Thu, May 28, 2026
Volume 13, Issue 4 (Autumn 2023)
PTJ 2023, 13(4): 267-278 |
Back to browse issues page


Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Asadpour E, Mohammad Rahimi N, Aminzadeh R. Effectiveness of Functional Training on Respiratory Function and Functional Movements Among Female Bodybuilders. PTJ 2023; 13 (4) :267-278
URL: http://ptj.uswr.ac.ir/article-1-591-en.html
URL: http://ptj.uswr.ac.ir/article-1-591-en.html



1- Department of Sports Sciences, Faculty of Literature and Humanities, Imam Reza International University, Mashhad, Iran.
Keywords: Respiratory function tests, Respiratory muscles, Chest wall, Mobility limitation, Upper extremity
Full-Text [PDF 2565 kb]
(955 Downloads)
| Abstract (HTML) (3037 Views)

Full-Text: (1186 Views)
1. Introduction
Musculoskeletal injuries can reduce performance and strength. Different training schedules have been evolved and carried out to prevent these injuries. A test that can evaluate functional movement is necessary before establishing a training program [1].
Researchers have been using movement evaluations that involve comprehensive movement patterns to predict injury. Plisky et al. hypothesized that tests evaluating multiple territories of function simultaneously may enhance the precision of recognizing athletes at risk for injury through pre-participation assessment [2].
The functional movement screen (FMS) is a form to analyze functional movement with seven items: Deep squat, hurdle-step, in-line lunge, shoulder mobility, active straight leg raise, trunk stability push-up, and rotary stability. Each item is ranked on a three-point scale ranging from zero (pain during the action) to three (action performed correctly) [1, 3, 4].
Athletes whose total FMS scores are less than 14 are more prone to injury [3]. A total score of less than 14 indicates a greater risk of injury than a score of ≥14 [5]. FMS can help identify potential injury risks for an athlete [6].
Also, training exercise interventions based on functional movements can enhance the FMS score or reduce the chance of injury [6, 7, 8]. Emphasizing the optimum performance pyramid, adequate functional movement can provide a full range of motion and power efficiency [7]. Stability and mobility, which can be assessed by FMS, are the basis of and related to muscle strength and flexibility [1]. This suggests that the FMS may donate to enhancing muscle strength and flexibility, but this has not been studied directly. Rather, the main subject of study has been injury prognosis or confirmation of reliability and reality [3].
Chest mobility (the difference between full inhalation and exhalation excursion) and respiratory function (tests of the respiratory rate (RR), inspiratory breath-hold time (IBHT), and expiratory breath-hold time (EBHT) in a standing position) are important in predicting athletes’ performance and preventing their injuries. Studies have shown the effect of increasing chest mobility and respiratory function on improving people’s performance [9, 10, 11]. Bodybuilding exercises are based on science that strengthens and develops body systems by activating appropriate predetermined work programs with special tools and machines. Due to the expansion of bodybuilding, we observe daily reports of sports-related injuries. In the past decades, risk factors, such as lack of neuromuscular control, instability in the core region, previous injuries, incorrect movement patterns, and movement asymmetry in the body due to changes in joint movements and movements and reduced function of respiratory organs, have been introduced as risk factors of this sport [5, 12]. So far, no research has been done on the relationship between functional exercises and improvement in FMS test scores, chest mobility, respiratory function, and quality of functional movements among female bodybuilders in reducing the likelihood of sports injury. Considering the spread of this sport among women and the high probability of their injury, as well as the high costs of treatment and disability during the recovery period, this study investigated the effectiveness of six weeks of functional training in chest mobility, respiratory function, and the quality of functional movements in female bodybuilders.
2. Materials and Methods
This semi-experimental and applied study was conducted on female bodybuilders aged 19-39 years at the Titan Gym in Mashhad. At baseline, the participants were informed about the details of the study, and a consent form was obtained from them. They also had the right to leave the research.
We estimated the sample size based on power analysis for the repeated-measures analysis of variance using G*Power software, version 3.1.9.2, a power of 0.80, a moderate effect size of 0.50, and a significance level of 5% (2-tailed). We utilized a group allocation ratio of 1:1. Therefore, 40 participants (20 in each group) were required.
Following the completion of all initial assessments, the participants were randomized to the functional training group (n=20) or the control group (n=20) via random number generation. Both groups were equal in number and homogenized as much as possible in height, weight, and age. The inclusion criteria were performing at least four months of regular exercise experience, no use of medication, no specific cardiovascular or orthopedic diseases, and no pregnancy. Furthermore, volunteers had no special pre-existing injuries affecting the research process. Exclusion criteria included smoking and drug use, any injury, announcement of pregnancy by the participant, and absence of more than three training sessions. First, measurement of chest mobility, respiratory function, FMS, and closed kinetic chain upper extremity stability test (CKCUEST) was done, then the functional exercise group performed the functional exercises three times per week for six weeks along with their routine exercises and the control group participated in the routine program during the same period. The participants did their bodybuilding exercises and after finishing the program, the test was taken again.
Chest mobility
The mobility of the chest (the difference between completed inhalation and exhalation) was evaluated in the standing position. A 150 cm measuring tape was utilized to measure the circumference of the rib cage at two different levels: 1) The axillary line for upper chest mobility (UCM) (the horizontal line of the spinous process of the fifth thoracic vertebrae and the third intercostal space (axillary line) at the mid-clavicular line); 2) lower chest mobility (LCM) facilitated by the horizontal line of the spinous process of the tenth thoracic vertebrae and the tip of the xiphoid process.
The difference between completed inspiration and expiration (holding breath for at least 2 seconds) was calculated for all three measured circumferences [8]. The intra-rater has a high level of reliability for both upper and lower chest expansion. It is 0.90 to 0.93 for upper CE and 0.85 to 0.86 for lower chest expansion [13].
Respiratory function tests
Breathing performance was examined using RR, IBHT, and EBHT in a standing position. The examiner stood in front of the subject and the number of breaths was recorded by counting the movements of the shoulders, chest, and abdomen of the subject in one minute [14]. Also, for IBHT EBHT assessments, the subject was requested to take a deep breath and hold the breath, and the duration of the subject’s breath-holding was recorded using a stopwatch in seconds. Then, the amount of breath holding after deep exhalation was also measured [9]. This test has a test re-test reliability of 0.91 [15, 16].
FMS test
The full FMS protocol, which includes seven different movement patterns, was applied to evaluate participants by developed methods. These movement patterns consisted of deep squat, hurdle step, in-line lunge, shoulder mobility, active straight-leg raise, trunk stability push-up, and rotary stability. Cook et al. provided complete descriptions of each test and scoring techniques [1]. The participants obtained detailed explanations of each movement pattern in a standard method from the assessor. Three trials of each movement were performed by participants, and the rater considered the best performance for analysis. The capability to execute the movement pattern was controlled by the assessor, who individually rated the task performance on a four-point scale (0-3), and documented the highest score from three trials. Participants were asked to repeat the movement pattern if there was a mismatch at each tested score [8, 19].
Score 3: Performing the movement correctly and completely.
Score 2: Performing the movement incompletely and doing it with help or when loss of body balance is observed.
Score 1: Inability to move.
Score 0: The person feels pain in any part of the movement or the pain detection tests are positive.
The maximum score on this test is 21, and researchers have predicted that athletes who score less than 14 are more likely to be injured [20]. The intra-rater reliability of this test is reported to be 95% [21] (Appendix 1).

CKCUEST test
This test examines muscle strength and endurance and the stability of the closed kinetic chain of the upper limbs. It was developed by Davies and Dickoff Hoffman (1993), in which two pieces of sports band are placed 90 cm apart, and the subjects are requested to take a swimming position and cross their arms in 15 seconds. The number of touches is the person’s score [2].
The results of previous research indicated that CKCUEST is a reliable evaluation tool. The intra-rater reliability of this test is reported to be 92% [15] (Appendix 2).

Functional training program (intervention)
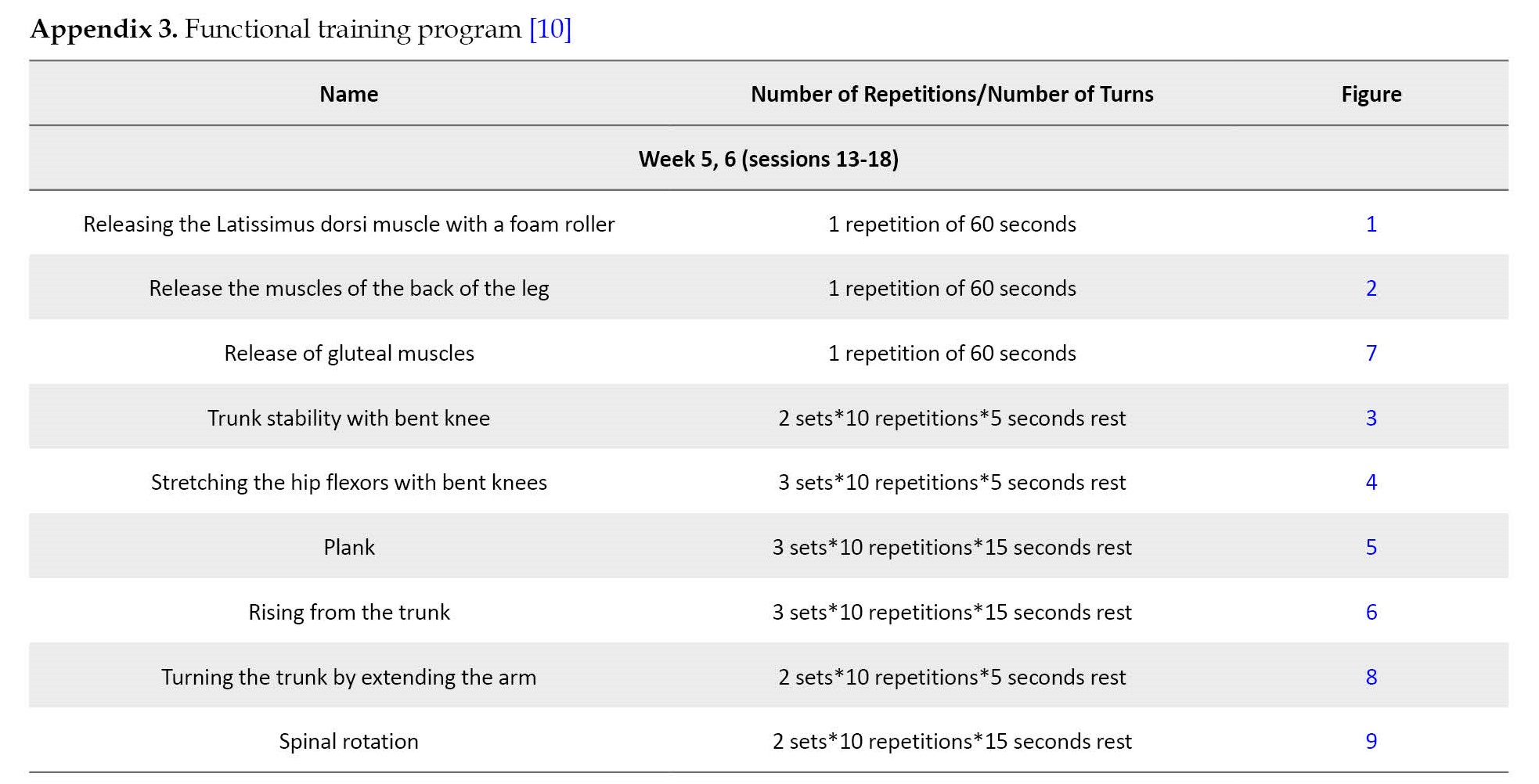
The exercises were done for six weeks, three sessions per week for 30 minutes. The exercises were designed to strengthen the stability and central muscles of the body, stretch muscles that are likely to be overused and increase mobility of the thoracic spine.
The program includes nine exercises. In the first two weeks, only six exercises (release of the Latissimus dorsi muscle with a foam roller, release of the muscles of the back of the leg, trunk stability with bent knee, stretching the hip flexors with bent knees, plank, and rising from the trunk) were presented. In the second two weeks, another exercise (release of gluteal muscles) was added. In the third two weeks, a new exercise was presented (turning the trunk by extending the arm, and spinal rotation). At the beginning of each session, 5 minutes of warm-up and 5 minutes of cool-down were considered at the end of each session. The exercises were done for six weeks, three sessions per week for 30 minutes. Due to the importance of correct execution of these exercises, they were taught by an experienced trainer [20]. The exercises were taken from the following site with more than 500 functional exercises [21] (Appendix 3).
Statistical analysis
Data were analyzed using repeated-measures analysis of variance (RM-ANOVA) by Statistical Package for the Social Sciences (SPSS software, version 23, Inc., Chicago, Illinois). A p<0.05 was considered statistically significant.
3. Results
The participants of the functional exercise and control groups conducted the 6-week program. Table 1 presents the mean age, weight, height, and BMI of the functional training and control groups.

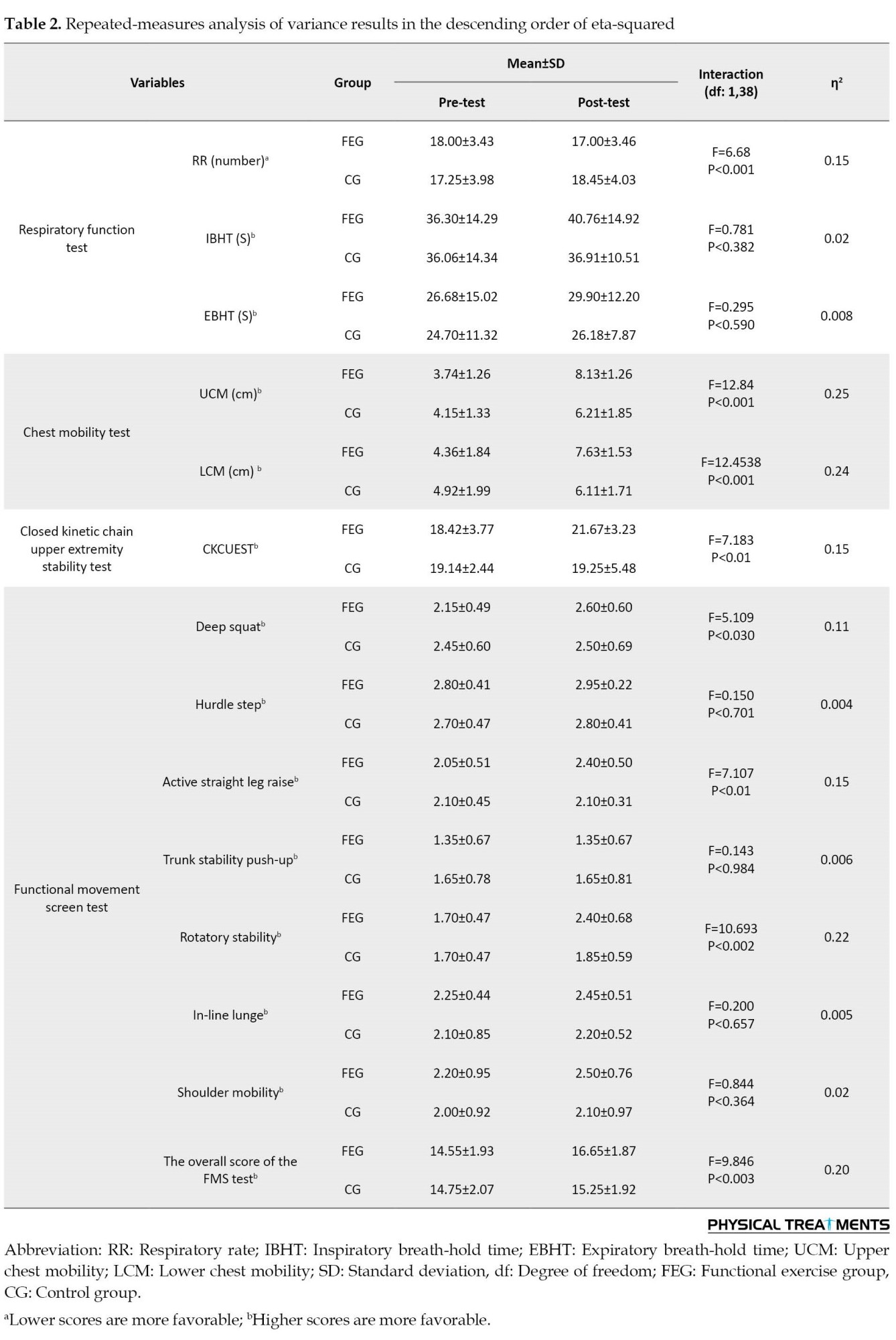
According to Table 2, the analysis of chest mobility, physical performance, and the quality of functional movements of the functional exercise group before and after six weeks of exercises showed no significant difference in RR, IBHT, and EBHT, but chest mobility (UCM and LCM), CKCUEST, and the overall score of FMS showed a statistically significant difference in the functional exercise group.
4. Discussion
The results of this study showed that as a non-invasive method, six weeks of selected functional training can cause statistically significant improvement in UCM, LCM, RR, CKCUEST, and FMS test scores.
The improvement in the mobility of the chest can be due to the inclusion of exercises for the balanced mobility and stability of the thoracic spine and compliance with the principle of inhaling and exhaling the diaphragm in the exercise program.
Csepregi et al. (2022) investigated the effectiveness of classical breathing training on posture, spinal, and chest mobility among female university students compared to traditional exercise programs. They indicated that breathing exercises may be an adequate intervention to improve posture, flexibility, and strength. In conclusion, mobility balance and stability of intervertebral joints in healthy young adults were achieved by breathing exercises in most cases evaluated [22].
The clinical test outcomes evaluated at baseline and after the interventions. To avoid influencing the results and have reliable results, homogenous female groups were evaluated and compared to each other in our study due to the difference between genders in strength and flexibility.
Moreover, Ghavipanje et al. (2020) investigated the impact of six weeks effects of dynamic neuromuscular stabilization training on various spirometry metrics in inactive, hunched-over students. There was an improvement in the measured factors after performing the designed exercises [16].
Our results regarding chest wall mobility are in line with the research by Csepregi (2022) and Mohammad Rahimi (2020), which can be due to the emphasis on correct breathing during the exercises.
The results indicated no significant difference in respiration rate in the functional exercises group, but it increased significantly in the control group. A possible reason for the lack of improvement in breathing in the functional exercises group is the lack of exercises designed specifically for respiratory muscles. The reason for the increase in the respiration rate in the control group can be strength exercises without strengthening the respiratory system.
Finally, IBHT and EBHT did not change significantly, which can be attributed to the lack of aerobic capacity in bodybuilders and no aerobic exercises in the selected exercises of this research.
Madanmohan et al. (1992) investigated the effectiveness of yoga exercises in reaction time, respiratory endurance, and muscle strength and showed an improvement in the measured items after performing the designed exercises [9].
In this context, our results are not consistent with the results of Madanmohan (1992). The possible reason for this difference is no specific exercises designed to strengthen the deep muscles in the training protocol.
In addition, the current research showed a significant improvement in the results of the CKCUEST. Considering that the CKCUEST is designed to evaluate the performance and stability of the upper limbs, and the results of the present research showed a significant improvement after the designed exercise protocol, it can be concluded that the possible reason for this success was focusing on the stability and core muscles of the body while designing the exercises.
Laurinavičiūtė et al. (2021) investigated the effect of a neuromuscular exercise intervention program on the functional aspects of the upper extremity in handball and basketball athletes. They indicated an improvement in the measured factors after performing the exercises designed [23].
Strutt et al. (2018) studied the effect of a four-week upper-extremity exercise program on a balance device improves power and stability in collegiate golfers and demonstrated that specific upper-extremity exercises on a balance device improved upper-extremity power, upper-extremity stability, and over-head shoulder flexibility within four weeks [24].
The results of the current research are consistent with those of Laurinavičiūtė et al. (2021) and Strutt et al (2018) [23, 24]. The reason for this consistency can be the design of stability exercises in this research.
Also, our research indicated considerable progress in the final result of the FMS test, which can be attributed to exclusive exercises to strengthen the stability and central muscles of the body, stretching exercises to stretch the muscles that are likely to be overused, and the mobility of the thoracic spine. Additionally, myofascial release exercises are beneficial for muscles that are usually overused.
Usluer et al. (2021) investigated the effect of corrective training on the FMS test results and motor skills. They indicated considerable progress in the FMS test results after the exercise protocol [25].
Guler et al. (2021) investigated the effectiveness of functional strength exercises in functional movement and balance in middle-aged people. Functional strength training improved middle-aged persons’ balance ability and the overall FMS test score [26].
Sawczyn (2020) studied the effectiveness of a periodic functional strength exercise (FST) on the FMS test results in sports science students and 45% of the subjects in the first FMS testing indicated a total score of 14. The experimental group performing the functional strength exercise showed a significant change in FMS total scores after 12 weeks. Also, there were considerable differences in FMS total scores between the groups after the study [27].
Our results are in line with the research by Usluer et al. (2021), Guler et al. (2021), and Sawczyn (2020) [25-27]. The possible reason for this alignment can be attributed to the special attention given to the body’s chain reactions in the exercises designed in the researc-h. As a final result, it can be stated that the selected functional training can have a positive influence on chest mobility, CKCUEST, and the overall score of the FMS.
5. Conclusion
Functional training can improve the breathing performance of athletes, chest mobility, FMS test results, and CKCUEST results. It can be concluded that the inclusion of functional exercises in the training program of athletes is effective in preventing and improving their sports performance. Consequently, exercise protocols, such as those used in the present study, are suggested to strengthen the respiratory system and central muscles.
Study limitations
Although the sample size and age range of participants were small, the study had sufficient statistical capability to identify distinctions. Therefore, additional investigations are needed to consider the effectiveness of functional training over a lengthy duration and on other age groups.
Ethical Considerations
Compliance with ethical guidelines
The Research Ethics Committee of the Faculty of Physical Education and Sports Science of Imam Reza International University approved this study (Code: IR.IMAMREZA.REC.1401.012).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Supervision: Nasser Mohammad Rahimi and Reza Aminzadeh; Data collection and investigation: Ensieh Asadpour; Data analysis, writing, review, and editing: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors thank all patients for participating in this clinical trial.
References

Musculoskeletal injuries can reduce performance and strength. Different training schedules have been evolved and carried out to prevent these injuries. A test that can evaluate functional movement is necessary before establishing a training program [1].
Researchers have been using movement evaluations that involve comprehensive movement patterns to predict injury. Plisky et al. hypothesized that tests evaluating multiple territories of function simultaneously may enhance the precision of recognizing athletes at risk for injury through pre-participation assessment [2].
The functional movement screen (FMS) is a form to analyze functional movement with seven items: Deep squat, hurdle-step, in-line lunge, shoulder mobility, active straight leg raise, trunk stability push-up, and rotary stability. Each item is ranked on a three-point scale ranging from zero (pain during the action) to three (action performed correctly) [1, 3, 4].
Athletes whose total FMS scores are less than 14 are more prone to injury [3]. A total score of less than 14 indicates a greater risk of injury than a score of ≥14 [5]. FMS can help identify potential injury risks for an athlete [6].
Also, training exercise interventions based on functional movements can enhance the FMS score or reduce the chance of injury [6, 7, 8]. Emphasizing the optimum performance pyramid, adequate functional movement can provide a full range of motion and power efficiency [7]. Stability and mobility, which can be assessed by FMS, are the basis of and related to muscle strength and flexibility [1]. This suggests that the FMS may donate to enhancing muscle strength and flexibility, but this has not been studied directly. Rather, the main subject of study has been injury prognosis or confirmation of reliability and reality [3].
Chest mobility (the difference between full inhalation and exhalation excursion) and respiratory function (tests of the respiratory rate (RR), inspiratory breath-hold time (IBHT), and expiratory breath-hold time (EBHT) in a standing position) are important in predicting athletes’ performance and preventing their injuries. Studies have shown the effect of increasing chest mobility and respiratory function on improving people’s performance [9, 10, 11]. Bodybuilding exercises are based on science that strengthens and develops body systems by activating appropriate predetermined work programs with special tools and machines. Due to the expansion of bodybuilding, we observe daily reports of sports-related injuries. In the past decades, risk factors, such as lack of neuromuscular control, instability in the core region, previous injuries, incorrect movement patterns, and movement asymmetry in the body due to changes in joint movements and movements and reduced function of respiratory organs, have been introduced as risk factors of this sport [5, 12]. So far, no research has been done on the relationship between functional exercises and improvement in FMS test scores, chest mobility, respiratory function, and quality of functional movements among female bodybuilders in reducing the likelihood of sports injury. Considering the spread of this sport among women and the high probability of their injury, as well as the high costs of treatment and disability during the recovery period, this study investigated the effectiveness of six weeks of functional training in chest mobility, respiratory function, and the quality of functional movements in female bodybuilders.
2. Materials and Methods
This semi-experimental and applied study was conducted on female bodybuilders aged 19-39 years at the Titan Gym in Mashhad. At baseline, the participants were informed about the details of the study, and a consent form was obtained from them. They also had the right to leave the research.
We estimated the sample size based on power analysis for the repeated-measures analysis of variance using G*Power software, version 3.1.9.2, a power of 0.80, a moderate effect size of 0.50, and a significance level of 5% (2-tailed). We utilized a group allocation ratio of 1:1. Therefore, 40 participants (20 in each group) were required.
Following the completion of all initial assessments, the participants were randomized to the functional training group (n=20) or the control group (n=20) via random number generation. Both groups were equal in number and homogenized as much as possible in height, weight, and age. The inclusion criteria were performing at least four months of regular exercise experience, no use of medication, no specific cardiovascular or orthopedic diseases, and no pregnancy. Furthermore, volunteers had no special pre-existing injuries affecting the research process. Exclusion criteria included smoking and drug use, any injury, announcement of pregnancy by the participant, and absence of more than three training sessions. First, measurement of chest mobility, respiratory function, FMS, and closed kinetic chain upper extremity stability test (CKCUEST) was done, then the functional exercise group performed the functional exercises three times per week for six weeks along with their routine exercises and the control group participated in the routine program during the same period. The participants did their bodybuilding exercises and after finishing the program, the test was taken again.
Chest mobility
The mobility of the chest (the difference between completed inhalation and exhalation) was evaluated in the standing position. A 150 cm measuring tape was utilized to measure the circumference of the rib cage at two different levels: 1) The axillary line for upper chest mobility (UCM) (the horizontal line of the spinous process of the fifth thoracic vertebrae and the third intercostal space (axillary line) at the mid-clavicular line); 2) lower chest mobility (LCM) facilitated by the horizontal line of the spinous process of the tenth thoracic vertebrae and the tip of the xiphoid process.
The difference between completed inspiration and expiration (holding breath for at least 2 seconds) was calculated for all three measured circumferences [8]. The intra-rater has a high level of reliability for both upper and lower chest expansion. It is 0.90 to 0.93 for upper CE and 0.85 to 0.86 for lower chest expansion [13].
Respiratory function tests
Breathing performance was examined using RR, IBHT, and EBHT in a standing position. The examiner stood in front of the subject and the number of breaths was recorded by counting the movements of the shoulders, chest, and abdomen of the subject in one minute [14]. Also, for IBHT EBHT assessments, the subject was requested to take a deep breath and hold the breath, and the duration of the subject’s breath-holding was recorded using a stopwatch in seconds. Then, the amount of breath holding after deep exhalation was also measured [9]. This test has a test re-test reliability of 0.91 [15, 16].
FMS test
The full FMS protocol, which includes seven different movement patterns, was applied to evaluate participants by developed methods. These movement patterns consisted of deep squat, hurdle step, in-line lunge, shoulder mobility, active straight-leg raise, trunk stability push-up, and rotary stability. Cook et al. provided complete descriptions of each test and scoring techniques [1]. The participants obtained detailed explanations of each movement pattern in a standard method from the assessor. Three trials of each movement were performed by participants, and the rater considered the best performance for analysis. The capability to execute the movement pattern was controlled by the assessor, who individually rated the task performance on a four-point scale (0-3), and documented the highest score from three trials. Participants were asked to repeat the movement pattern if there was a mismatch at each tested score [8, 19].
Score 3: Performing the movement correctly and completely.
Score 2: Performing the movement incompletely and doing it with help or when loss of body balance is observed.
Score 1: Inability to move.
Score 0: The person feels pain in any part of the movement or the pain detection tests are positive.
The maximum score on this test is 21, and researchers have predicted that athletes who score less than 14 are more likely to be injured [20]. The intra-rater reliability of this test is reported to be 95% [21] (Appendix 1).
CKCUEST test
This test examines muscle strength and endurance and the stability of the closed kinetic chain of the upper limbs. It was developed by Davies and Dickoff Hoffman (1993), in which two pieces of sports band are placed 90 cm apart, and the subjects are requested to take a swimming position and cross their arms in 15 seconds. The number of touches is the person’s score [2].
The results of previous research indicated that CKCUEST is a reliable evaluation tool. The intra-rater reliability of this test is reported to be 92% [15] (Appendix 2).
Functional training program (intervention)
The exercises were done for six weeks, three sessions per week for 30 minutes. The exercises were designed to strengthen the stability and central muscles of the body, stretch muscles that are likely to be overused and increase mobility of the thoracic spine.
The program includes nine exercises. In the first two weeks, only six exercises (release of the Latissimus dorsi muscle with a foam roller, release of the muscles of the back of the leg, trunk stability with bent knee, stretching the hip flexors with bent knees, plank, and rising from the trunk) were presented. In the second two weeks, another exercise (release of gluteal muscles) was added. In the third two weeks, a new exercise was presented (turning the trunk by extending the arm, and spinal rotation). At the beginning of each session, 5 minutes of warm-up and 5 minutes of cool-down were considered at the end of each session. The exercises were done for six weeks, three sessions per week for 30 minutes. Due to the importance of correct execution of these exercises, they were taught by an experienced trainer [20]. The exercises were taken from the following site with more than 500 functional exercises [21] (Appendix 3).
Statistical analysis
Data were analyzed using repeated-measures analysis of variance (RM-ANOVA) by Statistical Package for the Social Sciences (SPSS software, version 23, Inc., Chicago, Illinois). A p<0.05 was considered statistically significant.
3. Results
The participants of the functional exercise and control groups conducted the 6-week program. Table 1 presents the mean age, weight, height, and BMI of the functional training and control groups.
According to Table 2, the analysis of chest mobility, physical performance, and the quality of functional movements of the functional exercise group before and after six weeks of exercises showed no significant difference in RR, IBHT, and EBHT, but chest mobility (UCM and LCM), CKCUEST, and the overall score of FMS showed a statistically significant difference in the functional exercise group.
4. Discussion
The results of this study showed that as a non-invasive method, six weeks of selected functional training can cause statistically significant improvement in UCM, LCM, RR, CKCUEST, and FMS test scores.
The improvement in the mobility of the chest can be due to the inclusion of exercises for the balanced mobility and stability of the thoracic spine and compliance with the principle of inhaling and exhaling the diaphragm in the exercise program.
Csepregi et al. (2022) investigated the effectiveness of classical breathing training on posture, spinal, and chest mobility among female university students compared to traditional exercise programs. They indicated that breathing exercises may be an adequate intervention to improve posture, flexibility, and strength. In conclusion, mobility balance and stability of intervertebral joints in healthy young adults were achieved by breathing exercises in most cases evaluated [22].
The clinical test outcomes evaluated at baseline and after the interventions. To avoid influencing the results and have reliable results, homogenous female groups were evaluated and compared to each other in our study due to the difference between genders in strength and flexibility.
Moreover, Ghavipanje et al. (2020) investigated the impact of six weeks effects of dynamic neuromuscular stabilization training on various spirometry metrics in inactive, hunched-over students. There was an improvement in the measured factors after performing the designed exercises [16].
Our results regarding chest wall mobility are in line with the research by Csepregi (2022) and Mohammad Rahimi (2020), which can be due to the emphasis on correct breathing during the exercises.
The results indicated no significant difference in respiration rate in the functional exercises group, but it increased significantly in the control group. A possible reason for the lack of improvement in breathing in the functional exercises group is the lack of exercises designed specifically for respiratory muscles. The reason for the increase in the respiration rate in the control group can be strength exercises without strengthening the respiratory system.
Finally, IBHT and EBHT did not change significantly, which can be attributed to the lack of aerobic capacity in bodybuilders and no aerobic exercises in the selected exercises of this research.
Madanmohan et al. (1992) investigated the effectiveness of yoga exercises in reaction time, respiratory endurance, and muscle strength and showed an improvement in the measured items after performing the designed exercises [9].
In this context, our results are not consistent with the results of Madanmohan (1992). The possible reason for this difference is no specific exercises designed to strengthen the deep muscles in the training protocol.
In addition, the current research showed a significant improvement in the results of the CKCUEST. Considering that the CKCUEST is designed to evaluate the performance and stability of the upper limbs, and the results of the present research showed a significant improvement after the designed exercise protocol, it can be concluded that the possible reason for this success was focusing on the stability and core muscles of the body while designing the exercises.
Laurinavičiūtė et al. (2021) investigated the effect of a neuromuscular exercise intervention program on the functional aspects of the upper extremity in handball and basketball athletes. They indicated an improvement in the measured factors after performing the exercises designed [23].
Strutt et al. (2018) studied the effect of a four-week upper-extremity exercise program on a balance device improves power and stability in collegiate golfers and demonstrated that specific upper-extremity exercises on a balance device improved upper-extremity power, upper-extremity stability, and over-head shoulder flexibility within four weeks [24].
The results of the current research are consistent with those of Laurinavičiūtė et al. (2021) and Strutt et al (2018) [23, 24]. The reason for this consistency can be the design of stability exercises in this research.
Also, our research indicated considerable progress in the final result of the FMS test, which can be attributed to exclusive exercises to strengthen the stability and central muscles of the body, stretching exercises to stretch the muscles that are likely to be overused, and the mobility of the thoracic spine. Additionally, myofascial release exercises are beneficial for muscles that are usually overused.
Usluer et al. (2021) investigated the effect of corrective training on the FMS test results and motor skills. They indicated considerable progress in the FMS test results after the exercise protocol [25].
Guler et al. (2021) investigated the effectiveness of functional strength exercises in functional movement and balance in middle-aged people. Functional strength training improved middle-aged persons’ balance ability and the overall FMS test score [26].
Sawczyn (2020) studied the effectiveness of a periodic functional strength exercise (FST) on the FMS test results in sports science students and 45% of the subjects in the first FMS testing indicated a total score of 14. The experimental group performing the functional strength exercise showed a significant change in FMS total scores after 12 weeks. Also, there were considerable differences in FMS total scores between the groups after the study [27].
Our results are in line with the research by Usluer et al. (2021), Guler et al. (2021), and Sawczyn (2020) [25-27]. The possible reason for this alignment can be attributed to the special attention given to the body’s chain reactions in the exercises designed in the researc-h. As a final result, it can be stated that the selected functional training can have a positive influence on chest mobility, CKCUEST, and the overall score of the FMS.
5. Conclusion
Functional training can improve the breathing performance of athletes, chest mobility, FMS test results, and CKCUEST results. It can be concluded that the inclusion of functional exercises in the training program of athletes is effective in preventing and improving their sports performance. Consequently, exercise protocols, such as those used in the present study, are suggested to strengthen the respiratory system and central muscles.
Study limitations
Although the sample size and age range of participants were small, the study had sufficient statistical capability to identify distinctions. Therefore, additional investigations are needed to consider the effectiveness of functional training over a lengthy duration and on other age groups.
Ethical Considerations
Compliance with ethical guidelines
The Research Ethics Committee of the Faculty of Physical Education and Sports Science of Imam Reza International University approved this study (Code: IR.IMAMREZA.REC.1401.012).
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Supervision: Nasser Mohammad Rahimi and Reza Aminzadeh; Data collection and investigation: Ensieh Asadpour; Data analysis, writing, review, and editing: All authors.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors thank all patients for participating in this clinical trial.
References
- Cook G, Burton L, Hoogenboom B. Pre-participation screening: The use of fundamental movements as an assessment of function - part 1. North American Journal of Sports Physical Therapy: NAJSPT. 2006a;1(2):62-72. [PMID]
- Plisky PJ, Rauh MJ, Kaminski TW, Underwood FB. Star excursion balance test as a predictor of lower extremity injury in high school basketball players. The Journal of Orthopaedic and Sports Physical Therapy. 2006; 36(12):911-9. [PMID]
- Kiesel K, Plisky PJ, Voight ML. Can serious injury in professional football be predicted by a preseason functionalmovementscreen? North American Journal of Sports Physical Therapy : NAJSPT. 2007; 2(3):147-58. [PMID]
- Minick KI, Kiesel KB, Burton L, Taylor A, Plisky P, Butler RJ. Interrater reliability of the functional movement screen. Journal of Strength and Conditioning Research. 2010; 24(2):479-86. [DOI:10.1519/JSC.0b013e3181c09c04] [PMID]
- Chorba RS, Chorba DJ, Bouillon LE, Overmyer CA, Landis JA. Use of a functional movement screening tool to determine injury risk in female collegiate athletes. North American Journal of Sports Physical Therapy: NAJSPT. 2010; 5(2):47-54. [PMID]
- Kiesel K, Plisky P, Butler R. Functional movement test scores improve following a standardized off-season intervention program in professional football players. Scandinavian Journal of Medicine & Science in Sports. 2011; 21(2):287-92. [DOI:10.1111/j.1600-0838.2009.01038.x] [PMID]
- Cook G. Athletic body in balance. Champaign: Human Kinetics; 2003. [Link]
- Peate WF, Bates G, Lunda K, Francis S, Bellamy K. Core strength: A new model for injury prediction and prevention. Journal of Occupational Medicine and Toxicology. 2007; 2:3. [DOI:10.1186/1745-6673-2-3] [PMID]
- Madanmohan, Thombre DP, Balakumar B, Nambinarayanan TK, Thakur S, Krishnamurthy N, et al. Effect of yoga training on reaction time, respiratory endurance and muscle strength. Indian Journal of Physiology and Pharmacology, 1992; 36(4):229-33. [PMID]
- Kim CB, Yang JM, Choi JD. The effects of chest expansion resistance exercise on chest expansion and maximal respiratory pressure in elderly with inspiratory muscle weakness. Journal of Physical Therapy Science. 2015; 27(4):1121-4. [DOI:10.1589/jpts.27.1121] [PMID]
- Kiesel K, Rhodes T, Mueller J, Waninger A, Butler R. Development of a screening protocol to identify individuals with dysfunctional breathing. International Journal of Sports Physical Therapy. 2017; 12(5):774-86. [PMID]
- Minthorn LM, Fayson SD, Stobierski LM, Welch CE, Anderson BE. The functional movement screen’s ability to detect changes in movement patterns after a training intervention. Journal of Sport Rehabilitation. 2015; 24(3):322-6. [DOI:10.1123/jsr.2013-0146] [PMID]
- Reddy RS, Alahmari KA, Silvian PS, Ahmad IA, Kakarparthi VN, Rengaramanujam K. Reliability of chest wall mobility and its correlation with lung functions in healthy nonsmokers, healthy smokers, and patients with COPD. Canadian Respiratory Journal. 2019; 2019:5175949.[DOI:10.1155/2019/5175949] [PMID]
- Pinto RS, Correa CS, Radaelli R, Cadore EL, Brown LE, Bottaro M. Short-term strength training improves muscle quality and functional capacity of elderly women. Age. 2014; 36: 36(1):365-72. [DOI:10.1007/s11357-013-9567-2] [PMID]
- Hoffmann B, Flatt AA, Silva LEV, Młyńczak M, Baranowski R, Dziedzic E, et al. A pilot study of the reliability and agreement of heart rate, respiratory rate and short-term heart rate variability in elite modern pentathlon athletes. Diagnostics. 2020; 10(10):833. [DOI:10.3390/diagnostics10100833] [PMID]
- Ghavipanje V, Rahimi NM, Akhlaghi F. Six weeks effects of dynamic neuromuscular stabilization (DNS) training in obese postpartum women with low back pain: A randomized controlled trial. Biological Research for Nursing. 2022; 24(1):106-14. [DOI:10.1177/10998004211044828] [PMID]
- Zhao R, Zhao M, Xu Z. The effects of differing resistance training modes on the preservation of bone mineral density in postmenopausal women: A meta-analysis. Osteoporosis International. 2015; 26(5):1605-18. [DOI:10.1007/s00198-015-3034-0] [PMID]
- Paoli A, Gentil P, Moro T, Marcolin G, Bianco A. Resistance training with single vs. multi-joint exercises at equal total load volume: Effects on body composition, cardiorespiratory fitness, and muscle strength. Frontiers in Physiology. 2017; 8:1105. [DOI:10.3389/fphys.2017.01105] [PMID]
- Goldbeck TG, Davies GJ. Test-retest reliability of the closed kinetic chain upper extremity stability test: A clinical field test. Journal of Sport Rehabilitation. 2000; 9(1):35-45. [DOI:10.1123/jsr.9.1.35]
- Basar MJ, Stanek JM, Dodd DD, Begalle RL. The influence of corrective exercises on functional movement screen and physical fitness performance in army ROTC cadets. Journal of Sport Rehabilitation. 2019; 28(4):360-7. [DOI:10.1123/jsr.2018-0086] [PMID]
- Pedersen BK, Saltin B. Exercise as medicine-evidence for prescribing exercise as therapy in 26 different chronic diseases. Scandinavian Journal of Medicine & Science in Sports. 2015; 25 (Suppl 3):1-72. [DOI:10.1111/sms.12581] [PMID]
- Csepregi É, Gyurcsik Z, Veres-Balajti I, Nagy AC, Szekanecz Z, Szántó S. Effects of classical breathing exercises on posture, spinal and chest mobility among female university students compared to currently popular training programs. Int J Environ Res Public Health. 2022 Mar 21;19(6):3728. [DOI:10.3390/ijerph19063728] [PMID]
- Laurinavičiūtė E, Šiupšinskas L. The effect of neuromuscular training program on functional characteristics of upper extremity in handball and basketball players. Paper presented at: The 7th International Scientific Conference" Exercise for Health and Rehabilitation. 3 December 2021; Kaunas: Lithuanian University of Health Science. [Link]
- Strutt EP, Waller M, Daniel JU, ZAJIC K. A four-week upper-extremity exercise program on a balance device improves power and stability in collegiate golfers. International Journal of Sport Culture and Science. 2018; 6(1):48-55. [Link]
- Usluer ŞN, Aktuğ ZB, İbiş S, Aka H. The effect of corrective exercises on functional movement screen test and motor skills: [Turkish]. Journal of Human Science. 2021; 18(3):390-9. [Link]
- Guler O, Tuncel O, Bianco A. Effects of functional strength training on functional movement and balance in middle-aged adults. Sustainability. 2021; 13(3):1074. [DOI: 10.3390/su13031074]
- Sawczyn M. Effects of a periodized functional strength training program (FST) on functional movement screen (FMS) in physical education students. Physical Education of Students. 2020; 24(3):162-7. [DOI: 0000-0002-0077-3965]
- Cook G, Burton L, Hoogenboom BJ, Voight M. Functional movement screening: The use of fundamental movements as an assessment of function-part 2. International Journal of Sports Physical Therapy. 2014; 9(4):549-63. [PMID]
- de Oliveira VM, Pitangui AC, Nascimento VY, da Silva HA, Dos Passos MH, de Araújo RC. Test-retest reliability of the closed kinetic chain upper extremity stability test (CKCUEST) in adolescents: Reliability of CKCUEST in adolescents. International Journal of Sports Physical Therapy. 2017; 12(1):125-32. [PMID]
Type of Study: Research |
Subject:
General
Received: 2023/07/23 | Accepted: 2023/09/17 | Published: 2023/10/14
Received: 2023/07/23 | Accepted: 2023/09/17 | Published: 2023/10/14
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
