Fri, Apr 19, 2024
Volume 9, Issue 1 (Winter 2019)
PTJ 2019, 9(1): 23-30 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Zolghadr H, Sedaghati P, Daneshmandi H. The Effect of Selected Balance/Corrective Exercises on the Balance Performance of Mentally-Retarded Students With Developmental Coordination Disorder. PTJ 2019; 9 (1) :23-30
URL: http://ptj.uswr.ac.ir/article-1-381-en.html
URL: http://ptj.uswr.ac.ir/article-1-381-en.html



1- Department of Corrective Exercises and Sport Injuries, Faculty of Physical Education and Sport Sciences, University of Guilan , Rasht, Iran.
Keywords: Balance exercises, Corrective exercises, Mental retardation, Developmental coordination disorder
Full-Text [PDF 562 kb]
(2027 Downloads)
| Abstract (HTML) (3408 Views)

Full-Text: (1575 Views)
1. Introduction
Mental retardation is one of the main problems of human societies and affects about 3% of the population [1]. It is crucial for people with mental retardation to maintain strength and muscular endurance and dynamic balance to achieve a better life and functional independence. The ability to maintain independent living is a significant factor for mentally-retarded people [2]. Educable mentally-retarded children compared to healthy children with the same age have lower physical strength, tolerance, agility, running speed, reaction time, and balance scores. They are two or four years behind healthy children in motor skills [3].
Balance refers to keep stability for voluntary activities in dealing with internal and external perturbations. In terms of biomechanics, it maintains the body center of gravity over the base of support [4]. The mentally-retarded child is weak in terms of psychomotor development and has problems in sensory-motor capacities, body awareness, static and dynamic balance, and coordination of fine and gross movements [5]. Many studies have been carried out in this field, and various treatments have been used. For example, Sretenović et al. assessed the balance in preschool children. Their results showed that the mentally-retarded group had a lower balance ability than the typically developed group [6]. Pise et al. evaluated the effect of yoga on psycho-motor skills of mentally-retarded children and reported that it could improve their static balance, eye-hand coordination, agility, and reaction time [7].
Yalfani et al. studied the effect of 8-week play therapy on the balance of 10-12 years old mentally-retarded children. Their results revealed that the subjects’ balance (total balance and in anterior/posterior and medial/lateral directions) in pre-test and post-test stages was significantly different compared to the control group [8].
Among mentally-retarded children, Educable Mentally-Retarded (EMR) children are those who, in spite of their ability to learn skills of reading, writing, and arithmetic through education, are different from their healthy peers. One of these differences is that they have Developmental Coordination Disorder (DCD) [9]. DCD refers to the child’s inability to coordinate the components of motor activity to perform age-appropriate activities. EMR children also have difficulties in fine motor skills, perceptual-motor skills, including balance and motor coordination problems [10]. People with DCD have a deficiency in balance in comparison to ordinary people [11].
According to Carmeli et al., children with DCD, due to sensory-motor processing impairment, obtain lower scores in balance and perceptual-motor tests than normal children, and their balance status is more unstable than that of healthy ones [12]. In the study of Sohrabi et al. who evaluated the effect of strength training based on process approach intervention on the balance of children with DCD, it was shown that the strength training increased muscle strength and improved static balance in these children, but did not affect their dynamic balance performance [13].
Dadmehr et al. studied the effect of sensorimotor stimulation intervention on motor coordination of EMR children with DCD and showed that this intervention could improve their motor coordination [14]. Rezaei et al. evaluated the effect of 8-week selective exercises on the balance of children with DCD and reported that these exercises could improve their balance [15].
In another study, Mohammadi et al. studied the effect of core stability training on the static and dynamic balance of children with DCD. Their results showed that this training could improve their balance where the experimental group had better performance in static and dynamic balance compared to the controls [16]. Since mental retardation cannot be cured, the main task is to rehabilitate and educate these patients [1]. Considering what was discussed, the importance of balance in mentally-retarded people and those with DCD is very high. Balance is one of the most important factors of physical fitness and health in individuals, and this factor is of great importance in mentally-retarded people because the poor balance causes limitations in their daily activities and life.
As studies have shown, the balance in these people compared to healthy people is impaired and requires attention and exercise, including balance exercises. Because of the association between posture and balance in mentally-retarded people, it is better to use balance and corrective exercises simultaneously to have a better effect both on their balance and posture. In this regard, a balance/corrective exercise program, in addition to improving balance and posture as well as motor coordination in mentally-retarded people and reducing the related problems, can strengthen their other motor skills and be a means to solve their psychological and social issues. Moreover, no study was found using a balance/corrective exercise program in mentally-retarded adolescents with DCD. In this regard, this study aimed to examine the effect of exclusive balance/corrective exercises on the balance of mentally-retarded students with DCD.
2. Materials and Methods
This was a quasi-experimental study with pre-test and post-test design and control group. The study population consisted of male students with mental retardation in a high school located in Rasht City, Iran, during 2017-2018 (n=56). The inclusion criteria for the study were not using nerve drugs or drugs affecting balance, no history of lower limb injury and or operation over the past 1 year, no disease in the vestibular system and not having cochlear implant, no visual impairment and having normal vision without wearing glasses, and willingness and ability to participate in the test [17]. Those who met these criteria were selected, and then their parents completed DCD inventory [18] for them. Those children who had DCD were selected as study samples (n=24, age=14-18 years, IQ=50-75) using purposive and convenience sampling techniques and were randomly assigned in two groups of intervention (n=12) and control (n=12). One child in the control group was excluded from the study due to not participating in the tests. In the pre-test stage, the static and dynamic balance of the samples were assessed. Then, the samples in the intervention group performed the selective balance/corrective exercises for eight weeks. Meanwhile, the control group only continued their daily activities in the school. At the end of the intervention, both groups performed all the tests again. The collected data were analyzed in SPSS V. 25 using the Independent t test and Analysis of Covariance (ANCOVA).
Static balance was assessed by modified Stork test with both eyes open and closed on the dominant leg. Before the assessment, the correct form of the test was taught to subjects. They were asked to stand comfortably with hands on their hips while the sole of the non-dominant foot is against the inner side (kneecap) of the dominant foot. They were asked to maintain this state as long as possible. When the dominant leg heel touches the ground, the hands move away from the hip, or the sole of non-dominant foot moves away from the kneecap of the dominant foot, the test is terminated and the time is recorded. Since it was not possible for subjects to do this test with these conditions, they stood on the entire sole surface of the foot. Each subject repeated the test twice with a 15-s resting interval. The maximum time for this test is 60 seconds [7].
To assess dynamic balance, the Timed Up and Go (TUG) test was used. For performing this test, a chair with armrests and a 3-m distance are required. The 3-m path starts from the chair bases. The subject sits on the chair and leans back while wearing casual shoes and clothes. On the command “Go”, the subject stands up, walks the path, turns around and walks back to the chair (traveled distance=6 m). The time in seconds is recorded as the subject’s score. The time less than 20 seconds indicates a good performance [19].
The Pediatric Balance Scale (PBS), which is a modified version of the Berg Balance Scale, was used to assess functional balance. It has 14 items which are as follows: sitting to standing, standing to sitting, transfers, standing unsupported, sitting unsupported, standing with eyes closed, standing with feet together, standing with one foot in front, standing on one foot, turning 360°, turning to look behind, retrieving object from floor, placing alternate foot on stool, and reaching forward with outstretched arms. Each item is rated from 0 to 4; score 4 is for when the subject can perform the movements correctly and without assistance; score 3 when he can perform the movements but needs minor help; score 2 when he can perform the movements but needs more assistance; score 1 when he needs assistance to complete the movements; and score 0 when he is unable to perform the movements. The total score ranges from 0 to 56. A lower score indicates a lower functional balance [20].
The protocol of balance-corrective exercises
In the balance/corrective exercises program, each session includes three parts: warm-up, main exercise, and cooling down. In the warm-up section, all subjects do the walking and stretching movements for 10 minutes. The program took 8 weeks, three days a week, and each session lasted for 60 minutes. The intervention program was divided into two stages, each for 4 weeks, and the overload principle was applied accordingly. The balance exercises were heel-toe walking, walking on the line, sideways walking, reverse walking, zigzag walking, walking with long steps, tandem standing, standing with feet together, standing on one foot, and weight transfer. The corrective exercises were posture correction, neck extension, cat stretch, plank, V shape movement, and bridge on a Swiss ball. The exercises were conducted under the supervision of the examiner. Before beginning, the exercises were taught to the subjects. At each stage, maintaining the status and proper posture were reminded to the subjects. A chronometer was used to measure the time. The exercise intensity was also adjusted according to the subjects’ power. During the intervention, the control group only participated in physical activities as sports curriculum for one hour a day. At the end of the intervention, both intervention and control groups received assessments.
3. Results
Table 1 presents the demographic characteristics of participants in both groups. According to the results, both groups were homogenous in terms of demographic characteristics. Based on ANCOVA results, after controlling the effect of pre-test (covariate), there was a significant difference between the two groups in terms of static balance and dynamic balance (P<0.05) where the scores of samples in the intervention group were better compared to that of the controls (Table 2).
Mental retardation is one of the main problems of human societies and affects about 3% of the population [1]. It is crucial for people with mental retardation to maintain strength and muscular endurance and dynamic balance to achieve a better life and functional independence. The ability to maintain independent living is a significant factor for mentally-retarded people [2]. Educable mentally-retarded children compared to healthy children with the same age have lower physical strength, tolerance, agility, running speed, reaction time, and balance scores. They are two or four years behind healthy children in motor skills [3].
Balance refers to keep stability for voluntary activities in dealing with internal and external perturbations. In terms of biomechanics, it maintains the body center of gravity over the base of support [4]. The mentally-retarded child is weak in terms of psychomotor development and has problems in sensory-motor capacities, body awareness, static and dynamic balance, and coordination of fine and gross movements [5]. Many studies have been carried out in this field, and various treatments have been used. For example, Sretenović et al. assessed the balance in preschool children. Their results showed that the mentally-retarded group had a lower balance ability than the typically developed group [6]. Pise et al. evaluated the effect of yoga on psycho-motor skills of mentally-retarded children and reported that it could improve their static balance, eye-hand coordination, agility, and reaction time [7].
Yalfani et al. studied the effect of 8-week play therapy on the balance of 10-12 years old mentally-retarded children. Their results revealed that the subjects’ balance (total balance and in anterior/posterior and medial/lateral directions) in pre-test and post-test stages was significantly different compared to the control group [8].
Among mentally-retarded children, Educable Mentally-Retarded (EMR) children are those who, in spite of their ability to learn skills of reading, writing, and arithmetic through education, are different from their healthy peers. One of these differences is that they have Developmental Coordination Disorder (DCD) [9]. DCD refers to the child’s inability to coordinate the components of motor activity to perform age-appropriate activities. EMR children also have difficulties in fine motor skills, perceptual-motor skills, including balance and motor coordination problems [10]. People with DCD have a deficiency in balance in comparison to ordinary people [11].
According to Carmeli et al., children with DCD, due to sensory-motor processing impairment, obtain lower scores in balance and perceptual-motor tests than normal children, and their balance status is more unstable than that of healthy ones [12]. In the study of Sohrabi et al. who evaluated the effect of strength training based on process approach intervention on the balance of children with DCD, it was shown that the strength training increased muscle strength and improved static balance in these children, but did not affect their dynamic balance performance [13].
Dadmehr et al. studied the effect of sensorimotor stimulation intervention on motor coordination of EMR children with DCD and showed that this intervention could improve their motor coordination [14]. Rezaei et al. evaluated the effect of 8-week selective exercises on the balance of children with DCD and reported that these exercises could improve their balance [15].
In another study, Mohammadi et al. studied the effect of core stability training on the static and dynamic balance of children with DCD. Their results showed that this training could improve their balance where the experimental group had better performance in static and dynamic balance compared to the controls [16]. Since mental retardation cannot be cured, the main task is to rehabilitate and educate these patients [1]. Considering what was discussed, the importance of balance in mentally-retarded people and those with DCD is very high. Balance is one of the most important factors of physical fitness and health in individuals, and this factor is of great importance in mentally-retarded people because the poor balance causes limitations in their daily activities and life.
As studies have shown, the balance in these people compared to healthy people is impaired and requires attention and exercise, including balance exercises. Because of the association between posture and balance in mentally-retarded people, it is better to use balance and corrective exercises simultaneously to have a better effect both on their balance and posture. In this regard, a balance/corrective exercise program, in addition to improving balance and posture as well as motor coordination in mentally-retarded people and reducing the related problems, can strengthen their other motor skills and be a means to solve their psychological and social issues. Moreover, no study was found using a balance/corrective exercise program in mentally-retarded adolescents with DCD. In this regard, this study aimed to examine the effect of exclusive balance/corrective exercises on the balance of mentally-retarded students with DCD.
2. Materials and Methods
This was a quasi-experimental study with pre-test and post-test design and control group. The study population consisted of male students with mental retardation in a high school located in Rasht City, Iran, during 2017-2018 (n=56). The inclusion criteria for the study were not using nerve drugs or drugs affecting balance, no history of lower limb injury and or operation over the past 1 year, no disease in the vestibular system and not having cochlear implant, no visual impairment and having normal vision without wearing glasses, and willingness and ability to participate in the test [17]. Those who met these criteria were selected, and then their parents completed DCD inventory [18] for them. Those children who had DCD were selected as study samples (n=24, age=14-18 years, IQ=50-75) using purposive and convenience sampling techniques and were randomly assigned in two groups of intervention (n=12) and control (n=12). One child in the control group was excluded from the study due to not participating in the tests. In the pre-test stage, the static and dynamic balance of the samples were assessed. Then, the samples in the intervention group performed the selective balance/corrective exercises for eight weeks. Meanwhile, the control group only continued their daily activities in the school. At the end of the intervention, both groups performed all the tests again. The collected data were analyzed in SPSS V. 25 using the Independent t test and Analysis of Covariance (ANCOVA).
Static balance was assessed by modified Stork test with both eyes open and closed on the dominant leg. Before the assessment, the correct form of the test was taught to subjects. They were asked to stand comfortably with hands on their hips while the sole of the non-dominant foot is against the inner side (kneecap) of the dominant foot. They were asked to maintain this state as long as possible. When the dominant leg heel touches the ground, the hands move away from the hip, or the sole of non-dominant foot moves away from the kneecap of the dominant foot, the test is terminated and the time is recorded. Since it was not possible for subjects to do this test with these conditions, they stood on the entire sole surface of the foot. Each subject repeated the test twice with a 15-s resting interval. The maximum time for this test is 60 seconds [7].
To assess dynamic balance, the Timed Up and Go (TUG) test was used. For performing this test, a chair with armrests and a 3-m distance are required. The 3-m path starts from the chair bases. The subject sits on the chair and leans back while wearing casual shoes and clothes. On the command “Go”, the subject stands up, walks the path, turns around and walks back to the chair (traveled distance=6 m). The time in seconds is recorded as the subject’s score. The time less than 20 seconds indicates a good performance [19].
The Pediatric Balance Scale (PBS), which is a modified version of the Berg Balance Scale, was used to assess functional balance. It has 14 items which are as follows: sitting to standing, standing to sitting, transfers, standing unsupported, sitting unsupported, standing with eyes closed, standing with feet together, standing with one foot in front, standing on one foot, turning 360°, turning to look behind, retrieving object from floor, placing alternate foot on stool, and reaching forward with outstretched arms. Each item is rated from 0 to 4; score 4 is for when the subject can perform the movements correctly and without assistance; score 3 when he can perform the movements but needs minor help; score 2 when he can perform the movements but needs more assistance; score 1 when he needs assistance to complete the movements; and score 0 when he is unable to perform the movements. The total score ranges from 0 to 56. A lower score indicates a lower functional balance [20].
The protocol of balance-corrective exercises
In the balance/corrective exercises program, each session includes three parts: warm-up, main exercise, and cooling down. In the warm-up section, all subjects do the walking and stretching movements for 10 minutes. The program took 8 weeks, three days a week, and each session lasted for 60 minutes. The intervention program was divided into two stages, each for 4 weeks, and the overload principle was applied accordingly. The balance exercises were heel-toe walking, walking on the line, sideways walking, reverse walking, zigzag walking, walking with long steps, tandem standing, standing with feet together, standing on one foot, and weight transfer. The corrective exercises were posture correction, neck extension, cat stretch, plank, V shape movement, and bridge on a Swiss ball. The exercises were conducted under the supervision of the examiner. Before beginning, the exercises were taught to the subjects. At each stage, maintaining the status and proper posture were reminded to the subjects. A chronometer was used to measure the time. The exercise intensity was also adjusted according to the subjects’ power. During the intervention, the control group only participated in physical activities as sports curriculum for one hour a day. At the end of the intervention, both intervention and control groups received assessments.
3. Results
Table 1 presents the demographic characteristics of participants in both groups. According to the results, both groups were homogenous in terms of demographic characteristics. Based on ANCOVA results, after controlling the effect of pre-test (covariate), there was a significant difference between the two groups in terms of static balance and dynamic balance (P<0.05) where the scores of samples in the intervention group were better compared to that of the controls (Table 2).
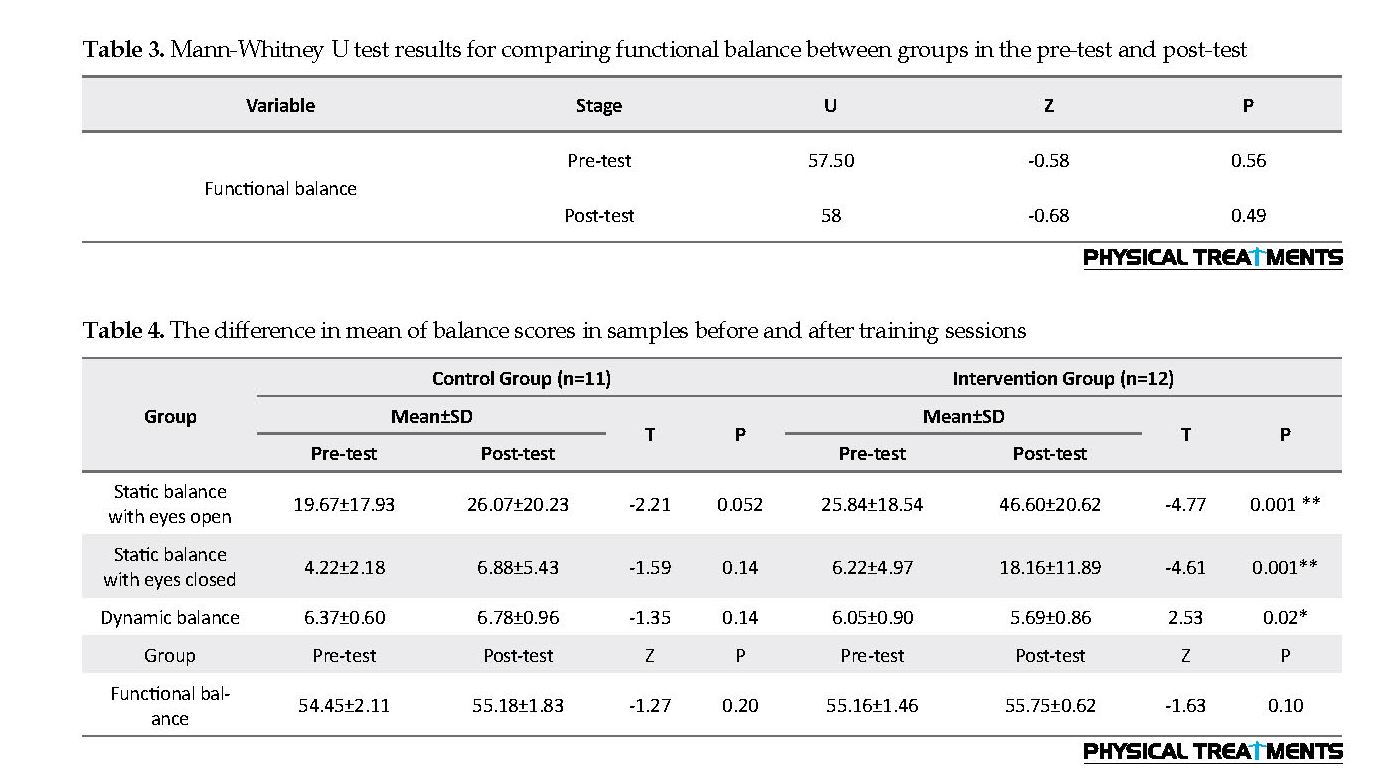
Because of the non-normal distribution of the functional balance scores, the non-parametric Mann–Whitney U test was used to examine the differences between the control and intervention groups. Its results indicate no significant difference between them in terms of functional balance (P>0.05) (Table 3).
To test the difference between pre-test and post-test scores in both groups separately, the correlated t test (for normal variables) and Wilcoxon test (for functional balance variable) were used. The results are shown in Table 4. Based on the t test results, the balance/corrective exercises program had a significant effect on the static and dynamic balance (P<0.01) but did not affect their functional balance (P=0.10). In the control group, there was no significant difference between pre-test and post-test scores after the 8-week intervention.
4. Discussion
The purpose of this study was to evaluate the effect of an 8-week selective balance/corrective exercises program on the functional performance of mentally-retarded students with DCD. The results showed that this program had a significant impact on their static and dynamic balance, but it could not significantly affect their functional balance. In terms of static and dynamic balance, our result is consistent with the results of previous studies [6-8, 17, 21, 22]. They also showed that physical exercises could improve the static and dynamic balance in mentally-retarded people. In the study of Taghian et al. [23] who investigated the effect of 8-week combined exercises (strength and balance) on the balance (static and dynamic) and aggression of 7-14 years old children with EMR, the results showed that combined exercises had a significant effect on the static and dynamic balance of EMR children. These results are consistent with ours. Also, Oviedo et al. [21] investigated the effects of aerobic, resistance, and balance training in adults with intellectual disabilities. Their results reported that cardiovascular fitness, handgrip strength, leg strength, and balance in the intervention group were significantly different from those of the control group.
Ahmadi et al. [22] examined the effect of a 6-week core stabilization training program on the balance of EMR students and showed that it could improve their balance. Kubilay et al. [17] also studied the effect of balance training and posture exercises on functional level in mentally-retarded children. Their results showed that their static, dynamic, and functional balance improved after the 8-week intervention. In terms of static and dynamic balance, their result is consistent with our results but are against ours on functional balance. This discrepancy can be due to the difference in number and type of samples. In their study, the number of samples was higher, and their motor performance level was lower than adults while in the present study, considering the limited number of our samples, they had better motor performance than older children. Another reason may be related to the PBS test.
It is a more comfortable test for adolescents than children, which is why differences in their functional balance were not observed. In another study, Hossaini et al. [24] investigated the effect of 8-week posture and balance exercises on physical fitness of children with mental disabilities and reported their effect on static balance (consistent with our results) but not on dynamic balance (against our results). Furthermore, the result of this study on the balance of mentally-retarded children with DCD is consistent with the results of previous studies [13, 15, 16].
We recommend using the proposed interventional program because of the importance of static and dynamic balance in the activity and everyday life of mentally-retarded people, as well as the low cost and availability of the equipment needed for these exercises. Studies have shown that balance exercises improve balance status [23]. According to previous studies and the physiological mechanisms, the gravity always pulls the body down to the ground and disturbs the balance. There are various and complex mechanisms that interfere with this process and keep the body in balance.
The initiation of these mechanisms is when the body is at risk of falling. In this case, these mechanisms are activated to re-establish balance. These mechanisms include natural muscle contraction, stimulation of proprioceptors, and recall for motion patterns which are controlled and coordinated with certain patterns in the brain. The involvement of these systems is proportional to automatic reactions and includes predictable changes in muscle contraction with regard to head and trunk position. These changes are accompanied by an adaptive increase in flexor/extensor muscles activity to recover balance [25].
Considering the few participants in this study because of the selection of DCD samples from mentally-retarded samples, further studies are recommended using a larger sample size. Based on the above findings, we can justify the significant effect of selective balance/corrective exercises on the static and dynamic balance of mentally-retarded students with DCD. These exercises can be used for rehabilitation and physical activities in the sports curriculum of special schools for mentally-retarded students as a suitable method and intervention for improving their balance.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Guilan Medical Sciences (Code: IR.GUMS.REC.1397.477).
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for- profit sectors.
Authors' contributions
Conceptualization, Methodology, Supervision: All authors; Investigation, Writing original draft, Funding acquisition, Resources: Hamid Zolghadr; Writing-review and editing: Parisa Sedaghati, Hassan Daneshmandi.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank the Vice-Chancellor for Research of Guilan University of Medical Sciences, Department of Education in Rasht City, the staff of Hemmat Exceptional School, and all study students for their sincere cooperation.
References
Yektamaram SAM, Gholami Soltanmoradi R. [How to interact with people with disabilities (Persian)]. Tehran: Welfare Organization of the Country, Public Relations; 2009.
Kajbaf MB, Mahmood M, Ejeie J, Dadsetan P. [Survey and diagnosis of mental retardation based Piaget tests and Lambert scale (Persian)]. Psychology. 2000; 12(17):341-57.
Sharifidaramadi P. [Mental retardation children: Mental and educational approach (Persian)] [PhD. dissertation]. Iran: Tarbiat Modares University; 1998.
Zamani J. [Comparison of the effect of eight weeks of plyometric, equilibrium and combined (plyometric and balance) exercises on knee joint proprioception and static equilibrium (Persian)] [MA thesis]. Isfahan: Isfahan University; 2010.
Ramezani Nezhad R. [Physical education in schools (Persian)]. Tehran: SAMT; 2002.
Sretenović I, Nedović G, Đorđević S. Assessment of balance in younger school children with intellectual disability. Facta Universitatis, Series: Physical Education and Sport. 2019; 16(3):687-96. [DOI.org/10.22190/FUPES171010061S]
Pise V, Pradhan B, Gharote M. Effect of yoga practices on psycho-motor abilities among intellectually disabled children. Journal of Exercise Rehabilitation. 2018; 14(4):581-5. [DOI:10.12965/jer.1836290.145] [PMID] [PMCID]
Yalfani A, Jalali N, Gholami B, Gholami Borujeni B, Ahmadenzhad L. The effect of eight weeks playing therapy program on balance of 10-12 years old mentally retarded children. Journal of Paramedical sciences & Rehabilitation, 2017; 6(1):64-73. [DOI: 10.22038/JPSR.2017.13996.1295]
Simingalam M, Alibakhshi H. The investigation of motor-free visual perception skills in educable children with developmental coordination (Persian)]. Knowledge and Research in Applied Psychology. 2011; 12(45):71-8.
Lingam R, Hunt L, Golding J, Jongmans M, Emond A. Prevalence of developmental coordination disorder using the DSM-IV at 7 years of age: A UK population-based study. Pediatrics. 2009; 123(4):e693-700. [DOI:10.1542/peds.2008-1770] [PMID]
Baumeister AA, Kellas G. Distribution of reaction times of retardates and normals. American Journal of Mental Deficiency. 1968; 72(5)715-8. [PMID]
Carmeli E, Bar-Yossef T, Ariav C, Levy R, Liebermann DG. Perceptual-motor coordination in persons with mild intellectual disability. Disability and Rehabilitation. 2008; 30(5):323-9. [DOI:10.1080/09638280701265398] [PMID]
Kordi H, Sohrabi M, Kakhki AS, Attarzadeh SR. The effect of strength training based on process approach intervention on balance of children with developmental coordination disorder. Archivos Argentinos de Pediatria. 2016; 114(6):526-33. [DOI:10.5546/aap.2016.eng.526]
Malekpour M, Dadmehr A, Ghomrani A. [Interventional effect of sensorimotor stimulation on motor coordination in educable mentally retarded students DCD (Persian)]. Psychology of Exceptional Individuals. 2014; 4(14):63-82.
Rezaei S, Arabameri E, Sohrabi MM. [Examination of the Impact of an Eight-Week Exclusive Exercise on the Balance of Children with Developmental Coordination Disorders (Persian)]. Scientific Journal of Rehabilitation Medicine. 2017; 5(4):57-64.
Eslamdost M, Sheikh M, Mohammadi M, Ahmadi G. The effect of core stability training on static and dynamic balance in children with developmental coordination disorder. Community Health Journal. 2017; 11(2):20-8. [DOI:10.22123/chj.2018.85447].
Kubilay, N.S., et al., Effect of balance training and posture exercises on functional level in mental retardation. Fizyoterapi Rehabilitasyon. 2011; 22(2):55-64.
Wilson BN, Crawford SG, Green D, Roberts G, Aylott A, Kaplan BJ. Psychometric properties of the revised developmental coordination disorder questionnaire. Physical & Occupational Therapy in Pediatrics. 2009; 29(2):182-202. [DOI:10.1080/01942630902784761] [PMID]
Shumway-Cook A, Brauer S, Woollacott M. Predicting the probability for falls in community-dwelling older adults using the Timed Up & Go Test. Physical Therapy. 2000; 80(9):896-903. [PMID]
Hawk C, Cambron J. Chiropractic care for older adults: Effects on balance, dizziness, and chronic pain. Journal of Manipulative and Physiological Therapeutics. 2009; 32(6):431-7. [DOI:10.1016/j.jmpt.2009.06.009] [PMID]
Oviedo GR, Guerra-Balic M, Baynard T, Javierre C. Effects of aerobic, resistance and balance training in adults with intellectual disabilities. Research in Developmental Disabilities. 2014; 35(11):2624-34. [DOI:10.1016/j.ridd.2014.06.025] [PMID]
Ahmadi R, Daneshmandi H, Barati AH. [The effect of 6 weeks core stabilization training program on the balance in mentally retarded students (Persian)]. International Journal of Sport Studies. 2012; 2(10)496-501.
Taghian H, Ghasemi GA, Sadeghi M. Effect of combined exercises (strength and balance) on balance and aggression in 7-14 year-old educabe intelectual disability boys. Scientific Journal of Rehabilitation Medicine. 2017; 6(3):174-81.
Hossaini SA, Zar A, Khodadoust M, Hejazi E. The effect of eight-weekly exercise exercises on physical fitness factors of mental retardation children. Pediatric Nursing. 2017; 3(3):25-30. [DOI:10.21859/jpen-03035]
Daneshmandi H, Alizadeh MH, Gharakhanloo R. Corrective exercises (diagnosis and prescription). 14th edition. Tehran: SAMT; 2011.
4. Discussion
The purpose of this study was to evaluate the effect of an 8-week selective balance/corrective exercises program on the functional performance of mentally-retarded students with DCD. The results showed that this program had a significant impact on their static and dynamic balance, but it could not significantly affect their functional balance. In terms of static and dynamic balance, our result is consistent with the results of previous studies [6-8, 17, 21, 22]. They also showed that physical exercises could improve the static and dynamic balance in mentally-retarded people. In the study of Taghian et al. [23] who investigated the effect of 8-week combined exercises (strength and balance) on the balance (static and dynamic) and aggression of 7-14 years old children with EMR, the results showed that combined exercises had a significant effect on the static and dynamic balance of EMR children. These results are consistent with ours. Also, Oviedo et al. [21] investigated the effects of aerobic, resistance, and balance training in adults with intellectual disabilities. Their results reported that cardiovascular fitness, handgrip strength, leg strength, and balance in the intervention group were significantly different from those of the control group.
Ahmadi et al. [22] examined the effect of a 6-week core stabilization training program on the balance of EMR students and showed that it could improve their balance. Kubilay et al. [17] also studied the effect of balance training and posture exercises on functional level in mentally-retarded children. Their results showed that their static, dynamic, and functional balance improved after the 8-week intervention. In terms of static and dynamic balance, their result is consistent with our results but are against ours on functional balance. This discrepancy can be due to the difference in number and type of samples. In their study, the number of samples was higher, and their motor performance level was lower than adults while in the present study, considering the limited number of our samples, they had better motor performance than older children. Another reason may be related to the PBS test.
It is a more comfortable test for adolescents than children, which is why differences in their functional balance were not observed. In another study, Hossaini et al. [24] investigated the effect of 8-week posture and balance exercises on physical fitness of children with mental disabilities and reported their effect on static balance (consistent with our results) but not on dynamic balance (against our results). Furthermore, the result of this study on the balance of mentally-retarded children with DCD is consistent with the results of previous studies [13, 15, 16].
We recommend using the proposed interventional program because of the importance of static and dynamic balance in the activity and everyday life of mentally-retarded people, as well as the low cost and availability of the equipment needed for these exercises. Studies have shown that balance exercises improve balance status [23]. According to previous studies and the physiological mechanisms, the gravity always pulls the body down to the ground and disturbs the balance. There are various and complex mechanisms that interfere with this process and keep the body in balance.
The initiation of these mechanisms is when the body is at risk of falling. In this case, these mechanisms are activated to re-establish balance. These mechanisms include natural muscle contraction, stimulation of proprioceptors, and recall for motion patterns which are controlled and coordinated with certain patterns in the brain. The involvement of these systems is proportional to automatic reactions and includes predictable changes in muscle contraction with regard to head and trunk position. These changes are accompanied by an adaptive increase in flexor/extensor muscles activity to recover balance [25].
Considering the few participants in this study because of the selection of DCD samples from mentally-retarded samples, further studies are recommended using a larger sample size. Based on the above findings, we can justify the significant effect of selective balance/corrective exercises on the static and dynamic balance of mentally-retarded students with DCD. These exercises can be used for rehabilitation and physical activities in the sports curriculum of special schools for mentally-retarded students as a suitable method and intervention for improving their balance.
Ethical Considerations
Compliance with ethical guidelines
This study was approved by the Ethics Committee of Guilan Medical Sciences (Code: IR.GUMS.REC.1397.477).
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for- profit sectors.
Authors' contributions
Conceptualization, Methodology, Supervision: All authors; Investigation, Writing original draft, Funding acquisition, Resources: Hamid Zolghadr; Writing-review and editing: Parisa Sedaghati, Hassan Daneshmandi.
Conflict of interest
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank the Vice-Chancellor for Research of Guilan University of Medical Sciences, Department of Education in Rasht City, the staff of Hemmat Exceptional School, and all study students for their sincere cooperation.
References
Yektamaram SAM, Gholami Soltanmoradi R. [How to interact with people with disabilities (Persian)]. Tehran: Welfare Organization of the Country, Public Relations; 2009.
Kajbaf MB, Mahmood M, Ejeie J, Dadsetan P. [Survey and diagnosis of mental retardation based Piaget tests and Lambert scale (Persian)]. Psychology. 2000; 12(17):341-57.
Sharifidaramadi P. [Mental retardation children: Mental and educational approach (Persian)] [PhD. dissertation]. Iran: Tarbiat Modares University; 1998.
Zamani J. [Comparison of the effect of eight weeks of plyometric, equilibrium and combined (plyometric and balance) exercises on knee joint proprioception and static equilibrium (Persian)] [MA thesis]. Isfahan: Isfahan University; 2010.
Ramezani Nezhad R. [Physical education in schools (Persian)]. Tehran: SAMT; 2002.
Sretenović I, Nedović G, Đorđević S. Assessment of balance in younger school children with intellectual disability. Facta Universitatis, Series: Physical Education and Sport. 2019; 16(3):687-96. [DOI.org/10.22190/FUPES171010061S]
Pise V, Pradhan B, Gharote M. Effect of yoga practices on psycho-motor abilities among intellectually disabled children. Journal of Exercise Rehabilitation. 2018; 14(4):581-5. [DOI:10.12965/jer.1836290.145] [PMID] [PMCID]
Yalfani A, Jalali N, Gholami B, Gholami Borujeni B, Ahmadenzhad L. The effect of eight weeks playing therapy program on balance of 10-12 years old mentally retarded children. Journal of Paramedical sciences & Rehabilitation, 2017; 6(1):64-73. [DOI: 10.22038/JPSR.2017.13996.1295]
Simingalam M, Alibakhshi H. The investigation of motor-free visual perception skills in educable children with developmental coordination (Persian)]. Knowledge and Research in Applied Psychology. 2011; 12(45):71-8.
Lingam R, Hunt L, Golding J, Jongmans M, Emond A. Prevalence of developmental coordination disorder using the DSM-IV at 7 years of age: A UK population-based study. Pediatrics. 2009; 123(4):e693-700. [DOI:10.1542/peds.2008-1770] [PMID]
Baumeister AA, Kellas G. Distribution of reaction times of retardates and normals. American Journal of Mental Deficiency. 1968; 72(5)715-8. [PMID]
Carmeli E, Bar-Yossef T, Ariav C, Levy R, Liebermann DG. Perceptual-motor coordination in persons with mild intellectual disability. Disability and Rehabilitation. 2008; 30(5):323-9. [DOI:10.1080/09638280701265398] [PMID]
Kordi H, Sohrabi M, Kakhki AS, Attarzadeh SR. The effect of strength training based on process approach intervention on balance of children with developmental coordination disorder. Archivos Argentinos de Pediatria. 2016; 114(6):526-33. [DOI:10.5546/aap.2016.eng.526]
Malekpour M, Dadmehr A, Ghomrani A. [Interventional effect of sensorimotor stimulation on motor coordination in educable mentally retarded students DCD (Persian)]. Psychology of Exceptional Individuals. 2014; 4(14):63-82.
Rezaei S, Arabameri E, Sohrabi MM. [Examination of the Impact of an Eight-Week Exclusive Exercise on the Balance of Children with Developmental Coordination Disorders (Persian)]. Scientific Journal of Rehabilitation Medicine. 2017; 5(4):57-64.
Eslamdost M, Sheikh M, Mohammadi M, Ahmadi G. The effect of core stability training on static and dynamic balance in children with developmental coordination disorder. Community Health Journal. 2017; 11(2):20-8. [DOI:10.22123/chj.2018.85447].
Kubilay, N.S., et al., Effect of balance training and posture exercises on functional level in mental retardation. Fizyoterapi Rehabilitasyon. 2011; 22(2):55-64.
Wilson BN, Crawford SG, Green D, Roberts G, Aylott A, Kaplan BJ. Psychometric properties of the revised developmental coordination disorder questionnaire. Physical & Occupational Therapy in Pediatrics. 2009; 29(2):182-202. [DOI:10.1080/01942630902784761] [PMID]
Shumway-Cook A, Brauer S, Woollacott M. Predicting the probability for falls in community-dwelling older adults using the Timed Up & Go Test. Physical Therapy. 2000; 80(9):896-903. [PMID]
Hawk C, Cambron J. Chiropractic care for older adults: Effects on balance, dizziness, and chronic pain. Journal of Manipulative and Physiological Therapeutics. 2009; 32(6):431-7. [DOI:10.1016/j.jmpt.2009.06.009] [PMID]
Oviedo GR, Guerra-Balic M, Baynard T, Javierre C. Effects of aerobic, resistance and balance training in adults with intellectual disabilities. Research in Developmental Disabilities. 2014; 35(11):2624-34. [DOI:10.1016/j.ridd.2014.06.025] [PMID]
Ahmadi R, Daneshmandi H, Barati AH. [The effect of 6 weeks core stabilization training program on the balance in mentally retarded students (Persian)]. International Journal of Sport Studies. 2012; 2(10)496-501.
Taghian H, Ghasemi GA, Sadeghi M. Effect of combined exercises (strength and balance) on balance and aggression in 7-14 year-old educabe intelectual disability boys. Scientific Journal of Rehabilitation Medicine. 2017; 6(3):174-81.
Hossaini SA, Zar A, Khodadoust M, Hejazi E. The effect of eight-weekly exercise exercises on physical fitness factors of mental retardation children. Pediatric Nursing. 2017; 3(3):25-30. [DOI:10.21859/jpen-03035]
Daneshmandi H, Alizadeh MH, Gharakhanloo R. Corrective exercises (diagnosis and prescription). 14th edition. Tehran: SAMT; 2011.
Type of Study: Research |
Subject:
Special
Received: 2018/07/5 | Accepted: 2018/11/17 | Published: 2019/01/1
Received: 2018/07/5 | Accepted: 2018/11/17 | Published: 2019/01/1
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Physical Treatments (PTJ)
University of Social Welfare and Rehabilitation Sciences, Koodakyar Alley, Daneshjoo Blv., Evin, Tehran, Iran
Journal Office Tel: +9821 71732822
Publisher Tel: +9821 4535 5555, 4535 5000 (EXT: 108)
Email: physicaltreatments@gmail.com
