all MVCs, a 5-second countdown was provided, and participants were directed to contract as hard as possible for 5 seconds using the targeted muscles. Two minutes of rest were given between each repetition.
Reaching task
Surface electromyography of the UT, MT, LT, and PEC was collected during a reaching task where participants sat at a height-adjustable workstation with a touchscreen monitor (NEC EX241UN-PT-H, Sharp NEC Display Solutions Ltd., USA). The workstation was configured to their height and reach, where the table height allowed their elbows to be flexed to ~80° with their hands flat on the table. The monitor was set at a distance where the elbows were flexed to ~20° degrees to touch the center of the screen. This reaching task aimed to simulate a functional activity that is common in everyday activities and occupational settings, involving tasks, such as computer operation and grasping for small objects.
A custom-written E-Prime program (v3.0 Psychology)
Software Tools Inc., Pittsburgh, PA, United States) was used for the reaching task. Participants reached from a “home” button (a consistent starting position located on the tabletop) to one of five targets displayed on the monitor. Each target appeared as a black square and was presented in a pseudorandomized order. Each target, located in the center or any of the four corners of the monitor, appeared 12 times, for a total of 60 targets per testing block. The reaching task took approximately 4 minutes to complete.
Participants completed a short familiarization block that demonstrated the location of all five targets. The home key, consisting of a microswitch (Submini Snap Action Switch, Philmore Manufacturing, Rockford, USA), was embedded on the table surface in front of the participants. Participants were instructed to press and hold the home button, which triggered a “fixation” screen for a short, random period (2000 to 2500 ms). One of the five targets appeared randomly, and participants released the home button, reached the center of the target, and pressed the center of the target as quickly and accurately as possible using their right arm. Participants returned to the home position once the target was pressed. E-Prime recorded participant reactions and movement times via the microswitch and touchscreen. Only movements to the top-right target position were analyzed to account for the variance in muscle excitation patterns between target locations. To prevent repetitive and anticipated movements, additional target locations were included.
Interventions
Both treatments were administered by an RMT (18 years of experience) with training in MFR to the right pectoral fascia; however, only the MFR treatment was examined for this analysis. In order to maintain consistent placement and reduce impedance between measurements, electrode locations were outlined after the PRE intervention measurements and removed to allow for treatment. Researchers were blinded to the treatment condition and left the laboratory prior to treatment initiation.
Participants lay supine on a plinth with their arms resting by their sides and a bolster under their knees. The intervention given during both sessions was unknown to the participants. The RMT instructed participants to notify them to change the pressure if they felt seven out of ten or more discomfort or a burning sensation; however, no participant reported this.
The MFR intervention lasted 4 minutes, given previous reports that 3.3 minutes of MFR modifies fascial fibrosis [14]. The RMT applied a cross-hand technique to the superficial right pectoral fascia, where one hand (anchoring hand) was placed on the right edge of the sternum (ribs 3-6), and the other hand (mobilizing hand) was placed over the anterior aspect of the humerus at the PEC insertion point. They applied gentle posterior pressure to the anchoring hand to “hold” the fascia in place and moderate posterolateral pressure to the mobilizing hand to take up the slack within the fascial tissue. This allowed for a mechanical stretch of the pectoral fascia without gliding. After 4 minutes, the therapist gradually released any pressure exerted by the mobilizing hand followed by the anchoring hand after each intervention. The PEC electrodes were reapplied to the outline on the participant’s chest. A modified t-shirt was provided to visually conceal the treatment area but could allow access to the electrode wiring.
Surface electromyography data processing
Data processing was performed by a blinded investigator. Also, sEMG signals were recorded and processed using OT BioLab+(v1.3.2, OT Bioelettronica, Torino, Italy). Data were sampled at 2,048 in a bipolar configuration with a gain of 500, band-pass filtered (-3 dB bandwidth, 10-500 Hz), and digitally converted by a 16-bit A/D converter (Quattrocento, OT Bioelettronica, Torino, Italy). Signals were digitally band-pass Butterworth filtered at 30-500 Hz post-collection to remove electrocardiogram contamination from the EMG signal [15]. The root-mean-square (RMS) was calculated for each pair of bipolar electrodes. Data were exported from OT BioLab+ as a .csv file in 0.001 epochs.
Each muscle’s peak excitation was identified, and a one-second period (0.5 s before/after) surrounding the peak was used as a reference. The movement time of each top-right target was used to assess muscle excitation during the reaching task (i.e. release of the microswitch to touch of target), as movement onset for each target was timestamped on the sEMG recording. The mean RMS of the 12 movement times was divided by the respective muscle’s MVC to yield a percentage of excitation for each muscle, which was used for analysis.
Statistical analysis
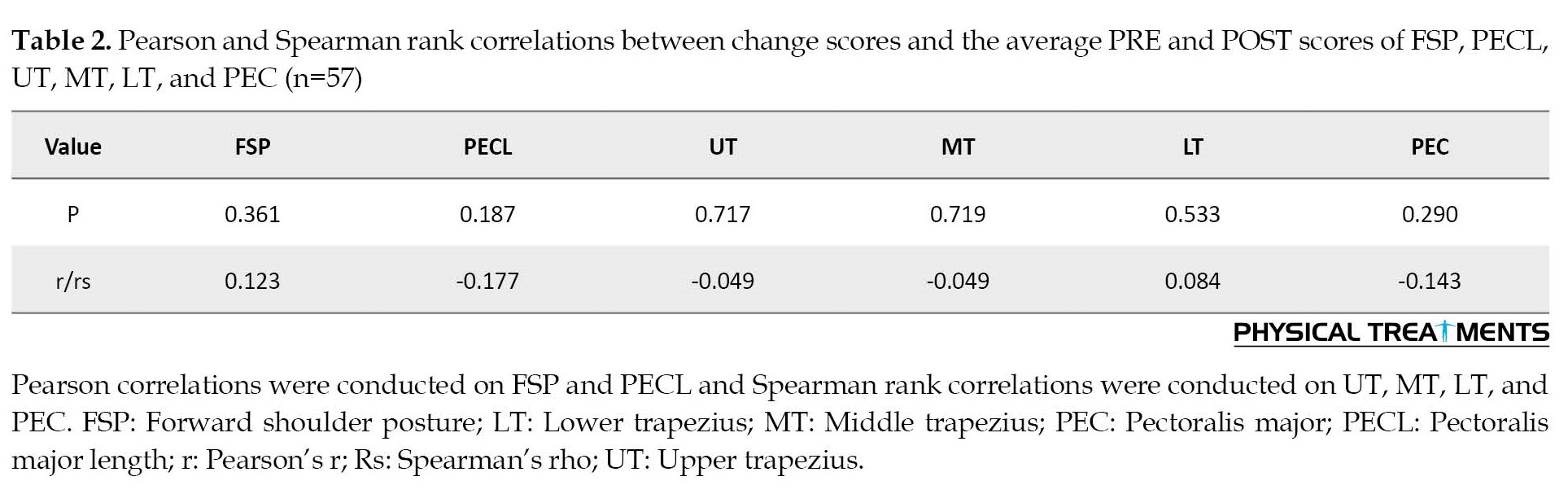
Statistical analysis was performed using Jamovi 2.3. Normality was assessed using the Shapiro-Wilk test, where p>0.05 indicated that the data were normally distributed. Using the Oldham method [6], correlations were conducted on the difference between PRE and POST values (PRE – POST; Δ) and the sum of PRE and POST values divided by 2 ([PRE+POST]/2; x̄) for each of the following variables: FSP, PECL, and muscle excitation (UT, MT, LT, and PEC). Pearson correlations were conducted on normally distributed data, and Spearman rank correlations were conducted on abnormally distributed data. Statistical significance was accepted at p<0.05, and correlation coefficients (r/rs) were interpreted as low <0.3, moderate 0.3-0.49, and high >0.5.
3. Results
FSP and PECL Data were normally distributed, while UT, MT, LT, and PEC data were not normally distributed (p<0.05); thus, the Pearson’s and Spearman’s Rank correlations were conducted, respectively. Descriptive statistics for all variables are presented in Table 1.
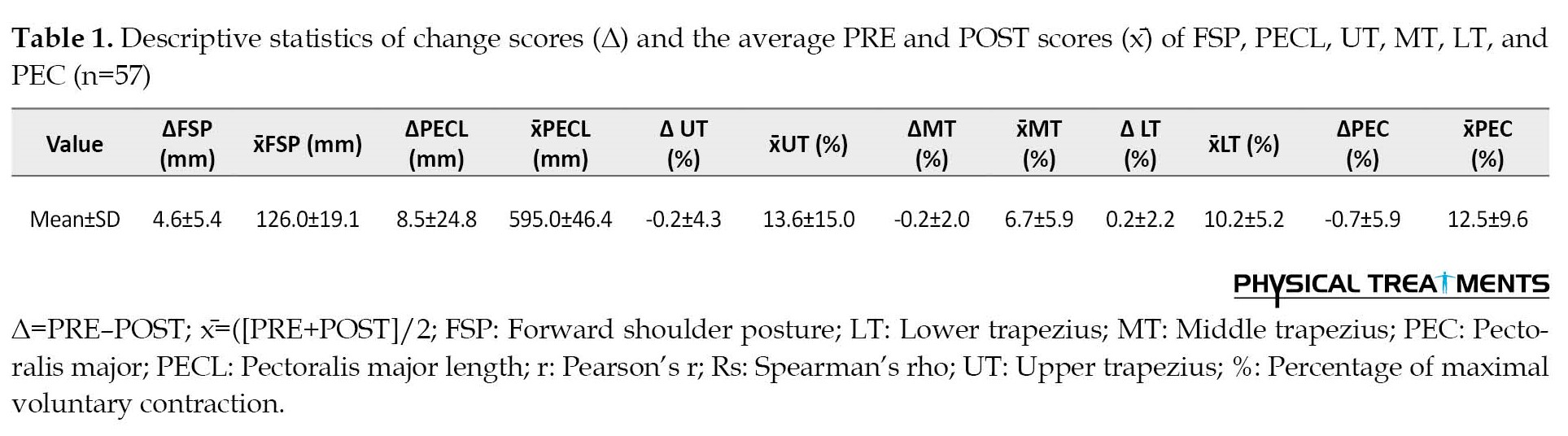
There were no significant correlations between the changes in scores and the average PRE and POST scores for any variable (Table 2).
4. Discussion
The current study determined whether there is a rate-dependent effect on FSP, PECL, and muscle excitation of the upper, middle, and lower trapezius, and pectoralis major following 4 minutes of myofascial release to the pectoral fascia. Contrary to our hypothesis, there was no significant correlation between the variables and, therefore, there was no rate-dependent effect on treatment outcomes, whereby the magnitude and direction of the response after the MFR intervention were influenced by the baseline level of that variable.
Rate dependence is essential to improving our understanding of variability in individual responses when implementing interventions. Several authors support that considering the baseline level of a variable is essential to accurately assess the impact of interventions, design effective strategies to achieve desired outcomes and identify individuals most likely to respond to a particular treatment [2, 3]. While no investigation to date has explored rate dependence following a massage therapy intervention, several reports have indicated substantial variability, as demonstrated by large standard deviations, in participant responses to MFR interventions. For example, variability in head posture [16], head, shoulder, and spine alignment [17], muscle tension [17], shoulder range of motion, and forward scapular position [18]have been demonstrated in response to MFR treatments. Given this large variability, it is surprising that little work has aimed to determine factors affecting some patients experience larger, potentially clinically significant, changes in outcomes following an MFR treatment, while others experience little or no change.
To our knowledge, our results are the first to demonstrate that rate dependence does not influence patient responses to a 4-minute MFR treatment. The results of our previous between-group analyses demonstrated that MFR reduced FSP, but not PECL or excitation of the UT, MT, LT, and PEC [1]. Thus, while 4 minutes of MFR reduced FSP at a group level, the magnitude of change following treatment does not differ if a patient has more (or less) severe FSP. Further, while no group effect was observed in PECL or excitation of the UT, MT, LT, and PEC [1], treatment response was also not impacted by pre-treatment levels of these variables.
Given that there are no known studies that have examined the speed dependence of the response to massage, it is challenging to compare our results with the relevant existing literature. One study exploring the impact of two different stretching interventions reported that baseline flexibility does not affect hip ROM in elite gymnasts [19]. While these results appear to support our observations that baseline PECL (measured via horizontal abduction range of motion) does not affect changes in PECL following the MFR intervention, it is important to note that a systematic evaluation of the impact of baseline flexibility on hip ROM was not performed in this investigation [19]. Instead, the authors concluded that because baseline flexibility differed between the groups at baseline and their responses to the two different interventions differed, this baseline flexibility did not affect the hip range of motion after stretching.
5. Conclusion
There were no rate-dependent effects on FSP, PECL, and muscle activation of the upper, middle, and lower trapezius and pectoralis major after 4 minutes of myofascial release to the pectoral fascia. Thus, patients receiving MFR may experience improvements following treatment that are not dependent on the level of that variable prior to treatment.
Limitations and future directions
There are certain limitations regarding the present study that should be taken into consideration when interpreting our findings. First, it is important to acknowledge that the generalizability of the results is limited to younger individuals with asymptomatic shoulders and FSP. Future work should determine if rate-dependence is present in response to MFR treatments in patients with symptomatic shoulders as it is plausible that this population may have different factors contributing to MFR responsiveness than asymptomatic shoulders. Additionally, it should be noted that the MFR treatments were administered by an experienced RMT who aimed to employ the same intensity of treatment for all participants. However, given that it was not possible to measure the pressure applied by the therapist to each patient, it remains uncertain to what extent the pressure applied during the treatments was consistent across different sessions. Future research should quantify and standardize the applied pressure during various manual treatments. This would enable a more precise evaluation of the effects of different pressure levels on outcomes following MFR and other massage techniques. It is also uncertain whether rate dependence would contribute to individual responses to longer MFR treatments or several treatments over days or weeks. Future research should evaluate rate dependence in response to different doses of MFR treatments.
The potential impact of random sampling on the range of baseline values observed in the study sample must also be considered. Because the sample was chosen randomly, it may not include all possible baseline values needed to see the full range of the inverse rate-dependent relationship. However, it is important to note that a complete inverse relationship is not a prerequisite for the presence of rate dependence.
Furthermore, because muscle excitation data are presented and interpreted as a percentage change relative to MVC, the score cannot be less than zero and the percent cannot be greater than 100, which limits the range of variability available for change to occur.
While our results suggest there is no rate-dependent effect on treatment outcomes following a 4-minute MFR treatment, it is not known whether all types of dependent variables and populations may operate in a rate-dependent manner. Thus, future work should investigate whether other outcome variables and populations respond in a rate-dependent way following MFR treatments.
Ethical Considerations
Compliance with ethical guidelines
Participants of the current study were informed of the purpose of the study, its methods, that their information would remain confidential and that they were free to leave the study whenever they wished, and if desired, the research results would be available to them. All participants signed written informed consent to participate in the present study whose experimental procedures were conducted in compliance with the Declaration of Helsinki. This study was approved by the The University of Manitoba Research Ethics Board (Code: HS22668) and was registered at the US National Library of Medicine (ClinicalTrials.gov database; NCT04944745).
Funding
The work was funded by the Massage Therapy Research Foundation and the Massage Therapy Association of Manitoba (MTAM).
Authors' contributions
Conceptualization, methodology, supervision and Funding acquisition: Sarah Bohunicky and Trisha D Scribbans; Investigation and writing: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to express their sincere gratitude to all participants who generously dedicated their time and effort to participate in this study.
References
Systematic clinical investigations (i.e. randomized controlled trials) aim to establish if patients report outcomes or disease status changes following a given intervention by testing for mean differences in outcomes before and after treatment. If no difference is observed between groups or time points, investigators often conclude that an intervention was ineffective. For example, recently a massage therapy intervention did not alter pectoralis major length (PECL) and muscle excitation in individuals with forward shoulder posture (FSP) due to a lack of difference in group means [1]. However, when our data was examined on an individual basis, a range of responses was present for all variables, where some individuals experienced larger responses and others experienced little or no response (e.g. mean range: -1% (-9 to 10) change in PECL). The heterogeneity in our group data suggests that some individuals experienced substantial, potentially clinically important effects from the massage therapy treatment that were concealed by analyses of the mean values of the groups. While a variety of factors contribute to an individual’s response to an intervention, individual participants’ baseline values are known to influence changes in the same outcome variable post-treatment [2]. Thus, it is plausible that the massage therapy intervention we employed was effective at improving FSP, PECL, and/or muscle excitation for a particular subgroup within our study population.
It is well established that the magnitude and direction of response or change in an outcome variable following an intervention is affected by the baseline level of that variable [2, 3]. This phenomenon, often referred to as rate dependence, has been observed in many investigations and contexts, including drug and non-drug interventions [1]. While many previous reports have correlated pre-intervention to change scores to explore if baseline level impacts individual response [4], the correlation between these variables induces mathematical coupling and regression to the mean [1, 5]. An alternative approach, the Oldham method, determines the rate dependence of treatment effects without mathematical coupling and regression to the mean [6].
Thus, the current study determined whether there is a rate-dependent effect on FSP, PECL (as measured via shoulder horizontal abduction range of motion (ROM)), and muscle excitation of the upper (UT), middle (MT), and lower trapezius (LT), and pectoralis major (PEC) following 4 minutes of myofascial release (MFR) to the pectoral fascia. Given that restricted pectoral soft tissues are associated with FSP [7], which increases scapular protractor excitation [8] and is hypothesized to decrease scapular retractor excitation, therapists often use manual techniques, like MFR to lengthen pectoral soft tissues, reduce FSP, and correct alterations in muscle excitation. Thus, while the results of our preliminary between-group analyses indicated that MFR reduced FSP but did not affect PECL or the excitability of UT, MT, LT, and PEC, it is plausible that there were unobserved rate-dependent effects on these outcomes. For example, those with greater FSP at baseline might have experienced a larger change in FSP, while those with lesser FSP experience a smaller or no change in FSP following MFR. Therefore, we hypothesized that a rate-dependant effect will be observed for all variables examined. The results of this study may identify subpopulations that benefited from the MFR intervention, which will inform the methodological design of future massage therapy research regarding participant demographics and baseline characteristics. Further, to determine the rate-dependent effect on FSP, PECL, and muscle excitation following MFR, the first attempt is to define whether a patient’s baseline characteristics affect individual responses to a massage intervention.
2. Materials and Methods
Research design
A within-subjects, repeated-measures single-blinded crossover study was conducted where participants attended two 1-hour sessions (MFR and control [CON]) in random order (Research Randomizer 4.0, Social Psychology Network, USA). Only data from the MFR session were used. The University of Manitoba Education/ Nursing Research Ethics Board approved all experimental procedures that were conducted in compliance with the Declaration of Helsinki [9]. Informed consent was given by participants following written and verbal details of the experimental procedures.
Before (PRE) and after (POST) the MFR intervention, FSP, PECL, and excitation of the UT, MT, LT, and PEC during a reaching task were measured. A researcher took all measurements on the right side and all treatments were performed by a registered massage therapist (RMT). The current study was a retrospective analysis of data from a previous study exploring the effect of 4 minutes of MFR or soft-touch control treatment on FSP, PECL, and excitation of the UT, MT, LT, and PEC during a reaching task [1].
Participants
Sixty-six individuals were recruited from the University of Manitoba and neighboring communities via convenience sampling. Potential participants were screened for eligibility using the following inclusion criteria: the age of 18-60 years, right-hand dominant cases, no experience of recent (<6 months) pain, injury, or orthopedic disorders to the shoulders, upper back, or neck (e.g. rotator cuff tear and whiplash), and no previous diagnosis of any neurological or musculoskeletal disorders (e.g. muscular dystrophy). A minimum of 1 cm of anterior deviation of the acromion process from the lateral plum line was additionally required for participants to be considered to have FSP [10]. After attrition, 59 participants (27±9 years old, 30 females) were eligible and included in the current analysis. Participants were instructed to abstain from intense physical activity of the upper body for 48 hours leading up to each session.
FSP measurement
The double-square method was used to measure FSP. Participants stood in a relaxed position against a wall where a modified combination square (Swanson Tool Company 12-in Combo Square, Frankfurt, IL, United States) was used to measure the distance from the wall to their anterior acromion [11]. The mean of three measurements was used for analysis, and participants were instructed to step forward and shake their arms in order to reset their posture before returning to the wall for each measurement.
PECL
Since there is no standardized way to measure pectoralis major length, it was found by measuring horizontal abduction ROM (i.e. the pectoral stretch position). Participants laid supine on a plinth and horizontally abducted their right shoulder with their elbow and shoulder flexed at 90°. A meter stick was used to measure the distance between the participant’s olecranon process and the ground. The mean of three separate measurements was used for analysis. Participants horizontally adducted their arms between each measurement to the starting position.
Muscle excitation: Surface electromyography
During a goal-directed reaching task, bipolar surface electromyography (sEMG) was collected from the UT, MT, LT, and sternal fibers of PEC (Figure 1).
Maximal voluntary contractions (MVCs)
Participants performed one familiarization maximal voluntary contraction (MVC), followed by three MVCs for the trapezius, and then the PEC to use as a reference contraction for excitation during the reaching task.
For the trapezius MVC, participants assumed an LT-MVC prone position on a plinth with their shoulder abducted to 120°. Participants were instructed to extend their arms, pulling up on an inextensible handle towards the ceiling. Compared to individual test positions for the UT and MT, the LT MVC position provides the greatest excitation for all three regions of the trapezius and was therefore used for the trapezius MVC. For the PEC MVC, participants attempted to horizontally adduct the handle while lying supine on the plinth with their shoulder abducted at 90° [13]. For all MVCs, a 5-second countdown was provided, and participants were directed to contract as hard as possible for 5 seconds using the targeted muscles. Two minutes of rest were given between each repetition.
Reaching task
Surface electromyography of the UT, MT, LT, and PEC was collected during a reaching task where participants sat at a height-adjustable workstation with a touchscreen monitor (NEC EX241UN-PT-H, Sharp NEC Display Solutions Ltd., USA). The workstation was configured to their height and reach, where the table height allowed their elbows to be flexed to ~80° with their hands flat on the table. The monitor was set at a distance where the elbows were flexed to ~20° degrees to touch the center of the screen. This reaching task aimed to simulate a functional activity that is common in everyday activities and occupational settings, involving tasks, such as computer operation and grasping for small objects.
A custom-written E-Prime program (v3.0 Psychology)
Software Tools Inc., Pittsburgh, PA, United States) was used for the reaching task. Participants reached from a “home” button (a consistent starting position located on the tabletop) to one of five targets displayed on the monitor. Each target appeared as a black square and was presented in a pseudorandomized order. Each target, located in the center or any of the four corners of the monitor, appeared 12 times, for a total of 60 targets per testing block. The reaching task took approximately 4 minutes to complete.
Participants completed a short familiarization block that demonstrated the location of all five targets. The home key, consisting of a microswitch (Submini Snap Action Switch, Philmore Manufacturing, Rockford, USA), was embedded on the table surface in front of the participants. Participants were instructed to press and hold the home button, which triggered a “fixation” screen for a short, random period (2000 to 2500 ms). One of the five targets appeared randomly, and participants released the home button, reached the center of the target, and pressed the center of the target as quickly and accurately as possible using their right arm. Participants returned to the home position once the target was pressed. E-Prime recorded participant reactions and movement times via the microswitch and touchscreen. Only movements to the top-right target position were analyzed to account for the variance in muscle excitation patterns between target locations. To prevent repetitive and anticipated movements, additional target locations were included.
Interventions
Both treatments were administered by an RMT (18 years of experience) with training in MFR to the right pectoral fascia; however, only the MFR treatment was examined for this analysis. In order to maintain consistent placement and reduce impedance between measurements, electrode locations were outlined after the PRE intervention measurements and removed to allow for treatment. Researchers were blinded to the treatment condition and left the laboratory prior to treatment initiation.
Participants lay supine on a plinth with their arms resting by their sides and a bolster under their knees. The intervention given during both sessions was unknown to the participants. The RMT instructed participants to notify them to change the pressure if they felt seven out of ten or more discomfort or a burning sensation; however, no participant reported this.
The MFR intervention lasted 4 minutes, given previous reports that 3.3 minutes of MFR modifies fascial fibrosis [14]. The RMT applied a cross-hand technique to the superficial right pectoral fascia, where one hand (anchoring hand) was placed on the right edge of the sternum (ribs 3-6), and the other hand (mobilizing hand) was placed over the anterior aspect of the humerus at the PEC insertion point. They applied gentle posterior pressure to the anchoring hand to “hold” the fascia in place and moderate posterolateral pressure to the mobilizing hand to take up the slack within the fascial tissue. This allowed for a mechanical stretch of the pectoral fascia without gliding. After 4 minutes, the therapist gradually released any pressure exerted by the mobilizing hand followed by the anchoring hand after each intervention. The PEC electrodes were reapplied to the outline on the participant’s chest. A modified t-shirt was provided to visually conceal the treatment area but could allow access to the electrode wiring.
Surface electromyography data processing
Data processing was performed by a blinded investigator. Also, sEMG signals were recorded and processed using OT BioLab+(v1.3.2, OT Bioelettronica, Torino, Italy). Data were sampled at 2,048 in a bipolar configuration with a gain of 500, band-pass filtered (-3 dB bandwidth, 10-500 Hz), and digitally converted by a 16-bit A/D converter (Quattrocento, OT Bioelettronica, Torino, Italy). Signals were digitally band-pass Butterworth filtered at 30-500 Hz post-collection to remove electrocardiogram contamination from the EMG signal [15]. The root-mean-square (RMS) was calculated for each pair of bipolar electrodes. Data were exported from OT BioLab+ as a .csv file in 0.001 epochs.
Each muscle’s peak excitation was identified, and a one-second period (0.5 s before/after) surrounding the peak was used as a reference. The movement time of each top-right target was used to assess muscle excitation during the reaching task (i.e. release of the microswitch to touch of target), as movement onset for each target was timestamped on the sEMG recording. The mean RMS of the 12 movement times was divided by the respective muscle’s MVC to yield a percentage of excitation for each muscle, which was used for analysis.
Statistical analysis
Statistical analysis was performed using Jamovi 2.3. Normality was assessed using the Shapiro-Wilk test, where p>0.05 indicated that the data were normally distributed. Using the Oldham method [6], correlations were conducted on the difference between PRE and POST values (PRE – POST; Δ) and the sum of PRE and POST values divided by 2 ([PRE+POST]/2; x̄) for each of the following variables: FSP, PECL, and muscle excitation (UT, MT, LT, and PEC). Pearson correlations were conducted on normally distributed data, and Spearman rank correlations were conducted on abnormally distributed data. Statistical significance was accepted at p<0.05, and correlation coefficients (r/rs) were interpreted as low <0.3, moderate 0.3-0.49, and high >0.5.
3. Results
FSP and PECL Data were normally distributed, while UT, MT, LT, and PEC data were not normally distributed (p<0.05); thus, the Pearson’s and Spearman’s Rank correlations were conducted, respectively. Descriptive statistics for all variables are presented in Table 1.
There were no significant correlations between the changes in scores and the average PRE and POST scores for any variable (Table 2).
4. Discussion
The current study determined whether there is a rate-dependent effect on FSP, PECL, and muscle excitation of the upper, middle, and lower trapezius, and pectoralis major following 4 minutes of myofascial release to the pectoral fascia. Contrary to our hypothesis, there was no significant correlation between the variables and, therefore, there was no rate-dependent effect on treatment outcomes, whereby the magnitude and direction of the response after the MFR intervention were influenced by the baseline level of that variable.
Rate dependence is essential to improving our understanding of variability in individual responses when implementing interventions. Several authors support that considering the baseline level of a variable is essential to accurately assess the impact of interventions, design effective strategies to achieve desired outcomes and identify individuals most likely to respond to a particular treatment [2, 3]. While no investigation to date has explored rate dependence following a massage therapy intervention, several reports have indicated substantial variability, as demonstrated by large standard deviations, in participant responses to MFR interventions. For example, variability in head posture [16], head, shoulder, and spine alignment [17], muscle tension [17], shoulder range of motion, and forward scapular position [18]have been demonstrated in response to MFR treatments. Given this large variability, it is surprising that little work has aimed to determine factors affecting some patients experience larger, potentially clinically significant, changes in outcomes following an MFR treatment, while others experience little or no change.
To our knowledge, our results are the first to demonstrate that rate dependence does not influence patient responses to a 4-minute MFR treatment. The results of our previous between-group analyses demonstrated that MFR reduced FSP, but not PECL or excitation of the UT, MT, LT, and PEC [1]. Thus, while 4 minutes of MFR reduced FSP at a group level, the magnitude of change following treatment does not differ if a patient has more (or less) severe FSP. Further, while no group effect was observed in PECL or excitation of the UT, MT, LT, and PEC [1], treatment response was also not impacted by pre-treatment levels of these variables.
Given that there are no known studies that have examined the speed dependence of the response to massage, it is challenging to compare our results with the relevant existing literature. One study exploring the impact of two different stretching interventions reported that baseline flexibility does not affect hip ROM in elite gymnasts [19]. While these results appear to support our observations that baseline PECL (measured via horizontal abduction range of motion) does not affect changes in PECL following the MFR intervention, it is important to note that a systematic evaluation of the impact of baseline flexibility on hip ROM was not performed in this investigation [19]. Instead, the authors concluded that because baseline flexibility differed between the groups at baseline and their responses to the two different interventions differed, this baseline flexibility did not affect the hip range of motion after stretching.
5. Conclusion
There were no rate-dependent effects on FSP, PECL, and muscle activation of the upper, middle, and lower trapezius and pectoralis major after 4 minutes of myofascial release to the pectoral fascia. Thus, patients receiving MFR may experience improvements following treatment that are not dependent on the level of that variable prior to treatment.
Limitations and future directions
There are certain limitations regarding the present study that should be taken into consideration when interpreting our findings. First, it is important to acknowledge that the generalizability of the results is limited to younger individuals with asymptomatic shoulders and FSP. Future work should determine if rate-dependence is present in response to MFR treatments in patients with symptomatic shoulders as it is plausible that this population may have different factors contributing to MFR responsiveness than asymptomatic shoulders. Additionally, it should be noted that the MFR treatments were administered by an experienced RMT who aimed to employ the same intensity of treatment for all participants. However, given that it was not possible to measure the pressure applied by the therapist to each patient, it remains uncertain to what extent the pressure applied during the treatments was consistent across different sessions. Future research should quantify and standardize the applied pressure during various manual treatments. This would enable a more precise evaluation of the effects of different pressure levels on outcomes following MFR and other massage techniques. It is also uncertain whether rate dependence would contribute to individual responses to longer MFR treatments or several treatments over days or weeks. Future research should evaluate rate dependence in response to different doses of MFR treatments.
The potential impact of random sampling on the range of baseline values observed in the study sample must also be considered. Because the sample was chosen randomly, it may not include all possible baseline values needed to see the full range of the inverse rate-dependent relationship. However, it is important to note that a complete inverse relationship is not a prerequisite for the presence of rate dependence.
Furthermore, because muscle excitation data are presented and interpreted as a percentage change relative to MVC, the score cannot be less than zero and the percent cannot be greater than 100, which limits the range of variability available for change to occur.
While our results suggest there is no rate-dependent effect on treatment outcomes following a 4-minute MFR treatment, it is not known whether all types of dependent variables and populations may operate in a rate-dependent manner. Thus, future work should investigate whether other outcome variables and populations respond in a rate-dependent way following MFR treatments.
Ethical Considerations
Compliance with ethical guidelines
Participants of the current study were informed of the purpose of the study, its methods, that their information would remain confidential and that they were free to leave the study whenever they wished, and if desired, the research results would be available to them. All participants signed written informed consent to participate in the present study whose experimental procedures were conducted in compliance with the Declaration of Helsinki. This study was approved by the The University of Manitoba Research Ethics Board (Code: HS22668) and was registered at the US National Library of Medicine (ClinicalTrials.gov database; NCT04944745).
Funding
The work was funded by the Massage Therapy Research Foundation and the Massage Therapy Association of Manitoba (MTAM).
Authors' contributions
Conceptualization, methodology, supervision and Funding acquisition: Sarah Bohunicky and Trisha D Scribbans; Investigation and writing: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to express their sincere gratitude to all participants who generously dedicated their time and effort to participate in this study.
References
- Stegeman D, Hermens H. Standards for surface electromyography: The European project surface EMG for non-invasive assessment of muscles (SENIAM). Enschede: Roessingh Research and Development. 2007; 10:8-12. [Link]
- Snider SE, Quisenberry AJ, Bickel WK. Order in the absence of an effect: Identifying rate-dependent relationships. Behavioural Processes. 2016; 127:18-24. [DOI:10.1016/j.beproc.2016.03.012] [PMID]
- Tu YK, Gilthorpe MS. Revisiting the relation between change and initial value: A review and evaluation. Statistics in Medicine. 2007; 26(2):443-57. [DOI:10.1002/sim.2538] [PMID]
- Bickel WK, Quisenberry AJ, Snider SE. Does impulsivity change rate dependently following stimulant administration? A translational selective review and re-analysis. Psychopharmacology. 2016; 233(1):1-18. [DOI:10.1007/s00213-015-4148-y] [PMID]
- Jin P. Toward a reconceptualization of the law of initial value. Psychological Bulletin. 1992; 111(1):176-84. [DOI:10.1037/0033-2909.111.1.176] [PMID]
- Oldham PD. A note on the analysis of repeated measurements of the same subjects. Journal of Chronic Diseases. 1962; 15:969-977. [DOI:10.1016/0021-9681(62)90116-9] [PMID]
- Lee JH, Cynn HS, Yi CH, Kwon OY, Yoon TL. Predictor variables for forward scapular posture including posterior shoulder tightness. Journal of Bodywork and Movement Therapies. 2015; 19(2):253-60. [DOI:10.1016/j.jbmt.2014.04.010] [PMID]
- Yoo WG. Comparison of shoulder muscles activation for shoulder abduction between forward shoulder posture and asymptomatic persons. Journal of Physical Therapy Science. 2013; 25(7):815-6. [DOI:10.1589/jpts.25.815] [PMID]
- Cook, RJ, Dickens, BM, Fathalla MF. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. In: Cook RJ, Dickens BM, Fathalla MF, editors. Reproductive health and human rights: Integrating Medicine, ethics, and law. Oxford: Oxford University Press; 2003. [DOI:10.1093/acprof:oso/9780199241323.003.0025]
- Roddey TS, Olson SL, Grant SE. The effect of pectoralis muscle stretching on the resting position of the scapula in persons with varying degrees of forward head/rounded shoulder posture. Journal of Manual & Manipulative Therapy. 2002; 10(3):124-8. [DOI:10.1179/106698102790819247]
- Peterson DE, Blankenship KR, Robb JB, Walker MJ, Bryan JM, Stetts DM, etal. Investigation of the validity and reliability of four objective techniques for forward shoulder. Journal of Orthopaedic & Sports Physical Therapy. 1997; 25(1):34-42.[DOI:10.2519/jospt.1997.25.1.34] [PMID]
- No author. Recommendations for sensor locations in shoulder or neck muscles [internet]. [Updated 2019 Oct 29]. Available from: [Link]
- Henderson ZJ, Bohunicky S, Rochon J, Dacanay M, Scribbans TD. Muscle activation in specific regions of the trapezius during modified Kendall Manual Muscle Tests. Journal of Athletic Training. 2021; 56(10):1078-85. [DOI:10.4085/545-20] [PMID]
- Ercole B, Antonio S, Julie Ann D, Stecco C. How much time is required to modify a fascial fibrosis? Journal of Bodywork and Movement Therapies. 2010; 14(4):318-25. [DOI:10.1016/j.jbmt.2010.04.006] [PMID]
- Drake JD, Callaghan JP. Elimination of electrocardiogram contamination from electromyogram signals: An evaluation of currently used removal techniques. Journal of Electromyography and Kinesiology. 2006; 16(2):175-87. [DOI:10.1016/j.jelekin.2005.07.003] [PMID]
- Sharma A, Sharma A, Rizvi M, Kumari S, Sharma P. Comparing the effect of myofascial release and muscle energy technique on craniovertebral angle and headache in tension type headache patients. Journal of Physiotherapy Research. 2022.
- Cardoso R, Meneses RF, Lumini-Oliveira J, Pestana P. Myofascial release effects in teachers’ posture, muscle tension and voice quality: A randomized controlled trial. Journal of Voice. 2021; 37(4):635.e15-27. [DOI:10.1016/j.jvoice.2021.03.029] [PMID]
- Laudner K, Thorson K. Acute effects of pectoralis minor self-mobilization on shoulder motion and posture: a blinded and randomized placebo-controlled study in Asymptomatic Individuals. Journal of Sport Rehabilitation. 2019; 29(4):420-4. [DOI:10.1123/jsr.2018-0220] [PMID]
- Donti O, Tsolakis C, Bogdanis GC. Effects of baseline levels of flexibility and vertical jump ability on performance following different volumes of static stretching and potentiating exercises in elite gymnasts. Journal of Sports Science & Medicine. 2014; 13(1):105-13. [PMID]
Type of Study: Research |
Subject:
General
Received: 2023/10/7 | Accepted: 2023/11/8 | Published: 2023/10/14
Received: 2023/10/7 | Accepted: 2023/11/8 | Published: 2023/10/14
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
