Thu, Apr 18, 2024
Volume 7, Issue 1 (Spring 2017)
PTJ 2017, 7(1): 13-18 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Rastgar Koutenaei F, Mosallanezhad Z, Naghikhani M, Ezati K, Biglarian A, Nouroozi M et al . The Effect of Low Level Laser Therapy on Pain and Range of Motion of Patients With Knee Osteoarthritis. PTJ 2017; 7 (1) :13-18
URL: http://ptj.uswr.ac.ir/article-1-313-en.html
URL: http://ptj.uswr.ac.ir/article-1-313-en.html
Forouzan Rastgar Koutenaei1 
 , Zahra Mosallanezhad * 1, Mehrdad Naghikhani1 , Kamran Ezati2 , Akbar Biglarian3 , Mahdi Nouroozi4 , Maryam Ghodrati1
, Zahra Mosallanezhad * 1, Mehrdad Naghikhani1 , Kamran Ezati2 , Akbar Biglarian3 , Mahdi Nouroozi4 , Maryam Ghodrati1
, Zahra Mosallanezhad * 1, Mehrdad Naghikhani1 , Kamran Ezati2 , Akbar Biglarian3 , Mahdi Nouroozi4 , Maryam Ghodrati1
1- Department of Physiotherapy, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
2- Department of Physical Therapy, School of Medicine, Guilan University of Medical Sciences, Guilan, Iran.
3- Department of Biostatistics,University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
4- Social Determinants of Health Research Center, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
2- Department of Physical Therapy, School of Medicine, Guilan University of Medical Sciences, Guilan, Iran.
3- Department of Biostatistics,University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
4- Social Determinants of Health Research Center, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
Full-Text [PDF 505 kb]
(2850 Downloads)
| Abstract (HTML) (7909 Views)


Full-Text: (2781 Views)
1. Introduction
steoarthritis is one of the most common chronic diseases of the joints with many physical and psychological complications as well as huge costs for society [1, 2]. Prevalence of osteoarthritis is rising because of obesity and population aging [3, 4]. The knee joint is one of the most common joints that is affected by osteoarthritis [5-7]. Half of the people older than 50 years report some pain in their knees during a year and about 25% of those who reach the age of 50, report knee pain [5]. Women are more affected than men [1, 8]. The disease occurs when the dynamic balance between destruction and repair of knee cartilage tissue is interrupted [1, 3, 9] and often where mechanical stress is more than that could be tolerated by joint tissue [9]. Osteoarthritis of the knee is characterized by destruction of articular cartilage, muscle atrophy, and dysfunction of the ligament; clinical manifestations of the disease include joint pain, stiffness, decreased motion, deepening changes, and disruption of daily activities [1, 9].
Osteoarthrosis has no definitive cure [10-12], however, some treatments are recommended [3, 9, 13]. One of the non-invasive treatments for knee osteoarthritis is application of laser power. Given the inflammatory nature of osteoarthritis, laser therapy is believed to be effective by reducing inflammation [9, 11, 14]. It also promotes fibroblasts, collagen synthesis, cell oxygen recovery, and bone remodeling [7, 12]. Recently, low-power laser has gained popularity in physiotherapy, but the effectiveness of the laser is still controversial [15]. Laser efficacy depends on 4 factors of wavelength, duration of treatment, dose, and areas of the application [4, 13, 16]. High prevalence of osteoarthritis and its effect on quality of life highlights the importance of identifying the appropriate approach to treat it. This study aimed to investigate the effectiveness of a low-power laser in reducing pain and increasing the range of motion, compared to placebo laser group. The laser was administered with a wavelength of 810 nm and power of 100 mW at 8 points around the knee for two weeks.
2. Materials and Methods
This study was a double-blind clinical trial study, which was conducted in Shahed Clinic, Tehran, Iran. In this study, 40 patients (men and women) participated with knee osteoarthritis. Orthopedics practitioner evaluated patients before entering the study.
Inclusion criteria included diagnosis of knee joint osteoarthritis based on diagnostic criteria of the American College of Rheumatology and doctor’s diagnosis, radiographic image with intensity of 2 to 4 based on the category of Kellgren and Lawrence, having at least three months of knee pain, aged between 40 and 60 years, acute and chronic osteoarthritis, at least three months of having passed since the last physiotherapy, and severity of pain between 3 and 10 based on the visual scale of pain. In addition, exclusion criteria comprised taking anti-inflammatory drugs during the study, having hip osteoarthritis symptoms; any disease that has laser counter-indication such as diabetes and cancer, history of surgery and trauma to the knee, neurological diseases, and various types of rheumatologic diseases.
A total of 40 people with knee osteoarthritis voluntarily participated in this study based on inclusion and exclusion criteria and were assigned randomly (using random blocks) in the intervention group (real laser therapy, conventional physiotherapy, and therapeutic exercise) and the control group (placebo treatment, conventional physiotherapy, and exercise therapy). Treatment was provided for both groups 5 sessions per week and for 10 sessions. Sports exercises that were given to both groups included training for lower limbs with straight knee in supine position and isometric contraction of the quadriceps muscle 30 times a day.
In this research, we used the Metron laser model B-860 (made in Australia) with a wavelength of 810 nm, the power of 100 mW and the diameter of 5 mm. Eight points (three points on the inside of the knee, three points on the outside of the knee, and two on the internal edges of the tendon of the muscle of the biceps femoris and tandinosis in the popliteal cavity) were emitted with a dose of 7 Jules per point for 70 seconds with a total dose of 56 Jules at each session. The placebo group also lasted for 70 seconds in these places, but the laser had no output. Assessments including pain intensity in rest and activity (walking) were conducted with the help of the visual scale of pain measurement and measuring the flexion and extension of the knee with goniometer. These assessments were done before the intervention, after the intervention, and finally after 2 weeks of follow-up.
This study was confirmed and conducted at the Research Ethics Committee of the University of Social Welfare and Rehabilitation Sciences and ethics principles, including providing sufficient explanations to the participants, information confidentiality and so on were observed and their informed consent forms were obtained.Data analyses were done by repeated measurement test using SPSS Version 20.
3. Results
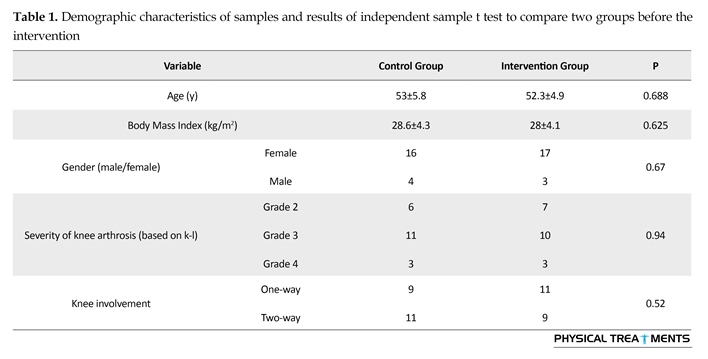
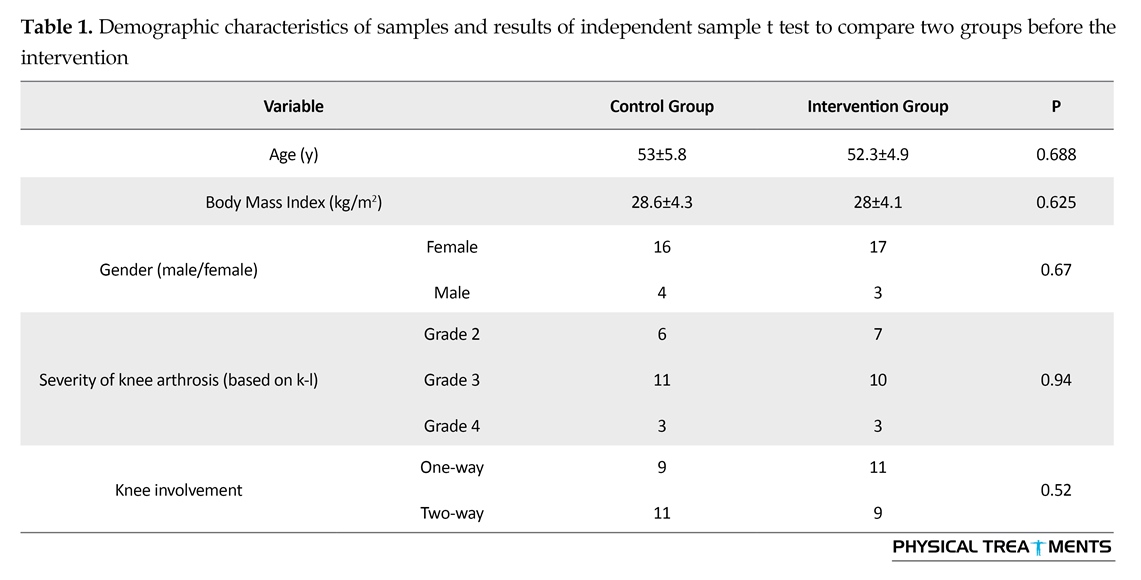
Table 1 presents the demographic characteristics of samples. Also, to evaluate the effectiveness of low-power laser after two weeks, first the Kolmogorov-Smirnov test was performed among the intervention and control groups, and given the normal distribution of data, parametric t test was used to examine the similarity of the two groups before treatment. Moreover, to study the effect and stability of low-power laser, the repeated measurement method was used and the results are presented in Tables 2 and 3.
According to Table 3, the intervention significantly decreased the pain variable in the rest mode over time (P<0.0001). However, the variable effect of the group was not significant, i.e. there was no significant difference between the mean scores of pain in the resting mode (P=0.691). According to Table 3, there was no significant difference between the mean scores of pain at the rest (P=0.691). Also there was no significant difference between the mean scores of active mode (P=0.751) and the variable effect of the group was not significant.
However, the variable effect of the group was not significant, i.e. there was no significant difference between the mean scores of knee flexion movement range (P=0.435). Moreover, intervention caused a significant decrease in the variable of knee extension movement range (P<0.0001). However, the variable effect of the group was not significant, i.e. there was no significant difference between the mean scores of knee extension movement range (P=0.885).
4. Discussion
This study showed that the effectiveness of low-power laser in reducing pain and improving the range of motion in patients with knee osteoarthritis is similar to the effectiveness of the placebo laser. Low-power laser is recognized as an appropriate medical modality to treat knee osteoarthritis in animals and humans and can be used along with acupuncture or exercise [17]. Studies have shown that laser reduces inflammation [18-20]. Evidence strongly suggests that laser can reduce acute pain with modulation of inflammatory markers such as PGE2, mRNA Cox 2, IL-1β, TNFα [21]. Moreover, laser can repair joint cartilage, proliferate cartilage cells, and synthesize and secret the extracellular matrix [22]. Ohshiro study showed that the laser had positive effects on blood flow and temperature, and thereby on reducing pain [23].
According to the Global Laser Association, the lowest density energy useful for treating knee arthritis is 4 Jules at any point and a wavelength of 780-860 or 904 nm, 2 weeks duration of treatment every day or up to 3 and 4 weeks every other day [12]. In Tascioqu et al. study, one group received laser with a wavelength of 830 nm and a dose of 1.5 Jules at any point, other group received laser with 3 Jules per point, and the other group which was placebo received no intervention. The treatment continued for 2 weeks and 10 sessions but the laser therapy could not reduce pain [24]. However, in Fudka et al. study, a laser with a wavelength of 904 nm was used in patients with knee osteoarthritis for three days a week
steoarthritis is one of the most common chronic diseases of the joints with many physical and psychological complications as well as huge costs for society [1, 2]. Prevalence of osteoarthritis is rising because of obesity and population aging [3, 4]. The knee joint is one of the most common joints that is affected by osteoarthritis [5-7]. Half of the people older than 50 years report some pain in their knees during a year and about 25% of those who reach the age of 50, report knee pain [5]. Women are more affected than men [1, 8]. The disease occurs when the dynamic balance between destruction and repair of knee cartilage tissue is interrupted [1, 3, 9] and often where mechanical stress is more than that could be tolerated by joint tissue [9]. Osteoarthritis of the knee is characterized by destruction of articular cartilage, muscle atrophy, and dysfunction of the ligament; clinical manifestations of the disease include joint pain, stiffness, decreased motion, deepening changes, and disruption of daily activities [1, 9].
Osteoarthrosis has no definitive cure [10-12], however, some treatments are recommended [3, 9, 13]. One of the non-invasive treatments for knee osteoarthritis is application of laser power. Given the inflammatory nature of osteoarthritis, laser therapy is believed to be effective by reducing inflammation [9, 11, 14]. It also promotes fibroblasts, collagen synthesis, cell oxygen recovery, and bone remodeling [7, 12]. Recently, low-power laser has gained popularity in physiotherapy, but the effectiveness of the laser is still controversial [15]. Laser efficacy depends on 4 factors of wavelength, duration of treatment, dose, and areas of the application [4, 13, 16]. High prevalence of osteoarthritis and its effect on quality of life highlights the importance of identifying the appropriate approach to treat it. This study aimed to investigate the effectiveness of a low-power laser in reducing pain and increasing the range of motion, compared to placebo laser group. The laser was administered with a wavelength of 810 nm and power of 100 mW at 8 points around the knee for two weeks.
2. Materials and Methods
This study was a double-blind clinical trial study, which was conducted in Shahed Clinic, Tehran, Iran. In this study, 40 patients (men and women) participated with knee osteoarthritis. Orthopedics practitioner evaluated patients before entering the study.
Inclusion criteria included diagnosis of knee joint osteoarthritis based on diagnostic criteria of the American College of Rheumatology and doctor’s diagnosis, radiographic image with intensity of 2 to 4 based on the category of Kellgren and Lawrence, having at least three months of knee pain, aged between 40 and 60 years, acute and chronic osteoarthritis, at least three months of having passed since the last physiotherapy, and severity of pain between 3 and 10 based on the visual scale of pain. In addition, exclusion criteria comprised taking anti-inflammatory drugs during the study, having hip osteoarthritis symptoms; any disease that has laser counter-indication such as diabetes and cancer, history of surgery and trauma to the knee, neurological diseases, and various types of rheumatologic diseases.
A total of 40 people with knee osteoarthritis voluntarily participated in this study based on inclusion and exclusion criteria and were assigned randomly (using random blocks) in the intervention group (real laser therapy, conventional physiotherapy, and therapeutic exercise) and the control group (placebo treatment, conventional physiotherapy, and exercise therapy). Treatment was provided for both groups 5 sessions per week and for 10 sessions. Sports exercises that were given to both groups included training for lower limbs with straight knee in supine position and isometric contraction of the quadriceps muscle 30 times a day.
In this research, we used the Metron laser model B-860 (made in Australia) with a wavelength of 810 nm, the power of 100 mW and the diameter of 5 mm. Eight points (three points on the inside of the knee, three points on the outside of the knee, and two on the internal edges of the tendon of the muscle of the biceps femoris and tandinosis in the popliteal cavity) were emitted with a dose of 7 Jules per point for 70 seconds with a total dose of 56 Jules at each session. The placebo group also lasted for 70 seconds in these places, but the laser had no output. Assessments including pain intensity in rest and activity (walking) were conducted with the help of the visual scale of pain measurement and measuring the flexion and extension of the knee with goniometer. These assessments were done before the intervention, after the intervention, and finally after 2 weeks of follow-up.
This study was confirmed and conducted at the Research Ethics Committee of the University of Social Welfare and Rehabilitation Sciences and ethics principles, including providing sufficient explanations to the participants, information confidentiality and so on were observed and their informed consent forms were obtained.Data analyses were done by repeated measurement test using SPSS Version 20.
3. Results
Table 1 presents the demographic characteristics of samples. Also, to evaluate the effectiveness of low-power laser after two weeks, first the Kolmogorov-Smirnov test was performed among the intervention and control groups, and given the normal distribution of data, parametric t test was used to examine the similarity of the two groups before treatment. Moreover, to study the effect and stability of low-power laser, the repeated measurement method was used and the results are presented in Tables 2 and 3.
According to Table 3, the intervention significantly decreased the pain variable in the rest mode over time (P<0.0001). However, the variable effect of the group was not significant, i.e. there was no significant difference between the mean scores of pain in the resting mode (P=0.691). According to Table 3, there was no significant difference between the mean scores of pain at the rest (P=0.691). Also there was no significant difference between the mean scores of active mode (P=0.751) and the variable effect of the group was not significant.
However, the variable effect of the group was not significant, i.e. there was no significant difference between the mean scores of knee flexion movement range (P=0.435). Moreover, intervention caused a significant decrease in the variable of knee extension movement range (P<0.0001). However, the variable effect of the group was not significant, i.e. there was no significant difference between the mean scores of knee extension movement range (P=0.885).
4. Discussion
This study showed that the effectiveness of low-power laser in reducing pain and improving the range of motion in patients with knee osteoarthritis is similar to the effectiveness of the placebo laser. Low-power laser is recognized as an appropriate medical modality to treat knee osteoarthritis in animals and humans and can be used along with acupuncture or exercise [17]. Studies have shown that laser reduces inflammation [18-20]. Evidence strongly suggests that laser can reduce acute pain with modulation of inflammatory markers such as PGE2, mRNA Cox 2, IL-1β, TNFα [21]. Moreover, laser can repair joint cartilage, proliferate cartilage cells, and synthesize and secret the extracellular matrix [22]. Ohshiro study showed that the laser had positive effects on blood flow and temperature, and thereby on reducing pain [23].
According to the Global Laser Association, the lowest density energy useful for treating knee arthritis is 4 Jules at any point and a wavelength of 780-860 or 904 nm, 2 weeks duration of treatment every day or up to 3 and 4 weeks every other day [12]. In Tascioqu et al. study, one group received laser with a wavelength of 830 nm and a dose of 1.5 Jules at any point, other group received laser with 3 Jules per point, and the other group which was placebo received no intervention. The treatment continued for 2 weeks and 10 sessions but the laser therapy could not reduce pain [24]. However, in Fudka et al. study, a laser with a wavelength of 904 nm was used in patients with knee osteoarthritis for three days a week

and 9 sessions. In this study every point was emitted with 3 Jules power and finally the study result showed effectiveness of laser, compared with the placebo in reducing pain and improving function [22]. Our study was similar to Bulow et al. study who emitted laser with wavelength of 830 nm and a total dose of 22.5 Jules on 9 points around the knee. Both the active laser and placebo groups induced improvement in patients and there was no significant difference between two groups [25]. In a blinded clinical trial carried out in 2015 by Meneses et al. in Brazil, low-power laser effects (904 nm) and static stroke exercises were administered and investigated in

patients with osteoarthritis. At the end, this study confirmed the effectiveness of low-power laser and arthrosis training in the treatment of patients with knee osteoarthritis, but it acknowledged that the dose and frequency for laser therapy should be determined and the present study was also consistent with the results of their study [9]. A systematic review study was published in 2014 that reviewed 9 clinical trials. The researchers concluded that the evidence does not support low-power laser as a proper treatment for osteoarthritis and the main factors in the effectiveness of the laser are wavelength selection, frequency, and appropriate dose [12].
One of the reasons for the difference in the outcome of this study with previous studies, relates to control group. In previous studies, low-power laser was compared with placebo, but in the present study patients in the control group received routine physiotherapy in addition to low-power laser treatment. In addition, previous studies mostly reported short-term effect of low-power laser, but in the present study, the long-term impact of the laser was measured. In this study, wavelength selection frequency and laser dose was administrated similar to past studies protocols (due to the limitations of the laser device) and therefore, low-power laser was used. It is recommended that in future studies, the effectiveness of different wavelengths, laser frequencies, and doses be compared with each other and also the effect of low-power laser be compared with high-power laser. According to the study results, the effectiveness of low-power laser in reducing pain and improving the range of motion in patients with knee arthritis is similar to the effectiveness of the placebo laser.
Acknowledgments
The authors are grateful of all participants for their contribution to the present study. The study was supported by the Department of Physiotherapy at the University of Social Welfare and Rehabilitation Sciences. We also thank the Shahed Clinic that supported the place and devises for visiting the patients.
Conflict of Interest
The authors declared no conflicts of interest.
Reference
[1]Litwic A, Edwards MH, Dennison EM, Cooper C. Epidemiology and burden of osteoarthritis. British Medical Bulletin. 2013; 105(1):185-99. doi: 10.1093/bmb/lds038
[2]Arden N, Nevitt MC. Osteoarthritis: Epidemiology. Best Practice & Research Clinical Rheumatology. 2006; 20(1):3-25. doi: 10.1016/j.berh.2005.09.007
[3]Bijlsma JW, Berenbaum F, Lafeber FP. Osteoarthritis: An update with relevance for clinical practice. The Lancet. 2011; 377(9783):2115-26. doi: 10.1016/s0140-6736(11)60243-2
[4]Al Rashoud A, Abboud R, Wang W, Wigderowitz C. Efficacy of low-level laser therapy applied at acupuncture points in knee osteoarthritis: A randomised double-blind comparative trial. Physiotherapy. 2014; 100(3):242-8. doi: 10.1016/j.physio.2013.09.007
[5]Blagojevic M, Jinks C, Jeffery A, Jordan K. Risk factors for onset of osteoarthritis of the knee in older adults: A systematic review and meta-analysis. Osteoarthritis and Cartilage. 2010; 18(1):24-33. doi: 10.1016/j.joca.2009.08.010
[6]Assis L, Milares LP, Almeida T, Tim C, Magri A, Fernandes KR, et al. Aerobic exercise training and low-level laser therapy modulate inflammatory response and degenerative process in an experimental model of knee osteoarthritis in rats. Osteoarthritis and Cartilage. 2016; 24(1):169-77. doi: 10.1016/j.joca.2015.07.020
[7]De Faria Coelho C, Leal-Junior ECP, Biasotto-Gonzalez DA, Bley AS, Politti F, De Oliveira Gonzalez T, et al. Effectiveness of phototherapy incorporated into an exercise program for osteoarthritis of the knee: Study protocol for a randomized controlled trial. Trials. 2014; 15(1):221. doi: 10.1186/1745-6215-15-221
[8]Lawrence RC, Felson DT, Helmick CG, Arnold LM, Choi H, Deyo RA, et al. Estimates of the prevalence of arthritis and other rheumatic conditions in the United States: Part II. Arthritis & Rheumatism. 2008; 58(1):26-35. doi: 10.1002/art.23176
[9]De Meneses SRF, Hunter DJ, Docko EY, Marques AP. Effect of low-level laser therapy (904 nm) and static stretching in patients with knee osteoarthritis: A 10.1186/s12891-015-0709-9 protocol of randomised controlled trial. BMC Musculoskeletal Disorders. 2015; 16(1):252. doi:
Das SK, Farooqi A. Osteoarthritis. Best Practice & Research Clinical Rheumatology. 2008; 22(4):657–75. doi: 10.1016/j.berh.2008.07.002
[10]Siebuhr A, Petersen KK, Arendt-Nielsen L, Egsgaard LL, Eskehave T, Christiansen C, et al. Identification and characterisation of osteoarthritis patients with inflammation derived tissue turnover. Osteoarthritis and Cartilage. 2014; 22(1):44-50. doi: 10.1016/j.joca.2013.10.020
[11]Huang Z, Chen J, Ma J, Shen B, Pei F, Kraus VB. Effectiveness of low-level laser therapy in patients with knee osteoarthritis: A systematic review and meta-analysis. Osteoarthritis and Cartilage. 2015; 23(9):1437-44. doi: 10.1016/j.joca.2015.04.005
[12]Alghadir A, Omar MTA, Al-Askar AB, Al-Muteri NK. Effect of low-level laser therapy in patients with chronic knee osteoarthritis: A single-blinded randomized clinical study.
[13]Lasers in Medical Science. 2014; 29(2):749-55. doi: 10.1007/s10103-013-1393-3
[14]Sanchez-Ramirez DC, van der Leeden M, van der Esch M, Roorda LD, Verschueren S, van Dieën JH, et al. Elevated C-reactive protein is associated with lower increase in knee muscle strength in patients with knee osteoarthritis: A 2-year follow-up study in the Amsterdam Osteoarthritis (AMS-OA) cohort. Arthritis Research & Therapy. 2014; 16(3):R123. doi: 10.1186/ar4580
[15]Gur A, Cosut A, Jale Sarac A, Cevik R, Nas K, Uyar A. Efficacy of different therapy regimes of low‐power laser in painful osteoarthritis of the knee: A double‐blind and randomized‐controlled trial. Lasers in Surgery and Medicine. 2003; 33(5):330-8. doi: 10.1002/lsm.10236
[16]Alfredo PP, Bjordal JM, Dreyer SH, Meneses SRF, Zaguetti G, Ovanessian V, et al. Efficacy of low level laser therapy associated with exercises in knee osteoarthritis: A randomized double-blind study. Clinical Rehabilitation. 2012; 26(6):523-33. doi: 10.1177/0269215511425962
[17]Kheshie AR, Alayat MSM, Ali MME. High-intensity versus low-level laser therapy in the treatment of patients with knee osteoarthritis: A randomized controlled trial. Lasers in Medical Science. 2014; 29(4):1371-6. doi: 10.1007/s10103-014-1529-0
[18]Bjordal J, Lopes-Martins R, Iversen V. A randomised, placebo controlled trial of low level laser therapy for activated Achilles tendinitis with microdialysis measurement of peritendinous prostaglandin E2 concentrations. British Journal of Sports Medicine. 2006; 40(1):76-80. doi: 10.1136/bjsm.2005.020842
[19]Castano AP, Dai T, Yaroslavsky I, Cohen R, Apruzzese WA, Smotrich MH, et al. Low‐level laser therapy for zymosan‐induced arthritis in rats: Importance of illumination time. Lasers in Surgery and Medicine. 2007; 39(6):543-50. doi: 10.1002/lsm.20516
[20]Rubio CR, Cremonezzi D, Moya M, Soriano F, Palma J, Campana V. Helium-neon laser reduces the inflammatory process of arthritis. Photomedicine and Laser Surgery. 2010; 28(1):125-9. doi: 10.1089/pho.2008.2472
[21]Bjordal JM, Johnson MI, Iversen V, Aimbire F, Lopes-Martins RAB. Low-level laser therapy in acute pain: A systematic review of possible mechanisms of action and clinical effects in randomized placebo-controlled trials. Photomedicine and Laser Therapy. 2006; 24(2):158-68. doi: 10.1089/pho.2006.24.158
[22]Fukuda VO, Fukuda TY, Guimarães M, Shiwa S, de Lima BDC, Martins RÁBL, et al. Short-term efficacy of low-level laser therapy in patients with knee osteoarthritis: A randomized placebo-controlled, double-blind clinical trial. Revista Brasileira de Ortopedia (English Edition). 2011; 46(5):526-33. doi: 10.1016/s2255-4971(15)30407-9
[23]Hegedűs B, Viharos L, Gervain M, Gálfi M. The effect of low-level laser in knee osteoarthritis: A double-blind, randomized, placebo-controlled trial. Photomedicine and Laser Surgery. 2009; 27(4):577-84. doi: 10.1089/pho.2008.2297
[24]Tascioglu F, Armagan O, Tabak Y, Corapci I, Oner C. Low power laser treatment in patients with knee osteoarthritis. Swiss Medical Weekly. 2004; 134(17-18):254-8. doi: PMID: 15243853
[25]Bülow P, Jensen H, Danneskiold-Samsøe B. Low power Ga-Al-As laser treatment of painful osteoarthritis of the knee. A double-blind placebo-controlled study. Scandinavian Journal of Rehabilitation Medicine. 1994; 26(3):155-9. PMID: 7801065
One of the reasons for the difference in the outcome of this study with previous studies, relates to control group. In previous studies, low-power laser was compared with placebo, but in the present study patients in the control group received routine physiotherapy in addition to low-power laser treatment. In addition, previous studies mostly reported short-term effect of low-power laser, but in the present study, the long-term impact of the laser was measured. In this study, wavelength selection frequency and laser dose was administrated similar to past studies protocols (due to the limitations of the laser device) and therefore, low-power laser was used. It is recommended that in future studies, the effectiveness of different wavelengths, laser frequencies, and doses be compared with each other and also the effect of low-power laser be compared with high-power laser. According to the study results, the effectiveness of low-power laser in reducing pain and improving the range of motion in patients with knee arthritis is similar to the effectiveness of the placebo laser.
Acknowledgments
The authors are grateful of all participants for their contribution to the present study. The study was supported by the Department of Physiotherapy at the University of Social Welfare and Rehabilitation Sciences. We also thank the Shahed Clinic that supported the place and devises for visiting the patients.
Conflict of Interest
The authors declared no conflicts of interest.
Reference
[1]Litwic A, Edwards MH, Dennison EM, Cooper C. Epidemiology and burden of osteoarthritis. British Medical Bulletin. 2013; 105(1):185-99. doi: 10.1093/bmb/lds038
[2]Arden N, Nevitt MC. Osteoarthritis: Epidemiology. Best Practice & Research Clinical Rheumatology. 2006; 20(1):3-25. doi: 10.1016/j.berh.2005.09.007
[3]Bijlsma JW, Berenbaum F, Lafeber FP. Osteoarthritis: An update with relevance for clinical practice. The Lancet. 2011; 377(9783):2115-26. doi: 10.1016/s0140-6736(11)60243-2
[4]Al Rashoud A, Abboud R, Wang W, Wigderowitz C. Efficacy of low-level laser therapy applied at acupuncture points in knee osteoarthritis: A randomised double-blind comparative trial. Physiotherapy. 2014; 100(3):242-8. doi: 10.1016/j.physio.2013.09.007
[5]Blagojevic M, Jinks C, Jeffery A, Jordan K. Risk factors for onset of osteoarthritis of the knee in older adults: A systematic review and meta-analysis. Osteoarthritis and Cartilage. 2010; 18(1):24-33. doi: 10.1016/j.joca.2009.08.010
[6]Assis L, Milares LP, Almeida T, Tim C, Magri A, Fernandes KR, et al. Aerobic exercise training and low-level laser therapy modulate inflammatory response and degenerative process in an experimental model of knee osteoarthritis in rats. Osteoarthritis and Cartilage. 2016; 24(1):169-77. doi: 10.1016/j.joca.2015.07.020
[7]De Faria Coelho C, Leal-Junior ECP, Biasotto-Gonzalez DA, Bley AS, Politti F, De Oliveira Gonzalez T, et al. Effectiveness of phototherapy incorporated into an exercise program for osteoarthritis of the knee: Study protocol for a randomized controlled trial. Trials. 2014; 15(1):221. doi: 10.1186/1745-6215-15-221
[8]Lawrence RC, Felson DT, Helmick CG, Arnold LM, Choi H, Deyo RA, et al. Estimates of the prevalence of arthritis and other rheumatic conditions in the United States: Part II. Arthritis & Rheumatism. 2008; 58(1):26-35. doi: 10.1002/art.23176
[9]De Meneses SRF, Hunter DJ, Docko EY, Marques AP. Effect of low-level laser therapy (904 nm) and static stretching in patients with knee osteoarthritis: A 10.1186/s12891-015-0709-9 protocol of randomised controlled trial. BMC Musculoskeletal Disorders. 2015; 16(1):252. doi:
Das SK, Farooqi A. Osteoarthritis. Best Practice & Research Clinical Rheumatology. 2008; 22(4):657–75. doi: 10.1016/j.berh.2008.07.002
[10]Siebuhr A, Petersen KK, Arendt-Nielsen L, Egsgaard LL, Eskehave T, Christiansen C, et al. Identification and characterisation of osteoarthritis patients with inflammation derived tissue turnover. Osteoarthritis and Cartilage. 2014; 22(1):44-50. doi: 10.1016/j.joca.2013.10.020
[11]Huang Z, Chen J, Ma J, Shen B, Pei F, Kraus VB. Effectiveness of low-level laser therapy in patients with knee osteoarthritis: A systematic review and meta-analysis. Osteoarthritis and Cartilage. 2015; 23(9):1437-44. doi: 10.1016/j.joca.2015.04.005
[12]Alghadir A, Omar MTA, Al-Askar AB, Al-Muteri NK. Effect of low-level laser therapy in patients with chronic knee osteoarthritis: A single-blinded randomized clinical study.
[13]Lasers in Medical Science. 2014; 29(2):749-55. doi: 10.1007/s10103-013-1393-3
[14]Sanchez-Ramirez DC, van der Leeden M, van der Esch M, Roorda LD, Verschueren S, van Dieën JH, et al. Elevated C-reactive protein is associated with lower increase in knee muscle strength in patients with knee osteoarthritis: A 2-year follow-up study in the Amsterdam Osteoarthritis (AMS-OA) cohort. Arthritis Research & Therapy. 2014; 16(3):R123. doi: 10.1186/ar4580
[15]Gur A, Cosut A, Jale Sarac A, Cevik R, Nas K, Uyar A. Efficacy of different therapy regimes of low‐power laser in painful osteoarthritis of the knee: A double‐blind and randomized‐controlled trial. Lasers in Surgery and Medicine. 2003; 33(5):330-8. doi: 10.1002/lsm.10236
[16]Alfredo PP, Bjordal JM, Dreyer SH, Meneses SRF, Zaguetti G, Ovanessian V, et al. Efficacy of low level laser therapy associated with exercises in knee osteoarthritis: A randomized double-blind study. Clinical Rehabilitation. 2012; 26(6):523-33. doi: 10.1177/0269215511425962
[17]Kheshie AR, Alayat MSM, Ali MME. High-intensity versus low-level laser therapy in the treatment of patients with knee osteoarthritis: A randomized controlled trial. Lasers in Medical Science. 2014; 29(4):1371-6. doi: 10.1007/s10103-014-1529-0
[18]Bjordal J, Lopes-Martins R, Iversen V. A randomised, placebo controlled trial of low level laser therapy for activated Achilles tendinitis with microdialysis measurement of peritendinous prostaglandin E2 concentrations. British Journal of Sports Medicine. 2006; 40(1):76-80. doi: 10.1136/bjsm.2005.020842
[19]Castano AP, Dai T, Yaroslavsky I, Cohen R, Apruzzese WA, Smotrich MH, et al. Low‐level laser therapy for zymosan‐induced arthritis in rats: Importance of illumination time. Lasers in Surgery and Medicine. 2007; 39(6):543-50. doi: 10.1002/lsm.20516
[20]Rubio CR, Cremonezzi D, Moya M, Soriano F, Palma J, Campana V. Helium-neon laser reduces the inflammatory process of arthritis. Photomedicine and Laser Surgery. 2010; 28(1):125-9. doi: 10.1089/pho.2008.2472
[21]Bjordal JM, Johnson MI, Iversen V, Aimbire F, Lopes-Martins RAB. Low-level laser therapy in acute pain: A systematic review of possible mechanisms of action and clinical effects in randomized placebo-controlled trials. Photomedicine and Laser Therapy. 2006; 24(2):158-68. doi: 10.1089/pho.2006.24.158
[22]Fukuda VO, Fukuda TY, Guimarães M, Shiwa S, de Lima BDC, Martins RÁBL, et al. Short-term efficacy of low-level laser therapy in patients with knee osteoarthritis: A randomized placebo-controlled, double-blind clinical trial. Revista Brasileira de Ortopedia (English Edition). 2011; 46(5):526-33. doi: 10.1016/s2255-4971(15)30407-9
[23]Hegedűs B, Viharos L, Gervain M, Gálfi M. The effect of low-level laser in knee osteoarthritis: A double-blind, randomized, placebo-controlled trial. Photomedicine and Laser Surgery. 2009; 27(4):577-84. doi: 10.1089/pho.2008.2297
[24]Tascioglu F, Armagan O, Tabak Y, Corapci I, Oner C. Low power laser treatment in patients with knee osteoarthritis. Swiss Medical Weekly. 2004; 134(17-18):254-8. doi: PMID: 15243853
[25]Bülow P, Jensen H, Danneskiold-Samsøe B. Low power Ga-Al-As laser treatment of painful osteoarthritis of the knee. A double-blind placebo-controlled study. Scandinavian Journal of Rehabilitation Medicine. 1994; 26(3):155-9. PMID: 7801065
Type of Study: Research |
Subject:
Special
Received: 2016/10/23 | Accepted: 2017/01/16 | Published: 2017/04/1
Received: 2016/10/23 | Accepted: 2017/01/16 | Published: 2017/04/1
References
1. Litwic A, Edwards MH, Dennison EM, Cooper C. Epidemiology and burden of osteoarthritis. British Medical Bulletin. 2013; 105(1):185-99. doi: 10.1093/bmb/lds038 [DOI:10.1093/bmb/lds038]
2. Arden N, Nevitt MC. Osteoarthritis: Epidemiology. Best Practice & Research Clinical Rheumatology. 2006; 20(1):3-25. doi: 10.1016/j.berh.2005.09.007 [DOI:10.1016/j.berh.2005.09.007]
3. Bijlsma JW, Berenbaum F, Lafeber FP. Osteoarthritis: An update with relevance for clinical practice. The Lancet. 2011; 377(9783):2115-26. doi: 10.1016/s0140-6736(11)60243-2 [DOI:10.1016/S0140-6736(11)60243-2]
4. Al Rashoud A, Abboud R, Wang W, Wigderowitz C. Efficacy of low-level laser therapy applied at acupuncture points in knee osteoarthritis: A randomised double-blind comparative trial. Physiotherapy. 2014; 100(3):242-8. doi: 10.1016/j.physio.2013.09.007 [DOI:10.1016/j.physio.2013.09.007]
5. Blagojevic M, Jinks C, Jeffery A, Jordan K. Risk factors for onset of osteoarthritis of the knee in older adults: A systematic review and meta-analysis. Osteoarthritis and Cartilage. 2010; 18(1):24-33. doi: 10.1016/j.joca.2009.08.010 [DOI:10.1016/j.joca.2009.08.010]
6. Assis L, Milares LP, Almeida T, Tim C, Magri A, Fernandes KR, et al. Aerobic exercise training and low-level laser therapy modulate inflammatory response and degenerative process in an experimental model of knee osteoarthritis in rats. Osteoarthritis and Cartilage. 2016; 24(1):169-77. doi: 10.1016/j.joca.2015.07.020 [DOI:10.1016/j.joca.2015.07.020]
7. De Faria Coelho C, Leal-Junior ECP, Biasotto-Gonzalez DA, Bley AS, Politti F, De Oliveira Gonzalez T, et al. Effectiveness of phototherapy incorporated into an exercise program for osteoarthritis of the knee: Study protocol for a randomized controlled trial. Trials. 2014; 15(1):221. doi: 10.1186/1745-6215-15-221 [DOI:10.1186/1745-6215-15-221]
8. Lawrence RC, Felson DT, Helmick CG, Arnold LM, Choi H, Deyo RA, et al. Estimates of the prevalence of arthritis and other rheumatic conditions in the United States: Part II. Arthritis & Rheumatism. 2008; 58(1):26-35. doi: 10.1002/art.23176 [DOI:10.1002/art.23176]
9. De Meneses SRF, Hunter DJ, Docko EY, Marques AP. Effect of low-level laser therapy (904 nm) and static stretching in patients with knee osteoarthritis: A 10.1186/s12891-015-0709-9 protocol of randomised controlled trial. BMC Musculoskeletal Disorders. 2015; 16(1):252. doi:
10. Das SK, Farooqi A. Osteoarthritis. Best Practice & Research Clinical Rheumatology. 2008; 22(4):657–75. doi: 10.1016/j.berh.2008.07.002 [DOI:10.1016/j.berh.2008.07.002]
11. Siebuhr A, Petersen KK, Arendt-Nielsen L, Egsgaard LL, Eskehave T, Christiansen C, et al. Identification and characterisation of osteoarthritis patients with inflammation derived tissue turnover. Osteoarthritis and Cartilage. 2014; 22(1):44-50. doi: 10.1016/j.joca.2013.10.020 [DOI:10.1016/j.joca.2013.10.020]
12. Huang Z, Chen J, Ma J, Shen B, Pei F, Kraus VB. Effectiveness of low-level laser therapy in patients with knee osteoarthritis: A systematic review and meta-analysis. Osteoarthritis and Cartilage. 2015; 23(9):1437-44. doi: 10.1016/j.joca.2015.04.005 [DOI:10.1016/j.joca.2015.04.005]
13. Alghadir A, Omar MTA, Al-Askar AB, Al-Muteri NK. Effect of low-level laser therapy in patients with chronic knee osteoarthritis: A single-blinded randomized clinical study. Lasers in Medical Science. 2014; 29(2):749-55. doi: 10.1007/s10103-013-1393-3 [DOI:10.1007/s10103-013-1393-3]
14. Sanchez-Ramirez DC, van der Leeden M, van der Esch M, Roorda LD, Verschueren S, van Dieën JH, et al. Elevated C-reactive protein is associated with lower increase in knee muscle strength in patients with knee osteoarthritis: A 2-year follow-up study in the Amsterdam Osteoarthritis (AMS-OA) cohort. Arthritis Research & Therapy. 2014; 16(3):R123. doi: 10.1186/ar4580 [DOI:10.1186/ar4580]
15. Gur A, Cosut A, Jale Sarac A, Cevik R, Nas K, Uyar A. Efficacy of different therapy regimes of low‐power laser in painful osteoarthritis of the knee: A double‐blind and randomized‐controlled trial. Lasers in Surgery and Medicine. 2003; 33(5):330-8. doi: 10.1002/lsm.10236 [DOI:10.1002/lsm.10236]
16. Alfredo PP, Bjordal JM, Dreyer SH, Meneses SRF, Zaguetti G, Ovanessian V, et al. Efficacy of low level laser therapy associated with exercises in knee osteoarthritis: A randomized double-blind study. Clinical Rehabilitation. 2012; 26(6):523-33. doi: 10.1177/0269215511425962 [DOI:10.1177/0269215511425962]
17. Kheshie AR, Alayat MSM, Ali MME. High-intensity versus low-level laser therapy in the treatment of patients with knee osteoarthritis: A randomized controlled trial. Lasers in Medical Science. 2014; 29(4):1371-6. doi: 10.1007/s10103-014-1529-0 [DOI:10.1007/s10103-014-1529-0]
18. Bjordal J, Lopes-Martins R, Iversen V. A randomised, placebo controlled trial of low level laser therapy for activated Achilles tendinitis with microdialysis measurement of peritendinous prostaglandin E2 concentrations. British Journal of Sports Medicine. 2006; 40(1):76-80. doi: 10.1136/bjsm.2005.020842 [DOI:10.1136/bjsm.2005.020842]
19. Castano AP, Dai T, Yaroslavsky I, Cohen R, Apruzzese WA, Smotrich MH, et al. Low‐level laser therapy for zymosan‐induced arthritis in rats: Importance of illumination time. Lasers in Surgery and Medicine. 2007; 39(6):543-50. doi: 10.1002/lsm.20516 [DOI:10.1002/lsm.20516]
20. Rubio CR, Cremonezzi D, Moya M, Soriano F, Palma J, Campana V. Helium-neon laser reduces the inflammatory process of arthritis. Photomedicine and Laser Surgery. 2010; 28(1):125-9. doi: 10.1089/pho.2008.2472 [DOI:10.1089/pho.2008.2472]
21. Bjordal JM, Johnson MI, Iversen V, Aimbire F, Lopes-Martins RAB. Low-level laser therapy in acute pain: A systematic review of possible mechanisms of action and clinical effects in randomized placebo-controlled trials. Photomedicine and Laser Therapy. 2006; 24(2):158-68. doi: 10.1089/pho.2006.24.158 [DOI:10.1089/pho.2006.24.158]
22. Fukuda VO, Fukuda TY, Guimarães M, Shiwa S, de Lima BDC, Martins RÁBL, et al. Short-term efficacy of low-level laser therapy in patients with knee osteoarthritis: A randomized placebo-controlled, double-blind clinical trial. Revista Brasileira de Ortopedia (English Edition). 2011; 46(5):526-33. doi: 10.1016/s2255-4971(15)30407-9 [DOI:10.1016/S2255-4971(15)30407-9]
23. Hegedűs B, Viharos L, Gervain M, Gálfi M. The effect of low-level laser in knee osteoarthritis: A double-blind, randomized, placebo-controlled trial. Photomedicine and Laser Surgery. 2009; 27(4):577-84. doi: 10.1089/pho.2008.2297 [DOI:10.1089/pho.2008.2297]
24. Tascioglu F, Armagan O, Tabak Y, Corapci I, Oner C. Low power laser treatment in patients with knee osteoarthritis. Swiss Medical Weekly. 2004; 134(17-18):254-8. doi: PMID: 15243853
25. Bülow P, Jensen H, Danneskiold-Samsøe B. Low power Ga-Al-As laser treatment of painful osteoarthritis of the knee. A double-blind placebo-controlled study. Scandinavian Journal of Rehabilitation Medicine. 1994; 26(3):155-9. PMID: 7801065 [PMID]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Physical Treatments (PTJ)
University of Social Welfare and Rehabilitation Sciences, Koodakyar Alley, Daneshjoo Blv., Evin, Tehran, Iran
Journal Office Tel: +9821 71732822
Publisher Tel: +9821 4535 5555, 4535 5000 (EXT: 108)
Email: physicaltreatments@gmail.com
