Sun, Aug 25, 2024
Volume 12, Issue 4 (Autumn 2022)
PTJ 2022, 12(4): 213-232 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Mahdavi S, Minoonejhad H, Rajabi R, Sheikhhoseini R. Improving Lower Extremity Functional Indices of People With Dynamic Knee Valgus With Therapeutic Exercises: A Systematic Review and Meta-analysis. PTJ 2022; 12 (4) :213-232
URL: http://ptj.uswr.ac.ir/article-1-537-en.html
URL: http://ptj.uswr.ac.ir/article-1-537-en.html



1- Department of Health and Sport Medicine, Faculty of Physical Education and Sport Sciences, University of Tehran, Tehran, Iran.
2- Department of Corrective Exercise and Sport Injury, Faculty of Physical Education and Sport Sciences, Allameh Tabataba’i University, Tehran, Iran.
2- Department of Corrective Exercise and Sport Injury, Faculty of Physical Education and Sport Sciences, Allameh Tabataba’i University, Tehran, Iran.
Full-Text [PDF 928 kb]
(598 Downloads)
| Abstract (HTML) (1830 Views)

Study characteristics
The seven investigations reported 250 individuals, 200 of whom participated in different sports (football, soccer, handball, and basketball), 26 were university/college physical education students, and 24 were inactive. One research failed to disclose the gender distribution of the intervention and control groups [15]. According to the researchers that provided this information, 118 men and 52 women participated. Several types of exercise training had been prescribed in the studies, including two studies on neuromuscular training [15, 31], one study on a comprehensive corrective exercise program [20], one study on plyometric training [6], one study on jump-landing [32] and one study on strengthening training [8] and one studies on a combination of closed-kinematic chain, corrective, plyometric, and balance-challenging exercises [33]. Training lessons were placed 2-4 times each week, and interventions lasted 6–10 weeks. The control group members either engaged in the regular exercise program or did not exercise. As a screening test, DKV was assessed using several tests, including single-leg squat in 3 studies [8, 20, 33], double-leg squat in 2 studies [31, 32], single-leg landing in 1 study [6], and drop vertical jump in 1 study [15] by motion capture data analysis, as illustrated in Table 3.


Risk of bias assessment
Five of the seven investigations were assigned a low risk of bias rating (LR), whereas two were assigned a high risk of bias grade. Table 4 presents the outcomes of the quality assessment.

3. Results
Results of individual studies
Table 5 presents individual research results as simple between-group (intervention vs. control) effect sizes for every investigation and the 95% confidence interval at posttest for each study relying on raw data.

Results of syntheses
The review study’s findings suggested that various exercise interventions may be useful for enhancing dynamic balance (SD=0.93 degrees, 95%CI: 0.54-1.32, P<0.001) and functional performance (Hedge’s g=1.695, 95% CI=1.22-2.17, Z=6.99, P<0.001) in a total of 250 DKV participants.
Description of the selected variables
Balance: One studies had used the bass stick test to evaluate static balance [31] and four studies used YBT to evaluate dynamic balance [6, 8, 31, 33].
Performance: Four studies reported data on performance outcomes using the following scales, Boddington’s basketball jump shooting accuracy test [32], quality of one-leg squat performance [20] and vertical jump height [6], and the 1-leg hop test [15].
Data synthesis
The meta-analysis was conducted by applying the standardized mean differences and Hedge’s g determined at the beginning and end of the exercise protocols for balance and performance for the intervention and control groups.
Static balance
The effectiveness of therapeutic exercise programs on static balance was investigated in just one research [31]. Compared to the control group, the intervention program substantially enhanced the training group’s static balance (P≤0.01).
Dynamic balance
Y-balance test (YBT) (composite score)
Meta-analysis was performed on four eligible studies [6, 8, 31, 33] that had obtained data on YBT among a total of 112 participants with DKV. The pooled estimated standard difference was 0.93 degrees (95%CI: 0.54- 1.32, P<0.001). The Y-balance composite score was significantly increased in exercise groups compared to controls (Figure 2).






Full-Text: (551 Views)
1. Introduction
The inappropriate movement pattern of dynamic knee valgus (DKV) appears to be a risk factor for lower extremity injury. Lower extremity injuries appear to be common in sports that require a high frequency of jump-landing movements [1]. Anterior cruciate ligament (ACL) sprains and Achilles tendinitis are ligamentous injuries linked to these jump-landing movements [2]. Other non-ligamentous injuries, including bone and cartilaginous injuries, may result from the jump landing movements [3]. Incorrect landing movement patterns, such as reduced knee and hip flexion, increased hip internal rotation, and knee valgus, could enhance the risk of injury [4, 5]. It indicates that DKV accurately predicts acute injuries and frequent lower extremity usage. The adduction and internal rotation of the femur, the abduction of the knee, the anterior translation of the tibia, the external rotation of the tibia, and the eversion of the ankle indicate the modified hip, knee, and ankle kinematics related to inappropriate patterns of lower limb function [6]. The pattern indicates knee valgus movement by demonstrating medial knee displacement above the line connecting the foot and the thigh [7]. Balance loss, particularly dynamic balance, is another factor that increases the risk of lower extremity injuries. A practical test to determine dynamic balance is indeed the Y-balance test (YBT). In different populations, a lower YBT score is linked to lower extremity injuries [8]. Additionally, a DKV, which has decreased neuromuscular efficiency, can interfere with dynamic balance control [9].
Correcting improper movement patterns may help avoid ACL and other lower extremity injuries, both of which have modifiable risk factors [10]. Individuals with low movement quality benefit most from exercise programs, and investigators have worked to develop efficient training programs and cutting-edge techniques to enhance it [6]. The efficiency of plyometric exercises as one of the tools for enhancing physical and movement fitness has been the subject of some current studies in this field. Plyometric training programs appear to reduce the knee valgus angle and the ground reaction forces by emphasizing knee alignment and superior landing methods throughout vigorous activities [11]. Additionally, by using fast forces, such training enhances feedback and feed-forward activities while matching muscle and joint receptors [12].
In this regard, other researchers have noticed the improvement of knee biomechanics by strengthening hip muscles [13]. The most proximal joint of the lower extremities in the closed kinetic chain, the hip, seems to be the key to improving knee control. This is corroborated by research linking hip muscle strength to a non-contact ACL injury [14]. More particularly, higher knee valgus angles throughout landing are all related to muscle weakness in hip abduction, external rotation, and extension. Strengthening hip muscles to properly control the femur may avoid significant valgus deviation by keeping the distal femur in a more neutral alignment with the proximal tibia at the knee [13].
Some research suggests that preventative training can be effective for common sports injuries to the lower extremities, such as the ankle, knee, or ACL [15]. Neuromuscular training (NMT) seeks to reduce knee valgus angles and enhance single-leg stability and balance, two variables that have a significant impact on injury prevention. In addition, it is unclear to what degree the various components of such programs contribute to reducing injury risk [16]. It significantly reduces peak landing forces, knee valgus, and varus torques, and improves single-limb stability, balance, knee valgus angle, and landing error score [15]. Some research findings on the efficacy of dynamic resistance and/or neuromuscular (plyometric, agility, balance) exercise protocols have demonstrated that such interventions can improve jump landing movement mechanics in controlled settings [17]. In contrast, another investigation demonstrates muscular strength but no changes in lower extremity movement mechanics [18].
Research suggests that exercise protocols can positively improve the lower extremity functional indices of patients with DKV; nevertheless, the efficacy of certain exercise protocols seems controversial [19, 20]. The discrepancies in outcomes between investigations can be partially attributable to variations in the exercises, exercise intensity and or duration, and the characteristics of the study participants.
Numerous systematic review studies have assessed how exercise may reduce DKV. In healthy individuals, Cashman et al. investigated the impact of external rotators or weak hip abductors on knee valgus kinematics [21]. Ford et al. in a narrative review provide insight into a hip-focused neuromuscular training strategy to enhance DKV [22]. Wilczynski et al. undertook a literature review to determine the effects of different variables and diverse exercise training techniques on DKV in single-leg movement activities [7]. The major subjects of the assessment and meta-analysis by Sahabuddin et al. (2021) were the advantages of an exercise intervention emphasizing a bottom-up (ankle-focused) or top-down (hip-focused) kinetic chain on DKV [23].
Concerning DKV, one of the primary risk factors for ACL injury, the efficacy of interventional exercises in this population is unclear. Therefore, a comprehensive evaluation with pooled meta-analysis would demonstrate these exercises’ impact on the lower extremities’ functional indices in individuals experiencing DKV. In addition, moderator variables, including participant characteristics (age, gender, and degree of physical activity) and intervention characteristics, should be investigated (duration, intensity, volume, type, etc.) A systematic review and meta-analysis assessed the impact of exercise therapy on the functional indicators of the lower extremities in patients experiencing DKV.
2. Materials and Methods
Protocol and registration
The preferred reporting items for systematic reviews and meta-analyses (PRISMA) guidelines for network meta-analysis protocols (PRISMA-P) were followed in this systematic investigation [24]. The research protocol was included in the international prospective registry of systematic reviews (PROSPERO-CRD42021264396).Also, after registering the information provided in the protocol, the sections of search strategy, main outcomes, different outcomes, risk of bias (quality) assessment, review team members, and review status at the time of the most recent submission were changed on February 10, 2022, with the supervisors’ approval.
Data sources and search strategy
Scopus, PubMed, Web of Science (WOS), Google Scholar (restricted to the first 1000 citations), and Iranian databases SID and Magiran were searched online from the oldest record until September 2021 to discover relevant studies. The Google Scholar database was searched to find articles not indexed in those databases. The final articles of research references were thoroughly examined for extra details. Each search combined free text search phrases, synonyms, and variants with medical subject headings (MeSH). The search phrases were divided into three categories. The main keywords (between each category and the other category) were merged into the databases using the Boolean “and” operator, and their synonymous keywords (within every category) were combined by applying the Boolean “or” operator (Table 1).
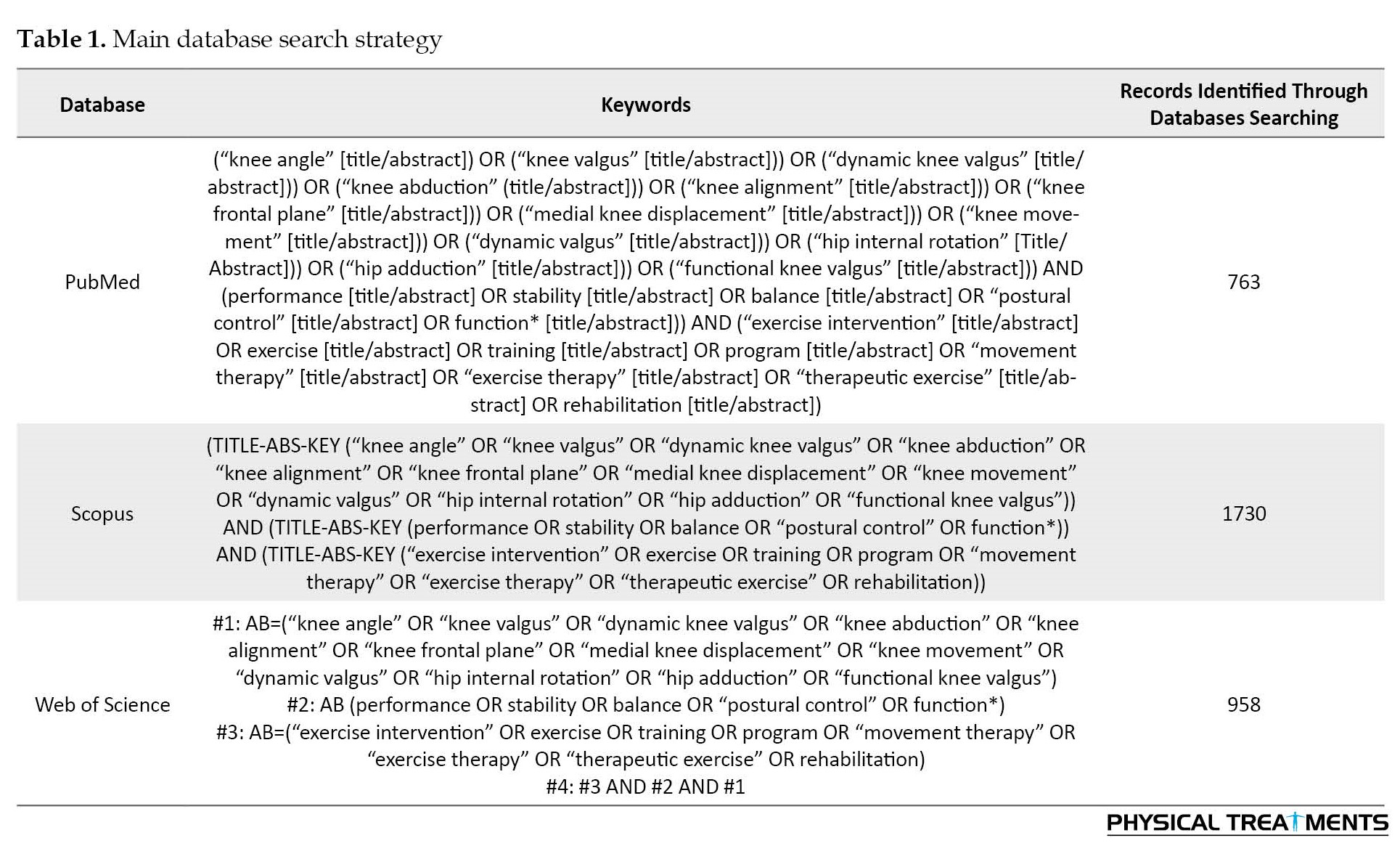
It should be noted that no filters or restrictions were set when searching the databases. All the searched citations with their abstracts were imported to the EndNote X7 software for more detailed checks.
Study selection
Inclusion criteria
1) Individuals experiencing DKV were randomly allocated to intervention and control groups regardless to their physical activity level or gender to compare the results with an active or passive control group. 2) Articles that provided the pre-test and post-test Means±SD, P, and sample sizes or had acceptable indices for estimating the effect size. 3) Full-text articles published in English/Persian peer-reviewed journals until September 2021. 3) PICOS (participants, intervention, comparators, outcome, and setting) was further described using the Cochrane approach [25], and Table 2 presents the results.

Exclusion criteria
The following study designs were excluded from this review: systematic reviews, meta-analyses, case reports and series, cross-sections, animal testing experiments, concepts, editorials, opinions, and test-tube research. Additionally, the search was not conducted on conferences, posters, letters, or texts that included only abstracts.
After deleting duplicates from the first search, two authors (SM and AF) read the titles and abstracts separately. The items were preserved following the previously specified inclusion and exclusion criteria. The complete texts of any publications that either of the two reviewers believed to be pertinent were obtained, and both independently confirmed their eligibility. Any conflicts or disagreements concerning the exclusion or inclusion of articles between two authors were resolved through discussion and exchange of opinions, or if necessary, by asking the third author (RS).
Data extraction
Before tabulation, the primary researcher (SM) retrieved study characteristics and had a secondary researcher review them (AF). Data extracted from every research encompasses the first writer’s name, publication year, sample description, the sample size for intervention and control groups, participant demographics, a screening test to determine DKV, intervention, and control description, the primary utilized tools and methods, the primary outcomes of the retrieved studies, and each study’s quality assessment score. It should be mentioned that if the data was unclear or the published articles could not be downloaded or available, researchers contacted the corresponding author or the first author of the article by email to receive the missing or additional information.
Quality assessment
Two reviewers (SM and AF) applied the most current version of the Downs and Black quality assessment to estimate the risk of bias in certain investigations. The checklist has previously demonstrated high reliability and validity [26]. The modified list contains 23 questions from the original checklist, items 1-7, 10 from “reporting”; items 11 and 12 from “external validity”; items 14-16, 18-20 from “internal validity-bias; items 21-26 from “internal validity-selection bias; item 27 from “power.” “Were appropriate power calculations reported?” was changed to item 27. Then the rating went from 0 to 5 to 0 or 1. (Appendix 1).
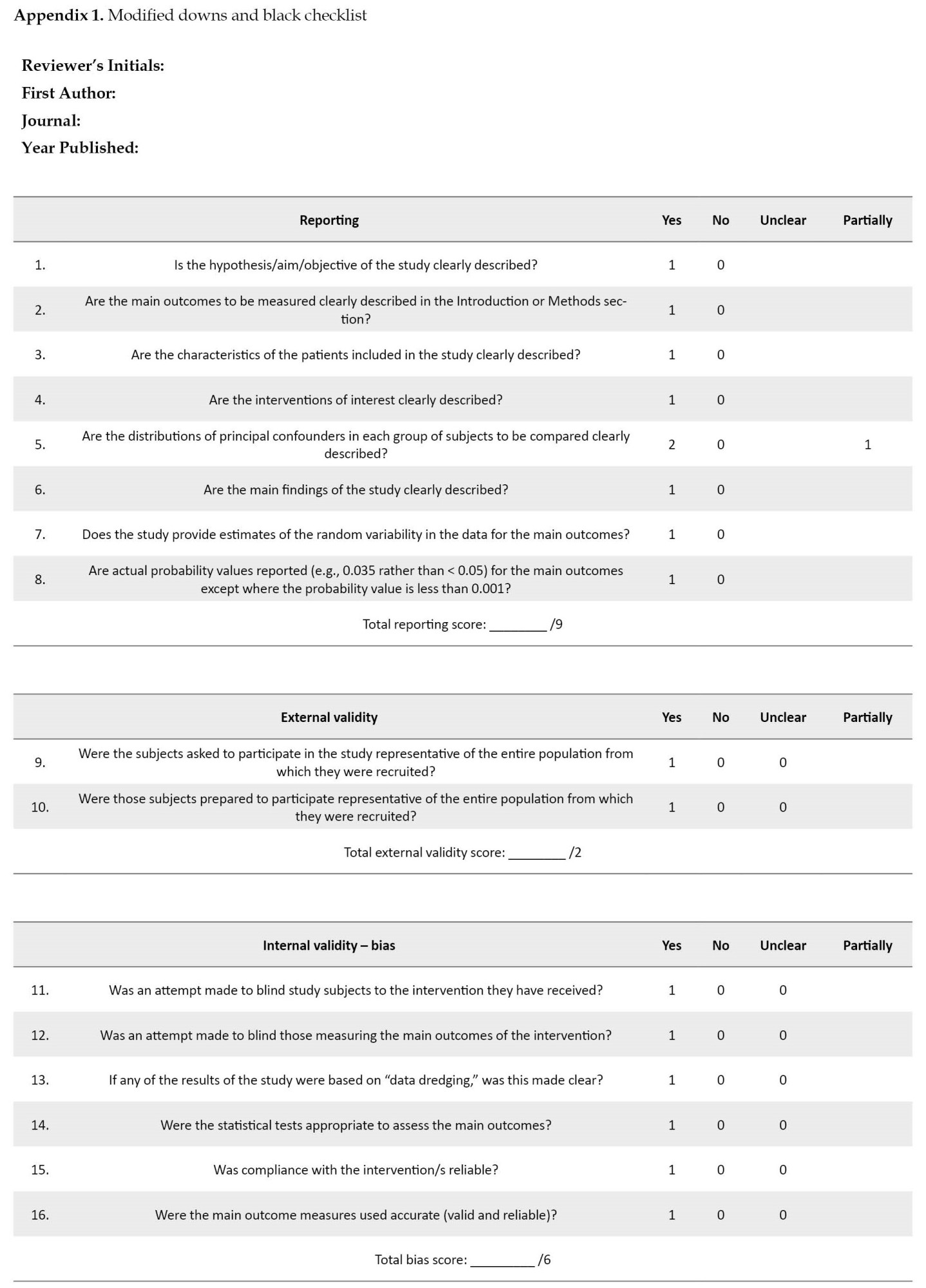

If a preliminary power analysis was performed, investigations were assigned a score of “1.” [27]. On a scale from 1 to 24, the modified Downs and Black quality index was graded. The risk of bias was determined to be low for investigations with a score of 15.6 or above (65%) and high for those below this level [28]. A consensus conference was held to reconcile the disparity between the two evaluators’ ratings. Without unanimity, a third reviewer was contacted (RS).
Level of evidence
Van Tulder et al. [29] defined the degree of evidence for every variable [28].
1. Pooled data from three or more research, including at least two investigations with minimal bias and homogeneity (P>0.05), can provide strong evidence. A significant or non-significant pool may or may not support the analysis.
2. Strong evidence shows that since multiple investigations with a high risk of bias that appears to be homogenous (P>0.05) or at least one research with a low risk of bias that is statistically heterogeneous (P<0.05) yield statistically significant pooled results.
3. Evidence is limited whether it comes from single research with a low risk of bias or from many investigations with a high risk of bias and statistical heterogeneity (P<0.05).
4. The results of a single study provide very limited evidence with a high risk of bias.
5. Conflicting evidence is provided by statistically diverse, non-significant pooled data from several studies of varied quality that are inconsistent (P<0.05).
Statistical analysis
The required information was obtained from qualified research (including pre-test and post-test Mean±SD, P, sample sizes, and possible Mean differences). The study findings were pooled utilizing a random-effects meta-analysis model and the forest plot of standard differences in means and estimated the standardized Hedge’s g effect size with a 95% confidence interval. Q-test was employed to examine data heterogeneity, whereas I2 was utilized to evaluate the extent of any possible data heterogeneity. When data heterogeneity was observed, a subgroup analysis was performed to evaluate whether gender influenced the meta-results. Publication bias was evaluated using Egger’s tests and funnel plots. The trim-and-fill method was employed to evaluate how additional random trials may affect the results. Comprehensive meta-analysis (CMA) software version 3 was employed for statistical analysis (Biostat Inc, Englewood, New Jersey)
3. Results
Search results
The database search yielded 3451 references. After eliminating duplicate references, 242 specific references were evaluated; 15 people were selected for full-text examination. During the review process, 19 more relevant papers were found in reference lists and other sources, including eligible research found in citations and searches of the Google Scholar database. Twenty-seven of the 34 full-text articles were discarded, while seven met the inclusion criteria. One study was eligible for inclusion in the review but did not report sufficient data [30]. Despite phone calls and sending several emails to the corresponding author, the necessary data was not sent to us, and we had to remove this article from our study. The PRISMA diagram displays the research selection procedure in Figure 1.
The inappropriate movement pattern of dynamic knee valgus (DKV) appears to be a risk factor for lower extremity injury. Lower extremity injuries appear to be common in sports that require a high frequency of jump-landing movements [1]. Anterior cruciate ligament (ACL) sprains and Achilles tendinitis are ligamentous injuries linked to these jump-landing movements [2]. Other non-ligamentous injuries, including bone and cartilaginous injuries, may result from the jump landing movements [3]. Incorrect landing movement patterns, such as reduced knee and hip flexion, increased hip internal rotation, and knee valgus, could enhance the risk of injury [4, 5]. It indicates that DKV accurately predicts acute injuries and frequent lower extremity usage. The adduction and internal rotation of the femur, the abduction of the knee, the anterior translation of the tibia, the external rotation of the tibia, and the eversion of the ankle indicate the modified hip, knee, and ankle kinematics related to inappropriate patterns of lower limb function [6]. The pattern indicates knee valgus movement by demonstrating medial knee displacement above the line connecting the foot and the thigh [7]. Balance loss, particularly dynamic balance, is another factor that increases the risk of lower extremity injuries. A practical test to determine dynamic balance is indeed the Y-balance test (YBT). In different populations, a lower YBT score is linked to lower extremity injuries [8]. Additionally, a DKV, which has decreased neuromuscular efficiency, can interfere with dynamic balance control [9].
Correcting improper movement patterns may help avoid ACL and other lower extremity injuries, both of which have modifiable risk factors [10]. Individuals with low movement quality benefit most from exercise programs, and investigators have worked to develop efficient training programs and cutting-edge techniques to enhance it [6]. The efficiency of plyometric exercises as one of the tools for enhancing physical and movement fitness has been the subject of some current studies in this field. Plyometric training programs appear to reduce the knee valgus angle and the ground reaction forces by emphasizing knee alignment and superior landing methods throughout vigorous activities [11]. Additionally, by using fast forces, such training enhances feedback and feed-forward activities while matching muscle and joint receptors [12].
In this regard, other researchers have noticed the improvement of knee biomechanics by strengthening hip muscles [13]. The most proximal joint of the lower extremities in the closed kinetic chain, the hip, seems to be the key to improving knee control. This is corroborated by research linking hip muscle strength to a non-contact ACL injury [14]. More particularly, higher knee valgus angles throughout landing are all related to muscle weakness in hip abduction, external rotation, and extension. Strengthening hip muscles to properly control the femur may avoid significant valgus deviation by keeping the distal femur in a more neutral alignment with the proximal tibia at the knee [13].
Some research suggests that preventative training can be effective for common sports injuries to the lower extremities, such as the ankle, knee, or ACL [15]. Neuromuscular training (NMT) seeks to reduce knee valgus angles and enhance single-leg stability and balance, two variables that have a significant impact on injury prevention. In addition, it is unclear to what degree the various components of such programs contribute to reducing injury risk [16]. It significantly reduces peak landing forces, knee valgus, and varus torques, and improves single-limb stability, balance, knee valgus angle, and landing error score [15]. Some research findings on the efficacy of dynamic resistance and/or neuromuscular (plyometric, agility, balance) exercise protocols have demonstrated that such interventions can improve jump landing movement mechanics in controlled settings [17]. In contrast, another investigation demonstrates muscular strength but no changes in lower extremity movement mechanics [18].
Research suggests that exercise protocols can positively improve the lower extremity functional indices of patients with DKV; nevertheless, the efficacy of certain exercise protocols seems controversial [19, 20]. The discrepancies in outcomes between investigations can be partially attributable to variations in the exercises, exercise intensity and or duration, and the characteristics of the study participants.
Numerous systematic review studies have assessed how exercise may reduce DKV. In healthy individuals, Cashman et al. investigated the impact of external rotators or weak hip abductors on knee valgus kinematics [21]. Ford et al. in a narrative review provide insight into a hip-focused neuromuscular training strategy to enhance DKV [22]. Wilczynski et al. undertook a literature review to determine the effects of different variables and diverse exercise training techniques on DKV in single-leg movement activities [7]. The major subjects of the assessment and meta-analysis by Sahabuddin et al. (2021) were the advantages of an exercise intervention emphasizing a bottom-up (ankle-focused) or top-down (hip-focused) kinetic chain on DKV [23].
Concerning DKV, one of the primary risk factors for ACL injury, the efficacy of interventional exercises in this population is unclear. Therefore, a comprehensive evaluation with pooled meta-analysis would demonstrate these exercises’ impact on the lower extremities’ functional indices in individuals experiencing DKV. In addition, moderator variables, including participant characteristics (age, gender, and degree of physical activity) and intervention characteristics, should be investigated (duration, intensity, volume, type, etc.) A systematic review and meta-analysis assessed the impact of exercise therapy on the functional indicators of the lower extremities in patients experiencing DKV.
2. Materials and Methods
Protocol and registration
The preferred reporting items for systematic reviews and meta-analyses (PRISMA) guidelines for network meta-analysis protocols (PRISMA-P) were followed in this systematic investigation [24]. The research protocol was included in the international prospective registry of systematic reviews (PROSPERO-CRD42021264396).Also, after registering the information provided in the protocol, the sections of search strategy, main outcomes, different outcomes, risk of bias (quality) assessment, review team members, and review status at the time of the most recent submission were changed on February 10, 2022, with the supervisors’ approval.
Data sources and search strategy
Scopus, PubMed, Web of Science (WOS), Google Scholar (restricted to the first 1000 citations), and Iranian databases SID and Magiran were searched online from the oldest record until September 2021 to discover relevant studies. The Google Scholar database was searched to find articles not indexed in those databases. The final articles of research references were thoroughly examined for extra details. Each search combined free text search phrases, synonyms, and variants with medical subject headings (MeSH). The search phrases were divided into three categories. The main keywords (between each category and the other category) were merged into the databases using the Boolean “and” operator, and their synonymous keywords (within every category) were combined by applying the Boolean “or” operator (Table 1).
It should be noted that no filters or restrictions were set when searching the databases. All the searched citations with their abstracts were imported to the EndNote X7 software for more detailed checks.
Study selection
Inclusion criteria
1) Individuals experiencing DKV were randomly allocated to intervention and control groups regardless to their physical activity level or gender to compare the results with an active or passive control group. 2) Articles that provided the pre-test and post-test Means±SD, P, and sample sizes or had acceptable indices for estimating the effect size. 3) Full-text articles published in English/Persian peer-reviewed journals until September 2021. 3) PICOS (participants, intervention, comparators, outcome, and setting) was further described using the Cochrane approach [25], and Table 2 presents the results.
Exclusion criteria
The following study designs were excluded from this review: systematic reviews, meta-analyses, case reports and series, cross-sections, animal testing experiments, concepts, editorials, opinions, and test-tube research. Additionally, the search was not conducted on conferences, posters, letters, or texts that included only abstracts.
After deleting duplicates from the first search, two authors (SM and AF) read the titles and abstracts separately. The items were preserved following the previously specified inclusion and exclusion criteria. The complete texts of any publications that either of the two reviewers believed to be pertinent were obtained, and both independently confirmed their eligibility. Any conflicts or disagreements concerning the exclusion or inclusion of articles between two authors were resolved through discussion and exchange of opinions, or if necessary, by asking the third author (RS).
Data extraction
Before tabulation, the primary researcher (SM) retrieved study characteristics and had a secondary researcher review them (AF). Data extracted from every research encompasses the first writer’s name, publication year, sample description, the sample size for intervention and control groups, participant demographics, a screening test to determine DKV, intervention, and control description, the primary utilized tools and methods, the primary outcomes of the retrieved studies, and each study’s quality assessment score. It should be mentioned that if the data was unclear or the published articles could not be downloaded or available, researchers contacted the corresponding author or the first author of the article by email to receive the missing or additional information.
Quality assessment
Two reviewers (SM and AF) applied the most current version of the Downs and Black quality assessment to estimate the risk of bias in certain investigations. The checklist has previously demonstrated high reliability and validity [26]. The modified list contains 23 questions from the original checklist, items 1-7, 10 from “reporting”; items 11 and 12 from “external validity”; items 14-16, 18-20 from “internal validity-bias; items 21-26 from “internal validity-selection bias; item 27 from “power.” “Were appropriate power calculations reported?” was changed to item 27. Then the rating went from 0 to 5 to 0 or 1. (Appendix 1).
If a preliminary power analysis was performed, investigations were assigned a score of “1.” [27]. On a scale from 1 to 24, the modified Downs and Black quality index was graded. The risk of bias was determined to be low for investigations with a score of 15.6 or above (65%) and high for those below this level [28]. A consensus conference was held to reconcile the disparity between the two evaluators’ ratings. Without unanimity, a third reviewer was contacted (RS).
Level of evidence
Van Tulder et al. [29] defined the degree of evidence for every variable [28].
1. Pooled data from three or more research, including at least two investigations with minimal bias and homogeneity (P>0.05), can provide strong evidence. A significant or non-significant pool may or may not support the analysis.
2. Strong evidence shows that since multiple investigations with a high risk of bias that appears to be homogenous (P>0.05) or at least one research with a low risk of bias that is statistically heterogeneous (P<0.05) yield statistically significant pooled results.
3. Evidence is limited whether it comes from single research with a low risk of bias or from many investigations with a high risk of bias and statistical heterogeneity (P<0.05).
4. The results of a single study provide very limited evidence with a high risk of bias.
5. Conflicting evidence is provided by statistically diverse, non-significant pooled data from several studies of varied quality that are inconsistent (P<0.05).
Statistical analysis
The required information was obtained from qualified research (including pre-test and post-test Mean±SD, P, sample sizes, and possible Mean differences). The study findings were pooled utilizing a random-effects meta-analysis model and the forest plot of standard differences in means and estimated the standardized Hedge’s g effect size with a 95% confidence interval. Q-test was employed to examine data heterogeneity, whereas I2 was utilized to evaluate the extent of any possible data heterogeneity. When data heterogeneity was observed, a subgroup analysis was performed to evaluate whether gender influenced the meta-results. Publication bias was evaluated using Egger’s tests and funnel plots. The trim-and-fill method was employed to evaluate how additional random trials may affect the results. Comprehensive meta-analysis (CMA) software version 3 was employed for statistical analysis (Biostat Inc, Englewood, New Jersey)
3. Results
Search results
The database search yielded 3451 references. After eliminating duplicate references, 242 specific references were evaluated; 15 people were selected for full-text examination. During the review process, 19 more relevant papers were found in reference lists and other sources, including eligible research found in citations and searches of the Google Scholar database. Twenty-seven of the 34 full-text articles were discarded, while seven met the inclusion criteria. One study was eligible for inclusion in the review but did not report sufficient data [30]. Despite phone calls and sending several emails to the corresponding author, the necessary data was not sent to us, and we had to remove this article from our study. The PRISMA diagram displays the research selection procedure in Figure 1.
Study characteristics
The seven investigations reported 250 individuals, 200 of whom participated in different sports (football, soccer, handball, and basketball), 26 were university/college physical education students, and 24 were inactive. One research failed to disclose the gender distribution of the intervention and control groups [15]. According to the researchers that provided this information, 118 men and 52 women participated. Several types of exercise training had been prescribed in the studies, including two studies on neuromuscular training [15, 31], one study on a comprehensive corrective exercise program [20], one study on plyometric training [6], one study on jump-landing [32] and one study on strengthening training [8] and one studies on a combination of closed-kinematic chain, corrective, plyometric, and balance-challenging exercises [33]. Training lessons were placed 2-4 times each week, and interventions lasted 6–10 weeks. The control group members either engaged in the regular exercise program or did not exercise. As a screening test, DKV was assessed using several tests, including single-leg squat in 3 studies [8, 20, 33], double-leg squat in 2 studies [31, 32], single-leg landing in 1 study [6], and drop vertical jump in 1 study [15] by motion capture data analysis, as illustrated in Table 3.
Risk of bias assessment
Five of the seven investigations were assigned a low risk of bias rating (LR), whereas two were assigned a high risk of bias grade. Table 4 presents the outcomes of the quality assessment.
3. Results
Results of individual studies
Table 5 presents individual research results as simple between-group (intervention vs. control) effect sizes for every investigation and the 95% confidence interval at posttest for each study relying on raw data.
Results of syntheses
The review study’s findings suggested that various exercise interventions may be useful for enhancing dynamic balance (SD=0.93 degrees, 95%CI: 0.54-1.32, P<0.001) and functional performance (Hedge’s g=1.695, 95% CI=1.22-2.17, Z=6.99, P<0.001) in a total of 250 DKV participants.
Description of the selected variables
Balance: One studies had used the bass stick test to evaluate static balance [31] and four studies used YBT to evaluate dynamic balance [6, 8, 31, 33].
Performance: Four studies reported data on performance outcomes using the following scales, Boddington’s basketball jump shooting accuracy test [32], quality of one-leg squat performance [20] and vertical jump height [6], and the 1-leg hop test [15].
Data synthesis
The meta-analysis was conducted by applying the standardized mean differences and Hedge’s g determined at the beginning and end of the exercise protocols for balance and performance for the intervention and control groups.
Static balance
The effectiveness of therapeutic exercise programs on static balance was investigated in just one research [31]. Compared to the control group, the intervention program substantially enhanced the training group’s static balance (P≤0.01).
Dynamic balance
Y-balance test (YBT) (composite score)
Meta-analysis was performed on four eligible studies [6, 8, 31, 33] that had obtained data on YBT among a total of 112 participants with DKV. The pooled estimated standard difference was 0.93 degrees (95%CI: 0.54- 1.32, P<0.001). The Y-balance composite score was significantly increased in exercise groups compared to controls (Figure 2).
To evaluate the potential for publication bias, a funnel plot was utilized. Even though publication bias can be detected in the asymmetrical funnel plot in Figure 3, Egger’s test did not reveal any statistically significant differences in the intercept’s value (intercept 1.84, P=0.452).
Nevertheless, the trim-and-fill method showed that adding a study to the left side of the plot may not significantly influence the main result. Additionally, the data had no heterogeneity (Q=1.75, P=0.626, I2=0.00%).
Y-balance test (YBT) (anterior, posteromedial, and posterolateral reach)
Four studies [6, 8, 31, 33] reported the YBT anterior, posteromedial, and posterolateral reach outcomes. Accordingly, 112 participants were included in the studies. Improvements in the YBT were consistently statistically significant across research. The improvement was particularly noteworthy for the anterior reach: 8.79 cm (95% CI=3.26-14.24; P=0.002). The investigations were not particularly consistent (Q=7.36, P=0.061, I2=59.23) despite the substantial effect size (SMD=1.01; 95% CI=0.37-1.66). The effects in the posterior-medial and -lateral directions were less than those in the anterior-medial direction (MD=5.66 and 5.13 cm; SMD=0.58 and 0.66) yet remained statistically significant (P=0.003 and 0.001, correspondingly) (Figure 4).
Y-balance test (YBT) (anterior, posteromedial, and posterolateral reach)
Four studies [6, 8, 31, 33] reported the YBT anterior, posteromedial, and posterolateral reach outcomes. Accordingly, 112 participants were included in the studies. Improvements in the YBT were consistently statistically significant across research. The improvement was particularly noteworthy for the anterior reach: 8.79 cm (95% CI=3.26-14.24; P=0.002). The investigations were not particularly consistent (Q=7.36, P=0.061, I2=59.23) despite the substantial effect size (SMD=1.01; 95% CI=0.37-1.66). The effects in the posterior-medial and -lateral directions were less than those in the anterior-medial direction (MD=5.66 and 5.13 cm; SMD=0.58 and 0.66) yet remained statistically significant (P=0.003 and 0.001, correspondingly) (Figure 4).
In addition, the data indicated no signs of heterogeneity.
In prior research, YBT demonstrated high inter-rater and intra-rater reliability. This test’s intra-rater reliability ranges between 0.85 and 0.91, inter-rater reliability ranges between 0.99 and 0.99, and the composite reach score reliability ranges between 0.91 and 0.99 [34]. Additionally, given that three high-quality studies [6, 31, 33] show the significant effects of exercise training on dynamic balance; therefore, strong evidence are observed for these findings.
Functional performance indices:
The Boddington’s basketball jump shooting accuracy test was one of the functional performance outcomes reported in one of the four studies [6, 15, 20, 32]. However, it was not included in this research due to the disparity in performance between the upper and lower extremities. Hedge’s g standardized effect size was used to examine the data since the approved research using a variety of functional performance evaluation methodologies. The results of data synthesis among 130 participants showed that attending the intervention exercises may have no significant effect on functional indexes (Hedge’s g=-0.09, 95% CI=-3.41-3.22, Z=-0.055, P=0.956) (Figure 5).
In prior research, YBT demonstrated high inter-rater and intra-rater reliability. This test’s intra-rater reliability ranges between 0.85 and 0.91, inter-rater reliability ranges between 0.99 and 0.99, and the composite reach score reliability ranges between 0.91 and 0.99 [34]. Additionally, given that three high-quality studies [6, 31, 33] show the significant effects of exercise training on dynamic balance; therefore, strong evidence are observed for these findings.
Functional performance indices:
The Boddington’s basketball jump shooting accuracy test was one of the functional performance outcomes reported in one of the four studies [6, 15, 20, 32]. However, it was not included in this research due to the disparity in performance between the upper and lower extremities. Hedge’s g standardized effect size was used to examine the data since the approved research using a variety of functional performance evaluation methodologies. The results of data synthesis among 130 participants showed that attending the intervention exercises may have no significant effect on functional indexes (Hedge’s g=-0.09, 95% CI=-3.41-3.22, Z=-0.055, P=0.956) (Figure 5).
The asymmetrical funnel plot and the non-significant outcome of Egger’s test of the intercept (intercept=-13.797, P=0.179) indicate no overt trace of publication bias (Figure 6).
Moreover, a significant value of the Q test (Q=75.136, P<0.001) and high heterogeneity index (I2=97.338) showed a high magnitude of data heterogeneity. Gender differences had a significant impact on the outcomes, according to the findings of the subgroup analysis (Hedge’s g=1.695, 95% CI=1.22-2.17, Z=6.99, P<0.001) (Figure 7).
However, since few studies were observed, subgroup analysis could not be applied to accurately assess the cause of this heterogeneity.
High validity (0.96) has been observed for the one-leg squat performance test’s ability to assess motor impairment in the lower extremities [35]. Numerous authors [36] have discovered that the 1-leg hop test has significant test-retest reliability in healthy participants (ICC: 0.92-0.96; SEM: 4.56-4.62 cm); additionally, particularly for women [37], the vertical jump height exhibits great reliability and reproducibility (0.84). Since the functional performance tests showed good validity and reliability in previous studies and given that at least one high-quality study [6] showed the positive influence of exercise training on functional outcomes in the participants with DKV, a moderate level of evidence was assigned to these findings.
4. Discussion
The efficacy of several exercise programs on people with DKV was compared in this study for the first time systematically, emphasizing how well the participants performed in functional tasks and how well they could keep their balance. The outcomes showed that exercise interventions might be effective in enhancing dynamic balance (SD mean differences=0.93 degrees, 95%CI: 0.54-1.32, P<0.001) and functional indexes (Hedge’s g=1.695, 95% CI=1.22-2.17, Z=6.99, P<0.001). Examining the impact of several moderator factors, including participant characteristics (age, gender, and degree of physical activity), intervention features, and other secondary objectives. The necessary statistical methods (subgroup analyses or meta-regressions) could not be carried out since there were insufficient investigations with comparable outcome measures. Consequently, the impacts of moderator factors are only briefly discussed in qualitative terms.
Possible underlying mechanisms regarding the effects of exercise protocols on dynamic balance in people with dynamic knee valgus (DKV):
Our research results imply that different exercise interventions can help individuals with DKV balance. The YBT seems to be a dynamic balance evaluation tool that analyzes the integration of sensorimotor subsystems [38]. Postural performance linked to dynamic balance relates to the capability to sustain body balance under difficult postural conditions (dynamic stance) [39]. Motor systems maintain homeostasis by initiating timely and appropriate reactions to varied disturbances [40]. They initiate, select, and employ motor command programs and synergies to alter the biomechanical state toward the optimal equilibrium condition [41]. Exercise interventions could modify the movement control system, which might explain some of the benefits of exercise on balance performance.
Possible underlying mechanisms regarding the effects of exercise protocols on functional performance outcomes in people with dynamic knee valgus (DKV):
Our results demonstrated that exercise interventions could improve functional performance outcomes in people with DKV. It may be due to several physiological and psychological benefits of the exercise interventions leading to improved functional outcomes [42]. For example, it has been found that exercise training may increase self-confidence and self-efficacy [43], muscular function, and joint range of motion [44], and all of them may influence the population’s functional performance outcomes. Additionally, training interventions that emphasize the effectiveness of movement control and the alignment of the lower limbs and torso may help enhance knee valgus kinematics and functional performance results [45].
Additionally, the findings of our subgroup analysis demonstrated that, in patients with DKV, gender differences had a substantial impact on functional performance outcomes. It appears that men and women have distinct neuromuscular control techniques based on the activity at hand; women prefer to activate more quadriceps muscles than men throughout lunge maneuvers [6]. After completing a simulated risky task, researchers analyzed the gender differences in medial-to-lateral quadriceps activation ratios. Men balanced the activation of the lateral and medial quadriceps; however, females stimulated the lateral quadriceps more than males. Increased anterior shear force and knee valgus may occur from an unbalanced quadriceps muscle activation ratio, especially if the lateral quadriceps are more active [46]. The diminished control of frontal plane forces at the knee can be due to the lower medial quadriceps muscle activation ratio. Knee joint compression, particularly the pressure exerted by the medial condylar contact, can influence the frontal plane regulation of DKV. Due to decreased medial joint compression, women’s knees could be particularly susceptible to medial femoral condylar lift-off from the tibial plateau and larger pressures on the ACL during deceleration of a landing or cut maneuver, which could lower passive resistance to DKV [47]. Therefore, gender differences may influence functional performance outcomes in people with DKV.
Study limitations
It is crucial to comprehend the review’s and the included research’s limitations. Only seven studies were found that examined the impact of various exercise interventions on the functional indices of the lower extremities in individuals with DKV. This research used various individuals, study designs, and functional performance metrics. Participants in the research varied regarding their gender and age, which may impact how they reacted to training interventions. The review’s interventions varied in training intensity, duration, and frequency. It was not feasible to conduct a sensitivity study to confirm the reliability of the synthesis findings or to specifically pinpoint the cause of research heterogeneities using subgroup analyses or meta-regressions due to the limited number of studies. Since we lacked the resources and or knowledge to search in other languages, we limited our search to peer-reviewed journals and publications in English and Persian. However, the influence of language bias is disputed, and its effect has not been established [48, 49]. Although our study indicated that exercise treatments had a positive effect on functional indicators, it is essential to consider the significant levels of variability in the data when extending and interpreting these results to all forms of exercise.
5. Conclusion
As a result, according to our first systematic review and meta-analysis, exercise therapies appear to be an effective strategy to enhance dynamic balance and functional performance in adults with DKV; however, these outcomes should be regarded as preliminary due to the limited number of researchers. A more comprehensive study is necessary to better guide resource allocation, even if these findings may support the application of exercise programs by physicians, coaches, and athletic trainers. Investigators should use techniques of allocation concealment and examiner and subject blinding in future research to enhance intervention design and methodology with less risk of bias.
Ethical Considerations
Compliance with ethical guidelines
This article is a meta-analysis with no human or animal sample.
Funding
The present study is taken from the PhD thesis of Solmaz Mahdavi, in Department of Health and Sport Medicine, University of Tehran, supervised by Hooman Minoonejad and Reza Rajabi and advised by Rahman Shikhhoseini.
Authors' contributions
All authors contributed in designing, running, and writing all parts of the research.
Conflict of interest
The authors declared no conflict of interest.
References
High validity (0.96) has been observed for the one-leg squat performance test’s ability to assess motor impairment in the lower extremities [35]. Numerous authors [36] have discovered that the 1-leg hop test has significant test-retest reliability in healthy participants (ICC: 0.92-0.96; SEM: 4.56-4.62 cm); additionally, particularly for women [37], the vertical jump height exhibits great reliability and reproducibility (0.84). Since the functional performance tests showed good validity and reliability in previous studies and given that at least one high-quality study [6] showed the positive influence of exercise training on functional outcomes in the participants with DKV, a moderate level of evidence was assigned to these findings.
4. Discussion
The efficacy of several exercise programs on people with DKV was compared in this study for the first time systematically, emphasizing how well the participants performed in functional tasks and how well they could keep their balance. The outcomes showed that exercise interventions might be effective in enhancing dynamic balance (SD mean differences=0.93 degrees, 95%CI: 0.54-1.32, P<0.001) and functional indexes (Hedge’s g=1.695, 95% CI=1.22-2.17, Z=6.99, P<0.001). Examining the impact of several moderator factors, including participant characteristics (age, gender, and degree of physical activity), intervention features, and other secondary objectives. The necessary statistical methods (subgroup analyses or meta-regressions) could not be carried out since there were insufficient investigations with comparable outcome measures. Consequently, the impacts of moderator factors are only briefly discussed in qualitative terms.
Possible underlying mechanisms regarding the effects of exercise protocols on dynamic balance in people with dynamic knee valgus (DKV):
Our research results imply that different exercise interventions can help individuals with DKV balance. The YBT seems to be a dynamic balance evaluation tool that analyzes the integration of sensorimotor subsystems [38]. Postural performance linked to dynamic balance relates to the capability to sustain body balance under difficult postural conditions (dynamic stance) [39]. Motor systems maintain homeostasis by initiating timely and appropriate reactions to varied disturbances [40]. They initiate, select, and employ motor command programs and synergies to alter the biomechanical state toward the optimal equilibrium condition [41]. Exercise interventions could modify the movement control system, which might explain some of the benefits of exercise on balance performance.
Possible underlying mechanisms regarding the effects of exercise protocols on functional performance outcomes in people with dynamic knee valgus (DKV):
Our results demonstrated that exercise interventions could improve functional performance outcomes in people with DKV. It may be due to several physiological and psychological benefits of the exercise interventions leading to improved functional outcomes [42]. For example, it has been found that exercise training may increase self-confidence and self-efficacy [43], muscular function, and joint range of motion [44], and all of them may influence the population’s functional performance outcomes. Additionally, training interventions that emphasize the effectiveness of movement control and the alignment of the lower limbs and torso may help enhance knee valgus kinematics and functional performance results [45].
Additionally, the findings of our subgroup analysis demonstrated that, in patients with DKV, gender differences had a substantial impact on functional performance outcomes. It appears that men and women have distinct neuromuscular control techniques based on the activity at hand; women prefer to activate more quadriceps muscles than men throughout lunge maneuvers [6]. After completing a simulated risky task, researchers analyzed the gender differences in medial-to-lateral quadriceps activation ratios. Men balanced the activation of the lateral and medial quadriceps; however, females stimulated the lateral quadriceps more than males. Increased anterior shear force and knee valgus may occur from an unbalanced quadriceps muscle activation ratio, especially if the lateral quadriceps are more active [46]. The diminished control of frontal plane forces at the knee can be due to the lower medial quadriceps muscle activation ratio. Knee joint compression, particularly the pressure exerted by the medial condylar contact, can influence the frontal plane regulation of DKV. Due to decreased medial joint compression, women’s knees could be particularly susceptible to medial femoral condylar lift-off from the tibial plateau and larger pressures on the ACL during deceleration of a landing or cut maneuver, which could lower passive resistance to DKV [47]. Therefore, gender differences may influence functional performance outcomes in people with DKV.
Study limitations
It is crucial to comprehend the review’s and the included research’s limitations. Only seven studies were found that examined the impact of various exercise interventions on the functional indices of the lower extremities in individuals with DKV. This research used various individuals, study designs, and functional performance metrics. Participants in the research varied regarding their gender and age, which may impact how they reacted to training interventions. The review’s interventions varied in training intensity, duration, and frequency. It was not feasible to conduct a sensitivity study to confirm the reliability of the synthesis findings or to specifically pinpoint the cause of research heterogeneities using subgroup analyses or meta-regressions due to the limited number of studies. Since we lacked the resources and or knowledge to search in other languages, we limited our search to peer-reviewed journals and publications in English and Persian. However, the influence of language bias is disputed, and its effect has not been established [48, 49]. Although our study indicated that exercise treatments had a positive effect on functional indicators, it is essential to consider the significant levels of variability in the data when extending and interpreting these results to all forms of exercise.
5. Conclusion
As a result, according to our first systematic review and meta-analysis, exercise therapies appear to be an effective strategy to enhance dynamic balance and functional performance in adults with DKV; however, these outcomes should be regarded as preliminary due to the limited number of researchers. A more comprehensive study is necessary to better guide resource allocation, even if these findings may support the application of exercise programs by physicians, coaches, and athletic trainers. Investigators should use techniques of allocation concealment and examiner and subject blinding in future research to enhance intervention design and methodology with less risk of bias.
Ethical Considerations
Compliance with ethical guidelines
This article is a meta-analysis with no human or animal sample.
Funding
The present study is taken from the PhD thesis of Solmaz Mahdavi, in Department of Health and Sport Medicine, University of Tehran, supervised by Hooman Minoonejad and Reza Rajabi and advised by Rahman Shikhhoseini.
Authors' contributions
All authors contributed in designing, running, and writing all parts of the research.
Conflict of interest
The authors declared no conflict of interest.
References
- Mayer C, Rühlemann A, Jäger M. [Handball injuries and their prevention (German)]. Der Orthopade. 2019; 48(12):1036-41. [DOI:10.1007/s00132-019-03822-6] [PMID]
- Wertz J, Galli M, Borchers JR. Achilles tendon rupture: Risk assessment for aerial and ground athletes. Sports Health. 2013; 5(5):407-9. [DOI:10.1177/1941738112472165] [PMID] [PMCID]
- Aerts I, Cumps E, Verhagen E, Verschueren J, Meeusen R. A systematic review of different jump-landing variables in relation to injuries. The Journal of Sports Medicine and Physical Fitness. 2013; 53(5):509-19. [PMID]
- Mirzaee F, Sheikhhoseini R, Piri H. The acute effects of one session reactive neuromuscular training on balance and knee joint position sense in female athletes with dynamic knee valgus. Acta Gymnica. 2020; 50(3):122-9. [DOI:10.5507/ag.2020.011]
- Rabin A, Levi R, Abramowitz S, Kozol Z. A new real-time visual assessment method for faulty movement patterns during a jump-landing task. Physical Therapy in Sport. 2016; 20:7-12. [DOI:10.1016/j.ptsp.2015.11.001] [PMID]
- Saki F, Madhosh M, Sedaghati P. The effect of selective plyometric training on the lower extremity functional performance indexes of female athletes with dynamic knee valgus. Physical Treatments Journals. 2019; 9(1):31-8. [DOI:10.32598/PTJ.9.1.31]
- Wilczyński B, Zorena K, Ślęzak D. Dynamic knee valgus in single-leg movement tasks. potentially modifiable factors and exercise training options. A literature review. International Journal of Environmental Research and Public Health. 2020; 17(21):8208. [DOI:10.3390/ijerph17218208] [PMID] [PMCID]
- Wilczyński B, Wąż P, Zorena K. Impact of three strengthening exercises on dynamic knee valgus and balance with poor knee control among young football players: A randomized controlled trial. Healthcare. 2021; 9(5):558. [DOI:10.3390/healthcare9050558] [PMID] [PMCID]
- Booysen MJ, Gradidge PJ, Watson E. The relationships of eccentric strength and power with dynamic balance in male footballers. Journal of Sports Sciences. 2015; 33(20):2157-65. [DOI:10.1080/02640414.2015.1064152] [PMID]
- Padua DA, Marshall SW, Boling MC, Thigpen CA, Garrett WE Jr, Beutler AI. The landing error scoring system (LESS) Is a valid and reliable clinical assessment tool of jump-landing biomechanics: The JUMP-ACL study. The American Journal of Sports Medicine. 2009; 37(10):1996-2002. [DOI:10.1177/0363546509343200] [PMID]
- Colclough A, Munro AG, Herrington LC, McMahon JJ, Comfort P. The effects of a four week jump-training program on frontal plane projection angle in female gymnasts. Physical Therapy in Sport. 2018; 30:29-33. [DOI:10.1016/j.ptsp.2017.11.003] [PMID]
- Hewett TE, Zazulak BT, Myer GD, Ford KR. A review of electromyographic activation levels, timing differences, and increased anterior cruciate ligament injury incidence in female athletes. British Journal of Sports Medicine. 2005; 39(6):347-50. [DOI:10.1136/bjsm.2005.018572] [PMID] [PMCID]
- Jackson KM, Beach TA, Andrews DM. The effect of an isometric hip muscle strength training protocol on valgus angle during a drop vertical jump in competitive female volleyball players. International Journal of Kinesiology and Sports Science. 2017; 5(4):1-9. [DOI:10.7575/aiac.ijkss.v.5n.4p.1]
- Khayambashi K, Ghoddosi N, Straub RK, Powers CM. Hip muscle strength predicts noncontact anterior cruciate ligament injury in male and female athletes: A prospective study. The American Journal of Sports Medicine. 2016; 44(2):355-61. [DOI:10.1177/0363546515616237] [PMID]
- Barendrecht M, Lezeman HC, Duysens J, Smits-Engelsman BC. Neuromuscular training improves knee kinematics, in particular in valgus aligned adolescent team handball players of both sexes. Journal of Strength and Conditioning Research. 2011; 25(3):575-84. [DOI:10.1519/JSC.0b013e3182023bc7] [PMID]
- Taube W, Gruber M, Gollhofer A. Spinal and supraspinal adaptations associated with balance training and their functional relevance. Acta Physiologica. 2008 ; 193(2):101-16.[DOI:10.1111/j.1748-1716.2008.01850.x] [PMID]
- Myer GD, Ford KR, Palumbo JP, Hewett TE. Neuromuscular training improves performance and lower-extremity biomechanics in female athletes. Journal of Strength and Conditioning Research. 2005; 19(1):51-60. [DOI:10.1519/00124278-200502000-00010] [PMID]
- Ferber R, Kendall KD, Farr L. Changes in knee biomechanics after a hip-abductor strengthening protocol for runners with patellofemoral pain syndrome. Journal of Athletic Training. 2011; 46(2):142-9. [DOI:10.4085/1062-6050-46.2.142] [PMID] [PMCID]
- Araújo VL, Souza TR, Carvalhais VODC, Cruz AC, Fonseca ST. Effects of hip and trunk muscle strengthening on hip function and lower limb kinematics during step-down task. Clinical Biomechanics. 2017; 44:28-35 [DOI:10.1016/j.clinbiomech.2017.02.012] [PMID]
- Mozafaripour E, Seidi F, Minoonejad H, Shirzad E. [Effect of 8 weeks’ comprehensive corrective exercise program on knee proprioception and quality of one leg squat performance subjects with dynamic knee valgus (Persian)]. Studies in Sport Medicine. 2019; 11(25):17-34. [DOI:10.22089/smj.2019.6608.1343]
- Cashman GE. The effect of weak hip abductors or external rotators on knee valgus kinematics in healthy subjects: A systematic review. Journal of Sport Rehabilitation. 2012; 21(3):273-84. [DOI:10.1123/jsr.21.3.273] [PMID]
- Ford KR, Nguyen AD, Dischiavi SL, Hegedus EJ, Zuk EF, Taylor JB. An evidence-based review of hip-focused neuromuscular exercise interventions to address dynamic lower extremity valgus. Open Access Journal of Sports Medicine. 2015; 6:291-303. [DOI:10.2147/OAJSM.S72432] [PMID] [PMCID]
- Sahabuddin FNA, Jamaludin NI, Amir NH, Shaharudin S. The effects of hip- and ankle-focused exercise intervention on dynamic knee valgus: A systematic review. PeerJ. 2021; 9:e11731. [DOI:10.7717/peerj.11731] [PMID] [PMCID]
- Moher D, Shamseer L, Clarke M, Ghersi D, Liberati A, Petticrew M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Systematic Reviews. 2015; 4(1):1-9. [DOI:10.1186/2046-4053-4-1]
- Higgins JP, Green S. Cochrane handbook for systematic reviews of interventions. Hoboken: John Wiley & Sons; 2008. [DOI:10.1002/9780470712184]
- Downs SH, Black N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. Journal of Epidemiology and Community Health. 1998; 52(6):377-84. [DOI:10.1136/jech.52.6.377] [PMID] [PMCID]
- Neilson V, Ward S, Hume P, Lewis G, McDaid A. Effects of augmented feedback on training jump landing tasks for ACL injury prevention: A systematic review and meta-analysis. Physical Therapy in Sport . 2019; 39:126-35. [DOI:10.1016/j.ptsp.2019.07.004] [PMID]
- Kaur M, Ribeiro DC, Theis JC, Webster KE, Sole G. Movement patterns of the knee during gait following ACL reconstruction: A systematic review and meta-analysis. Sports Medicine. 2016; 46(12):1869-95. [DOI:10.1007/s40279-016-0510-4] [PMID]
- van Tulder M, Furlan A, Bombardier C, Bouter L; Editorial Board of the Cochrane Collaboration Back Review Group. Updated method guidelines for systematic reviews in the cochrane collaboration back review group. Spine. 2003; 28(12):1290-9. [DOI:10.1097/01.BRS.0000065484.95996.AF] [PMID]
- Mohammadi H, Daneshmandi H, Alizadeh M. [Effect of corrective exercises program on strength, ROM, and performance in basketball players with dynamic knee valgus (Persian)]. Scientific Journal of Rehabilitation Medicine. 2019; 8(3):29-41. [DOI:10.22037/JRM.2019.111286.1887]
- Babagoltabar Samakoush H, Norasteh AA. [The effect of neuromuscular training program on landing position, balance, range of motion and strength of selected lower limb muscles in athletes with dynamic knee valgus defect (Persian)]. Iranian Journal of Rehabilitation Research. 2021; 8(1):45-57. [DOI:10.22034/ijrn.8.1.45]
- Ghobadi Nezhad S, Hoseini SH, Norasteh AA. Effect of six weeks of progressive jump-landing training on jump shooting accuracy and knee valgus angle in male basketball players with dynamic knee valgus. Journal of Sport Biomechanics. 2021; 7(2):148-63. [DOI:10.32598/biomechanics.7.2.6]
- Dadfar M, Sheikhhoseini R, Eslami R, Farivar N. The effects of corrective exercise with and without visual feedback on lower extremity biomechanics and dynamic balance in adolescent female athletes with dynamic knee valgus: A pilot study. Journal of Modern Rehabilitation. 2022; 16(1):31-44. [DOI:10.18502/jmr.v16i1.8560]
- Plisky PJ, Gorman PP, Butler RJ, Kiesel KB, Underwood FB, Elkins B. The reliability of an instrumented device for measuring components of the star excursion balance test. North American Journal of Sports Physical Therapy. 2009; 4(2):92-9. [PMID] [PMCID]
- Page P, Frank CC, Lardner R. Assessment and treatment of muscle imbalance: the janda approach. Champaign: Human Kinetics; 2010. [DOI:10.5040/9781718211445]
- Ross MD, Langford B, Whelan PJ. Test-retest reliability of 4 single-leg horizontal hop tests. Journal of Strength and Conditioning Research. 2002; 16(4):617-22.[DOI:10.1519/00124278-200211000-00021] [PMID]
- Pauole K, Kent M, Garhammer J, Lacourse M, Rozenek R. Reliability and validity of the T-test as a measure of agility, leg power, and leg speed in college-aged men and women. The Journal of Strength & Conditioning Research. 2000; 14(4):443-50. [Link]
- Johnston W, Dolan K, Reid N, Coughlan GF, Caulfield B. Investigating the effects of maximal anaerobic fatigue on dynamic postural control using the Y-Balance Test. Journal of Science and Medicine in Sport. 2018; 21(1):103-8. [DOI:10.1016/j.jsams.2017.06.007] [PMID]
- Maïano C, Hue O, Morin AJS, Lepage G, Tracey D, Moullec G. Exercise interventions to improve balance for young people with intellectual disabilities: A systematic review and meta-analysis. Developmental Medicine and Child Neurology. 2019; 61(4):406-18. [DOI:10.1111/dmcn.14023] [PMID]
- Lawrence EL, Cesar GM, Bromfield MR, Peterson R, Valero-Cuevas FJ, Sigward SM. Strength, multijoint coordination, and sensorimotor processing are independent contributors to overall balance ability. BioMed Research International. 2015; 2015:561243. [DOI:10.1155/2015/561243] [PMID] [PMCID]
- Wang J, Xu J, An R. Effectiveness of backward walking training on balance performance: A systematic review and meta-analysis. Gait & Posture. 2019; 68:466-75. [DOI:10.1016/j.gaitpost.2019.01.002] [PMID]
- Basso JC, Suzuki WA. The effects of acute exercise on mood, cognition, neurophysiology, and neurochemical pathways: A review. Brain Plasticity. 2017; 2(2):127-52. [DOI:10.3233/BPL-160040] [PMID] [PMCID]
- Miller KJ, Mesagno C, McLaren S, Grace F, Yates M, Gomez R. Exercise, mood, self-efficacy, and social support as predictors of depressive symptoms in older adults: Direct and interaction effects. Frontiers in Psychology. 2019; 10:2145. [DOI:10.3389/fpsyg.2019.02145] [PMID] [PMCID]
- Bieler T, Siersma V, Magnusson SP, Kjaer M, Beyer N. Exercise induced effects on muscle function and range of motion in patients with hip osteoarthritis. Physiotherapy Research International. 2018; 23(1):e1697. [DOI:10.1002/pri.1697] [PMID]
- Attwood MJ, Roberts SP, Trewartha G, England ME, Stokes KA. Efficacy of a movement control injury prevention programme in adult men's community rugby :union:: A cluster randomised controlled trial. British Journal of Sports Medicine. 2018; 52(6):368-374. [DOI:10.1136/bjsports-2017-098005] [PMID] [PMCID]
- Myer GD, Ford KR, Hewett TE. The effects of gender on quadriceps muscle activation strategies during a maneuver that mimics a high ACL injury risk position. Journal of Electromyography and Kinesiology. 2005; 15(2):181-9. [DOI:10.1016/j.jelekin.2004.08.006] [PMID]
- Kim AW, Rosen AM, Brander VA, Buchanan TS. Selective muscle activation following electrical stimulation of the collateral ligaments of the human knee joint. Archives of Physical Medicine and Rehabilitation. 1995; 76(8):750-7.[DOI:10.1016/S0003-9993(95)80530-3] [PMID]
- Struyf F, Geraets J, Noten S, Meeus M, Nijs J. A multivariable prediction model for the chronification of non-traumatic shoulder pain: A systematic review. Pain Physician. 2016; 19(2):1-10. [DOI:10.36076/ppj/2016.19.1] [PMID]
- Kuijpers T, van der Windt DAWM, van der Heijden GJMG, Bouter LM. Systematic review of prognostic cohort studies on shoulder disorders. Pain. 2004; 109(3):420-31. [DOI:10.1016/j.pain.2004.02.017] [PMID]
Type of Study: Research |
Subject:
General
Received: 2022/08/8 | Accepted: 2022/12/24 | Published: 2022/10/20
Received: 2022/08/8 | Accepted: 2022/12/24 | Published: 2022/10/20
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
This is an open access article distributed under the terms of the Creative Commons Attribution License (CC-By-NC), which permits use, distribution, and reproduction in any medium, provided the original work is properly cited and is not used for commercial purposes.
Contact Information
