Thu, Apr 25, 2024
Volume 9, Issue 2 (Spring 2019)
PTJ 2019, 9(2): 97-106 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Gheitasi M, Bayattork M, Hovanloo F, Porrajab H. Comparing the Effect of a Fatigue Protocol on Kinematic Gait Parameters in Students With Genu Valgum and Genu Varum and Their Normal Peers. PTJ 2019; 9 (2) :97-106
URL: http://ptj.uswr.ac.ir/article-1-377-en.html
URL: http://ptj.uswr.ac.ir/article-1-377-en.html



1- Department of Health & Sport Rehabilitation, Sport Sciences and Health Faculty, Shahid Beheshti University, Tehran, Iran.
2- Department of Physical Education and Sport Sciences, Faculty of Letters and Humanities, University of Hormozgan, Bandar Abbas, Iran.
3- Department of Sport Pathology and Corrective Exercises, Faculty of Physical Education and Sport Sciences, Islamic Azad University Karaj, Alborz, Iran.
2- Department of Physical Education and Sport Sciences, Faculty of Letters and Humanities, University of Hormozgan, Bandar Abbas, Iran.
3- Department of Sport Pathology and Corrective Exercises, Faculty of Physical Education and Sport Sciences, Islamic Azad University Karaj, Alborz, Iran.
Full-Text [PDF 621 kb]
(1966 Downloads)
| Abstract (HTML) (2868 Views)

Finally, using the Kinovea software, time data were recorded for one gait cycle, as well as the stance time and stride length. Then, using the related formulas, the values of gait cycle length, velocity, distance covered in one minute, and the swing time were calculated.
The Shapiro-Wilk test was used to check the normal distribution of data in the study groups. The mean of indices was compared, using the repeated measures ANOVA over time and after inducing fatigue protocol in three groups. Bonferroni posthoc test was used to test the differences among the groups. All calculations were performed by SPSS V. 20, with a 95% confidence interval and at a significance level of 0.05.
3. Results
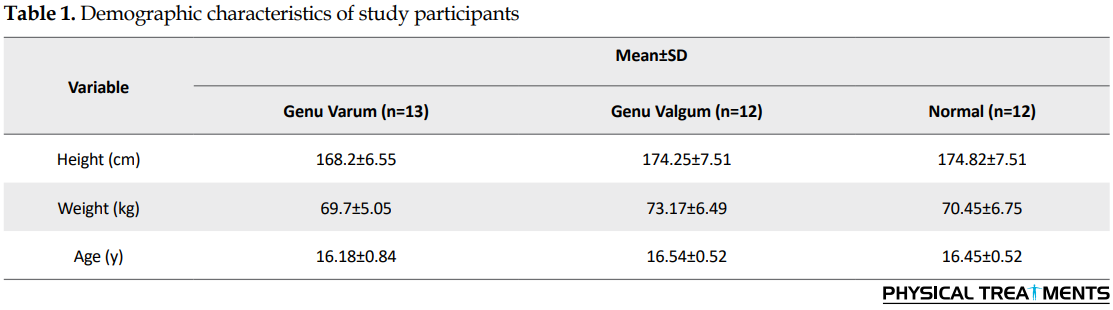
Table 1 presents the demographic characteristics of participants, while Table 2 presents data for stance time, swing time, step length, stride length, walking speed, number of steps, and walking distance for the three groups before and after inducing fatigue protocol, as well as the results of repeated measures ANOVA. As can be seen, the intra-group comparison results show that the parameters of stance time, swing time, step length, walking speed, number of steps, and walking distance were significantly different within the groups before and after inducing fatigue protocol. However, the parameter of stride length showed no significant difference within groups (P=0.055).

Moreover, according to the intergroup comparison results, there was a significant difference among three groups in terms of stance time (P<0.001), swing time (P=0.004), and stride length (P=0.001) after inducing fatigue protocol. The results of Bonferroni posthoc test showed that this difference was between genu varum and normal groups with the genu valgum group. However, in terms of step length, walking speed, number of steps, and walking distance, no significant difference was found among the three groups, although in genu valgum group after inducing fatigue protocol, the mean value of step length was more than that of other groups and their number of steps and walking distance were less than those of other groups. Furthermore, the interaction between the time factor (before and after applying the fatigue protocol) and the group factor (genu valgum, genu varum, normal) is observed only in terms of step length parameter (P<0.001).
4. Discussion
This study aimed to compare the effect of a fatigue protocol on kinematic gait parameters of students with genu valgum and genu varum and those with normal leg alignment. A significant difference was found in each group in terms of stance time, swing time, step length, walking speed, number of steps, and walking distance before and after inducing fatigue protocol except in stride length. Moreover, a significant difference was found between 3 study groups in terms of stance time, swing time, and stride length, where the genu varum group and normal peers were more significantly different than the genu valgum group.
According to the results of this study, the fatigue protocol, as an effective factor in changing the spatial variables of walking in students (adolescent boys), can change the gait pattern in them regardless of whether they have normal leg alignment or deformities (e.g. genu valgum and genu varum) in the lower extremities, especially in the knee joint. Students with genu valgum had fewer number of steps after inducing fatigue protocol compared to those with genu varum and normal peers, and their mean step length was more than that of other groups. Moreover, the distance covered by the genu valgum group compared to the other two groups after inducing fatigue protocol indicates the higher negative effect of this deformity on their walking efficiency. On the whole, the occurrence of fatigue in individuals with genu valgum leads to a change in their kinematic gait parameters, which eventually reduces one of the biomechanical outcomes of gait (distance) [1, 4, 5].
Concerning parameters of stance time, swing time, and stride length, we found a significant difference between groups after inducing fatigue protocol, where the increase in these parameters was significantly more in students with genu valgum compared to the other two groups. This finding also shows the negative effect of change in lower limb alignment in the form of deviation of the knee plate in the posterolateral direction (knock knees) on temporal gait parameters in students with genu valgum compared to other students. It can be argued that the deviation of lower limb alignment because of increased Q-angle, or in other words, the reduction of tibiofemoral angle, causes undesirable changes in temporal and spatial parameters of gait, which will eventually lead to a reduction in the mechanical advantage and efficiency of walking pattern [7, 12, 22, 26, 28].
Students with genu varum and normal peers had significantly shorter stance time than students with genu valgum after having fatigue, while no significant difference was found between genu varum and normal groups. This finding is consistent with the results of Naderi et al. [7]. They reported that stance time in a group with genu varum was almost equal to that of normal peers. Perhaps those with genu varum do not need to change or modify gait parameters to reduce the pressure on their lower limb joints. This issue is important from a biomechanical point of view. In people with genu varum, the deviation of the weight-bearing line is shifted onto the medial part and is generally compensated in the ankle joint and does not negatively affect the overall walking pattern in terms of temporal parameters.
Stief et al. also reported that individuals with genu varum, who still did not suffer from varus malalignment such as knee osteoarthritis, did not need to change their gait parameters to decrease knee joint loading, and often used postural compensatory mechanisms [29].
Considering the increase in the walking duration in samples with genu varum in the present study, it can be argued that muscle fatigue changes the gait kinematics in this group. This condition may be because of the displacement of the weight-bearing line outside the base of support, which causes the person with genu varum to spend more time to keep the balance during the stance phase [29]. Angular joint displacements and, consequently, the disturbance of optimal timing of muscle activity in lower extremity kinematic chain during walking change the magnitude of action and reaction forces between joints and ground surface. Biomechanical inefficiency in the foot plantar can cause deviations from the normal walking pattern probably because of the change in the alignment of the lower limb, and shifting the weight-bearing line onto the medial parts [19, 20, 22, 28, 29].
Students with genu varum and normal peers had a significantly longer swing time than students with genu valgum after having fatigue, while no significant difference was found between genu varum and normal groups. This finding is consistent with the results of Naderi et al. [7]. They also showed that temporal gait parameters in those with genu varum had values close to those of normal counterparts during swing and stance phases. The results indicate that subjects with genu varum do not need to change their gait parameters to reduce the pressure on the lower limb joints, probably because of postural adaptation created in proximal and distal joints. Shariati reported that the swing time during walking protocol was different between students with flat feet and their normal peers after inducing fatigue protocol [22].
Considering that people with genu valgum have somehow flatfeet or their knee alignment is affected by the decrease in the curvature of the foot plantar, the results of Shariati’s study can be compared with the results of the present study. The results of Stief et al. study showed that people with genu varum did not need to alter gait parameters to reduce the loads on the knee joint [29].
Perhaps one of the most important biomechanical features of the knee joint is that its posture as middle segment of lower limb is influenced by upper and lower joints, which is manifested in the form of compensatory postures. However, the pain, malalignment, or pathological conditions in lower limb joints are commonly compensated in the knee joint and cause changes in muscle activity patterns and decrease in the range of motion and postural adaptations in this joint, which can negatively affect the performance and efficiency of a person and his/her gait biomechanics, including the kinematic parameters [29]. Farr et al. also indicated the high biomechanical changes of the knee joint because of lower limb malalignment, especially in dynamic situations (walking) compared to the hip and ankle joints [30].
Therefore, considering the importance of knee joint in terms of dynamic stability and weight-bearing, any muscle imbalance in this joint accelerates functional and postural compensatory changes and influences the walking process and kinetic and kinematic parameters of the affected person. This theory can justify our results regarding the difference in temporal gait parameters of samples with genu valgum [29, 30].
There was no significant difference in step length among three study groups after inducing the fatigue protocol. The lower limb with multiple joints creates a unit of motion that provides stability, absorbs forces, induces pressure, and causes displacement. The function of its segments is related to each other, and their internal functioning and any change in the structure and function of one segment affect other segments.
Farr et al. also showed that although patients with genu valgum had different external knee and hip rotation and stride length compared to the controls, they had no different step length [30]. In contrast, Parijat and Lockhart reported that localized muscle fatigue affects spatial gait parameters, including step and stride lengths, which were higher in those with genu valgum compared to normal peers [25]. However, in their study, the participants were female adults, and their fatigue protocol was different from ours.
Based on the obtained results, we can indicate the importance of anthropometric dimensions, including the lower limb length in evaluating step length variable.
Moreover, the nature of the genu valgum deformity and the developed deviation in frontal (under static situation) and horizontal (under dynamic situation) plates can justify our result regarding no difference among the groups in terms of step length as a spatial variable in sagittal plate [26-29]. Based on previous studies and considering biomechanical principles ruling the walking pattern, people with normal varus alignment often compensate two variables of step length and walking speed together. Compensatory changes during the walking cycle and the hip rotation can also be another reason for the similarity between groups concerning the step length variable [29, 30]. The effect of fatigue protocol in any of the groups before and after inducing the protocol did not show a significant difference in terms of this variable.
Students with genu varum and their normal peers had significantly shorter stride length than students with genu valgum after having fatigue, while no significant difference was found between genu varum and normal groups.
Farr et al. study also showed that those with genu valgum had a significant increase in knee valgus and consequently, in stride length compared to the controls [30]. In people with genu valgum, the knees deviate to the medial part during standing. This medial deviation, which is more prominent in knee joint area, is exacerbated by fatigue and the lack of dynamic support because of the poor functioning of the muscles and can cause the knees to touch each other while walking. The most common compensatory strategy in this group is the hip rotation during the swing phase (suspended foot) around the stance leg. In static conditions, such as standing, they use the compensatory strategy of standing with feet apart by external rotation of the hip. This condition can increase the level of the base of support caused by the increased distance between two legs [28-30]. According to a study by Ganesan et al. in children, this condition is compensated by inward bending of one knee and excessive opening of another knee [31].
According to the results of this study, there was no significant difference between the effects of the fatigue protocol on the walking speed of students in three groups. The results of a study by Naderi et al. also indicated that the walking speed of those with genu varum equals to that of the normal people [7]. The lack of a significant difference between the three groups does not mean that the fatigue protocol does not affect the gait parameters (walking speed). Based on the results of the intra-group comparison, the use of fatigue protocol significantly reduced the walking speed of students in all three groups.
Based on the available scientific evidence, motor learning causes stable changes in various levels of the central nervous system. It is believed that these changes, regardless of whether they can be intentional or reactive, may recover the optimal function in any habitual and functional activity (e.g. in response to limb malalignment, postural changes, or changes in conditions).
Walking speed is one of temporal characteristics of gait and is highly influenced by the movement habits of people and the central nervous system. Perhaps one of the reasons for not finding a difference between groups is the non-interference of peripheral fatigue (muscle fatigue) with walking patterns affected by higher levels of motor control.
The results of our study also reported no significant difference between the effects of the fatigue protocol on the number of steps in the three groups. This result is consistent with the findings of studies by Naderi et al. Esmaeilipour et al. and Stief et al. They also reported that the temporal and spatial parameters of gait in those with genu varum were similar to those of normal people, where those with genu varum do not need to reduce the number of steps [12, 19, 31].
Because of the lack of significant difference in step length and walking speed variables among the study groups and the effect of these two variables on the number of steps, the lack of a significant difference seems logical. On the other hand, considering that the walking pattern of each person is a unique and exclusive characteristic and has been created and institutionalized for many years and is organized in lower levels of the central nervous system, the protocol of muscle fatigue and the presence of the subject in walking test conditions, despite fatigue, may not have a significant effect on their dominant walking pattern, although it does not mean that the fatigue protocol does not have any effect on walking speed. In other words, it can be argued that the lower limb alignment, as a biomechanical intervention, has no conditions for overcoming the neuromuscular pattern of walking in people, and changes in the lower extremity may be compensated by altering other biomechanical variables, including the center of gravity and motor patterns in the pelvic/hip regions. These are the reasons for not finding a significant difference among the study groups.
Finally, the results of this study revealed no significant difference between the effect of the fatigue protocol on the walking distance in the three groups and the distance per minute walking was not different in the groups after inducing fatigue protocol. One of the reasons for such results can be justified by the forces influencing the walking, including internal forces, forces generated by body organs (especially muscles), and external forces such as inertia, gravity, and ground reaction forces. A main part of forces (80%) that helps walk in natural conditions is external forces [32].
The type of muscle contraction used in a walking cycle includes more eccentric contractions, and because of the nature of these contractions, it can result in lower energy costs and higher muscular work efficiency. The three types of contractions produce the internal forces consistently and regularly, each of which performs positive or negative works considering the direction of displacement and forces, and eventually causes movement [12, 30].
Because of the lack of significant difference among the groups in terms of step length and walking speed variables and considering that the walking distance parameter is affected by the two variables, the lack of significant difference among the groups in terms of the walking distance is justified. Although walking in any person may be affected by other factors such as age, gender, height, size and shape of bones, joint mobility, muscle strength, habit, and physical and mental state, it can vary depending on the step length and gait speed and has a positive or negative effect on the covered distance and other gait parameters [32].
Based on the results of this study, the fatigue protocol applied as an environmental and muscular intervention could change the walking pattern considering the difference in lower limb alignment in students with genu valgum and genu varum, as well as those with normal alignment. The changes between the groups were different, and the effect of induced fatigue protocol on them was significant. Lower limb malalignment, including genu valgum and genu varum in adolescent male students, can be a determining factor for motor patterns such as walking; hence, fatigue can lead to different changes in some gait parameters, especially in people with genu valgum and genu varum, which calls for more attention to corrective programs for the improvement of varus deformities.
Ethical Considerations
Compliance with ethical guidelines
All ethical principles were considered in this article and all of the participants completed the written consent form. Also, this study was confirmed by ethic committee of Islamic Azad University of Karaj.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not for profit sectors.
Authors' contributions
All authors contributed in designing, running, and writing all parts of the research.
Conflict of interests
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank the staff and authorities of high schools in the Qods District for their valuable cooperation.
Refrences
Full-Text: (1254 Views)
1. Introduction
Human walking has always been a matter of concern. One of the special gait characteristics is the unique walking style of each person [1]. The normal walking in humans is rhythmic and is the result of a series of alternating movements of the lower limbs, which basically supports the movements of the trunk, head, and upper limbs. During walking, the head, upper limbs, and trunk should be balanced on one lower limb and transferred from one limb to another. The weight of these parts, as well as the weight of the lower limbs that are removed from the ground and moved forward when walking must be supported by one limb [2].
Scholars believe that walking is affected by impairment in the human motor system, from serious lesions of the central nervous system to minor deficits, such as functional limitation in the ankle or knee joints and even in the upper limbs [3].
The knee joint is the most important joint that causes stability and weight-bearing during gait, and any abnormality in this joint leads to instability and functional impairment [4, 5]. Among the most common abnormalities in this area, the postural deformities, including genu valgum (knock knees) and genu varum (bowlegs) have been investigated in several studies and their high prevalence, especially among children and adolescents, have been reported [6, 7]. Such deformities in the lower limb can disturb the line of gravity relative to the base of support and, finally, cause significant changes in the balance index and movement strategies [8]. Genu valgum causes the displacement of the weight-bearing line to the lateral part of the knee joint and increases the compressive forces over this part, while in genu varum, the weight-bearing line moves towards the medial part and increases the compressive forces over this area [9, 10]. This discrepancy disturbs the distribution of weight and causes instability in weight-bearing conditions, especially in dynamic situations such as walking [11].
Studies have shown that the mechanical axis deviation of the lower limb at various levels such as deformities in sagittal and frontal (genu valgum and genu varum) planes, which is more common in knee joint than in the other joints (because of a 3-dimensional deviation) , leads to changes in the internal and external force patterns, including the deviation of ground reaction forces and challenges postural control strategies during stance and gait [12, 13]. In another study, it has been shown that deformities in the knee (genu valgum and genu varum) and ankle (pronation or supination) cause poor postural control when standing on one leg [14]. This condition can change the location of the center of pressure on the foot plantar and make it difficult to maintain and restore balance [15].
Based on the study of Van Gheluwe et al. genu valgum can cause subtalar pronation moment at the contact phase and subtalar supination moment in the early propulsive phase, while genu varum causes subtalar pronation moment in both phases. The increase in pronation and supination moments changes the torque of the gravity force and increases the pressure and mechanical load resulting from weight-bearing and displacement activities [16]. This condition may cause excessive muscular energy consumption, fatigue, and loss of posture stability when standing on two legs, disturb the optimized movement pattern in dynamic situations such as walking, and end in prolonged prolific damages [17].
The effect of genu valgum and genu varum on the mechanical axis deviation of knee joint and the effect of pronation and supination moment on the mechanical axis deviation of ankle joint show that lower limb deficiency, including postural deviation of the knee area, is an important factor in the biomechanical characteristics of motor function in children and adolescents, especially during walking [1]. Several factors such as neuromuscular diseases, cerebrospinal lesions, joint injuries, and fatigue affect gait biomechanics and, as a result, alter the pattern of muscle activity and energy consumption.
Fatigue is defined as an inability to maintain the production of the necessary level of strength for physical activity [18]. It reduces voluntary power and the functional capacity of muscles, disrupts the simultaneous activation of agonist and antagonistic muscles, and ultimately decreases the function and efficiency of the musculoskeletal and nervous systems [19, 20]. Factors affecting fatigue include central and environmental factors [18]. Fatigue of muscles around a joint known as local fatigue changes the movement pattern and joint position sense and causes muscle co-contraction, which increases the likelihood of joint injury [21].
Fatigue is one of the factors influencing postural and gait control [22]. Barbieri et al. in a study on inactive and normal people showed that muscle fatigue affects kinetic and kinematic parameters of walking, regardless of the level of physical activity of individuals and gait [23]. In a study on the effect of fatigue on walking parameters of students with flat foot and normal peers, Shariati reported that fatigue protocol could have a different effect on some of the gait parameters in people with foot deformity [22]. Granacher et al. reported that fatigue protocol significantly decreased gait velocity and stride length in young adults, while it increased these parameters in older adults [24]. The fatigue of the muscle group in the knee joint may affect gait parameters because of repeated daily activities or various exercises [20, 25].
Given the importance and role of walking and gait patterns, the identification of abnormal gait patterns and providing appropriate corrective programs are possible only by having full knowledge of gait biomechanics. In this regard, this study aimed at comparing the effect of a fatigue protocol on some kinematic gait parameters of students with genu valgum and genu varum and their normal counterparts.
2. Materials and Methods
The study population consisted of all high school male students in Qods District, Tehran City, Iran. Firstly, 400 students aged 15 to 16 years from 4 schools entered into the study based on the inclusion criteria. In the second phase (screening), 110 students were selected (53 with genu varum, 26 with genu valgum, and 31 with normal alignment). They were examined for lower limb alignment assessment to determine the severity of the deformity. At the end, 37 were selected as study samples and divided into three groups of genu varum (n=13), genu valgum (n=12), and normal (n=12).
In the genu varum group, the distance between two knee medial epicondyles was >30mm, while in the genu valgum group, the distance between medial ankle bones was >30 mm [26]. In the normal group, under various standing conditions (weight-bearing situation), there was no distance between medial knee epicondyles and medial ankle bones; and the goniometry-based quadriceps angle (Q) was in a range of about 5±10 degrees [27].
The inclusion criteria consisted of no history of injury (bone fracture, ligament, and tear) in the lower limb, no shortening or asymmetry of lower limbs, no spinal abnormalities or deviations in other areas of the lower limb (except knee abnormalities) or any specific disease, no history of being athlete, normal Body Mass Index (BMI) (18≤ BMI ≤24 kg/m2), and parents’ written consent for voluntary participation in the study. On the other hand, the exclusion criteria were being reluctant to continue the study or leave it at the posttest phase.
To assess and determine the severity of knee deformity, the Q-angle of left and right feet was measured and recorded under weight-bearing situation while the subject was standing on both legs, and the knee and hip joints were fully extended and natural, and the quadriceps muscle was relaxed [7, 12]. For measurement, a universal goniometer (1° accuracy) was used [26].
Before measurement, the center of the patella, tibial tuberosity, and anterior superior iliac spine were found, and the area was marked. The goniometer axis was positioned over the center of the patella while its long arm was toward the anterior superior iliac spine and its short arm on tibial tuberosity (anatomical axis of the lower limb) [6].
To determine the severity of genu valgum and genu varum deformities quantitatively, an industrial caliper (1° accuracy) was used. To measure the genu varum, while the subject was at standing and relaxed position and his or her medial ankle bones were close to each other without any pressure and abnormal contraction, the distance between two knee medial epicondyles was measured in anterior view and recorded in millimeters. For genu valgum measurement, at the same positions and condition and when knee medial epicondyles were closed to each other, the distance between two medial ankle bones was measured in posterior view and recorded in millimeters [6-9].
To induce fatigue (intermediate variable), the standardized protocol of sit-to-stand movements was used [23]. For this purpose, an ergonomic chair with a dimension of height =43cm, width =41cm, and length =42cm without side flaps were used. The subject was, then, asked to perform sit-to-stand movements (30 repetitions per minute each for two seconds) while the arms were stretched across the chest. During standing, the knees must be completely open.
The fatigue protocol stops when the examiner finds out that the subject cannot move naturally and based on the correct pattern or cannot complete the repetition of movements at the appointed time. The time between performing fatigue protocol and walk test was considered three minutes so that no full recovery could be made [22-25].
A standard 10-m walk test was used to assess the kinematic gait parameters (Figure 1) [28]. A Full HD Camcorder (Sony HDR-CX900) with a shutter speed of 120 fps was used for cinematography. The camera was positioned 80 cm from the base, at a distance of 230 cm from the subject in the middle 10 m walkway indicated by two obstacles. The subject was asked to walk at a normal speed. Then, from the middle of the distance (5 m), the shooting was started and recorded. The test was performed three times and the average result of these three times was considered as the final result of the test for analysis [3]. This test was performed for each subject before and after inducing fatigue protocol, and 15 minutes was determined for resting before performing the fatigue protocol.
Human walking has always been a matter of concern. One of the special gait characteristics is the unique walking style of each person [1]. The normal walking in humans is rhythmic and is the result of a series of alternating movements of the lower limbs, which basically supports the movements of the trunk, head, and upper limbs. During walking, the head, upper limbs, and trunk should be balanced on one lower limb and transferred from one limb to another. The weight of these parts, as well as the weight of the lower limbs that are removed from the ground and moved forward when walking must be supported by one limb [2].
Scholars believe that walking is affected by impairment in the human motor system, from serious lesions of the central nervous system to minor deficits, such as functional limitation in the ankle or knee joints and even in the upper limbs [3].
The knee joint is the most important joint that causes stability and weight-bearing during gait, and any abnormality in this joint leads to instability and functional impairment [4, 5]. Among the most common abnormalities in this area, the postural deformities, including genu valgum (knock knees) and genu varum (bowlegs) have been investigated in several studies and their high prevalence, especially among children and adolescents, have been reported [6, 7]. Such deformities in the lower limb can disturb the line of gravity relative to the base of support and, finally, cause significant changes in the balance index and movement strategies [8]. Genu valgum causes the displacement of the weight-bearing line to the lateral part of the knee joint and increases the compressive forces over this part, while in genu varum, the weight-bearing line moves towards the medial part and increases the compressive forces over this area [9, 10]. This discrepancy disturbs the distribution of weight and causes instability in weight-bearing conditions, especially in dynamic situations such as walking [11].
Studies have shown that the mechanical axis deviation of the lower limb at various levels such as deformities in sagittal and frontal (genu valgum and genu varum) planes, which is more common in knee joint than in the other joints (because of a 3-dimensional deviation) , leads to changes in the internal and external force patterns, including the deviation of ground reaction forces and challenges postural control strategies during stance and gait [12, 13]. In another study, it has been shown that deformities in the knee (genu valgum and genu varum) and ankle (pronation or supination) cause poor postural control when standing on one leg [14]. This condition can change the location of the center of pressure on the foot plantar and make it difficult to maintain and restore balance [15].
Based on the study of Van Gheluwe et al. genu valgum can cause subtalar pronation moment at the contact phase and subtalar supination moment in the early propulsive phase, while genu varum causes subtalar pronation moment in both phases. The increase in pronation and supination moments changes the torque of the gravity force and increases the pressure and mechanical load resulting from weight-bearing and displacement activities [16]. This condition may cause excessive muscular energy consumption, fatigue, and loss of posture stability when standing on two legs, disturb the optimized movement pattern in dynamic situations such as walking, and end in prolonged prolific damages [17].
The effect of genu valgum and genu varum on the mechanical axis deviation of knee joint and the effect of pronation and supination moment on the mechanical axis deviation of ankle joint show that lower limb deficiency, including postural deviation of the knee area, is an important factor in the biomechanical characteristics of motor function in children and adolescents, especially during walking [1]. Several factors such as neuromuscular diseases, cerebrospinal lesions, joint injuries, and fatigue affect gait biomechanics and, as a result, alter the pattern of muscle activity and energy consumption.
Fatigue is defined as an inability to maintain the production of the necessary level of strength for physical activity [18]. It reduces voluntary power and the functional capacity of muscles, disrupts the simultaneous activation of agonist and antagonistic muscles, and ultimately decreases the function and efficiency of the musculoskeletal and nervous systems [19, 20]. Factors affecting fatigue include central and environmental factors [18]. Fatigue of muscles around a joint known as local fatigue changes the movement pattern and joint position sense and causes muscle co-contraction, which increases the likelihood of joint injury [21].
Fatigue is one of the factors influencing postural and gait control [22]. Barbieri et al. in a study on inactive and normal people showed that muscle fatigue affects kinetic and kinematic parameters of walking, regardless of the level of physical activity of individuals and gait [23]. In a study on the effect of fatigue on walking parameters of students with flat foot and normal peers, Shariati reported that fatigue protocol could have a different effect on some of the gait parameters in people with foot deformity [22]. Granacher et al. reported that fatigue protocol significantly decreased gait velocity and stride length in young adults, while it increased these parameters in older adults [24]. The fatigue of the muscle group in the knee joint may affect gait parameters because of repeated daily activities or various exercises [20, 25].
Given the importance and role of walking and gait patterns, the identification of abnormal gait patterns and providing appropriate corrective programs are possible only by having full knowledge of gait biomechanics. In this regard, this study aimed at comparing the effect of a fatigue protocol on some kinematic gait parameters of students with genu valgum and genu varum and their normal counterparts.
2. Materials and Methods
The study population consisted of all high school male students in Qods District, Tehran City, Iran. Firstly, 400 students aged 15 to 16 years from 4 schools entered into the study based on the inclusion criteria. In the second phase (screening), 110 students were selected (53 with genu varum, 26 with genu valgum, and 31 with normal alignment). They were examined for lower limb alignment assessment to determine the severity of the deformity. At the end, 37 were selected as study samples and divided into three groups of genu varum (n=13), genu valgum (n=12), and normal (n=12).
In the genu varum group, the distance between two knee medial epicondyles was >30mm, while in the genu valgum group, the distance between medial ankle bones was >30 mm [26]. In the normal group, under various standing conditions (weight-bearing situation), there was no distance between medial knee epicondyles and medial ankle bones; and the goniometry-based quadriceps angle (Q) was in a range of about 5±10 degrees [27].
The inclusion criteria consisted of no history of injury (bone fracture, ligament, and tear) in the lower limb, no shortening or asymmetry of lower limbs, no spinal abnormalities or deviations in other areas of the lower limb (except knee abnormalities) or any specific disease, no history of being athlete, normal Body Mass Index (BMI) (18≤ BMI ≤24 kg/m2), and parents’ written consent for voluntary participation in the study. On the other hand, the exclusion criteria were being reluctant to continue the study or leave it at the posttest phase.
To assess and determine the severity of knee deformity, the Q-angle of left and right feet was measured and recorded under weight-bearing situation while the subject was standing on both legs, and the knee and hip joints were fully extended and natural, and the quadriceps muscle was relaxed [7, 12]. For measurement, a universal goniometer (1° accuracy) was used [26].
Before measurement, the center of the patella, tibial tuberosity, and anterior superior iliac spine were found, and the area was marked. The goniometer axis was positioned over the center of the patella while its long arm was toward the anterior superior iliac spine and its short arm on tibial tuberosity (anatomical axis of the lower limb) [6].
To determine the severity of genu valgum and genu varum deformities quantitatively, an industrial caliper (1° accuracy) was used. To measure the genu varum, while the subject was at standing and relaxed position and his or her medial ankle bones were close to each other without any pressure and abnormal contraction, the distance between two knee medial epicondyles was measured in anterior view and recorded in millimeters. For genu valgum measurement, at the same positions and condition and when knee medial epicondyles were closed to each other, the distance between two medial ankle bones was measured in posterior view and recorded in millimeters [6-9].
To induce fatigue (intermediate variable), the standardized protocol of sit-to-stand movements was used [23]. For this purpose, an ergonomic chair with a dimension of height =43cm, width =41cm, and length =42cm without side flaps were used. The subject was, then, asked to perform sit-to-stand movements (30 repetitions per minute each for two seconds) while the arms were stretched across the chest. During standing, the knees must be completely open.
The fatigue protocol stops when the examiner finds out that the subject cannot move naturally and based on the correct pattern or cannot complete the repetition of movements at the appointed time. The time between performing fatigue protocol and walk test was considered three minutes so that no full recovery could be made [22-25].
A standard 10-m walk test was used to assess the kinematic gait parameters (Figure 1) [28]. A Full HD Camcorder (Sony HDR-CX900) with a shutter speed of 120 fps was used for cinematography. The camera was positioned 80 cm from the base, at a distance of 230 cm from the subject in the middle 10 m walkway indicated by two obstacles. The subject was asked to walk at a normal speed. Then, from the middle of the distance (5 m), the shooting was started and recorded. The test was performed three times and the average result of these three times was considered as the final result of the test for analysis [3]. This test was performed for each subject before and after inducing fatigue protocol, and 15 minutes was determined for resting before performing the fatigue protocol.
Finally, using the Kinovea software, time data were recorded for one gait cycle, as well as the stance time and stride length. Then, using the related formulas, the values of gait cycle length, velocity, distance covered in one minute, and the swing time were calculated.
The Shapiro-Wilk test was used to check the normal distribution of data in the study groups. The mean of indices was compared, using the repeated measures ANOVA over time and after inducing fatigue protocol in three groups. Bonferroni posthoc test was used to test the differences among the groups. All calculations were performed by SPSS V. 20, with a 95% confidence interval and at a significance level of 0.05.
3. Results
Table 1 presents the demographic characteristics of participants, while Table 2 presents data for stance time, swing time, step length, stride length, walking speed, number of steps, and walking distance for the three groups before and after inducing fatigue protocol, as well as the results of repeated measures ANOVA. As can be seen, the intra-group comparison results show that the parameters of stance time, swing time, step length, walking speed, number of steps, and walking distance were significantly different within the groups before and after inducing fatigue protocol. However, the parameter of stride length showed no significant difference within groups (P=0.055).
Moreover, according to the intergroup comparison results, there was a significant difference among three groups in terms of stance time (P<0.001), swing time (P=0.004), and stride length (P=0.001) after inducing fatigue protocol. The results of Bonferroni posthoc test showed that this difference was between genu varum and normal groups with the genu valgum group. However, in terms of step length, walking speed, number of steps, and walking distance, no significant difference was found among the three groups, although in genu valgum group after inducing fatigue protocol, the mean value of step length was more than that of other groups and their number of steps and walking distance were less than those of other groups. Furthermore, the interaction between the time factor (before and after applying the fatigue protocol) and the group factor (genu valgum, genu varum, normal) is observed only in terms of step length parameter (P<0.001).
4. Discussion
This study aimed to compare the effect of a fatigue protocol on kinematic gait parameters of students with genu valgum and genu varum and those with normal leg alignment. A significant difference was found in each group in terms of stance time, swing time, step length, walking speed, number of steps, and walking distance before and after inducing fatigue protocol except in stride length. Moreover, a significant difference was found between 3 study groups in terms of stance time, swing time, and stride length, where the genu varum group and normal peers were more significantly different than the genu valgum group.
According to the results of this study, the fatigue protocol, as an effective factor in changing the spatial variables of walking in students (adolescent boys), can change the gait pattern in them regardless of whether they have normal leg alignment or deformities (e.g. genu valgum and genu varum) in the lower extremities, especially in the knee joint. Students with genu valgum had fewer number of steps after inducing fatigue protocol compared to those with genu varum and normal peers, and their mean step length was more than that of other groups. Moreover, the distance covered by the genu valgum group compared to the other two groups after inducing fatigue protocol indicates the higher negative effect of this deformity on their walking efficiency. On the whole, the occurrence of fatigue in individuals with genu valgum leads to a change in their kinematic gait parameters, which eventually reduces one of the biomechanical outcomes of gait (distance) [1, 4, 5].
Concerning parameters of stance time, swing time, and stride length, we found a significant difference between groups after inducing fatigue protocol, where the increase in these parameters was significantly more in students with genu valgum compared to the other two groups. This finding also shows the negative effect of change in lower limb alignment in the form of deviation of the knee plate in the posterolateral direction (knock knees) on temporal gait parameters in students with genu valgum compared to other students. It can be argued that the deviation of lower limb alignment because of increased Q-angle, or in other words, the reduction of tibiofemoral angle, causes undesirable changes in temporal and spatial parameters of gait, which will eventually lead to a reduction in the mechanical advantage and efficiency of walking pattern [7, 12, 22, 26, 28].
Students with genu varum and normal peers had significantly shorter stance time than students with genu valgum after having fatigue, while no significant difference was found between genu varum and normal groups. This finding is consistent with the results of Naderi et al. [7]. They reported that stance time in a group with genu varum was almost equal to that of normal peers. Perhaps those with genu varum do not need to change or modify gait parameters to reduce the pressure on their lower limb joints. This issue is important from a biomechanical point of view. In people with genu varum, the deviation of the weight-bearing line is shifted onto the medial part and is generally compensated in the ankle joint and does not negatively affect the overall walking pattern in terms of temporal parameters.
Stief et al. also reported that individuals with genu varum, who still did not suffer from varus malalignment such as knee osteoarthritis, did not need to change their gait parameters to decrease knee joint loading, and often used postural compensatory mechanisms [29].
Considering the increase in the walking duration in samples with genu varum in the present study, it can be argued that muscle fatigue changes the gait kinematics in this group. This condition may be because of the displacement of the weight-bearing line outside the base of support, which causes the person with genu varum to spend more time to keep the balance during the stance phase [29]. Angular joint displacements and, consequently, the disturbance of optimal timing of muscle activity in lower extremity kinematic chain during walking change the magnitude of action and reaction forces between joints and ground surface. Biomechanical inefficiency in the foot plantar can cause deviations from the normal walking pattern probably because of the change in the alignment of the lower limb, and shifting the weight-bearing line onto the medial parts [19, 20, 22, 28, 29].
Students with genu varum and normal peers had a significantly longer swing time than students with genu valgum after having fatigue, while no significant difference was found between genu varum and normal groups. This finding is consistent with the results of Naderi et al. [7]. They also showed that temporal gait parameters in those with genu varum had values close to those of normal counterparts during swing and stance phases. The results indicate that subjects with genu varum do not need to change their gait parameters to reduce the pressure on the lower limb joints, probably because of postural adaptation created in proximal and distal joints. Shariati reported that the swing time during walking protocol was different between students with flat feet and their normal peers after inducing fatigue protocol [22].
Considering that people with genu valgum have somehow flatfeet or their knee alignment is affected by the decrease in the curvature of the foot plantar, the results of Shariati’s study can be compared with the results of the present study. The results of Stief et al. study showed that people with genu varum did not need to alter gait parameters to reduce the loads on the knee joint [29].
Perhaps one of the most important biomechanical features of the knee joint is that its posture as middle segment of lower limb is influenced by upper and lower joints, which is manifested in the form of compensatory postures. However, the pain, malalignment, or pathological conditions in lower limb joints are commonly compensated in the knee joint and cause changes in muscle activity patterns and decrease in the range of motion and postural adaptations in this joint, which can negatively affect the performance and efficiency of a person and his/her gait biomechanics, including the kinematic parameters [29]. Farr et al. also indicated the high biomechanical changes of the knee joint because of lower limb malalignment, especially in dynamic situations (walking) compared to the hip and ankle joints [30].
Therefore, considering the importance of knee joint in terms of dynamic stability and weight-bearing, any muscle imbalance in this joint accelerates functional and postural compensatory changes and influences the walking process and kinetic and kinematic parameters of the affected person. This theory can justify our results regarding the difference in temporal gait parameters of samples with genu valgum [29, 30].
There was no significant difference in step length among three study groups after inducing the fatigue protocol. The lower limb with multiple joints creates a unit of motion that provides stability, absorbs forces, induces pressure, and causes displacement. The function of its segments is related to each other, and their internal functioning and any change in the structure and function of one segment affect other segments.
Farr et al. also showed that although patients with genu valgum had different external knee and hip rotation and stride length compared to the controls, they had no different step length [30]. In contrast, Parijat and Lockhart reported that localized muscle fatigue affects spatial gait parameters, including step and stride lengths, which were higher in those with genu valgum compared to normal peers [25]. However, in their study, the participants were female adults, and their fatigue protocol was different from ours.
Based on the obtained results, we can indicate the importance of anthropometric dimensions, including the lower limb length in evaluating step length variable.
Moreover, the nature of the genu valgum deformity and the developed deviation in frontal (under static situation) and horizontal (under dynamic situation) plates can justify our result regarding no difference among the groups in terms of step length as a spatial variable in sagittal plate [26-29]. Based on previous studies and considering biomechanical principles ruling the walking pattern, people with normal varus alignment often compensate two variables of step length and walking speed together. Compensatory changes during the walking cycle and the hip rotation can also be another reason for the similarity between groups concerning the step length variable [29, 30]. The effect of fatigue protocol in any of the groups before and after inducing the protocol did not show a significant difference in terms of this variable.
Students with genu varum and their normal peers had significantly shorter stride length than students with genu valgum after having fatigue, while no significant difference was found between genu varum and normal groups.
Farr et al. study also showed that those with genu valgum had a significant increase in knee valgus and consequently, in stride length compared to the controls [30]. In people with genu valgum, the knees deviate to the medial part during standing. This medial deviation, which is more prominent in knee joint area, is exacerbated by fatigue and the lack of dynamic support because of the poor functioning of the muscles and can cause the knees to touch each other while walking. The most common compensatory strategy in this group is the hip rotation during the swing phase (suspended foot) around the stance leg. In static conditions, such as standing, they use the compensatory strategy of standing with feet apart by external rotation of the hip. This condition can increase the level of the base of support caused by the increased distance between two legs [28-30]. According to a study by Ganesan et al. in children, this condition is compensated by inward bending of one knee and excessive opening of another knee [31].
According to the results of this study, there was no significant difference between the effects of the fatigue protocol on the walking speed of students in three groups. The results of a study by Naderi et al. also indicated that the walking speed of those with genu varum equals to that of the normal people [7]. The lack of a significant difference between the three groups does not mean that the fatigue protocol does not affect the gait parameters (walking speed). Based on the results of the intra-group comparison, the use of fatigue protocol significantly reduced the walking speed of students in all three groups.
Based on the available scientific evidence, motor learning causes stable changes in various levels of the central nervous system. It is believed that these changes, regardless of whether they can be intentional or reactive, may recover the optimal function in any habitual and functional activity (e.g. in response to limb malalignment, postural changes, or changes in conditions).
Walking speed is one of temporal characteristics of gait and is highly influenced by the movement habits of people and the central nervous system. Perhaps one of the reasons for not finding a difference between groups is the non-interference of peripheral fatigue (muscle fatigue) with walking patterns affected by higher levels of motor control.
The results of our study also reported no significant difference between the effects of the fatigue protocol on the number of steps in the three groups. This result is consistent with the findings of studies by Naderi et al. Esmaeilipour et al. and Stief et al. They also reported that the temporal and spatial parameters of gait in those with genu varum were similar to those of normal people, where those with genu varum do not need to reduce the number of steps [12, 19, 31].
Because of the lack of significant difference in step length and walking speed variables among the study groups and the effect of these two variables on the number of steps, the lack of a significant difference seems logical. On the other hand, considering that the walking pattern of each person is a unique and exclusive characteristic and has been created and institutionalized for many years and is organized in lower levels of the central nervous system, the protocol of muscle fatigue and the presence of the subject in walking test conditions, despite fatigue, may not have a significant effect on their dominant walking pattern, although it does not mean that the fatigue protocol does not have any effect on walking speed. In other words, it can be argued that the lower limb alignment, as a biomechanical intervention, has no conditions for overcoming the neuromuscular pattern of walking in people, and changes in the lower extremity may be compensated by altering other biomechanical variables, including the center of gravity and motor patterns in the pelvic/hip regions. These are the reasons for not finding a significant difference among the study groups.
Finally, the results of this study revealed no significant difference between the effect of the fatigue protocol on the walking distance in the three groups and the distance per minute walking was not different in the groups after inducing fatigue protocol. One of the reasons for such results can be justified by the forces influencing the walking, including internal forces, forces generated by body organs (especially muscles), and external forces such as inertia, gravity, and ground reaction forces. A main part of forces (80%) that helps walk in natural conditions is external forces [32].
The type of muscle contraction used in a walking cycle includes more eccentric contractions, and because of the nature of these contractions, it can result in lower energy costs and higher muscular work efficiency. The three types of contractions produce the internal forces consistently and regularly, each of which performs positive or negative works considering the direction of displacement and forces, and eventually causes movement [12, 30].
Because of the lack of significant difference among the groups in terms of step length and walking speed variables and considering that the walking distance parameter is affected by the two variables, the lack of significant difference among the groups in terms of the walking distance is justified. Although walking in any person may be affected by other factors such as age, gender, height, size and shape of bones, joint mobility, muscle strength, habit, and physical and mental state, it can vary depending on the step length and gait speed and has a positive or negative effect on the covered distance and other gait parameters [32].
Based on the results of this study, the fatigue protocol applied as an environmental and muscular intervention could change the walking pattern considering the difference in lower limb alignment in students with genu valgum and genu varum, as well as those with normal alignment. The changes between the groups were different, and the effect of induced fatigue protocol on them was significant. Lower limb malalignment, including genu valgum and genu varum in adolescent male students, can be a determining factor for motor patterns such as walking; hence, fatigue can lead to different changes in some gait parameters, especially in people with genu valgum and genu varum, which calls for more attention to corrective programs for the improvement of varus deformities.
Ethical Considerations
Compliance with ethical guidelines
All ethical principles were considered in this article and all of the participants completed the written consent form. Also, this study was confirmed by ethic committee of Islamic Azad University of Karaj.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not for profit sectors.
Authors' contributions
All authors contributed in designing, running, and writing all parts of the research.
Conflict of interests
The authors declared no conflict of interest.
Acknowledgments
The authors would like to thank the staff and authorities of high schools in the Qods District for their valuable cooperation.
Refrences
- Mazinani E. [Comparing the kinematic parameters of the depressed students with normal weight, overweight and obesein (Persian)] [MSc. thesis]. Karaj: Azad University of Karaj Branch; 2015.
- Molaee kandagh M. Comparison of kinematic walking parameters of male students with flat feet and normal 18-16 year olds. (Persian)] [MSc. thesis]. Karaj: Azad University of Karaj Branch; 2014.
- Ahmadi E. [The effect of carrying a back pack on walking kinematic parameters of 10-12 year-old male children with lumbar and healthy lordosis. (Persian)] [MSc. Thesis]. Karaj: Azad University of Karaj Branch; 2014.
- Tanamas S, Hanna FS, Cicuttini FM, Wluka AE, Berry P, Urquhart DM. Does knee malalignment increase the risk of development and progression of knee osteoarthritis? A systematic review. Arthritis Care & Research. 2009; 61(4):459-67. [DOI:10.1002/art.24336] [PMID]
- Brouwer GM, van Tol AW, Bergink AP, Belo JN, Bernsen RM, Reijman M, et al. Association between valgus and varus alignment and the development and progression of radiographic osteoarthritis of the knee. Arthritis & Rheumatism. 2007; 56(4):1204-11. [DOI:10.1002/art.22515] [PMID]
- Agaja SB. Factors affecting angular deformities of the knees in Nigerian children: Llorin experience. West African Journal of Medicine. 2001; 20(4):246-50. [PMID]
- Naderi S, Mohammadi Pour F, Amir Seifo Dini MR. [Effect of different walking speed on the gait kinematics of individuals with knee varus (Persian)]. Scientific Journals Management System. 2015; 13(9):63-73. [DOI:10.18869/acadpub.jsmt.13.9.63]
- Bakhtiyari AH, Fatemi E, soltani A. [The effect of knee varus deformity on increasing postural oscillations and increasing risk (Persian)]. Komesh. 2012; 13(3):
- Levangie PK, Norkin CC. Joint structure and function. 4rd edition. Philadelphia: FA. Davis Company; 2005.
- Kendall FP, McCreary EK, Province PG, Rodgers MM, Romanin WA. Muscle testing and function with posture and pain, 5th edition. Philadelphia: Lippincott Williams & Wilkins; 2005.
- Anker LC, Weerdesteyn V, van Nes IJ, Nienhuis B, Straatman H, Geurts AC. The relation between postural stability and weight distribution in healthy subjects. Gait & Posture. 2008; 27(3):471-7. [DOI:10.1016/j.gaitpost.2007.06.002] [PMID]
- Naderi S, Mohamadipour F, Amirseifolahi AR. [The effect of various treadmill slopes and speeds on the kinematics of walking in people with parental knee varus (Persian)] [MSc. Thesis]. Karaj: Azad University of Karaj Branch; 2014.
- Desai SS, Shetty GM, Song HR, Lee SH, Kim TY, Hur CY. Effect of foot deformity on conventional mechanical axis deviation and ground mechanical axis deviation during single leg stance and two leg stance in genu varum. The Knee. 2007; 14(6):452-7. [DOI:10.1016/j.knee.2007.07.009] [PMID]
- Tsai LC, Yu B, Mercer VS, Gross MT. Comparison of different structural foot types for measures of standing postural control. Journal of Orthopaedic & Sports Physical Therapy. 2006; 36(12):942-53. [DOI:10.2519/jospt.2006.2336] [PMID]
- Van Gheluwe B, Kirby KA, Hagman F. Effects of simulated genu valgum and genu varum on ground reaction forces and subtalar joint function during gait. Journal of the American Podiatric Medical Association. 2005; 95(6):531-41. [DOI:10.7547/0950531] [PMID]
- Shubert TE, McCulloch K, Hartman M, Giuliani CA. The effect of an exercise-based balance intervention on physical and cognitive performance for older adults: A pilot study. Journal of Geriatric Physical Therapy. 2010; 33(4):157-64. [PMID]
- Cote KP, Brunet ME, Gansneder BM, Shultz SJ. Effects of pronated and supinated foot postures on static and dynamic postural stability. Journal of Athletic Training. 2005; 40(1):41-6. [PMID] [PMCID]
- Paillard T. Effects of general and local fatigue on postural control: A review. Neuroscience & Biobehavioral Reviews. 2012; 36(1):162-76. [DOI:10.1016/j.neubiorev.2011.05.009] [PMID]
- Esmaeilipour S, Shojaeddin SS, Khaleghi M. [The effect of local fatigue on selective parameters of kinematic gait in males with genu varum (Persian)]. Razi Journal of Medical Sciences. 2018; 25(168):30-8.
- Anbarian M, Esmailie H, Hosseini Nejad, Rabiei M, Binabaji H. [Comparison of knee joint muscle’s activity in subjects with genu varum and the controls during walking and running (Persian)]. Journal of Rehabilitation Sciences. 2011; 8(2):298-309.
- Hatfield G. The effects of quadriceps impairment on lower limb kinematics, kinetics and muscle activation during gait in young adults [MSc. thesis]. Halifax: Dalhousie University; 2009.
- Shariati H. [The effect of a fatigue protocol on same kinematic walking parameters in students with foot abnormalities (Persian)] [MSc. Thesis]. Karaj: Azad University of Karaj Branch; 2014.
- Barbieri FA, Lee YJ, Gobbi LT, Pijnappels M, Van Dieën JH. The effect of muscle fatigue on the last stride before stepping down a curb. Gait & Posture. 2013; 37(4):542-6. [DOI:10.1016/j.gaitpost.2012.09.015] [PMID]
- Granacher U, Wolf I, Wehrle A, Bridenbaugh S, Kressig RW. Effects of muscle fatigue on gait characteristics under single and dual-task conditions in young and older adults. Journal of Neuro Engineering and Rehabilitation. 2010; 7:56. [DOI:10.1186/1743-0003-7-56] [PMID] [PMCID]
- Parijat P, Lockhart TE. Effects of lower extremity muscle fatigue on the outcomes of slip-induced falls. Ergonomics. 2008; 51(12):1873-84. [DOI:10.1080/00140130802567087] [PMID] [PMCID]
- Gheitasi M, Alizadeh MH, Rajabi R. [Is Q-angle a factor in the damage of the ligament and Minisk casualties of the elite freelance wrestlers? (Persian)]. Harekat. 2009; 39(1):5-20.
- Alizadeh MH, Gheitasi M. Fundamental concepts of corrective exercises. Tehran: Sport Scince Research Center; 2012.
- Pirpiris M, Wilkinson AJ, Rodda J, Nguyen TC, Baker RJ, Nattrass GR, et al. Walking speed in children and young adults with neuromuscular disease: Comparison between two assessment methods. Journal of Pediatric Orthopaedics. 2003; 23(3):302-7. [DOI:10.1097/01241398-200305000-00006] [PMID]
- Stief F, Böhm H, Schwirtz A, Dussa CU, Döderlein L. Dynamic loading of the knee and hip joint and compensatory strategies in children and adolescents with varus malalignment. Gait & Posture. 2011; 33(3):490-5. [DOI:10.1016/j.gaitpost.2011.01.001] [PMID]
- Farr S, Kranzl A, Pablik E, Kaipel M, Ganger R. Functional and radiographic consideration of lower limb malalignment in children and adolescents with idiopathic genu valgum. Journal of Orthopaedic Research. 2014; 32(10):1362-70. [DOI:10.1002/jor.22684] [PMID]
- Ganesan B, Fong KN, Luximon A, Al-Jumaily A. Kinetic and kinematic analysis of gait pattern of 13-year-old children with unilateral genu valgum. European Review for Medical and Pharmacological Sciences. 2016; 20(15):3168-71. [PMID]
- Hoch MC, Weinhandl JT. Effect of valgus knee alignment on gait biomechanics in healthy women. Journal of Electromyography and Kinesiology. 2017; 35:17-23. [DOI:10.1016/j.jelekin.2017.05.003] [PMID]
Type of Study: Applicable |
Subject:
Special
Received: 2019/02/22 | Accepted: 2019/05/14 | Published: 2019/11/12
Received: 2019/02/22 | Accepted: 2019/05/14 | Published: 2019/11/12
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Physical Treatments (PTJ)
University of Social Welfare and Rehabilitation Sciences, Koodakyar Alley, Daneshjoo Blv., Evin, Tehran, Iran
Journal Office Tel: +9821 71732822
Publisher Tel: +9821 4535 5555, 4535 5000 (EXT: 108)
Email: physicaltreatments@gmail.com
