Sat, Feb 14, 2026
Volume 12, Issue 4 (Autumn 2022)
PTJ 2022, 12(4): 233-248 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Alizadeh M H, Jafari B, Amiri M R. The Effect of Prevention and Management Protocols on Low Back Pain in Athletes: A Systematic Review. PTJ 2022; 12 (4) :233-248
URL: http://ptj.uswr.ac.ir/article-1-547-en.html
URL: http://ptj.uswr.ac.ir/article-1-547-en.html



1- Department of Sports Medicine and Health, Faculty of Physical Education, University of Tehran, Tehran, Iran.
Full-Text [PDF 807 kb]
(2705 Downloads)
| Abstract (HTML) (3157 Views)
Full-Text: (1352 Views)
1. Introductiont
Participating in sports exercises and competitions, in addition to its advantages, is sometimes associated with acute and chronic injuries [1]. The popularization and industrialization of fitness over the past decade, with the rise of low-cost gyms and large group classes, has reduced the quality of initial training and assessment of practitioners, leading to the high risk of injury [2]. Low back pain (LBP) is the most common musculoskeletal disorder reported in the community, leading to chronic pain and disability. It is also a common health problem that creates a significant personal, social, and financial burden worldwide [1, 3]. Studies show that the prevalence of LBP in athletes who exercise daily increases after the age of 17 years [4]. Various studies have reported the prevalence of back pain in different sports; for example, the prevalence of back pain in wrestlers, elite gymnasts, and high school volleyball players was 59%, 79%, and 48%, respectively [1, 4]. Research shows that 21% of all reported injuries over eight seasons in a national rowing team were related to the lumbar spine [5, 6]. Recent research has focused on biomechanical and epidemiological analyzes to understand the mechanisms contributing to the onset of LBP. There has been a limited focus on management and prevention strategies [5]. Sports, such as dancing and football, which put a lot of pressure on the lumbar spine, are believed to have higher rates of LBP compared to less physically demanding activities [7]. Some movements help develop injuries, such as repetitive flexion, extension, rotation, and axial load-type movements [8]. LBP includes a range of different types of pain that often overlap with each other, and the elements that make up the lumbar spine is susceptible to different stresses, and each of these, alone or in combination, can contribute to back pain. Prevention of LBP is recognized as a major challenge in high-risk populations, and most management methods address only one method, whereas a multifaceted, interdisciplinary approach is necessary due to the complex nature of LBP [9]. However, the prevalence of LBP in athletes can be problematic for many reasons [10]. First, the failure to use generally accepted definitions of LBP in sports contains the severity, location, and duration of pain that organizes an episode of LBP [11, 12]. Second, the true potential for methodological flaws results in bias in the target population [13]. LBP is already a complex and vague entity confounded by the specific sport, etiology, and level of competition of the athlete [14]. According to Van Mechelen, the magnitude of the problem must first be identified with epidemiological studies to plan a preventive measure; hence determining the range of LBP exercise is the first step in prevention [1]. LBP prevention exercises and interventions are significantly effective when a functional diagnosis is made and then performed under the supervision of an expert before the start of the season [4]. Although the risk of back pain in athletes is high, most studies have been conducted on the management and prevention of LBP in other people, and the studies specifically on athletes were limited. Therefore, this review was conducted to determine the effect of prevention and management protocols on low back pain in athletes.
2. Materials and Methods
The current study is an evidence-based systematic review, and studies were eligible if they reported the prevalence of LBP in an athletic population from 2010 to 2022. No age or gender limitation existed in this systematic review. Researchers searched for related articles using the relevant keywords containing ‘back pain’ or ‘prevention’ or ‘low back pain’ or ‘backache’ or ‘athletes’ or ‘lumbago’ or ‘prevalence’ or the names of different sports listed by the International Olympic Committee [8] from specialized databases, including Science Direct, PubMed, Scopus, and Google Scholar. Also, the references of the articles were examined to find the articles that were not possible by searching the databases.
Selection of studies
The first researcher (B.J) checked all the titles in the databases and selected the articles that met the inclusion criteria, and then the second researcher (M.A) selected, checked, and confirmed the desired articles. During the search, the authors encountered similar reviews and meta-analyses, which were also excluded from the study, and the sources of these articles were used only if needed. The titles and abstracts of the found studies were examined regarding relevancy to the topic, and the full text of related studies was extracted for further evaluation. In this study, no specific definition for LBP was considered as an inclusion criterion.
Inclusion criteria
The inclusion criteria were limited to the following PICOS items, including population (athletes in different disciplines with back pain), interventions (prevention and management protocols), comparison (an intervention group that performed the exercise or method introduced to prevent and manage back pain and a control group), outcome (primary variable, visual analogue scale [VAS], and secondary variable, performance, etc.), and study design (randomized controlled trial [RCT] and clinical controlled trial [CCT]). Also, to access the full text of the article, the physiotherapy evidence database (PEDro) index score must be at least 4, and among the articles that contain back pain, only articles that had prevention programs for athletes were selected. Exercise interventions included all studies that used at least one protocol for the prevention and management of LBP that was clearly described, and other articles were excluded from the study. The reviewed articles should use appropriate and high validity and reliability tools. The most widely used and most reliable pain measurement methods in the world are McGill, the numerical pain rating scale (NPR), VAS, and Quebec. In addition, functional disability, which has been evaluated in many back pain studies, has been used by two widely used questionnaires with high validity and reliability, including Roland Morris disability questionnaires (RMDQ) with 24 items and Oswestry with 10 items. If the article searched by the browsers did not have this feature, it was excluded from the study.
Exclusion criteria
Review articles, articles about chiropractic and manipulation, articles that were not conducted on athletes, and non-athletic protocols, such as pharmacological or psychological training were excluded.
Level of evidence and quality assessment
Based on van Furlan et al. [15] conduct and report systematic reviews of trials in this field. SUMMARY OF BACKGROUND DATA. In 1997, the Cochrane Back Review Group published Method Guidelines for Systematic Reviews, which was updated in 2003. Since then, new methodologic evidence has emerged and standards have changed. Coupled with the upcoming revisions to the software and methods required by The Cochrane Collaboration, it was clear that revisions were needed to the existing guidelines. METHODS. The Cochrane Back Review Group editorial and advisory boards met in June 2006 to review the relevant new methodologic evidence and determine how it should be incorporated. Based on the discussion, the guidelines were revised and circulated for comment. As sections of the new Cochrane Handbook for Systematic Reviews of Interventions were made available, the guidelines were checked for consistency. A working draft was made available to review authors in The Cochrane Library 2008, issue 3. RESULTS. The final recommendations are divided into 7 categories: objectives, literature search, inclusion criteria, risk of bias assessment, data extraction, data analysis, and updating your review. Each recommendation is classified into minimum criteria (mandatory, the level of evidence has been classified into five levels by two independent researchers (BJ and MA). The PEDro index was used for the quality of the selected studies, which has high validity and reliability. This index determines whether RCTs have internal validity or not, whether the statistical information is appropriate to interpret the reported results, and also determines the external validity or generalizability of the study. This scale consists of 11 items; the answer to each item is indicated by a positive sign (correct execution of the desired item) and a negative sign (incorrect execution or not mentioning it). Each positive sign includes one point, but a negative sign does not include any points. In addition, the answer to the first question does not include a score; in the end, all the points are added and considered as the total score, and the scores obtained in this scale are considered from zero to 10 so that the score of 9 and 10 is excellent, 6-8 is considered good, 4 and 5 are considered poor, and a score less than 4 is considered very poor [16] the methodological quality of clinical trials? What is the hierarchy of items of the PEDro scale from least to most adhered to? Is there any effect of year of publication of trials on item adherence? Are PEDro scale ordinal scores equivalent to interval data? Design: Rasch analysis of two independent samples of 100 clinical trials from the PEDro database scored using the PEDro scale. Results: Both samples of PEDro data showed it to the Rasch model with no item misit. The PEDro scale item hierarchy was the same in both samples, ranging from the most adhered to item random allocation, to the least adhered to item therapist blinding. There was no differential item functioning by year of publication. Original PEDro ordinal scores were highly correlated with transformed PEDro interval scores (r=0.99).
3. Results
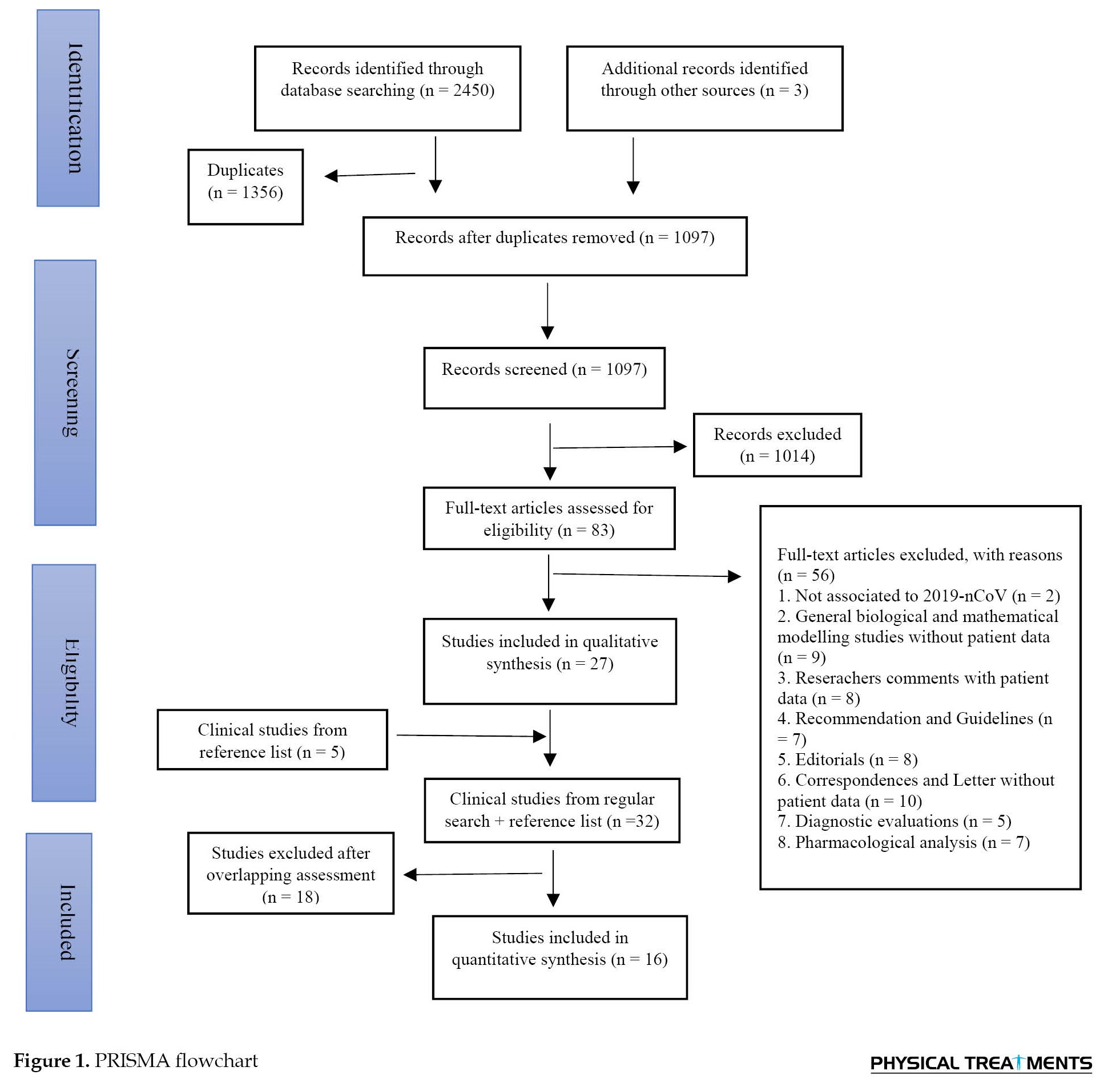
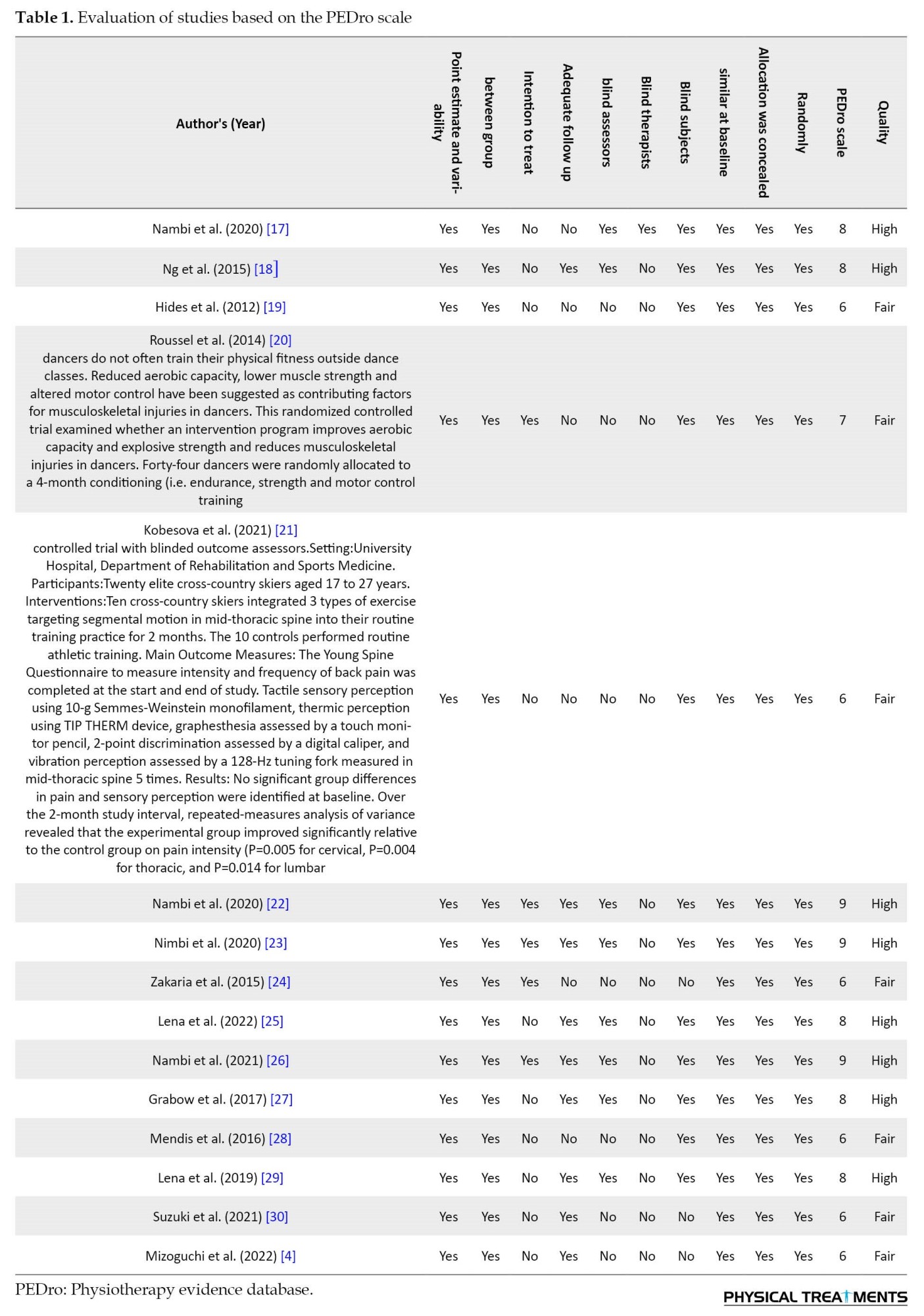
Primary searches in a combination of manual inspection for further relevant references yielded 2,453 records, including 1,356 duplicates which were removed. After screening the titles and abstracts, 1,014 records were excluded. Then, 83 potentially relevant studies were considered eligible for full-text assessment, resulting in 16 studies included in this systematic review for quality assessment, data extraction, and analysis. All 16 included studies were RCTs. They were all published in English. It should be noted that all the articles were first checked by the first researcher by the PEDro scale regarding the quality and then confirmed by the second researcher. Studies that scored equal to or more than four were included in the review. Table 1 presents the results of the quality assessment of the selected studies.
Since none of the incoming articles had similar conditions regarding implementation methods, measurement tools, evaluated parameters, and test status, it was not possible to conduct a meta-analysis. Table 2 presents that the subjects participating in the obtained articles included male and female athletes aged 14-40 years.


A total of 1,317 subjects participated in 16 selected studies, the smallest sample size was 20 subjects [21, 31] controlled trial with blinded outcome assessors.Setting:University Hospital, Department of Rehabilitation and Sports Medicine.Participants:Twenty elite cross-country skiers aged 17 to 27 years.Interventions:Ten cross-country skiers integrated 3 types of exercise targeting segmental motion in mid-thoracic spine into their routine training practice for 2 months. The 10 controls performed routine athletic training.Main Outcome Measures:The Young Spine Questionnaire to measure intensity and frequency of back pain was completed at the start and end of study. Tactile sensory perception using 10-g Semmes-Weinstein monofilament, thermic perception using TIP THERM device, graphesthesia assessed by a touch monitor pencil, 2-point discrimination assessed by a digital caliper, and vibration perception assessed by a 128-Hz tuning fork measured in mid-thoracic spine 5 times.Results:No significant group differences in pain and sensory perception were identified at baseline. Over the 2-month study interval, repeated-measures analysis of variance revealed that the experimental group improved significantly relative to the control group on pain intensity (P=0.005 for cervical, P=0.004 for thoracic, and P=0.014 for lumbar, and the largest sample size was 465 subjects [24]. In most research, in addition to evaluating the amount of pain and functional disability, factors, such as flexibility, strength, balance, endurance, and psychological factors, such as fear of performing movements, anxiety, and depression have been discussed in different periods. Duration of the protocols varies from immediately after intervention [32] to 24 weeks after intervention [25, 29, 31] lifting loads, or torsion movement. Objectives: This study aims to examine the effectiveness of the postural treatment of the Mézières method on elite rhythmic gymnastics athletes with low back pain. Design: Double-blind, randomized, controlled trial. Setting: The sports hall of “Puente Tocinos,” Murcia, Spain. Participants: Ninety gymnastics athletes were randomized into 2 parallel groups (intervention: n=39; control: n=51. The time frame of the prevention and management protocol for back pain in more than 80% of the articles was between 4 and 24 weeks.
Different protocols, such as kinesio taping [32], cognitive functional approach, movement patterns, conditioning, and lifestyle factors [18, 20] movement patterns, conditioning and lifestyle factors relevant to each rower for 8 weeks. The active control group (n=17, motor control [19, 20, 28] quadratus lumborum, and psoas muscles and the change in CSA of the trunk in response to an abdominal drawing-in task. These measures of muscle size and function were performed using magnetic resonance imaging. Availability of players for competition games was used to assess the effect of the intervention on the occurrence of injuries.
Participating in sports exercises and competitions, in addition to its advantages, is sometimes associated with acute and chronic injuries [1]. The popularization and industrialization of fitness over the past decade, with the rise of low-cost gyms and large group classes, has reduced the quality of initial training and assessment of practitioners, leading to the high risk of injury [2]. Low back pain (LBP) is the most common musculoskeletal disorder reported in the community, leading to chronic pain and disability. It is also a common health problem that creates a significant personal, social, and financial burden worldwide [1, 3]. Studies show that the prevalence of LBP in athletes who exercise daily increases after the age of 17 years [4]. Various studies have reported the prevalence of back pain in different sports; for example, the prevalence of back pain in wrestlers, elite gymnasts, and high school volleyball players was 59%, 79%, and 48%, respectively [1, 4]. Research shows that 21% of all reported injuries over eight seasons in a national rowing team were related to the lumbar spine [5, 6]. Recent research has focused on biomechanical and epidemiological analyzes to understand the mechanisms contributing to the onset of LBP. There has been a limited focus on management and prevention strategies [5]. Sports, such as dancing and football, which put a lot of pressure on the lumbar spine, are believed to have higher rates of LBP compared to less physically demanding activities [7]. Some movements help develop injuries, such as repetitive flexion, extension, rotation, and axial load-type movements [8]. LBP includes a range of different types of pain that often overlap with each other, and the elements that make up the lumbar spine is susceptible to different stresses, and each of these, alone or in combination, can contribute to back pain. Prevention of LBP is recognized as a major challenge in high-risk populations, and most management methods address only one method, whereas a multifaceted, interdisciplinary approach is necessary due to the complex nature of LBP [9]. However, the prevalence of LBP in athletes can be problematic for many reasons [10]. First, the failure to use generally accepted definitions of LBP in sports contains the severity, location, and duration of pain that organizes an episode of LBP [11, 12]. Second, the true potential for methodological flaws results in bias in the target population [13]. LBP is already a complex and vague entity confounded by the specific sport, etiology, and level of competition of the athlete [14]. According to Van Mechelen, the magnitude of the problem must first be identified with epidemiological studies to plan a preventive measure; hence determining the range of LBP exercise is the first step in prevention [1]. LBP prevention exercises and interventions are significantly effective when a functional diagnosis is made and then performed under the supervision of an expert before the start of the season [4]. Although the risk of back pain in athletes is high, most studies have been conducted on the management and prevention of LBP in other people, and the studies specifically on athletes were limited. Therefore, this review was conducted to determine the effect of prevention and management protocols on low back pain in athletes.
2. Materials and Methods
The current study is an evidence-based systematic review, and studies were eligible if they reported the prevalence of LBP in an athletic population from 2010 to 2022. No age or gender limitation existed in this systematic review. Researchers searched for related articles using the relevant keywords containing ‘back pain’ or ‘prevention’ or ‘low back pain’ or ‘backache’ or ‘athletes’ or ‘lumbago’ or ‘prevalence’ or the names of different sports listed by the International Olympic Committee [8] from specialized databases, including Science Direct, PubMed, Scopus, and Google Scholar. Also, the references of the articles were examined to find the articles that were not possible by searching the databases.
Selection of studies
The first researcher (B.J) checked all the titles in the databases and selected the articles that met the inclusion criteria, and then the second researcher (M.A) selected, checked, and confirmed the desired articles. During the search, the authors encountered similar reviews and meta-analyses, which were also excluded from the study, and the sources of these articles were used only if needed. The titles and abstracts of the found studies were examined regarding relevancy to the topic, and the full text of related studies was extracted for further evaluation. In this study, no specific definition for LBP was considered as an inclusion criterion.
Inclusion criteria
The inclusion criteria were limited to the following PICOS items, including population (athletes in different disciplines with back pain), interventions (prevention and management protocols), comparison (an intervention group that performed the exercise or method introduced to prevent and manage back pain and a control group), outcome (primary variable, visual analogue scale [VAS], and secondary variable, performance, etc.), and study design (randomized controlled trial [RCT] and clinical controlled trial [CCT]). Also, to access the full text of the article, the physiotherapy evidence database (PEDro) index score must be at least 4, and among the articles that contain back pain, only articles that had prevention programs for athletes were selected. Exercise interventions included all studies that used at least one protocol for the prevention and management of LBP that was clearly described, and other articles were excluded from the study. The reviewed articles should use appropriate and high validity and reliability tools. The most widely used and most reliable pain measurement methods in the world are McGill, the numerical pain rating scale (NPR), VAS, and Quebec. In addition, functional disability, which has been evaluated in many back pain studies, has been used by two widely used questionnaires with high validity and reliability, including Roland Morris disability questionnaires (RMDQ) with 24 items and Oswestry with 10 items. If the article searched by the browsers did not have this feature, it was excluded from the study.
Exclusion criteria
Review articles, articles about chiropractic and manipulation, articles that were not conducted on athletes, and non-athletic protocols, such as pharmacological or psychological training were excluded.
Level of evidence and quality assessment
Based on van Furlan et al. [15] conduct and report systematic reviews of trials in this field. SUMMARY OF BACKGROUND DATA. In 1997, the Cochrane Back Review Group published Method Guidelines for Systematic Reviews, which was updated in 2003. Since then, new methodologic evidence has emerged and standards have changed. Coupled with the upcoming revisions to the software and methods required by The Cochrane Collaboration, it was clear that revisions were needed to the existing guidelines. METHODS. The Cochrane Back Review Group editorial and advisory boards met in June 2006 to review the relevant new methodologic evidence and determine how it should be incorporated. Based on the discussion, the guidelines were revised and circulated for comment. As sections of the new Cochrane Handbook for Systematic Reviews of Interventions were made available, the guidelines were checked for consistency. A working draft was made available to review authors in The Cochrane Library 2008, issue 3. RESULTS. The final recommendations are divided into 7 categories: objectives, literature search, inclusion criteria, risk of bias assessment, data extraction, data analysis, and updating your review. Each recommendation is classified into minimum criteria (mandatory, the level of evidence has been classified into five levels by two independent researchers (BJ and MA). The PEDro index was used for the quality of the selected studies, which has high validity and reliability. This index determines whether RCTs have internal validity or not, whether the statistical information is appropriate to interpret the reported results, and also determines the external validity or generalizability of the study. This scale consists of 11 items; the answer to each item is indicated by a positive sign (correct execution of the desired item) and a negative sign (incorrect execution or not mentioning it). Each positive sign includes one point, but a negative sign does not include any points. In addition, the answer to the first question does not include a score; in the end, all the points are added and considered as the total score, and the scores obtained in this scale are considered from zero to 10 so that the score of 9 and 10 is excellent, 6-8 is considered good, 4 and 5 are considered poor, and a score less than 4 is considered very poor [16] the methodological quality of clinical trials? What is the hierarchy of items of the PEDro scale from least to most adhered to? Is there any effect of year of publication of trials on item adherence? Are PEDro scale ordinal scores equivalent to interval data? Design: Rasch analysis of two independent samples of 100 clinical trials from the PEDro database scored using the PEDro scale. Results: Both samples of PEDro data showed it to the Rasch model with no item misit. The PEDro scale item hierarchy was the same in both samples, ranging from the most adhered to item random allocation, to the least adhered to item therapist blinding. There was no differential item functioning by year of publication. Original PEDro ordinal scores were highly correlated with transformed PEDro interval scores (r=0.99).
3. Results
Primary searches in a combination of manual inspection for further relevant references yielded 2,453 records, including 1,356 duplicates which were removed. After screening the titles and abstracts, 1,014 records were excluded. Then, 83 potentially relevant studies were considered eligible for full-text assessment, resulting in 16 studies included in this systematic review for quality assessment, data extraction, and analysis. All 16 included studies were RCTs. They were all published in English. It should be noted that all the articles were first checked by the first researcher by the PEDro scale regarding the quality and then confirmed by the second researcher. Studies that scored equal to or more than four were included in the review. Table 1 presents the results of the quality assessment of the selected studies.
Since none of the incoming articles had similar conditions regarding implementation methods, measurement tools, evaluated parameters, and test status, it was not possible to conduct a meta-analysis. Table 2 presents that the subjects participating in the obtained articles included male and female athletes aged 14-40 years.
A total of 1,317 subjects participated in 16 selected studies, the smallest sample size was 20 subjects [21, 31] controlled trial with blinded outcome assessors.Setting:University Hospital, Department of Rehabilitation and Sports Medicine.Participants:Twenty elite cross-country skiers aged 17 to 27 years.Interventions:Ten cross-country skiers integrated 3 types of exercise targeting segmental motion in mid-thoracic spine into their routine training practice for 2 months. The 10 controls performed routine athletic training.Main Outcome Measures:The Young Spine Questionnaire to measure intensity and frequency of back pain was completed at the start and end of study. Tactile sensory perception using 10-g Semmes-Weinstein monofilament, thermic perception using TIP THERM device, graphesthesia assessed by a touch monitor pencil, 2-point discrimination assessed by a digital caliper, and vibration perception assessed by a 128-Hz tuning fork measured in mid-thoracic spine 5 times.Results:No significant group differences in pain and sensory perception were identified at baseline. Over the 2-month study interval, repeated-measures analysis of variance revealed that the experimental group improved significantly relative to the control group on pain intensity (P=0.005 for cervical, P=0.004 for thoracic, and P=0.014 for lumbar, and the largest sample size was 465 subjects [24]. In most research, in addition to evaluating the amount of pain and functional disability, factors, such as flexibility, strength, balance, endurance, and psychological factors, such as fear of performing movements, anxiety, and depression have been discussed in different periods. Duration of the protocols varies from immediately after intervention [32] to 24 weeks after intervention [25, 29, 31] lifting loads, or torsion movement. Objectives: This study aims to examine the effectiveness of the postural treatment of the Mézières method on elite rhythmic gymnastics athletes with low back pain. Design: Double-blind, randomized, controlled trial. Setting: The sports hall of “Puente Tocinos,” Murcia, Spain. Participants: Ninety gymnastics athletes were randomized into 2 parallel groups (intervention: n=39; control: n=51. The time frame of the prevention and management protocol for back pain in more than 80% of the articles was between 4 and 24 weeks.
Different protocols, such as kinesio taping [32], cognitive functional approach, movement patterns, conditioning, and lifestyle factors [18, 20] movement patterns, conditioning and lifestyle factors relevant to each rower for 8 weeks. The active control group (n=17, motor control [19, 20, 28] quadratus lumborum, and psoas muscles and the change in CSA of the trunk in response to an abdominal drawing-in task. These measures of muscle size and function were performed using magnetic resonance imaging. Availability of players for competition games was used to assess the effect of the intervention on the occurrence of injuries.
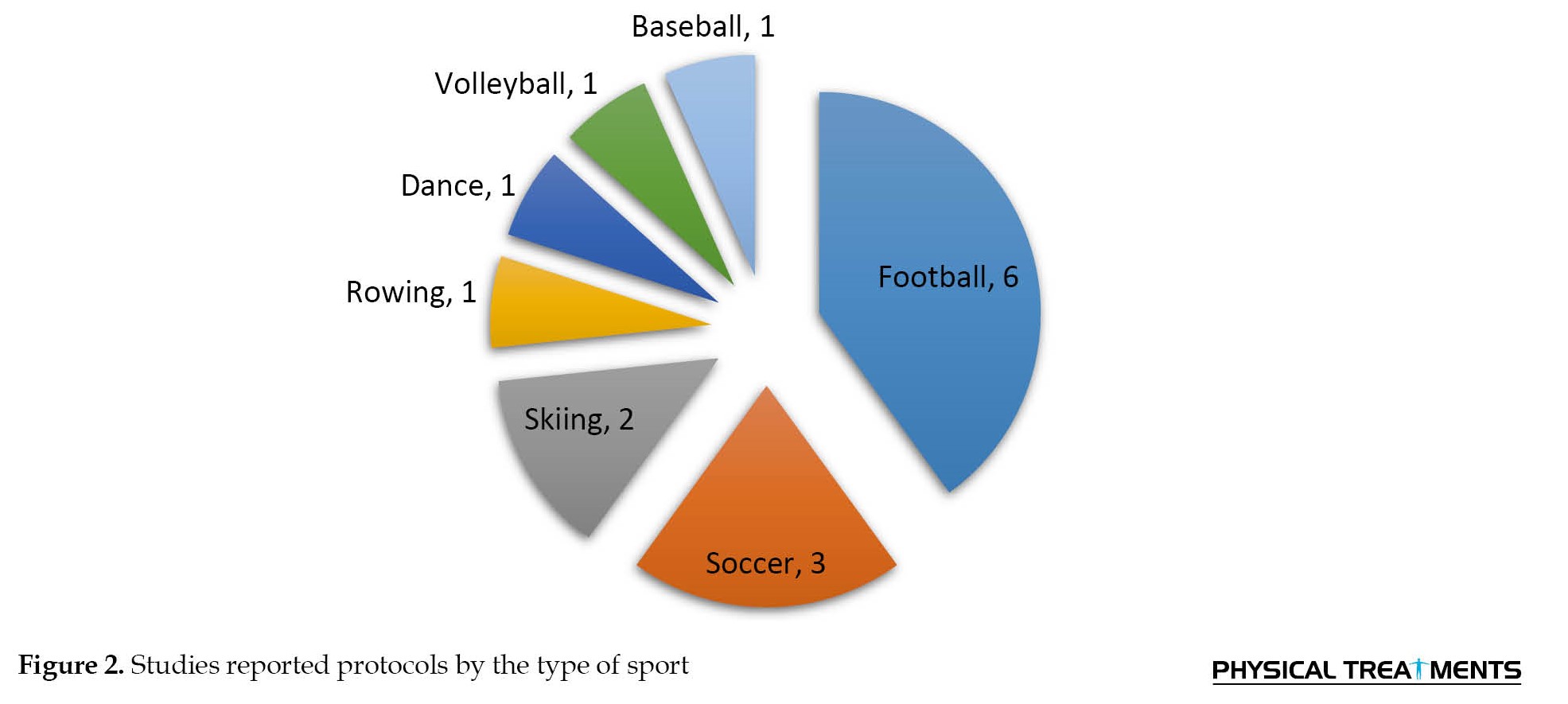
The motor control program involved performance of voluntary contractions of the multifidus and transversus abdominis muscles while receiving feedback from ultrasound imaging. Because all players were to receive the intervention, the trial was delivered as a stepped-wedge design with three treatment arms (a 15-wk intervention, a 8-wk intervention, and a waitlist control who received a 7-wk intervention toward the end of the playing season, segmental motion in the mid-thoracic spine [21] controlled trial with blinded outcome assessors. Setting: University Hospital, Department of Rehabilitation and Sports Medicine.Participants:Twenty elite cross-country skiers aged 17 to 27 years.Interventions:Ten cross-country skiers integrated 3 types of exercise targeting segmental motion in mid-thoracic spine into their routine training practice for 2 months. The 10 controls performed routine athletic training.Main Outcome Measures:The Young Spine Questionnaire to measure intensity and frequency of back pain was completed at the start and end of study. Tactile sensory perception using 10-g Semmes-Weinstein monofilament, thermic perception using TIP THERM device, graphesthesia assessed by a touch monitor pencil, 2-point discrimination assessed by a digital caliper, and vibration perception assessed by a 128-Hz tuning fork measured in mid-thoracic spine 5 times.Results:No significant group differences in pain and sensory perception were identified at baseline. Over the 2-month study interval, repeated-measures analysis of variance revealed that the experimental group improved significantly relative to the control group on pain intensity (P=0.005 for cervical, P=0.004 for thoracic, and P=0.014 for lumbar, functional movement system (FMS) training [30], isokinetic and core stabilization [22, 23], virtual reality training [26], dynamic and static stretching [24] Mézières method [25, 29, 31] rhythmic gymnastics, and basketball. Design: Randomized controlled trial. Setting: Training Camp. Participants: One hundred and thirty-nine elite athletes with low back pain of whom 69 were assigned to the experimental group. Intervention: The intervention consists of treatment with three lying postures in a 40-minute-long session twice a week. The session’s goal was to focus on breathing exercises, spine mobility, and stretching of the back muscles, with particular attention to the diaphragmatic, paravertebral, and latissimus dorsi muscles. Outcome measures: Assessments such as visual analogue scale (VAS, semi-customized exercises [4], had been working on elite and semi-elite athletes. Figure 2 shows the average of the sports that have been worked on in the present studies.
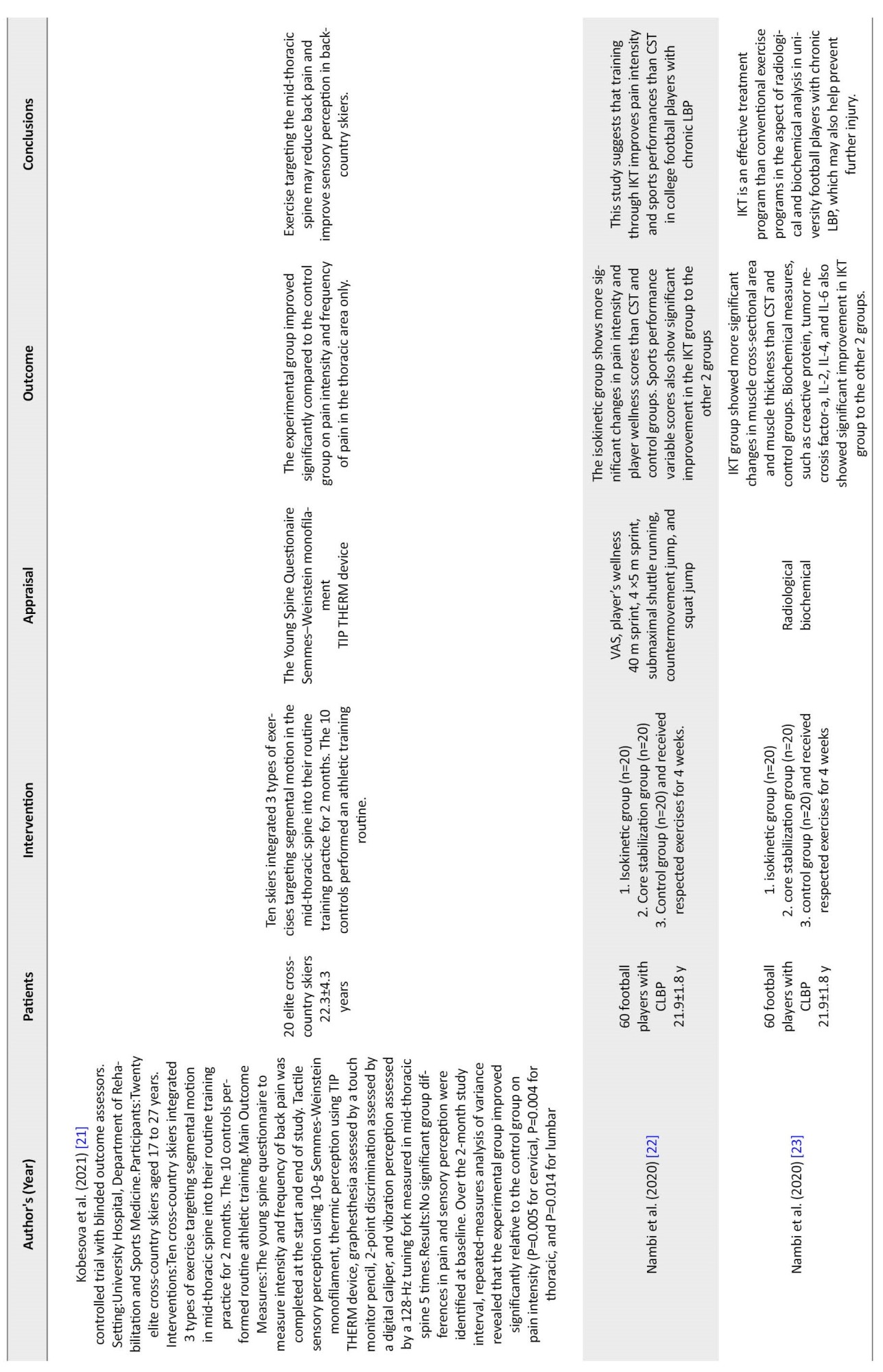
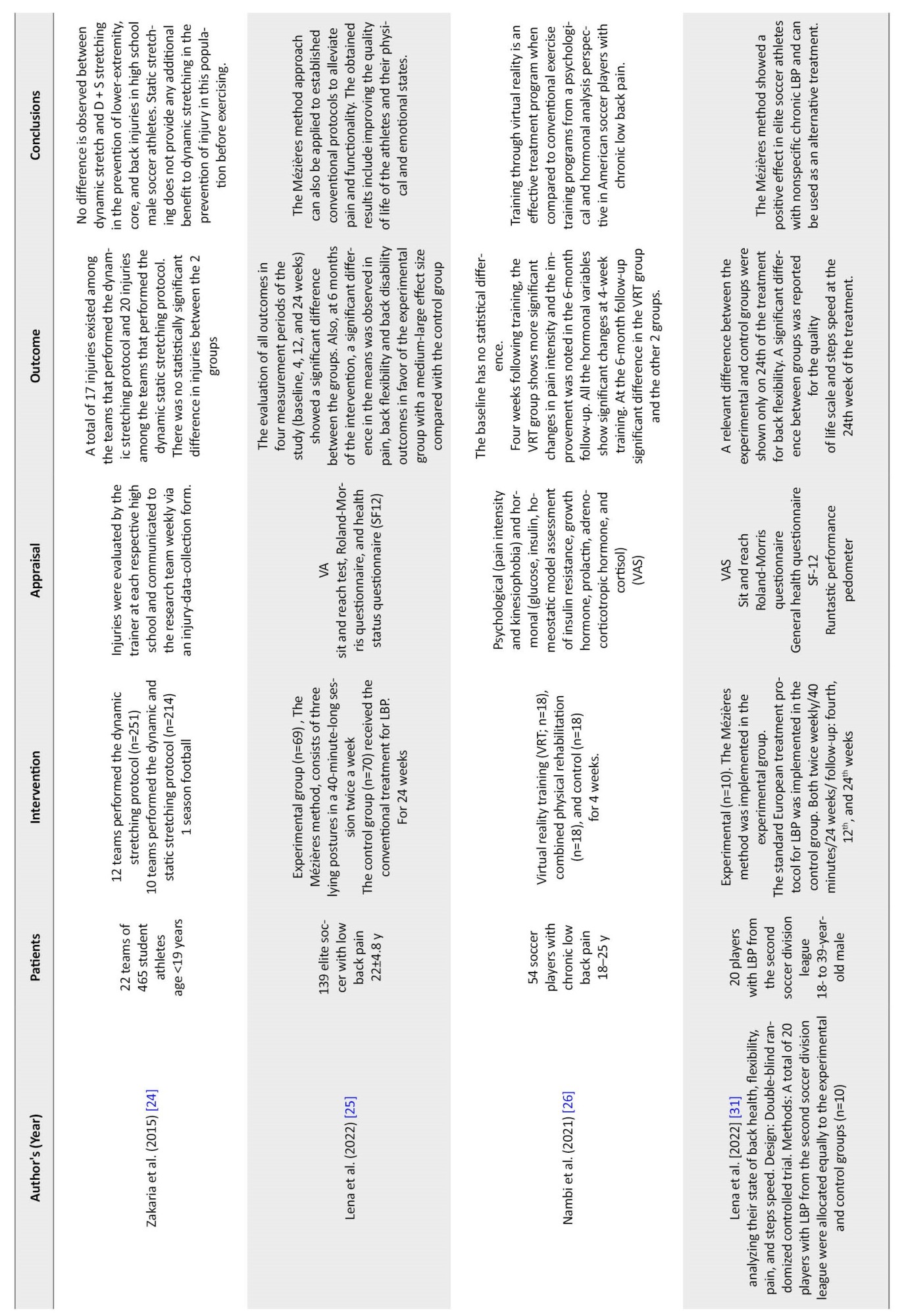
Except for three articles that did not have a control group and only compared training methods [19, 24, 28], the rest had a control group. In four studies, RMDQ was used to evaluate performance or functional disability [18, 25, 29, 31]. To evaluate the pain level, VAS, NPR, and McGill pain questionnaires (short form) were also used [18, 22, 25, 26, 29–33]. To evaluate people's quality of life, SF-12, SF-39, and SF-36 questionnaires were also used in five studies [20, 25, 29, 31, 33]. Functional tests that were conducted in the studies included patient-specific functional scale, Biering-Sorensen test [18], runtastic performance pedometer [25, 29, 31], braked bicycle ergometer, standing broad jump test, dance functional outcome survey, Baecke questionnaire [20], player's wellness 40 m sprint, 4×5 m sprint, submaximal shuttle running, counter movement jump, and squat jump [17, 22], FMS [30], and physical function tests [4, 17]. In five studies, data were collected from precision tools, such as Semmes–Weinstein monofilament TIP THERM device [34], real-time ultrasound imaging 1.5-T Siemens Sonata MR system [19], radiological, biochemical [23], and hormonal test [26], magnetic resonance images taken at three-time points during the season [28]. Table 2 provides an overview of the studies included in the study. The first steps in evaluating an athlete presenting with back pain include a thorough history and physical examination to uncover the mechanism of injury, identify any neurological deficits or signs of more serious injury, and direct the physician to take the appropriate actions [7].
4. Discussion
This systematic review aimed to determine the effect of the prevention and management protocols for LBP in athletes. Based on the inclusion and exclusion criteria, 16 articles with 1,317 subjects were included in the study. The present review shows that all the protocols implemented during the past 12 years have improved and prevented back pain. In these protocols, various methods have been used to prevent back pain. In some studies, in addition to pain factors, psychological, functional, and tissue physiological effects were discussed. The research process of the researchers was to activate the trunk muscles with various methods, and the best method that was mentioned in most studies was voluntary exercises with full knowledge of the person and individual training in the correct position.
Most of the reviews have examined studies that are more focused on a training protocol or focus on specific muscle groups, and fewer have examined different training methods in improving the pain and functional disability of athletes. Among these articles, nine studies used the cognitive and stability method alone or in comparison with other protocols, which is more than 50% of the articles. In the evaluation of the quality of these articles, the scores obtained are between 6 to 9, which are relatively high scores, such protocols can be highly effective in improving back pain and functional disability of athletes in various disciplines. The results of studies show that repetitive and risky movements in different sports cause imbalance and muscle weakness in the lumbar, pelvic, and central body areas, especially the multifidus muscles, diaphragm, pelvic floor, transverse and rectus abdominis muscles, and gluteal muscles [19, 28]. Vital muscles exist in the stability of the lumbopelvic region because the transversus abdominis muscle is connected to the lumbar vertebrae through the thoracolumbar fascia, and the contraction of this muscle creates the lumbar stability of the pelvis, and the contraction of the multifidus muscle also improves alignment and stabilizes the vertebral column [35]. Cognitive and stability protocols with a focus on designing and implementing a type of exercise aiming to maintain and increase local lumbar stability through proprioceptive retraining of the lumbar-pelvic region using the influence on the organs of this region play a crucial role in increasing stability. Several protocols have been presented in the reviewed studies, and the most prominent ones are discussed.
The Mézières method, which is an individual rehabilitation technique with a systematic postural approach based on physical and mathematical concepts, determines functional recovery through the correction of body symmetry [31] analyzing their state of back health, flexibility, pain, and steps speed. Design: Double-blind randomized controlled trial. Methods: A total of 20 players with LBP from the second soccer division league were allocated equally to the experimental and control groups (n=10. This method is a safe and adaptive treatment because it is based on static stretching [25]. In other words, a close relationship is observed between the mind and the body within the Mézières method, and this means that the treatment of physical, functional, and psychological aspects can improve the attitude, condition, and quality of life of the athlete with LBP [29]. Lena et al have stated in their studies that the benefits of this method are observed in a long period of treatment (24 weeks) because the morphological changes of muscle imbalance should be corrected again. In several articles, this method has been used to treat the back pain of athletes to retrain the posture of the whole body individually, and the results showed that this method could initially increase the flexibility of the back and ultimately reduce the disability and back pain of the athletes and also improves the quality of life and performance in athletes [25, 29, 31] analyzing their state of back health, flexibility, pain, and steps speed. Design: Double-blind randomized controlled trial. Methods: A total of 20 players with LBP from the second soccer division league were allocated equally to the experimental and control groups (n=10. On the other hand, movement improves the size and function of trunk muscles in elite soccer players with and without LBP [36] optimize rehabilitation, and enhance performance is a priority for practitioners. Different exercises produce different effects on neuromuscular performance. Clarity of the purpose of a prescribed exercise is central to a successful outcome. Spinal exercises need to be classified according to the objective of the exercise and planned physical outcome. Objective: To define the modifiable spinal abilities that underpin optimal function during skilled athletic performance, clarify the effect of spinal pain and pathologic conditions, and classify spinal exercises according to the objective of the exercise and intended physical outcomes to inform training and rehabilitation. Design: Qualitative study. Data Collection and Analysis: We conducted a qualitative consensus method of 4 iterative phases. An exploratory panel carried out an extended review of the English-language literature using CINAHL, EMBASE, MEDLINE, and PubMed to identify key themes and subthemes to inform the definitions of exercise categories, physical abilities, and physical outcomes. An expert project group reviewed panel findings. A draft classification was discussed with physiotherapists (n=49. Mendis et al investigated the changes in the size of trunk and thigh muscles during movement control exercises with the help of ultrasound, and the results indicated an increase in the size of these muscles [28].
Central stability exercises are also a special method of exercise that is usually used for the central muscles of the trunk in the treatment of back problems. In these exercises, Swiss balls of different sizes are applied to train the main muscles. These exercises are fun and reduce the difficulty of rehabilitation sessions. Exercise with a Swiss ball allows the processing of motor messages to transmit the best sensory message to the muscles and create neuroplastic changes for new motor learning. Studies in this field indicate an increase in the activity of the human sensory and motor system, which leads to a decrease in the intensity of back pain and an improvement in the strength, endurance, and flexibility of the trunk muscles and directly stabilizes sports performance [26, 37, 38] we aimed to investigate the effects of Tai Chi Chuan (TCC).
Another effective method that was addressed is the Dynamic Neuromuscular Stabilization (DNS) method, as a manual and rehabilitative approach to optimizing the motor system based on the scientific principles of developmental kinesiology. Dynamic stability is achieved through precise muscle coordination by the central nervous system. This method provides a framework for understanding the mutual integration of the skeleton, joints, muscles, and nerves along the dynamic kinetic chain [39] spinal extensors, gluteals or any other musculature; rather, core stabilization is accomplished through precise coordination of these muscles and intra-abdominal pressure regulation by the central nervous system. Understanding developmental kinesiology provides a framework to appreciate the regional interdependence and the inter-linking of the skeleton, joints, musculature during movement and the importance of training both the dynamic and stabilizing function of muscles in the kinetic chain. The dynamic neuromuscular stabilization (DNS). It was also done with a particular emphasis on the quality of training, complete awareness of the body, and prevention of hyperactivity. This training process makes the peripheral mechanoreceptors participate in the actions of the trunk muscles. Finally, the results of studies in this field show that a new sports program based on the principles of dynamic neuromuscular stabilization (DNS), which targets stabilization and segmental movement in the middle part of the thoracic spine, may reduce back pain and improve the quality of sensory perception in athletes [21, 34, 39] controlled trial with blinded outcome assessors.Setting:University Hospital, Department of Rehabilitation and Sports Medicine.Participants:Twenty elite cross-country skiers aged 17 to 27 years.Interventions:Ten cross-country skiers integrated 3 types of exercise targeting segmental motion in mid-thoracic spine into their routine training practice for 2 months. The 10 controls performed routine athletic training.Main Outcome Measures:The Young Spine Questionnaire to measure intensity and frequency of back pain was completed at the start and end of study. Tactile sensory perception using 10-g Semmes-Weinstein monofilament, thermic perception using TIP THERM device, graphesthesia assessed by a touch monitor pencil, 2-point discrimination assessed by a digital caliper, and vibration perception assessed by a 128-Hz tuning fork measured in mid-thoracic spine 5 times.Results:No significant group differences in pain and sensory perception were identified at baseline. Over the 2-month study interval, repeated-measures analysis of variance revealed that the experimental group improved significantly relative to the control group on pain intensity (P=0.005 for cervical, P=0.004 for thoracic, and P=0.014 for lumbar.
Another method that was addressed in Nambi’s studies is VRT, an advanced rehabilitation method dependent on artificial intelligence and machine learning because it accelerates the motor learning process in a step-by-step feedback manner. Tasks and games are customized according to the needs of the patient and the therapist and provide the environment and activities in real-time [17, 26, 40]. It also stimulates cognitive properties through sensory feedback (auditory, visual, and tactile), activates cortical and subcortical brain neurons, and reduces the feeling of pain in the body. In addition, it improves the functional capacity and perception of athletes by providing different physical activities [41]. Studies have also shown that VRT breaks the cycle of fear of movement through pain distraction techniques and has extensive beneficial effects on pain relief [26].
The common goal in all the presented protocols was to reduce pain and improve the quality of life of the athletes. Chiropractic treatments are an alternative treatment and have a temporary effect despite the activation of muscle receptors, but it should be done by trained people, and it is better to use multifaceted programs [42]. Kinesio taping is also an alternative treatment that needs more studies to evaluate its effects because studies have shown few benefits [43]. Other previous studies that combined different rehabilitation methods showed better results when manual therapy and exercise therapy were administered to subjects [44]. Scientific communities widely investigate the benefits of exercise for the health of people with low back pain, but the results of this research cannot be generalized to all people because the individuality and the motivation to explore the movement are of a diverse nature [45]. However, definitive results in this field need more and more detailed investigations in future studies.
5. Conclusion
According to the results from the articles, it can be proved that among the therapeutic interventions used, the exercises that tried to integrate the deep and superficial muscles by correcting the person’s posture and calling the muscles correctly had the greatest effect on the balance of the muscles. They created this process with mental knowledge and complete awareness of the person and finally created factors of strength, endurance, and flexibility in tissues. What was mentioned in all the studies was the individualization of the multifaceted protocols according to the needs of the individual.
Limitations
The terms “back pain” and “back injury” are different. Sometimes, the athlete complains of pain, but during the clinical examination, the pathology of the injury is not diagnosed for him. In the studies, these two terms are not properly distinguished, which was a challenge in this study. The limitations of this study include lack of inclusion of studies other than English and articles that were not presented as RCTs.
Ethical Considerations
Compliance with ethical guidelines
There were no ethical considerations to be considered in this research.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization, investigation, resources and funding acquisition: All authors; Methodology: Behrouz Jafari; Writing original draft: Behrouz Jafari; Writing, reviewing, and editing: Mohammad Hosein Alizadeh and Behrouz Jafari; Supervision: Mohammad Hosein Alizadeh.
Conflict of interest
The authors declared no conflict of interest in this study.
Acknowledgments
The authors thank the researchers whose papers helped us present the results of this study.
References
4. Discussion
This systematic review aimed to determine the effect of the prevention and management protocols for LBP in athletes. Based on the inclusion and exclusion criteria, 16 articles with 1,317 subjects were included in the study. The present review shows that all the protocols implemented during the past 12 years have improved and prevented back pain. In these protocols, various methods have been used to prevent back pain. In some studies, in addition to pain factors, psychological, functional, and tissue physiological effects were discussed. The research process of the researchers was to activate the trunk muscles with various methods, and the best method that was mentioned in most studies was voluntary exercises with full knowledge of the person and individual training in the correct position.
Most of the reviews have examined studies that are more focused on a training protocol or focus on specific muscle groups, and fewer have examined different training methods in improving the pain and functional disability of athletes. Among these articles, nine studies used the cognitive and stability method alone or in comparison with other protocols, which is more than 50% of the articles. In the evaluation of the quality of these articles, the scores obtained are between 6 to 9, which are relatively high scores, such protocols can be highly effective in improving back pain and functional disability of athletes in various disciplines. The results of studies show that repetitive and risky movements in different sports cause imbalance and muscle weakness in the lumbar, pelvic, and central body areas, especially the multifidus muscles, diaphragm, pelvic floor, transverse and rectus abdominis muscles, and gluteal muscles [19, 28]. Vital muscles exist in the stability of the lumbopelvic region because the transversus abdominis muscle is connected to the lumbar vertebrae through the thoracolumbar fascia, and the contraction of this muscle creates the lumbar stability of the pelvis, and the contraction of the multifidus muscle also improves alignment and stabilizes the vertebral column [35]. Cognitive and stability protocols with a focus on designing and implementing a type of exercise aiming to maintain and increase local lumbar stability through proprioceptive retraining of the lumbar-pelvic region using the influence on the organs of this region play a crucial role in increasing stability. Several protocols have been presented in the reviewed studies, and the most prominent ones are discussed.
The Mézières method, which is an individual rehabilitation technique with a systematic postural approach based on physical and mathematical concepts, determines functional recovery through the correction of body symmetry [31] analyzing their state of back health, flexibility, pain, and steps speed. Design: Double-blind randomized controlled trial. Methods: A total of 20 players with LBP from the second soccer division league were allocated equally to the experimental and control groups (n=10. This method is a safe and adaptive treatment because it is based on static stretching [25]. In other words, a close relationship is observed between the mind and the body within the Mézières method, and this means that the treatment of physical, functional, and psychological aspects can improve the attitude, condition, and quality of life of the athlete with LBP [29]. Lena et al have stated in their studies that the benefits of this method are observed in a long period of treatment (24 weeks) because the morphological changes of muscle imbalance should be corrected again. In several articles, this method has been used to treat the back pain of athletes to retrain the posture of the whole body individually, and the results showed that this method could initially increase the flexibility of the back and ultimately reduce the disability and back pain of the athletes and also improves the quality of life and performance in athletes [25, 29, 31] analyzing their state of back health, flexibility, pain, and steps speed. Design: Double-blind randomized controlled trial. Methods: A total of 20 players with LBP from the second soccer division league were allocated equally to the experimental and control groups (n=10. On the other hand, movement improves the size and function of trunk muscles in elite soccer players with and without LBP [36] optimize rehabilitation, and enhance performance is a priority for practitioners. Different exercises produce different effects on neuromuscular performance. Clarity of the purpose of a prescribed exercise is central to a successful outcome. Spinal exercises need to be classified according to the objective of the exercise and planned physical outcome. Objective: To define the modifiable spinal abilities that underpin optimal function during skilled athletic performance, clarify the effect of spinal pain and pathologic conditions, and classify spinal exercises according to the objective of the exercise and intended physical outcomes to inform training and rehabilitation. Design: Qualitative study. Data Collection and Analysis: We conducted a qualitative consensus method of 4 iterative phases. An exploratory panel carried out an extended review of the English-language literature using CINAHL, EMBASE, MEDLINE, and PubMed to identify key themes and subthemes to inform the definitions of exercise categories, physical abilities, and physical outcomes. An expert project group reviewed panel findings. A draft classification was discussed with physiotherapists (n=49. Mendis et al investigated the changes in the size of trunk and thigh muscles during movement control exercises with the help of ultrasound, and the results indicated an increase in the size of these muscles [28].
Central stability exercises are also a special method of exercise that is usually used for the central muscles of the trunk in the treatment of back problems. In these exercises, Swiss balls of different sizes are applied to train the main muscles. These exercises are fun and reduce the difficulty of rehabilitation sessions. Exercise with a Swiss ball allows the processing of motor messages to transmit the best sensory message to the muscles and create neuroplastic changes for new motor learning. Studies in this field indicate an increase in the activity of the human sensory and motor system, which leads to a decrease in the intensity of back pain and an improvement in the strength, endurance, and flexibility of the trunk muscles and directly stabilizes sports performance [26, 37, 38] we aimed to investigate the effects of Tai Chi Chuan (TCC).
Another effective method that was addressed is the Dynamic Neuromuscular Stabilization (DNS) method, as a manual and rehabilitative approach to optimizing the motor system based on the scientific principles of developmental kinesiology. Dynamic stability is achieved through precise muscle coordination by the central nervous system. This method provides a framework for understanding the mutual integration of the skeleton, joints, muscles, and nerves along the dynamic kinetic chain [39] spinal extensors, gluteals or any other musculature; rather, core stabilization is accomplished through precise coordination of these muscles and intra-abdominal pressure regulation by the central nervous system. Understanding developmental kinesiology provides a framework to appreciate the regional interdependence and the inter-linking of the skeleton, joints, musculature during movement and the importance of training both the dynamic and stabilizing function of muscles in the kinetic chain. The dynamic neuromuscular stabilization (DNS). It was also done with a particular emphasis on the quality of training, complete awareness of the body, and prevention of hyperactivity. This training process makes the peripheral mechanoreceptors participate in the actions of the trunk muscles. Finally, the results of studies in this field show that a new sports program based on the principles of dynamic neuromuscular stabilization (DNS), which targets stabilization and segmental movement in the middle part of the thoracic spine, may reduce back pain and improve the quality of sensory perception in athletes [21, 34, 39] controlled trial with blinded outcome assessors.Setting:University Hospital, Department of Rehabilitation and Sports Medicine.Participants:Twenty elite cross-country skiers aged 17 to 27 years.Interventions:Ten cross-country skiers integrated 3 types of exercise targeting segmental motion in mid-thoracic spine into their routine training practice for 2 months. The 10 controls performed routine athletic training.Main Outcome Measures:The Young Spine Questionnaire to measure intensity and frequency of back pain was completed at the start and end of study. Tactile sensory perception using 10-g Semmes-Weinstein monofilament, thermic perception using TIP THERM device, graphesthesia assessed by a touch monitor pencil, 2-point discrimination assessed by a digital caliper, and vibration perception assessed by a 128-Hz tuning fork measured in mid-thoracic spine 5 times.Results:No significant group differences in pain and sensory perception were identified at baseline. Over the 2-month study interval, repeated-measures analysis of variance revealed that the experimental group improved significantly relative to the control group on pain intensity (P=0.005 for cervical, P=0.004 for thoracic, and P=0.014 for lumbar.
Another method that was addressed in Nambi’s studies is VRT, an advanced rehabilitation method dependent on artificial intelligence and machine learning because it accelerates the motor learning process in a step-by-step feedback manner. Tasks and games are customized according to the needs of the patient and the therapist and provide the environment and activities in real-time [17, 26, 40]. It also stimulates cognitive properties through sensory feedback (auditory, visual, and tactile), activates cortical and subcortical brain neurons, and reduces the feeling of pain in the body. In addition, it improves the functional capacity and perception of athletes by providing different physical activities [41]. Studies have also shown that VRT breaks the cycle of fear of movement through pain distraction techniques and has extensive beneficial effects on pain relief [26].
The common goal in all the presented protocols was to reduce pain and improve the quality of life of the athletes. Chiropractic treatments are an alternative treatment and have a temporary effect despite the activation of muscle receptors, but it should be done by trained people, and it is better to use multifaceted programs [42]. Kinesio taping is also an alternative treatment that needs more studies to evaluate its effects because studies have shown few benefits [43]. Other previous studies that combined different rehabilitation methods showed better results when manual therapy and exercise therapy were administered to subjects [44]. Scientific communities widely investigate the benefits of exercise for the health of people with low back pain, but the results of this research cannot be generalized to all people because the individuality and the motivation to explore the movement are of a diverse nature [45]. However, definitive results in this field need more and more detailed investigations in future studies.
5. Conclusion
According to the results from the articles, it can be proved that among the therapeutic interventions used, the exercises that tried to integrate the deep and superficial muscles by correcting the person’s posture and calling the muscles correctly had the greatest effect on the balance of the muscles. They created this process with mental knowledge and complete awareness of the person and finally created factors of strength, endurance, and flexibility in tissues. What was mentioned in all the studies was the individualization of the multifaceted protocols according to the needs of the individual.
Limitations
The terms “back pain” and “back injury” are different. Sometimes, the athlete complains of pain, but during the clinical examination, the pathology of the injury is not diagnosed for him. In the studies, these two terms are not properly distinguished, which was a challenge in this study. The limitations of this study include lack of inclusion of studies other than English and articles that were not presented as RCTs.
Ethical Considerations
Compliance with ethical guidelines
There were no ethical considerations to be considered in this research.
Funding
This research did not receive any grant from funding agencies in the public, commercial, or non-profit sectors.
Authors' contributions
Conceptualization, investigation, resources and funding acquisition: All authors; Methodology: Behrouz Jafari; Writing original draft: Behrouz Jafari; Writing, reviewing, and editing: Mohammad Hosein Alizadeh and Behrouz Jafari; Supervision: Mohammad Hosein Alizadeh.
Conflict of interest
The authors declared no conflict of interest in this study.
Acknowledgments
The authors thank the researchers whose papers helped us present the results of this study.
References
- Ebrahimi Varkiani M, Ordibehesht A, Alizadeh MH, Moradi Shahpar F, Hakemi L. Incidence of low back injuries among iranian athletes in 12 disciplines of olympic sports. Physical Treatment Journal. 2021; 11(1):25-30. [DOI:10.32598/ptj.11.1.421.2]
- Michaud F, Pérez Soto M, Lugrís U, Cuadrado J. Lower back injury prevention and sensitization of hip hinge with neutral spine using wearable sensors during lifting exercises. Sensors. 2021; 21(16):5487. [DOI:10.3390/s21165487] [PMID] [PMCID]
- Hartvigsen J, Hancock MJ, Kongsted A, Louw Q, Ferreira ML, Genevay S, et al. What low back pain is and why we need to pay attention. Lancet. 2018; 391(10137):2356-67.[DOI:10.1016/S0140-6736(18)30480-X] [PMID]
- Mizoguchi Y, Akasaka K, Otsudo T, Shimada N, Naka H. Efficacy of semi-customized exercises in preventing low back pain in high school volleyball players: A randomized controlled trial. Medicine. 2022; 101(36):e30358.[DOI:10.1097/MD.0000000000030358] [PMID]
- Wilson F, Thornton JS, Wilkie K, Hartvigsen J, Vinther A, Ackerman KE, et al. 2021 consensus statement for preventing and managing low back pain in elite and subelite adult rowers. British Journal of Sports Medicine. 2021; 55(16):893-9. [DOI:10.1136/bjsports-2020-103385] [PMID]
- Trease L, Wilkie K, Lovell G, Drew M, Hooper I. Epidemiology of injury and illness in 153 Australian international-level rowers over eight international seasons. British Journal of Sports Medicine. 2020; 54(21):1288-93. [DOI:10.1136/bjsports-2019-101402] [PMID]
- Ball JR, Harris CB, Lee J, Vives MJ. Lumbar spine injuries in sports: Review of the literature and current treatment Recommendations. Sports Medicine Open. 2019; 5(1):26. [DOI:10.1186/s40798-019-0199-7] [PMID] [PMCID]
- Assenmacher B, Schroeder GD, Patel AA. On-field management of spine and spinal cord injuries. Operative Techniques in Sports Medicine. 2013; 21(3):152-8. [DOI:10.1053/j.otsm.2013.10.008]
- Chou R. Low back pain. Annals of Internal Medicine. 2021; 174(8):ITC113-28. [DOI:10.7326/AITC202108170] [PMID]
- Farahbakhsh F, Rostami M, Noormohammadpour P, Mehraki Zade A, Hassanmirazaei B, Faghih Jouibari M, et al. Prevalence of low back pain among athletes: A systematic review. Journal of Back and Musculoskeletal Rehabilitation. 2018; 31(5):901-16. [DOI:10.3233/BMR-170941] [PMID]
- Hangai M, Kaneoka K, Okubo Y, Miyakawa S, Hinotsu S, Mukai N, et al. Relationship between low back pain and competitive sports activities during youth. The American Journal of Sports Medicine. 2010; 38(4):791-6. [DOI:10.1177/0363546509350297] [PMID]
- Stanton TR, Latimer J, Maher CG, Hancock MJ. How do we define the condition 'recurrent low back pain'? A systematic review. European Spine Journal. 2010; 19(4):533-9. [DOI:10.1007/s00586-009-1214-3] [PMID] [PMCID]
- Hoy D, Brooks P, Woolf A, Blyth F, March L, Bain C, Baker P, Smith E, Buchbinder R. Assessing risk of bias in prevalence studies: modification of an existing tool and evidence of interrater agreement. Journal of Clinical Epidemiology. 2012; 65(9):934-9. [DOI:10.1016/j.jclinepi.2011.11.014] [PMID]
- Mo AZ, Gjolaj JP. Axial low back pain in elite athletes. Clinics in Sports Medicine. 2021; 40(3):491-9. [DOI:10.1016/j.csm.2021.03.005] [PMID]
- Furlan AD, Pennick V, Bombardier C, van Tulder M; Editorial Board, Cochrane Back Review Group. 2009 updated method guidelines for systematic reviews in the Cochrane Back Review Group. Spine. 2009; 34(18):1929-41. [DOI:10.1097/BRS.0b013e3181b1c99f] [PMID]
- de Morton NA. The PEDro scale is a valid measure of the methodological quality of clinical trials: A demographic study. The Australian Journal of Physiotherapy. 2009; 55(2):129-33. [DOI:10.1016/S0004-9514(09)70043-1] [PMID]
- Nambi G, Abdelbasset WK, Elsayed SH, Alrawaili SM, Abodonya AM, Saleh AK, et al. Comparative effects of isokinetic training and virtual reality training on sports performances in university football players with chronic low back pain-randomized controlled study. Evidence-Based Complementary And Alternative Medicine. 2020; 2020:2981273.[DOI:10.1155/2020/2981273] [PMID] [PMCID]
- Ng L, Cañeiro JP, Campbell A, Smith A, Burnett A, O'Sullivan P. Cognitive functional approach to manage low back pain in male adolescent rowers: a randomised controlled trial. British Journal of Sports Medicine. 2015; 49(17):1125-31.[DOI:10.1136/bjsports-2014-093984] [PMID]
- Hides JA, Stanton WR, Mendis MD, Gildea J, Sexton MJ. Effect of motor control training on muscle size and football games missed from injury. Medicine and Science in Sports and Exercise. 2012; 44(6):1141-9. [DOI:10.1249/MSS.0b013e318244a321] [PMID]
- Roussel NA, Vissers D, Kuppens K, Fransen E, Truijen S, Nijs J, et al. Effect of a physical conditioning versus health promotion intervention in dancers: A randomized controlled trial. Manual Therapy. 2014; 19(6):562-8. [DOI:10.1016/j.math.2014.05.008] [PMID]
- Kobesova A, Andel R, Cizkova K, Kolar P, Kriz J. Can exercise targeting mid-thoracic spine segmental movement reduce back pain and improve sensory perception in cross-country skiers? Clinical Journal of Sport Medicine. 2021; 31(2):e86-94. [DOI:10.1097/JSM.0000000000000699] [PMID]
- Nambi G, Abdelbasset WK, Alqahtani BA, Alrawaili SM, Abodonya AM, Saleh AK. Isokinetic back training is more effective than core stabilization training on pain intensity and sports performances in football players with chronic low back pain: A randomized controlled trial. Medicine. 2020; 99(21):e20418. [DOI:10.1097/MD.0000000000020418] [PMID] [PMCID]
- Nambi G, Abdelbasset WK, Alsubaie SF, Moawd SA, Verma A, Saleh AK, et al. Isokinetic training - its radiographic and inflammatory effects on chronic low back pain: A randomized controlled trial. Medicine. 2020; 99(51):e23555. [DOI:10.1097/MD.0000000000023555] [PMID] [PMCID]
- Zakaria AA, Kiningham RB, Sen A. Effects of static and dynamic stretching on injury prevention in high school soccer athletes: A randomized trial. Journal of Sport Rehabilitation. 2015; 24(3):229-35. [DOI:10.1123/jsr.2013-0114] [PMID]
- Lena O, Todri J, Todri A, Papajorgji P, Martínez-Fuentes J. A randomized controlled trial concerning the implementation of the postural Mézières treatment in elite athletes with low back pain. Postgraduate Medicine. 2022; 134(6):559-72. [DOI:10.1080/00325481.2022.2089464] [PMID]
- Nambi G, Abdelbasset WK, Alsubaie SF, Saleh AK, Verma A, Abdelaziz MA, et al. Short-term psychological and hormonal effects of virtual reality training on chronic low back pain in soccer players. Journal of Sport Rehabilitation. 2021; 30(6):884-93. [DOI:10.1123/jsr.2020-0075] [PMID]
- Grabow L, Young JD, Byrne JM, Granacher U, Behm DG. Unilateral rolling of the foot did not affect non-local range of motion or balance. Journal of Sports Science & Medicine. 2017; 16(2):209-18. [PMID] [PMCID]
- Mendis MD, Hides JA. Effect of motor control training on hip muscles in elite football players with and without low back pain. Journal of Science and Medicine in Sport. 2016; 19(11):866-71.[DOI:10.1016/j.jsams.2016.02.008] [PMID]
- Lena O, Todri J, Todri A, Gil JLM, Gallego MG. The effectiveness of the mézières method in elite rhythmic gymnastics athletes with low back pain: A randomized controlled trial. Journal of Sport Rehabilitation. 2019; 29(7):913-9. [DOI:10.1123/jsr.2019-0204] [PMID]
- Suzuki K, Akasaka K, Otsudo T, Sawada Y, Hattori H, Hasebe Y, et al. Effects of functional movement screen training in high-school baseball players: A randomized controlled clinical trial. Medicine. 2021; 100(14):e25423. [DOI:10.1097/MD.0000000000025423] [PMID] [PMCID]
- Lena O, Todri J, Todri A, Azorín LF, Fuentes JM, Papajorgji P, et al. The mézières method as a novel treatment for elite spanish second-division soccer league players with low back pain: A randomized controlled trial. Journal of Sport Rehabilitation. 2022; 31(4):398-413. [DOI:10.1123/jsr.2021-0047] [PMID]
- Merino-Marban R, Smuka I, Romero-Ramos O, Fernandez-Rodriguez E, Mayorga-Vega D. Acute and 24 h effect of kinesio taping on lower back muscle soreness during continued practice of cross-country skiing among collegiate students. A double-blind, randomized, placebo-controlled trial. Journal of Sports Sciences. 2021; 39(21):2427-33. [DOI:10.1080/02640414.2021.1936958] [PMID]
- Hoskins W, Pollard H. Retraction: The effect of a sports chiropractic manual therapy intervention on the prevention of back pain, hamstring and lower limb injuries in semi-elite Australian Rules footballers: A randomized controlled trial. BMC Musculoskeletal Disorders. 2011; 12:200.[DOI:10.1186/1471-2474-12-200] [PMID] [PMCID]
- Kobesova A, Davidek P, Morris CE, Andel R, Maxwell M, Oplatkova L, et al. Functional postural-stabilization tests according to Dynamic Neuromuscular Stabilization approach: Proposal of novel examination protocol. Journal of Bodywork and Movement Therapies. 2020; 24(3):84-95. [DOI:10.1016/j.jbmt.2020.01.009] [PMID]
- Smith CE, Nyland J, Caudill P, Brosky J, Caborn DN. Dynamic trunk stabilization: A conceptual back injury prevention program for volleyball athletes. The Journal of Orthopaedic and Sports Physical Therapy. 2008; 38(11):703-20. [DOI:10.2519/jospt.2008.2814] [PMID]
- Spencer S, Wolf A, Rushton A. Spinal-exercise prescription in sport: Classifying physical training and rehabilitation by intention and outcome. Journal of Athletic Training. 2016; 51(8):613-28. [DOI:10.4085/1062-6050-51.10.03] [PMID] [PMCID]
- Zou L, Zhang Y, Liu Y, Tian X, Xiao T, Liu X, et al. The Effects of tai chi chuan versus core stability training on lower-limb neuromuscular function in aging individuals with non-specific chronic lower back pain. Medicina. 2019; 55(3):60.[DOI:10.3390/medicina55030060] [PMID] [PMCID]
- Javadian Y, Akbari M, Talebi G, Taghipour-Darzi M, Janmohammadi N. Influence of core stability exercise on lumbar vertebral instability in patients presented with chronic low back pain: A randomized clinical trial. Caspian Journal of Internal Medicine. 2015; 6(2):98-102. [PMID] [PMCID]
- Frank C, Kobesova A, Kolar P. Dynamic neuromuscular stabilization & sports rehabilitation. International Journal of Sports Physical Therapy. 2013; 8(1):62-73. [PMID] [PMCID]
- Nambi G, Abdelbasset WK, Alrawaili SM, Alsubaie SF, Abodonya AM, Saleh AK. Virtual reality or isokinetic training; its effect on pain, kinesiophobia and serum stress hormones in chronic low back pain: A randomized controlled trial. Technology and Health Care. 2021; 29(1):155-66. [DOI:10.3233/THC-202301] [PMID]
- Paalanne N, Niinimäki J, Karppinen J, Taimela S, Mutanen P, Takatalo J, et al. Assessment of association between low back pain and paraspinal muscle atrophy using opposed-phase magnetic resonance imaging: A population-based study among young adults. Spine. 2011; 36(23):1961-8. [DOI:10.1097/BRS.0b013e3181fef890] [PMID]
- Coulter ID, Crawford C, Vernon H, Hurwitz EL, Khorsan R, Booth MS, et al. Manipulation and mobilization for treating chronic nonspecific neck pain: A systematic review and meta-analysis for an appropriateness panel. Pain Physician. 2019; 22(2):E55-70. [DOI:10.36076/ppj/2019.22.E55] [PMID] [PMCID]
- Luz Júnior MAD, Almeida MO, Santos RS, Civile VT, Costa LOP. Effectiveness of kinesio taping in patients with chronic nonspecific low back pain: A systematic review with meta-analysis. Spine. 2019; 44(1):68-78. [DOI:10.1097/BRS.0000000000002756] [PMID]
- Gomes-Neto M, Lopes JM, Conceição CS, Araujo A, Brasileiro A, Sousa C, Carvalho VO, Arcanjo FL. Stabilization exercise compared to general exercises or manual therapy for the management of low back pain: A systematic review and meta-analysis. Physical Therapy in Sport. 2017; 23:136-42. [DOI:10.1016/j.ptsp.2016.08.004] [PMID]
- Ahlsen B, Engebretsen E, Nicholls D, Mengshoel AM. The singular patient in patient-centred care: Physiotherapists' accounts of treatment of patients with chronic muscle pain. Medical Humanities. 2020; 46(3):226-33. [DOI:10.1136/medhum-2018-011603] [PMID]
Type of Study: Research |
Subject:
Sport injury and corrective exercises
Received: 2022/12/6 | Accepted: 2023/03/4 | Published: 2022/10/20
Received: 2022/12/6 | Accepted: 2023/03/4 | Published: 2022/10/20
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
