Thu, Apr 25, 2024
Volume 6, Issue 4 (Winter 2017)
PTJ 2017, 6(4): 195-200 |
Back to browse issues page



Download citation:
BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:



BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
Rastgar Koutenaei F, Mosallanezhad Z, Hosseinzadeh S. The Relationship Between Anthropometric Characteristics and Low Back Pain in Women. PTJ 2017; 6 (4) :195-200
URL: http://ptj.uswr.ac.ir/article-1-307-en.html
URL: http://ptj.uswr.ac.ir/article-1-307-en.html


1- Department of Physiotherapy, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
2- Department of Biostatistics, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
2- Department of Biostatistics, University of Social Welfare and Rehabilitation Sciences, Tehran, Iran.
Full-Text [PDF 432 kb]
(1823 Downloads)
| Abstract (HTML) (5335 Views)
Full-Text: (5654 Views)
1. Introduction
Back pain is one of the most common musculoskeletal problems worldwide [1-4], imposing a huge economic cost to health care systems, individual, and community [1, 2]. Estimates show that 70% to 85% of the community have suffered from backache at least once in their lifetime [5, 6]. The annual prevalence of back pain in the United States is estimated to be 17.6% [7]. Therefore, recognizing the risk factors for back pain is an important issue [2].
Also, obesity is as a major public health problem and a matter of concern; its prevalence in developed countries as well as developing countries is growing fast [4]. According to the documentation, fat people are at risk of catching a wide range of chronic diseases such as diabetes, cardiovascular disease, cancer, and musculoskeletal problems [4, 8].
Body weight is an important factor regarding the amount of load on the lumbar spine which could shrink and destruct disk space [3, 4]. Many researches and experts have assumed a relationship between back pain and overweight [3, 9]. Some studies have shown a positive relationship between obesity and low back pain (LBP) [2, 10, 11]. Clinical observations and some research results have shown that severity of pain in patients with LBP reduces with weight loss [10]. There are also, studies that rejected the relationship between Body Mass Index (BMI) and LBP [12, 13]. In a systematic review study conducted in 2000, only 32% of studies supported the relationship between BMI and LBP [12]. Excessive obesity can increase the risk of LBP, but this cannot be said definitely in relation with overweight [2].
Industrialization of society and changing the lifestyle of individuals have increased the prevalence of obesity and various illnesses, including musculoskeletal diseases, cardiovascular diseases, and high mortality rates [4, 8]. Nevertheless, studies have no consensus over the index that has the most impact on LBP and studies conducted so far have shown controversial results [10-13]. Therefore, according to the above mentioned, the importance of the present study is emphasized.
Many researchers regard the measurement of body anthropometric indices as the easiest way to evaluate obesity. The most important anthropometric indices evaluated in relation to the obesity are subcutaneous fat in different areas, BMI, waist circumference index, hip circumference, Waist to Hip Ratio (WHR), and Body Fat Percentage (FBP) [14, 15]. Therefore, in this research our goal is to investigate the relationship between these anthropometric indices with LBP over the past year.
2. Materials and Methods
This cross-sectional study is descriptive-analytical. The study participants were selected by convenience sampling method, including 60 women in age range of 20 and 40 years. Of them, 30 subjects had experienced back pain and 30 had no back pain over the past year. The study subjects were grouped into LBP and healthy. Exclusion criteria comprised pregnant women, those who gave birth during the last three months, and those who had a history of falling on the ground on their waist. First, the participants signed the consent form and completed the demographic questionnaire. The necessary explanations concerning the objectives and methods of study were given to them. In addition, they were reassured that their information remains confidential and the research process would not create any risks and complications for them.
Before starting the main study, repeatability of measurement methods was investigated. Then, measurements were done with tape, scales, and caliper based on specific landmarks. First, the subjects’ height and weight were measured with tape meter and balance. To measure waist circumference, the tape meter was placed at the level of the narrowest trunk area and to measure the hip circumference, the meter was placed around the hip over the thickest posterior prominence of the buttocks [14, 15]. To measure the thickness of subcutaneous fat of triceps, quadriceps, and suprailiac region, the caliper was used [15].
So that, after taking the skin with two fingers, caliber opening was put 1 to 1.5 cm lower than fingers. Then, the thickness of the skin is measured by caliper. To measure subcutaneous fat of triceps muscle, caliper was placed in the middle spot of the distance between the shoulder tips down to the back side of the arm and in an elbow extension position and the vertical skin fold was measured. The skin subcutaneous fat of the quadriceps muscle was measured through a vertical fold in the anterior mid-thigh position. To measure hip suprailiac fold, the caliper was placed on top of the anterior superior iliac spine and 3 cm towards the navel and the diagonal skin fold is measured. To measure BFP, the Jackson and Pollock formula was used in women [15].
Db=1/0994921-(0/0009929×SUM)+(0/0000023×(SUM)2)-(0/0001392×AGE)
The result of this formula is the density of the body and after calculating the total body density, the percentage of body fat is obtained through the following formula:
%BF=(495/Db)-450
A: Skinfold of triceps muscle; B: Skinfold of quadriceps muscle; C: Suprailiac skinfold; SUM: Sum of three points in millimeter; Db: Density of body; AGE: Age in year; and %BF: Body fat percentage.
Purpose and method of this study was approved by the Ethics Committee of the University of Social Welfare and Rehabilitation (code: IR.USWR.REC.1395.221). To analyze the data, SPSS22 was used and to test the hypotheses, a significant level of 0.05 was considered.
3. Results
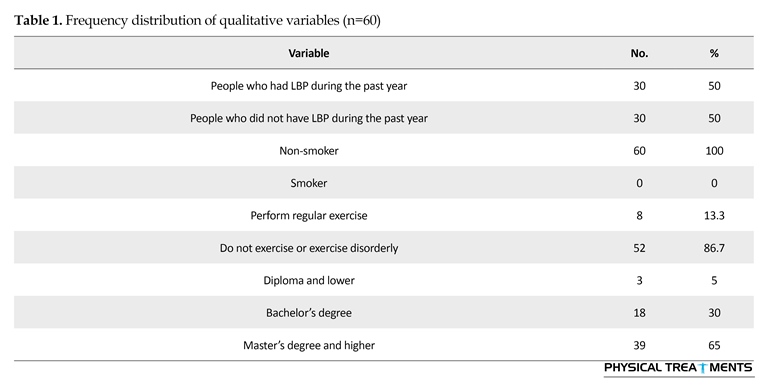
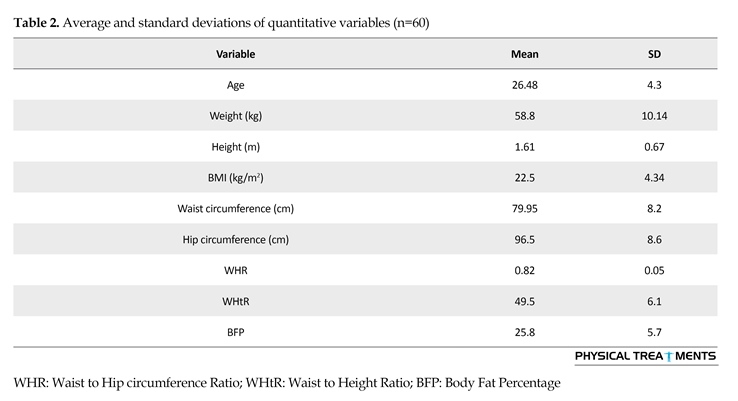
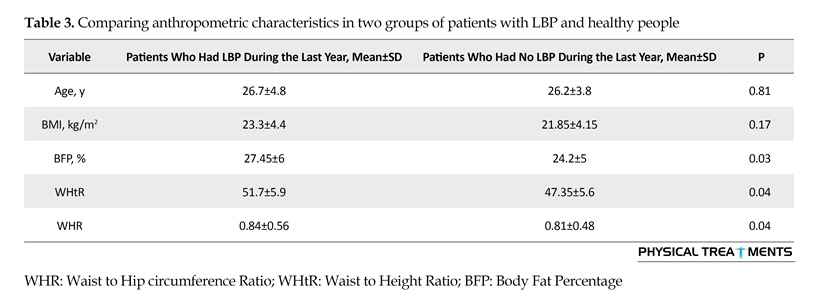
Repeatability results of measurement methods were acceptable. Demographic characteristics of the subjects are presented in Tables 1 and 2. Also, to investigate the distribution of data in two LBP and healthy groups, first the Kolmogorov-Smirnov test was performed. Regarding the lack of data normality, to investigate the relationship between anthropometric characteristics of individuals and LBP, non-parametric Mann-Whitney test was used. The results are presented in Table 3.
There was no significant difference between two groups with respect to their average age. Although the average BMI was higher in patients with LBP, the difference was not statistically significant (P=0.17). The mean values of WHR (P=0.04), WHtR (0.04), and BFP (P=0.03) were significantly higher in patients with LBP.
4. Discussion
Generally, the study results did not verify the relationship between body mass and back pain, but supported the relationship between other anthropometric indices and the incidence of LBP. BMI was not higher in the group with LBP, compared to the healthy group. The average values of WHR, WHtR, and BFP were higher in patients with LBP compared to healthy people.
In a study in 2016, the researchers concluded that patients with higher BMI and WHR have a wider lumbosacral angle; these biomechanical changes can have relationship with an increase in LBP [16]. In another study, they concluded that there was a relationship between obesity and ineffectiveness of LBP treatment. The researchers also reported a relationship between BMI and the outcome of treatment for patients with LBP [17]. Another study showed that higher BMI in women increased the prevalence of LBP in them but this relationship was not observed in men [18]. The results of these studies concerning the relationship of BMI and back pain are not consistent with the results of our study.
However, in a systematic review study conducted in 2015, some lose evidence of the relationship between chronic LBP and obesity was observed, nevertheless the authors pointed out that there was no significant relationship between overweight and back pain [1]. In another systematic review study, a poor relationship was observed between BMI and back pain in women but the relationship between obesity and non-specific chronic LBP was not observed in men [19]. Also, in a systematic review in 2000, it was concluded that only in 32% of studies there is a relationship between BMI and low back pain [12]. Another study also reported no relationship between BMI and LBP [6] and its results are consistent with our research. The results of the studies show that the main cause of LBP and various illnesses is obesity i.e., having the BMI between 25 and 30 [1, 6]. However, in the present study, BMI in the LBP group was lower than this amount. Therefore, this might be the reason why there is no relationship between high BMI and LBP in the present study and similar studies.
Back pain is one of the most common musculoskeletal problems worldwide [1-4], imposing a huge economic cost to health care systems, individual, and community [1, 2]. Estimates show that 70% to 85% of the community have suffered from backache at least once in their lifetime [5, 6]. The annual prevalence of back pain in the United States is estimated to be 17.6% [7]. Therefore, recognizing the risk factors for back pain is an important issue [2].
Also, obesity is as a major public health problem and a matter of concern; its prevalence in developed countries as well as developing countries is growing fast [4]. According to the documentation, fat people are at risk of catching a wide range of chronic diseases such as diabetes, cardiovascular disease, cancer, and musculoskeletal problems [4, 8].
Body weight is an important factor regarding the amount of load on the lumbar spine which could shrink and destruct disk space [3, 4]. Many researches and experts have assumed a relationship between back pain and overweight [3, 9]. Some studies have shown a positive relationship between obesity and low back pain (LBP) [2, 10, 11]. Clinical observations and some research results have shown that severity of pain in patients with LBP reduces with weight loss [10]. There are also, studies that rejected the relationship between Body Mass Index (BMI) and LBP [12, 13]. In a systematic review study conducted in 2000, only 32% of studies supported the relationship between BMI and LBP [12]. Excessive obesity can increase the risk of LBP, but this cannot be said definitely in relation with overweight [2].
Industrialization of society and changing the lifestyle of individuals have increased the prevalence of obesity and various illnesses, including musculoskeletal diseases, cardiovascular diseases, and high mortality rates [4, 8]. Nevertheless, studies have no consensus over the index that has the most impact on LBP and studies conducted so far have shown controversial results [10-13]. Therefore, according to the above mentioned, the importance of the present study is emphasized.
Many researchers regard the measurement of body anthropometric indices as the easiest way to evaluate obesity. The most important anthropometric indices evaluated in relation to the obesity are subcutaneous fat in different areas, BMI, waist circumference index, hip circumference, Waist to Hip Ratio (WHR), and Body Fat Percentage (FBP) [14, 15]. Therefore, in this research our goal is to investigate the relationship between these anthropometric indices with LBP over the past year.
2. Materials and Methods
This cross-sectional study is descriptive-analytical. The study participants were selected by convenience sampling method, including 60 women in age range of 20 and 40 years. Of them, 30 subjects had experienced back pain and 30 had no back pain over the past year. The study subjects were grouped into LBP and healthy. Exclusion criteria comprised pregnant women, those who gave birth during the last three months, and those who had a history of falling on the ground on their waist. First, the participants signed the consent form and completed the demographic questionnaire. The necessary explanations concerning the objectives and methods of study were given to them. In addition, they were reassured that their information remains confidential and the research process would not create any risks and complications for them.
Before starting the main study, repeatability of measurement methods was investigated. Then, measurements were done with tape, scales, and caliper based on specific landmarks. First, the subjects’ height and weight were measured with tape meter and balance. To measure waist circumference, the tape meter was placed at the level of the narrowest trunk area and to measure the hip circumference, the meter was placed around the hip over the thickest posterior prominence of the buttocks [14, 15]. To measure the thickness of subcutaneous fat of triceps, quadriceps, and suprailiac region, the caliper was used [15].
So that, after taking the skin with two fingers, caliber opening was put 1 to 1.5 cm lower than fingers. Then, the thickness of the skin is measured by caliper. To measure subcutaneous fat of triceps muscle, caliper was placed in the middle spot of the distance between the shoulder tips down to the back side of the arm and in an elbow extension position and the vertical skin fold was measured. The skin subcutaneous fat of the quadriceps muscle was measured through a vertical fold in the anterior mid-thigh position. To measure hip suprailiac fold, the caliper was placed on top of the anterior superior iliac spine and 3 cm towards the navel and the diagonal skin fold is measured. To measure BFP, the Jackson and Pollock formula was used in women [15].
Db=1/0994921-(0/0009929×SUM)+(0/0000023×(SUM)2)-(0/0001392×AGE)
The result of this formula is the density of the body and after calculating the total body density, the percentage of body fat is obtained through the following formula:
%BF=(495/Db)-450
A: Skinfold of triceps muscle; B: Skinfold of quadriceps muscle; C: Suprailiac skinfold; SUM: Sum of three points in millimeter; Db: Density of body; AGE: Age in year; and %BF: Body fat percentage.
Purpose and method of this study was approved by the Ethics Committee of the University of Social Welfare and Rehabilitation (code: IR.USWR.REC.1395.221). To analyze the data, SPSS22 was used and to test the hypotheses, a significant level of 0.05 was considered.
3. Results
Repeatability results of measurement methods were acceptable. Demographic characteristics of the subjects are presented in Tables 1 and 2. Also, to investigate the distribution of data in two LBP and healthy groups, first the Kolmogorov-Smirnov test was performed. Regarding the lack of data normality, to investigate the relationship between anthropometric characteristics of individuals and LBP, non-parametric Mann-Whitney test was used. The results are presented in Table 3.
There was no significant difference between two groups with respect to their average age. Although the average BMI was higher in patients with LBP, the difference was not statistically significant (P=0.17). The mean values of WHR (P=0.04), WHtR (0.04), and BFP (P=0.03) were significantly higher in patients with LBP.
4. Discussion
Generally, the study results did not verify the relationship between body mass and back pain, but supported the relationship between other anthropometric indices and the incidence of LBP. BMI was not higher in the group with LBP, compared to the healthy group. The average values of WHR, WHtR, and BFP were higher in patients with LBP compared to healthy people.
In a study in 2016, the researchers concluded that patients with higher BMI and WHR have a wider lumbosacral angle; these biomechanical changes can have relationship with an increase in LBP [16]. In another study, they concluded that there was a relationship between obesity and ineffectiveness of LBP treatment. The researchers also reported a relationship between BMI and the outcome of treatment for patients with LBP [17]. Another study showed that higher BMI in women increased the prevalence of LBP in them but this relationship was not observed in men [18]. The results of these studies concerning the relationship of BMI and back pain are not consistent with the results of our study.
However, in a systematic review study conducted in 2015, some lose evidence of the relationship between chronic LBP and obesity was observed, nevertheless the authors pointed out that there was no significant relationship between overweight and back pain [1]. In another systematic review study, a poor relationship was observed between BMI and back pain in women but the relationship between obesity and non-specific chronic LBP was not observed in men [19]. Also, in a systematic review in 2000, it was concluded that only in 32% of studies there is a relationship between BMI and low back pain [12]. Another study also reported no relationship between BMI and LBP [6] and its results are consistent with our research. The results of the studies show that the main cause of LBP and various illnesses is obesity i.e., having the BMI between 25 and 30 [1, 6]. However, in the present study, BMI in the LBP group was lower than this amount. Therefore, this might be the reason why there is no relationship between high BMI and LBP in the present study and similar studies.


Also, in a study, the researchers concluded that higher waist circumference, hip circumference, and WHR in women increase the prevalence of LBP in women, but this is not the case in men [18]. In another study, the relationship between higher waist circumference and the prevalence of LBP was proved [2]. In another study, it was shown that the higher WHR increases the chance of a positive SLR (straight leg raise) test and exacerbation of back pain in women [20]. These results are consistent with the present study. But in another study, higher WHR reduced the risk of exacerbation of LBP [21]. Also in several studies, LBP in tall people was not reported more severe than LBP in short subjects [2, 21]. However, in the present study, a significant and weak relationship was observed between WHtR with LBP in women.
In another study, a significant relationship was shown between BMI and BFP and the higher amount of these two indices increased the risk of LBP, although this relationship was weak [22]. On the other hand, the present study shows the greatest relationship between the incidence of LBP and BFP compared to other anthropometric features. One reason for the different results can be that in various studies, different areas have been considered for distribution of BFP [14].
Conducting further studies with more participants, a wider age range, and taking into account other indices can yield more findings. Also, evaluation of these indices in men can help identify gender differences in this regard. The results of this study did not approve the relationship between body mass and LBP, but the relationship between the incidence of LBP and the other anthropometric indices, including the WHR, WHtR, and BFP was supported. Moreover, the relationship between BFP and LBP was the strongest. This study showed that BFP can be a stronger indicator of LBP.
In another study, a significant relationship was shown between BMI and BFP and the higher amount of these two indices increased the risk of LBP, although this relationship was weak [22]. On the other hand, the present study shows the greatest relationship between the incidence of LBP and BFP compared to other anthropometric features. One reason for the different results can be that in various studies, different areas have been considered for distribution of BFP [14].
Conducting further studies with more participants, a wider age range, and taking into account other indices can yield more findings. Also, evaluation of these indices in men can help identify gender differences in this regard. The results of this study did not approve the relationship between body mass and LBP, but the relationship between the incidence of LBP and the other anthropometric indices, including the WHR, WHtR, and BFP was supported. Moreover, the relationship between BFP and LBP was the strongest. This study showed that BFP can be a stronger indicator of LBP.

Based on the results of this study, anthropometric indices, including the WHR, WHtR, the average value of BFP, and BMI above 25 are good indices to predict the incidence of LBP; among which the relationship of BFP index with the incidence of LBP was the strongest.
Acknowledgements
The present paper is extracted from the MSc. thesis of the first author, Forouzan Rastgar Koutenaei, at the Department of Physiotherapy, University of Social Welfare and Rehabilitation Sciences, Tehran. We appreciate the cooperation of all study participants and other people who helped us with conducting this study.
Conflict of Interest
The authors declared no conflict of interests.
References
[1]Alhalabi M, Alhaleeb H, Madani S. Risk factors associated with chronic low back pain in Syria. Avicenna Journal of Medicine. 2015; 5(4):110. doi: 10.4103/2231-0770.165123
[2]Heuch I, Heuch I, Hagen K, Zwart J.A. A comparison of anthropometric measures for assessing the association between body size and risk of chronic low back pain: The HUNT study. Plos One. 2015; 10(10):0141268. doi: 10.1371/journal.pone.0141268
[3]Han TS, Schouten JSAG, Lean MEJ, Seidell JC. The prevalence of low back pain and associations with body fatness, fat distribution and height. International Journal of Obesity. 1997; 21(7):600–7. doi: 10.1038/sj.ijo.0800448
[4]Dario AB, Ferreira ML, Refshauge KM, Lima TS, Ordoñana JR, Ferreira PH. The relationship between obesity, low back pain, and lumbar disc degeneration when genetics and the environment are considered: A systematic review of twin studies. Spine Journal. 2015; 15(5):1106–17. doi: 10.1016/j.spinee.2015.02.001
[5]Andersson GB. Epidemiological features of chronic low back pain. Lancet. 1999; 354(9178):581–5. doi: 10.1016/s0140-6736(99)01312-4
[6]Mirtz TA, Greene L. Is obesity a risk factor for low back pain? An example of using the evidence to answer a clinical question. Chiropractic & Manual Therapies. 2005; 13(1):2. doi: 10.1186/1746-1340-13-2
[7]Guo HR, Tanaka S, Halperin WE, Cameron LL. Back pain prevalence in US industry and estimates of lost workdays. American Journal of Public Health. 1999; 89(7):1029–35. doi: 10.2105/ajph.89.7.1029
[8]Dee A, Callinan A, Doherty E, O’Neill C, McVeigh T, Sweeney MR, et al. Overweight and obesity on the island of Ireland: An estimation of costs. BMJ Open . 2015; 5(3):006189. doi: 10.1136/bmjopen-2014-006189
[9]Popkess-Vawter S, Patzel B. Compounded problem: Chronic low back pain and overweight in adult females. Orthopaedic Nursing. 1992; 11(6):31. doi: 10.1097/00006416-199211000-00006
[10]Daentzer D, Hohls T, Noll C. Has overweight any influence on the effectiveness of conservative treatment in patients with low back pain. European Spine Journal. 2014; 24(3):467–73. doi: 10.1007/s00586-014-3425-5
[11]Urquhart DM, Berry P, Wluka AE, Strauss BJ, Wang Y, Proietto J, et al. Young investigator award winner. Spine. 2011; 36(16):1320–5. doi: 10.1097/brs.0b013e3181f9fb66
[12]Leboeuf-Yde C. Body weight and low back pain. Spine. 2000; 25(2):226. doi: 10.1097/00007632-200001150-00015
[13]Garzillo MJ, Garzillo TA. Does obesity cause low back pain. Journal of Manipulative and Physiological Therapeutics. 1994; 17(9):601-4. PMID: 7884330
[14]Jalalvand A , Ahanjan S , Golpayegani M , Anbarian M. [Relationship between anthropometric indexes and somatotype (Persian)]. Oloom-e Harkati va Varzesh. 2007; 5(9):83-94.
[15]Aghayari A, Honari H, Babaei Mobarakeh M. Standardization BMI, WHR, WC and body fat percentage among women candidates physical education course in Payame Noor University. Applied Research of Sport Management and Biology. 2012; 1(1):81-94.
[16]Onyemaechi N, Anyanwu G, Obikili E, Onwuasoigwe O, Nwankwo O. Impact of overweight and obesity on the musculoskeletal system using lumbosacral angles. Patient Preference and Adherence. 2016; 10:291. doi: 10.2147/ppa.s90967
[17]Ewald SC, Hurwitz EL, Kizhakkeveettil A. The effect of obesity on treatment outcomes for low back pain. Chiropractic & Manual Therapies. 2016; 24:48. doi: 10.1186/s12998-016-0129-4
[18]Shiri R, Solovieva S, Husgafvel-Pursiainen K, Taimela S, Saarikoski LA, Huupponen R, et al. The association between obesity and the prevalence of low back pain in young adults: The cardiovascular risk in young Finns study. American Journal of Epidemiology. 2008; 167(9):1110–9. doi: 10.1093/aje/kwn007
[19]Frilander H, Solovieva S, Mutanen P, Pihlajamäki H, Heliövaara M, Viikari-Juntura E. Role of overweight and obesity in low back disorders among men: A longitudinal study with a life course approach. BMJ. 2015; 5(8):007805. doi: 10.1136/bmjopen-2015-007805
[20]Toda Y, Segal N, Toda T, Morimoto T, Ogawa R. Lean body mass and body fat distribution in participants with chronic low back pain. Archives of Internal Medicine. 2000; 160(21):3265. doi: 10.1001/archinte.160.21.3265
[21]Yip YB, Ho SC, Chan SG. Tall stature, overweight and the prevalence of low back pain in Chinese middle-aged women. International Journal of Obesity. 2001; 25(6):887–92. doi: 10.1038/sj.ijo.0801557
[22]Dario AB, Ferreira ML, Refshauge K, Sánchez-Romera JF, Luque-Suarez A, Hopper JL, et al. Are obesity and body fat distribution associated with low back pain in women? A population-based study of 1128 Spanish twins. European Spine Journal. 2015; 25(4):1188–95. doi: 10.1007/s00586-015-4055-2
Acknowledgements
The present paper is extracted from the MSc. thesis of the first author, Forouzan Rastgar Koutenaei, at the Department of Physiotherapy, University of Social Welfare and Rehabilitation Sciences, Tehran. We appreciate the cooperation of all study participants and other people who helped us with conducting this study.
Conflict of Interest
The authors declared no conflict of interests.
References
[1]Alhalabi M, Alhaleeb H, Madani S. Risk factors associated with chronic low back pain in Syria. Avicenna Journal of Medicine. 2015; 5(4):110. doi: 10.4103/2231-0770.165123
[2]Heuch I, Heuch I, Hagen K, Zwart J.A. A comparison of anthropometric measures for assessing the association between body size and risk of chronic low back pain: The HUNT study. Plos One. 2015; 10(10):0141268. doi: 10.1371/journal.pone.0141268
[3]Han TS, Schouten JSAG, Lean MEJ, Seidell JC. The prevalence of low back pain and associations with body fatness, fat distribution and height. International Journal of Obesity. 1997; 21(7):600–7. doi: 10.1038/sj.ijo.0800448
[4]Dario AB, Ferreira ML, Refshauge KM, Lima TS, Ordoñana JR, Ferreira PH. The relationship between obesity, low back pain, and lumbar disc degeneration when genetics and the environment are considered: A systematic review of twin studies. Spine Journal. 2015; 15(5):1106–17. doi: 10.1016/j.spinee.2015.02.001
[5]Andersson GB. Epidemiological features of chronic low back pain. Lancet. 1999; 354(9178):581–5. doi: 10.1016/s0140-6736(99)01312-4
[6]Mirtz TA, Greene L. Is obesity a risk factor for low back pain? An example of using the evidence to answer a clinical question. Chiropractic & Manual Therapies. 2005; 13(1):2. doi: 10.1186/1746-1340-13-2
[7]Guo HR, Tanaka S, Halperin WE, Cameron LL. Back pain prevalence in US industry and estimates of lost workdays. American Journal of Public Health. 1999; 89(7):1029–35. doi: 10.2105/ajph.89.7.1029
[8]Dee A, Callinan A, Doherty E, O’Neill C, McVeigh T, Sweeney MR, et al. Overweight and obesity on the island of Ireland: An estimation of costs. BMJ Open . 2015; 5(3):006189. doi: 10.1136/bmjopen-2014-006189
[9]Popkess-Vawter S, Patzel B. Compounded problem: Chronic low back pain and overweight in adult females. Orthopaedic Nursing. 1992; 11(6):31. doi: 10.1097/00006416-199211000-00006
[10]Daentzer D, Hohls T, Noll C. Has overweight any influence on the effectiveness of conservative treatment in patients with low back pain. European Spine Journal. 2014; 24(3):467–73. doi: 10.1007/s00586-014-3425-5
[11]Urquhart DM, Berry P, Wluka AE, Strauss BJ, Wang Y, Proietto J, et al. Young investigator award winner. Spine. 2011; 36(16):1320–5. doi: 10.1097/brs.0b013e3181f9fb66
[12]Leboeuf-Yde C. Body weight and low back pain. Spine. 2000; 25(2):226. doi: 10.1097/00007632-200001150-00015
[13]Garzillo MJ, Garzillo TA. Does obesity cause low back pain. Journal of Manipulative and Physiological Therapeutics. 1994; 17(9):601-4. PMID: 7884330
[14]Jalalvand A , Ahanjan S , Golpayegani M , Anbarian M. [Relationship between anthropometric indexes and somatotype (Persian)]. Oloom-e Harkati va Varzesh. 2007; 5(9):83-94.
[15]Aghayari A, Honari H, Babaei Mobarakeh M. Standardization BMI, WHR, WC and body fat percentage among women candidates physical education course in Payame Noor University. Applied Research of Sport Management and Biology. 2012; 1(1):81-94.
[16]Onyemaechi N, Anyanwu G, Obikili E, Onwuasoigwe O, Nwankwo O. Impact of overweight and obesity on the musculoskeletal system using lumbosacral angles. Patient Preference and Adherence. 2016; 10:291. doi: 10.2147/ppa.s90967
[17]Ewald SC, Hurwitz EL, Kizhakkeveettil A. The effect of obesity on treatment outcomes for low back pain. Chiropractic & Manual Therapies. 2016; 24:48. doi: 10.1186/s12998-016-0129-4
[18]Shiri R, Solovieva S, Husgafvel-Pursiainen K, Taimela S, Saarikoski LA, Huupponen R, et al. The association between obesity and the prevalence of low back pain in young adults: The cardiovascular risk in young Finns study. American Journal of Epidemiology. 2008; 167(9):1110–9. doi: 10.1093/aje/kwn007
[19]Frilander H, Solovieva S, Mutanen P, Pihlajamäki H, Heliövaara M, Viikari-Juntura E. Role of overweight and obesity in low back disorders among men: A longitudinal study with a life course approach. BMJ. 2015; 5(8):007805. doi: 10.1136/bmjopen-2015-007805
[20]Toda Y, Segal N, Toda T, Morimoto T, Ogawa R. Lean body mass and body fat distribution in participants with chronic low back pain. Archives of Internal Medicine. 2000; 160(21):3265. doi: 10.1001/archinte.160.21.3265
[21]Yip YB, Ho SC, Chan SG. Tall stature, overweight and the prevalence of low back pain in Chinese middle-aged women. International Journal of Obesity. 2001; 25(6):887–92. doi: 10.1038/sj.ijo.0801557
[22]Dario AB, Ferreira ML, Refshauge K, Sánchez-Romera JF, Luque-Suarez A, Hopper JL, et al. Are obesity and body fat distribution associated with low back pain in women? A population-based study of 1128 Spanish twins. European Spine Journal. 2015; 25(4):1188–95. doi: 10.1007/s00586-015-4055-2
Type of Study: Research |
Subject:
Special
Received: 2017/03/6 | Accepted: 2017/07/3 | Published: 2017/08/6
Received: 2017/03/6 | Accepted: 2017/07/3 | Published: 2017/08/6
References
1. Aghayari A, Honari H, Babaei Mobarakeh M. Standardization BMI, WHR, WC and body fat percentage among women candidates physical education course in Payame Noor University. Applied Research of Sport Management and Biology. 2012; 1(1):81-94. [Article]
2. Alhalabi M, Alhaleeb H, Madani S. Risk factors associated with chronic low back pain in Syria. Avicenna Journal of Medicine. 2015; 5(4):110. doi: 10.4103/2231-0770.165123 [Article] [DOI]
3. Andersson GB. Epidemiological features of chronic low back pain. Lancet. 1999; 354(9178):581–5. doi: 10.1016/s0140- 6736(99)01312-4 [Article] [DOI]
4. Daentzer D, Hohls T, Noll C. Has overweight any influence on the effectiveness of conservative treatment in patients with low back pain. European Spine Journal. 2014; 24(3):467–73. doi: 10.1007/s00586-014-3425-5 [Article] [DOI]
5. Dario AB, Ferreira ML, Refshauge K, Sánchez-Romera JF, Luque-Suarez A, Hopper JL, et al. Are obesity and body fat distribution associated with low back pain in women? A population- based study of 1128 Spanish twins. European Spine Journal. 2015; 25(4):1188–95. doi: 10.1007/s00586-015-4055-2 [Article] [DOI]
6. Dario AB, Ferreira ML, Refshauge KM, Lima TS, Ordoñana JR, Ferreira PH. The relationship between obesity, low back pain, and lumbar disc degeneration when genetics and the environment are considered: A systematic review of twin studies. Spine Journal. 2015; 15(5):1106–17. doi: 10.1016/j. spinee.2015.02.001 [Article] [DOI]
7. Dee A, Callinan A, Doherty E, O’Neill C, McVeigh T, Sweeney MR, et al. Overweight and obesity on the island of Ireland: An estimation of costs. BMJ Open . 2015; 5(3):006189. doi: 10.1136/ bmjopen-2014-006189 [Article] [DOI]
8. Ewald SC, Hurwitz EL, Kizhakkeveettil A. The effect of obesity on treatment outcomes for low back pain. Chiropractic & Manual Therapies. 2016; 24:48. doi: 10.1186/s12998-016-0129-4 [Article] [DOI]
9. Frilander H, Solovieva S, Mutanen P, Pihlajamäki H, Heliövaara M, Viikari-Juntura E. Role of overweight and obesity in low back disorders among men: A longitudinal study with a life course approach. BMJ. 2015; 5(8):007805. doi: 10.1136/bmjopen-2015-007805 [Article] [DOI]
10. Garzillo MJ, Garzillo TA. Does obesity cause low back pain. Journal of Manipulative and Physiological Therapeutics. 1994; 17(9):601-4. PMID: 7884330 [Article] [PubMed]
11. Guo HR, Tanaka S, Halperin WE, Cameron LL. Back pain prevalence in US industry and estimates of lost workdays. American Journal of Public Health. 1999; 89(7):1029–35. doi: 10.2105/ajph.89.7.1029 [Article] [DOI]
12. Han TS, Schouten JSAG, Lean MEJ, Seidell JC. The prevalence of low back pain and associations with body fatness, fat distribution and height. International Journal of Obesity. 1997; 21(7):600–7. doi: 10.1038/sj.ijo.0800448 [Article] [DOI]
13. Heuch I, Heuch I, Hagen K, Zwart J.A. A comparison of anthropometric measures for assessing the association between body size and risk of chronic low back pain: The HUNT study. Plos One. 2015; 10(10):0141268. doi: 10.1371/journal.pone.0141268 [Article] [DOI]
14. Jalalvand A , Ahanjan S , Golpayegani M , Anbarian M. [Relationship between anthropometric indexes and somatotype (Persian)]. Oloom-e Harkati va Varzesh. 2007; 5(9):83-94. [Article]
15. Leboeuf-Yde C. Body weight and low back pain. Spine. 2000; 25(2):226. doi: 10.1097/00007632-200001150-00015 [Article] [DOI]
16. Mirtz TA, Greene L. Is obesity a risk factor for low back pain? An example of using the evidence to answer a clinical question. Chiropractic & Manual Therapies. 2005; 13(1):2. doi: 10.1186/1746-1340-13-2 [Article] [DOI]
17. Onyemaechi N, Anyanwu G, Obikili E, Onwuasoigwe O, Nwankwo O. Impact of overweight and obesity on the musculoskeletal system using lumbosacral angles. Patient Preference and Adherence. 2016; 10:291. doi: 10.2147/ppa.s90967 [Article] [DOI]
18. Popkess-Vawter S, Patzel B. Compounded problem: Chronic low back pain and overweight in adult females. Orthopaedic Nursing. 1992; 11(6):31. doi: 10.1097/00006416-199211000- 00006 [Article] [DOI]
19. Shiri R, Solovieva S, Husgafvel-Pursiainen K, Taimela S, Saarikoski LA, Huupponen R, et al. The association between obesity and the prevalence of low back pain in young adults: The cardiovascular risk in young Finns study. American Journal of Epidemiology. 2008; 167(9):1110–9. doi: 10.1093/aje/ kwn007 [Article] [DOI]
20. Toda Y, Segal N, Toda T, Morimoto T, Ogawa R. Lean body mass and body fat distribution in participants with chronic low back pain. Archives of Internal Medicine. 2000; 160(21):3265. doi: 10.1001/archinte.160.21.3265 [Article] [DOI]
Send email to the article author
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Physical Treatments (PTJ)
University of Social Welfare and Rehabilitation Sciences, Koodakyar Alley, Daneshjoo Blv., Evin, Tehran, Iran
Journal Office Tel: +9821 71732822
Publisher Tel: +9821 4535 5555, 4535 5000 (EXT: 108)
Email: physicaltreatments@gmail.com
